")
Back to Journals » Journal of Blood Medicine » Volume 12
A Third of Pregnant Women are Affected by Anemia in Eastern Ethiopia: A Facility-Based Study
Authors Debella A , Dheresa M , Geda B , Tiruye G , Fage SG
Received 12 February 2021
Accepted for publication 13 April 2021
Published 18 May 2021 Volume 2021:12 Pages 299—306
DOI https://doi.org/10.2147/JBM.S305567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Adera Debella,1 Merga Dheresa,1 Biftu Geda,2 Getahun Tiruye,1 Sagni Girma Fage1
1School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2Department of Nursing, College of Health and Medical Sciences, Meda Welabu University, Bale-Robe, Ethiopia
Correspondence: Sagni Girma Fage
School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, P.O. Box 235, Harar, Ethiopia
Email [email protected]
Background: Although it is a public health problem of pregnant women in low, middle and high-income countries, the highest prevalence rate of anemia is found among pregnant women of low-income countries, particularly in Africa. Therefore, this study has aimed to determine the magnitude of the anemia and its associated factors among pregnant women admitted to labor wards of public hospitals in eastern Ethiopia.
Methods and Materials: A health facility-based cross-sectional study was conducted among 405 pregnant women admitted to labor wards in four public hospitals of Harar town and Dire Dawa City Administration. A systematic random sampling technique was used to select the study participants. Data were collected through an interview using a structured questionnaire. The hemoglobin level was measured for each study participant. Binary and multivariable logistic regression models were fitted and statistical significance was declared at P< 0.05.
Results: The magnitude of anemia was 33.1% (95% CI: 28.4%, 37.8%). Being from rural areas (AOR: 3.8; 95% CI: 1.81, 7.94), no antenatal care (ANC) follow-up (AOR: 3.4; 95% CI: 1.34, 8.79), a habit of drinking milk with tea after meals (AOR: 2.8; 95% CI: 1.48, 5.61), taking a meal only 1– 2 times per day (AOR: 3.9; 95% CI: 1.69, 8.97), experiencing no blood loss in the current pregnancy (AOR: 0.25; 95% CI: 0.06, 0.96) and a habit of eating leafy vegetables (AOR: 0.12; 95% CI: 0.06, 0.24) were significantly associated with anemia.
Conclusion: About one in three pregnant women were anemic and anemia was a moderate public health problem in the study settings. Interventions targeting reducing or preventing anemia should focus on pregnant women in rural areas, promoting the benefits of ANC follow-up, reducing the habit of drinking milk with tea after meals, enhancing the consumption of leafy vegetables and increasing meal frequency per day to minimize or prevent anemia and its consequences during pregnancy.
Keywords: anemia, pregnant women, eastern Ethiopia
Introduction
Anemia – a pathologic state, in which the number of red blood cells or their oxygen carrying capacity is insufficient to meet physiologic needs – is a common medical problem during pregnancy. It is a global public health problem with major consequences for human health as well as socio-economic development.1
Among 1.62 billion globally anemic people, pregnant women constitute 41.8% and thus, anemia remains a significant public health problem. The highest prevalence rate (61.3%) is found among pregnant women from Africa.2 Rates of anemia are highest in low-income countries, especially in Central and West Africa (48% of reproductive-age women and 56% of pregnant women) and in South Asia (47% of reproductive-age women and 52% of pregnant women).3 Overall, in low and middle-income countries, 12% of low birth weight, 19% of preterm births and 18% of perinatal mortality were attributable to maternal anemia.4
Anemia is associated with morbidity and mortality of the growing fetus and neonates.5,6 It leads to premature births, low birth weight, fetal cognitive impairment and death.7–9 Similarly, maternal anemia increases the risk of preterm delivery and low birth weight, and iron-deficiency anemia underlies 115,000 maternal deaths and 591,000 perinatal deaths each year.3 Although anemia is a common problem of pregnant women in developing countries, pregnancy outcomes vary depending on the level of maternal hemoglobin.10
The Ethiopian Demographic and Health Survey (EDHS) showed that prevalence of anemia among women aged 15–49 years declined from 27% in 2005 to 17% in 2011, but increased to 24% in 2016 of which pregnant women account for 29%. But, due to different socio-economic status, behavioral, geographical and methodological differences, the national figures from the EDHS could not represent the prevalence of anemia among pregnant women in different parts of Ethiopia.11
Despite the government’s commitment and various stakeholders' interventions, the magnitude and the major risk factors of anemia remain unabated. Moreover, to the best knowledge of the investigators, there are few documented studies in eastern Ethiopia in general and no study on anemia among pregnant women in the study area. Therefore, this study has aimed to determine the magnitude of the anemia and its associated factors among pregnant women admitted to labor wards of public hospitals in eastern Ethiopia.
