")
Back to Journals » Transplant Research and Risk Management » Volume 14
A Unique Case of Tacrolimus-Induced Dysphagia and Dysarthria in the Absence of Diagnostic Findings
Authors Kanegi SL , Crane GD , Scott KJ, Thomas E
Received 22 June 2022
Accepted for publication 4 August 2022
Published 5 September 2022 Volume 2022:14 Pages 47—51
DOI https://doi.org/10.2147/TRRM.S378778
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qing Yi
Skyler L Kanegi, George D Crane, Kacie J Scott, Elizabeth Thomas
Department of Surgery, Long School of Medicine, The University of Texas Health Science Center at San Antonio, San Antonio, TX, USA
Correspondence: Elizabeth Thomas, Department of Surgery, Long School of Medicine, The University of Texas Health Science, 7703 Floyd Curl Drive, MSC: 7858, San Antonio, TX, 78229, USA, Tel +1 210-567-7000, Email [email protected]
Abstract: Tacrolimus is a cornerstone immunosuppressant with high efficacy in preventing graft rejection in liver recipients. However, neurotoxic side effects such as posterior reversible encephalopathy syndrome (PRES) may occur. Patients often exhibit seizures, encephalopathy, headache, and hypertension. This case describes a 68-year-old female who received deceased donor liver transplantation and was started on an immunosuppressive regiment of tacrolimus which was adjusted to therapeutic trough. Graft function was preserved throughout post-operative course. The patient experienced a prolonged intubation period complicated by failed spontaneous breathing tests until post-operative day (POD) 8. From POD 8– 16, the patient experienced dysphagia. From POD 13– 16, the patient exhibited altered mental status and dysarthria. Throughout presentation of these symptoms, the patient had no radiographic findings, lab findings, or hypertension. On POD 15, tacrolimus was discontinued in favor of cyclosporine. By POD 17, the patient experienced complete resolution of her encephalopathy, dysphagia, and dysarthria. The patient was discharged on POD 24. This is the first known case of dysphagia and dysarthria as major presenting symptoms of tacrolimus toxicity. Discontinuing tacrolimus in favor of cyclosporine can successfully resolve a constellation of neurotoxic symptoms that do not fit a classic picture of PRES.
Keywords: deceased, liver, PRES, neurotoxicity, dysarthria, dysphagia
Introduction
Calcineurin inhibitors, such as tacrolimus, represent a cornerstone immunosuppressant, because of their efficacy and prevalence. Tacrolimus, which inhibits FK-binding protein, can lead to metabolic syndrome, while cyclosporine, which inhibits cyclophilin, can lead to hypertension and vasculopathy.1
Despite these differences, tacrolimus was overwhelmingly superior across all patient groups in reducing one-year mortality, rate of rejection, and length of steroid-resistant rejection periods, when compared to cyclosporine.2 Thus, it is the most common anti-rejection prophylaxis and has a target trough of 6–12 ng/mL in the first month post-transplantation.3
However, calcineurin inhibitors, especially tacrolimus, are the second-most common cause of posterior reversible encephalopathy syndrome (PRES), after hypertension.4 Calcineurin is diffusely expressed in the brain, where it is the only calcium-activated phosphatase and a key regulator of synaptic and neuroexcitatory protein transcription. Tacrolimus may be neurotoxic in an estimated 1–10% of liver transplantation cases due to damage of the blood–brain barrier, excess endothelin, or alterations in mitochondria function, which may ultimately result in PRES.5
The most common presenting symptoms of PRES include seizures (74%), encephalopathy (28%), headache (26%), and visual disturbances (20%). Hypertension is present in 70% of cases, including in most cases caused by tacrolimus.4 Although MRI is the preferred imaging modality, MRI and CT have equal sensitivity for PRES in the literature.6
Here, we describe a unique case of a liver recipient who experienced tacrolimus-induced dysarthria and dysarthria without common presenting symptoms or radiographic findings.
Clinical Course
In March 2022, a 68-year-old female with past medical history of decompensated NASH cirrhosis was admitted to the transplant surgery service for deceased donor liver transplantation. Prior to surgery, her cirrhosis was manifested by ascites with no history of spontaneous bacterial peritonitis and mild portosystemic encephalopathy. Pre-transplantation MELD was 27. The liver was donated voluntarily with written informed consent, and consent was verified by the procuring surgeon and organ procurement organization, which complies with the Declaration of Istanbul.
ICU
The patient did well intraoperatively and had immediate graft function. On post-operative day (POD) 0, the patient was started on an immunosuppressive regiment of tacrolimus 1/1 sublingual, mycophenolate 1 g twice daily, and methylprednisolone taper.
On POD 1, the patient met criteria for extubation, including following commands and ongoing improving graft function. Later that day, she required reintubation for acute respiratory distress in the setting of flash pulmonary edema. The patient was also started on continuous renal replacement therapy (CRRT) for management of low urine output. She required high doses of pressors while on CRRT. Liver ultrasound showed resistivity indexes of 0.9, 0.7, and 0.7 for the common, right, and left hepatic arteries, respectively.
From POD 2–7, the patient remained intubated and failed multiple spontaneous breathing tests due to inadequate stamina. Her stamina improved, and she was successfully extubated on POD 8. However, despite stable respiratory status, the patient became progressively drowsy and weak. At this time, she was able to verbalize, and her mental status seemed to be at baseline. It was felt it was safe to transfer her out of the ICU, and the hope was that the transfer might help prevent delirium. Due to her history of re-intubation, intubation lasting over 48 hours, and weakness, the patient was evaluated by Speech and Language Pathologist (SLP), as is our standard practice. Evaluation by SLP deemed the patient at risk of aspiration. Therefore, the patient was kept nothing per orum (NPO), nasogastric tube was placed for medication and nutrition delivery. Thus, the patient continued on sublingual tacrolimus.
Downgraded to ACU
On POD 12, having been in the acute care and not intensive care unit overnight, the patient pulled out her nasogastric tube and had decreased mentation. On exam, she continued to appear weak. Her sleep quality worsened, and she began asking repetitive questions. The patient’s voice weakened, but she remained able to communicate.
At this point, her worsening mentation was attributed to hospital delirium. In an effort to reduce the delirium and improve sleep, her melatonin dose was increased from 5mg to 10mg, and she was placed on delirium precautions. To ensure the altered mental status was not due to infectious etiologies, cultures were obtained, and imaging was obtained, and they were all negative. Tacrolimus trough peaked at 12.0 (See Table 1).
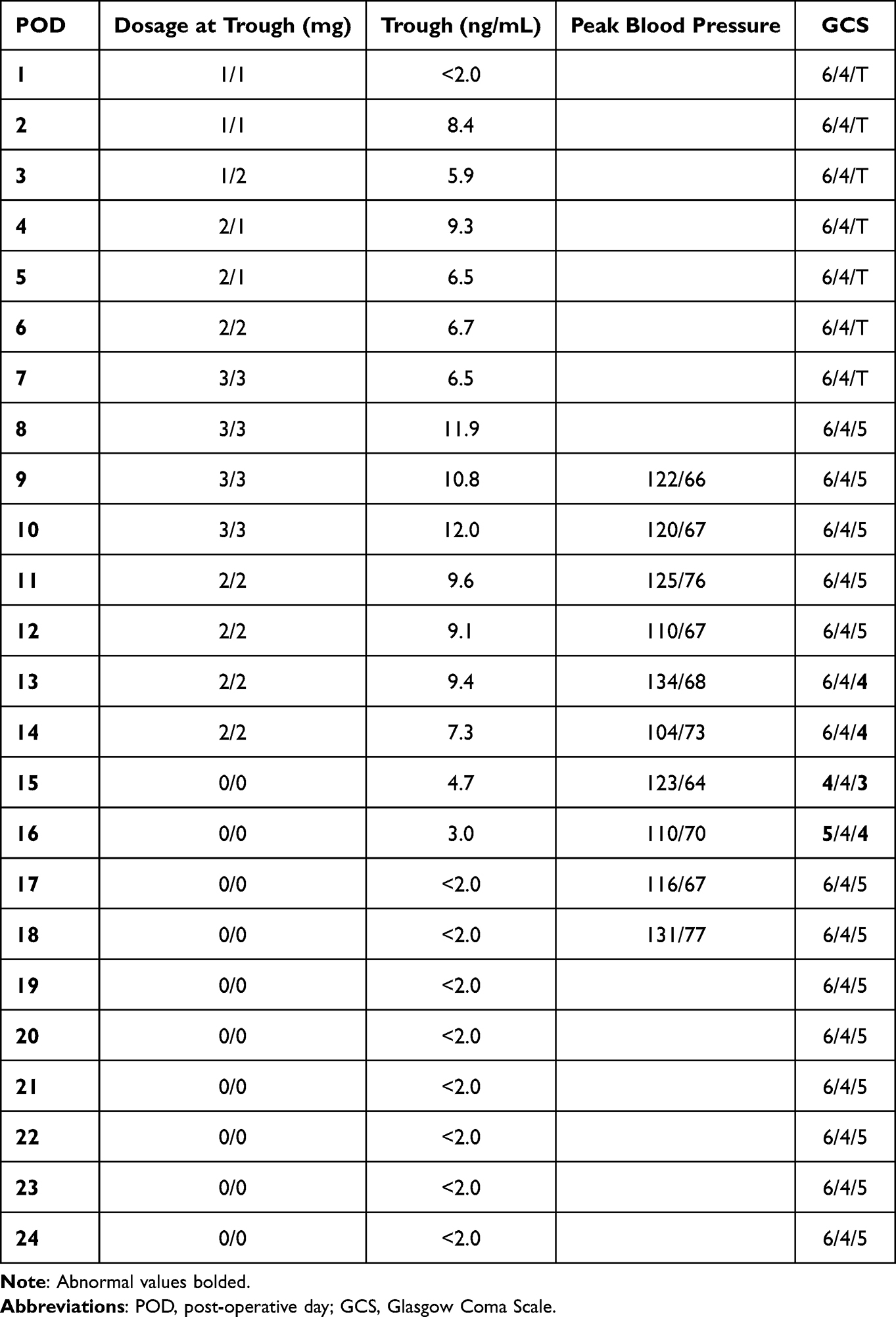 |
Table 1 Daily Tacrolimus Dosage and Corresponding Serum Troughs, Peak Blood Pressure, and Glasgow Coma Scale |