Methods and Materials
Study Design, Setting and Period
This hospital-based cross-sectional study was conducted from January 20 to February 19, 2018 in four public hospitals, of which one is a specialized university hospital, two are general hospitals and one is a primary hospital located at the Harari region and Dire Dawa City Administration in the eastern part of Ethiopia around 526 and 515 km from Addis Ababa respectively. The Harari region has a projected total population of 246,000 (124,000 males and 122,000 females), whereas the total population of Dire Dawa City Administration is projected to be 466,000 (234,000 males and 232,000 females).12 In all four hospitals, there were trained maternal health care providers.
Study Participants
All pregnant women admitted for delivery in those four public hospitals were the source population while women with singleton pregnancy selected by a systematic random sampling technique were the study population. Pregnant women with a past history of preterm delivery, who neither know LNMP nor had ultrasound diagnosis for gestational age, had pregnancy induced hypertension and multiple pregnancies, were excluded from the study.
Sample Size and Sampling Procedure
We calculated the sample size by using a single population proportion formula with the assumptions of Zα/2=1.96, 95% confidence level, 5% margin of error, the prevalence of anemia, p=39.1% from a study conducted in Woldia Hospital,13 12% for the non-response rate, and included 410 laboring mothers.
We first reviewed monthly clients’ flow to each hospital for delivery services in the previous six months from the registration book to estimate the expected number of women that could come for delivery in a month. Thus, the average numbers of women admitted for delivery per month in the previous six months were considered and the sample size 410 was then allocated to each hospital proportional to the total number of pregnant women expected to be admitted for delivery in each health facility in one-month period. A systematic random sampling technique was used to select the study participants and the first study subject for each hospital was randomly selected by a lottery method followed by enrolling every second woman.
Data Collection Tool and Procedure
The data were collected through an interview technique using a pretested structured questionnaire developed by reviewing the literature.13–20 The questionnaires comprised questions about socio-economic and demographic information, obstetric, health and lifestyle-related variables. Each woman was interviewed during the intrapartum period while she was relatively in stable condition. Eight midwives and four laboratory technicians collected the data after getting training on the tools and survey methods.
Measurements
To diagnose anemia, the hemoglobin level of the laboring mother was measured using a Hemocue HB 301 analyzer. A blood sample was collected through a finger prick by sterile lancet and dropped on a micro-cuvette for analysis. Hemoglobin was adjusted for altitude and smoking before deciding women’s status of anemia. To define anemia, WHO cut-off for hemoglobin values were used and hemoglobin <11 g/dL was considered as anemic while hemoglobin levels of 10–10.9 g/dL, 7–9.9 g/dL and <7 g/dL were considered as mild, moderate and severe anemia respectively.21
Data Quality Control
The questionnaire was initially prepared in English and translated to the local languages (Afaan Oromoo, Amharic and Somali). It was then translated back to English by language experts to check for its consistency. Training on the data collection tool and the procedures was provided to the data collectors and field supervisors. The questionnaire was pretested among 20 pregnant women in similar settings before the actual study. Regular supervision was done by experienced field research supervisors and the investigators.