On POD 13, the patient appeared confused and disoriented, and perseverated. At this time, neurology was consulted and recommended obtaining an ammonia level which was within normal limits. The next morning (POD 14), the patient was completely unresponsive to voice and non-verbal. Her eyes were open but did not track. She exhibited diffuse tremors and was only responsive to painful stimuli.
Upgraded to ICU
Because of her worsening mental status, neurology was called urgently to see the patient. They noted continuous shaking of hands and feet with involvement of the tongue and lower jaw. EEG and stat head CT were negative. A decision was made not to obtain an MRI due to agitation. Blood pressure remained within normal limits.
The next morning (POD 15), the patient’s mentation was unchanged. Although her tacrolimus trough, head CT, and blood pressure were normal throughout progression of these neurological symptoms, a decision was made to discontinue tacrolimus at this time and monitor symptoms. The patient was subsequently started on cyclosporine.
On day 1 after discontinuing tacrolimus (POD 16), the patient had a lucid interval in the morning where she appeared more aware of her surroundings but was still unable to talk to the team.
On day 2 after discontinuing tacrolimus (POD 17), the patient’s mentation was markedly improved. She was able to fully communicate with the team, and her Glasgow Coma Scale improved from 11 to 15. She also passed a video fluoroscopy swallow study.
Downgraded to ACU
Within a week, the patient was able to advance her diet to solid food and speak in fully formed, coherent sentences. The patient subsequently recovered sufficiently to be discharged on POD 24 to an inpatient rehab facility. Graft function was preserved throughout her post-operative course.
Discussion
After tacrolimus was discontinued in favor of cyclosporine, the patient experienced total resolution of encephalopathy, dysphagia, dysarthria, and diffuse tremors, with majority improvement in the first 48 hours after tacrolimus was discontinued.
Dysphagia is a common post-operative manifestation in liver transplantation, cited in 20 of 50 patients in a small study.7 Dysphagia was associated with prolonged ICU stay and intubation, and with increased age. Prolonged intubation and extubation are potential contributing factors to the dysphagia in this case. However, the patient demonstrated little to no improvement until tacrolimus was discontinued, then demonstrated immediate resolution following discontinuation. This suggests that the dysphagia in this case was primarily due to tacrolimus toxicity.
Dysarthria was cited as a significant presenting symptom of sirolimus toxicity in one older study, presenting six months after liver transplantation in the setting of acute hepatitis C.8 There are no cases in the literature of acute post-operative calcineurin inhibitor toxicity presenting with dysarthria.