Data Processing and Analysis
The collected data were checked for completeness, cleaned, coded and entered into EPI DATA version 3.1. Then, the data were exported to SPSS version 22 for analysis. Descriptive and summary statistics were done and the information was presented using tables and descriptive statements.
The outcome variable was recoded into binary as “anemia=1” and “no anemia=0”. A binary logistic regression model was fitted to check for association between independent variables and anemia. The model fitness was checked by Hosmer–Lemeshow statistics and Omnibus tests. All variables with p<0.25 in the bivariate analysis were included in the final multivariate analysis to identify the true predictors of anemia. A multi-collinearity test was carried out to check the presence of correlation between independent variables using the standard error and collinearity statistics. The direction and strength statistical association was measured by odds ratio (OR) along with the 95% confidence interval (CI). P value <0.05 was used to declare statistical significance.
Results
Socio-Economic and Demographic Characteristics
A total of 405 pregnant women participated in this study yielding a response rate of 98.8%. The mean (±SD) age of the study participants was 26.6 (±6.15) years. About half, 206 (50.9%) of the participants, were in the age group of 25–34 years. Three hundred and twenty-one (79.2%), 248 (61.2%) and 131 (32.3%) women were married, urban residents and unable to read and write respectively. The majority of the participants, 178 (44%), were housewives while only 19 (4.7%) were daily laborers in their occupation (Table 1).