Throughout the hospital stay, multiple videofluoroscopic swallow studies were performed which identified oropharyngeal dysfunction. Of note, the patient had intact esophageal function below the level of the vocal cords. The dysfunction could be due to either encephalopathy or peripheral neuromuscular dysfunction; these cannot be differentiated without EMG studies.
PRES cannot be ruled out as a major mechanism of the acute encephalopathy and tremors. However, it does not explain the dysphagia and dysarthria as the only observed focal neurological deficits. Furthermore, there was no evidence of hypertension, headache, seizures, or CT findings. An MRI might have provided additional evidence of PRES, but it could not be obtained due to agitation.
Endothelial dysfunction may exist on a spectrum that includes PRES as a more serious manifestation of tacrolimus toxicity, with a mortality rate as high as 60% in the setting of stem cell transplantation.9 This patient may have presented in early stages of endothelial dysfunction before hemodynamic instability and vasogenic edema had evolved and thus the symptoms were relatively easy to reverse.
More likely, tacrolimus simultaneously effected neurotoxicity centrally causing encephalopathy and diffuse tremors and peripherally in the oropharynx. Although tacrolimus-induced peripheral neurotoxicity is usually less dramatic than PRES, it can cause significant manifestations that increase morbidity and adversely affect hospital course.
Conclusion
This is the first known case of dysphagia and dysarthria as major presenting symptoms of tacrolimus toxicity. Discontinuing tacrolimus in favor of cyclosporine can successfully resolve a constellation of neurotoxic symptoms that do not fit a classic picture of PRES.
Ethics and Consent
Informed consent including publication of the case was obtained in person from the patient. Institutional approval was required and was obtained from University Health Services, San Antonio. This work was designated by the Institutional Review Board of the University of Texas Health Science Center at San Antonio as non-research and exempt from review.
Acknowledgments
Special thanks to Jillian Woodworth, Manager of Research Operations at the UT Health San Antonio Transplant Institute. There was no funding for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tasdogan BE, Ma M, Simsek C, Saberi B, Gurakar A. Update on immunosuppression in liver transplantation. Euroasian J Hepatogastroenterol. 2019;9(2):96–101. doi:10.5005/jp-journals-10018-1301
2. McAlister VC, Haddad E, Renouf E, Malthaner RA, Kjaer MS, Gluud LL. Cyclosporin versus tacrolimus as primary immunosuppressant after liver transplantation: a meta-analysis. Am J Transplant. 2006;6(7):1578–1585. doi:10.1111/j.1600-6143
3. Araya AA, Tasnif Y. Tacrolimus:statpearls [internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from. https://www.ncbi.nlm.nih.gov/books/NBK544318/.
4. Fugate JE, Claassen DO, Cloft HJ, Kallmes DF, Kozak OS, Rabinstein AA. Posterior reversible encephalopathy syndrome: associated clinical and radiologic findings. Mayo Clin Proc. 2010;85(5):427–432. doi:10.4065/mcp.2009.0590
5. Anghel D, Tanasescu R, Campeanu A, Lupescu I, Podda G, Bajenaru O. Neurotoxicity of immunosuppressive therapies in organ transplantation. Maedica. 2013;8(2):170–175.
6. Schwartz RB, Jones KM, Kalina P, et al. Hypertensive encephalopathy: findings on CT, MR imaging, and SPECT imaging in 14 cases. AJR Am J Roentgenol. 1992;159(2):379–383. doi:10.2214/ajr.159.2.1632361
7. Mukdad L, Toppen W, Nguyen S, et al. A targeted swallow screen for the detection of postoperative dysphagia in liver transplant patients. Prog Transplant. 2019;29(1):4–10. doi:10.1177/1526924818817035
8. Belli LS, De Carlis L, Romani F, et al. Dysarthria and cerebellar ataxia: late occurrence of severe neurotoxicity in a liver transplant recipient. Transpl Int. 1993;6(3):176–178. doi:10.1007/BF00336365
9. Hammerstrom AE, Howell J, Gulbis A, Rondon G, Champlin RE, Popat U. Tacrolimus-associated posterior reversible encephalopathy syndrome in hematopoietic allogeneic stem cell transplantation. Am J Hematol. 2013;88:301–305. doi:10.1002/ajh.23402
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.