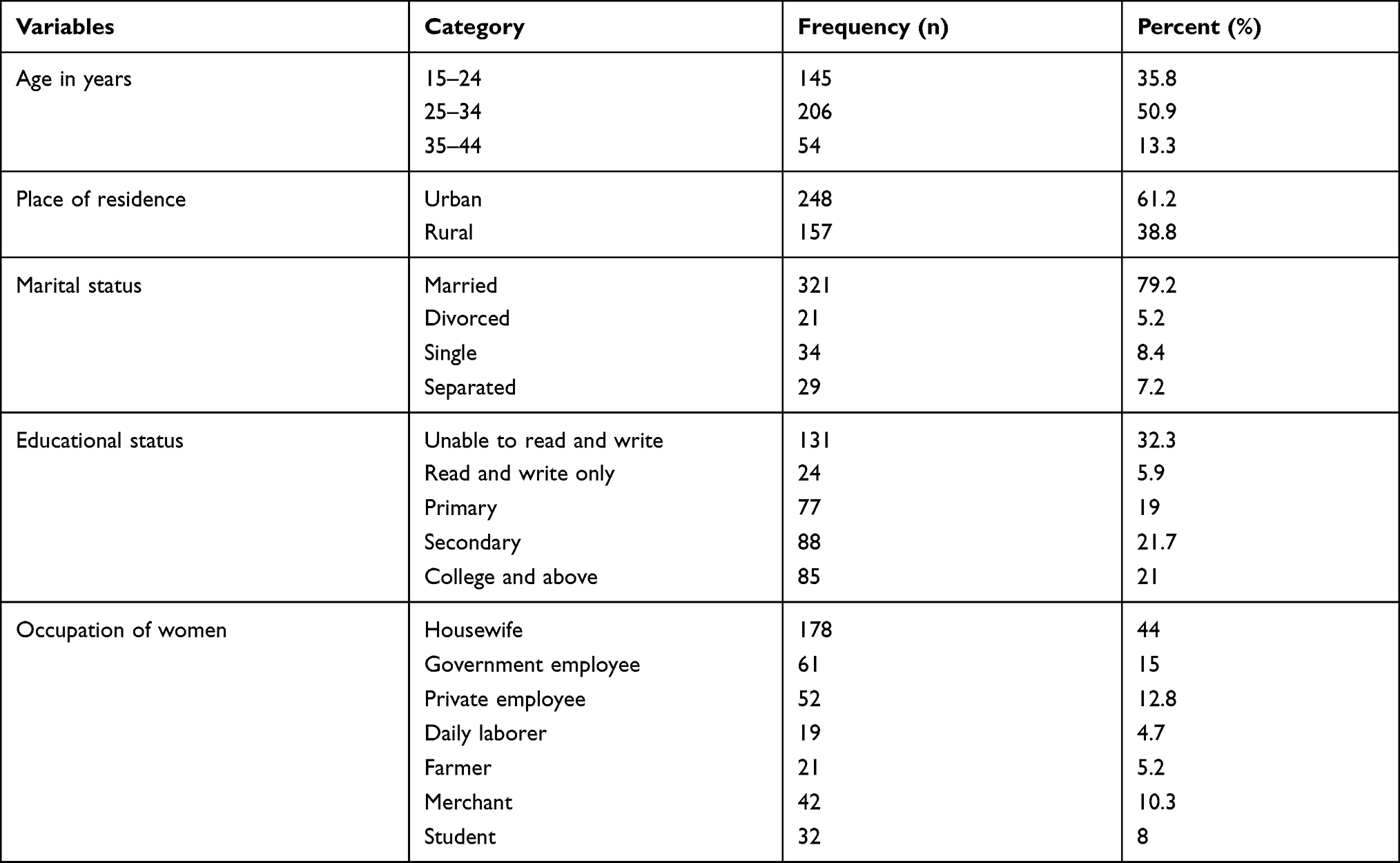 |
Table 1 Socio-Economic and Demographic Characteristics of Pregnant Women Admitted to Labor Wards of Public Hospitals in Eastern Ethiopia, 2018 (N=405) |
Obstetric, Health and Lifestyle of Participants
Of the total respondents, 327 (80.7%) had antenatal care (ANC) follow-up and half of them, 163 (40.2%), had less than four ANC visits. The majority of the women, 290 (71.6%), reported that they received iron/folic acid (IFA) in the current pregnancy. One hundred and eighty-two (44.9%) participants had history of contraceptive use and the birth interval between the current and the previous pregnancy was less than two years for 178 (44.0%) women. Among the participants, 38 (9.4%) had history of blood loss during the current pregnancy. Only 25 (6.2%) women reported having a habit of smoking cigarettes while food intake for the majority, 344 (84.9%), was three and above meals per day. About 33% of women reported that they have a habit of taking milk with tea after meals (Table 2).
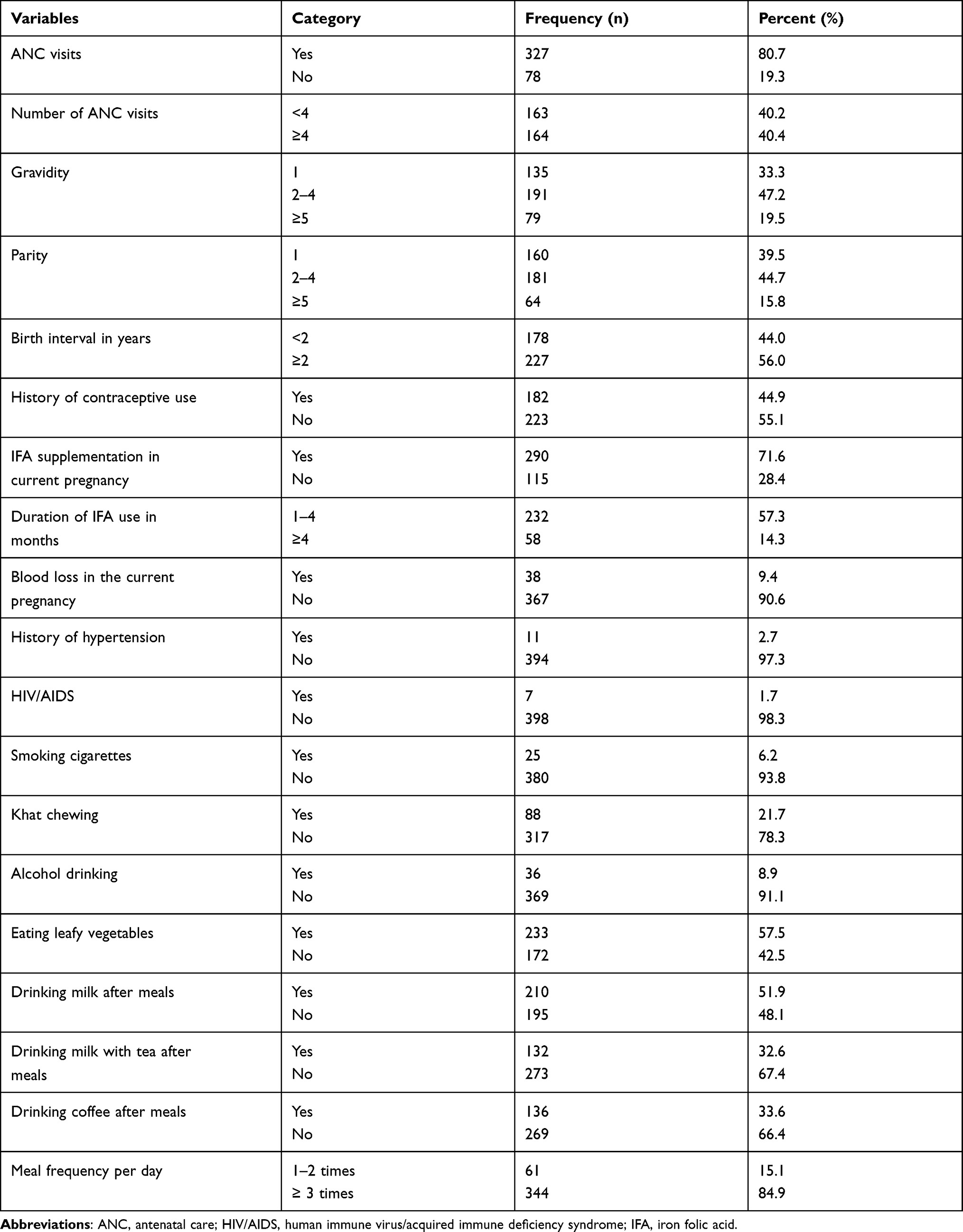 |
Table 2 Obstetric, Health and Lifestyle of Pregnant Women Admitted to Labor Wards of Public Hospitals in Eastern Ethiopia, 2018 (N=405) |
Anemia and Its Associated Factors
The overall magnitude of anemia was 33.1% (95% CI: 28.4–37.8%). Among the anemic women, 10 (2.5%), 58 (14.3%) and 66 (16.3%) had severe, moderate and mild anemia respectively.
In bivariate analysis, participants’ place of residence, marital status, ANC visit, birth interval, history of contraceptive use, IFA supplementation, blood loss in the current pregnancy, drinking alcohol, eating leafy vegetables, drinking milk with tea after meals and meal frequency per day were significantly associated with anemia among pregnant women. But, in the multivariable logistic regression, place of residence, ANC visit, blood loss in the current pregnancy, eating leafy vegetables, drinking milk with tea after meals and meal frequency per day were factors significantly associated with anemia.
Women who were from rural areas (AOR: 3.8; 95% CI: 1.81, 7.94), who had no ANC visit (AOR: 3.4; 95% CI: 1.34, 8.79), who had a habit of drinking milk with tea after meals (AOR: 2.8; 95% CI: 1.48, 5.61) and who had a meal frequency of 1–2 times per day (AOR: 3.9; 95% CI: 1.69, 8.97) were more likely to be anemic as compared to their counterparts. Pregnant women who did not experience blood loss in the current pregnancy were 75% less likely to be anemic (AOR: 0.25; 95% CI: 0.06, 0.96) and those who had a habit of eating leafy vegetables were 88% less likely to be anemic (AOR: 0.12; 95% CI: 0.06, 0.24) than their counterparts (Table 3).
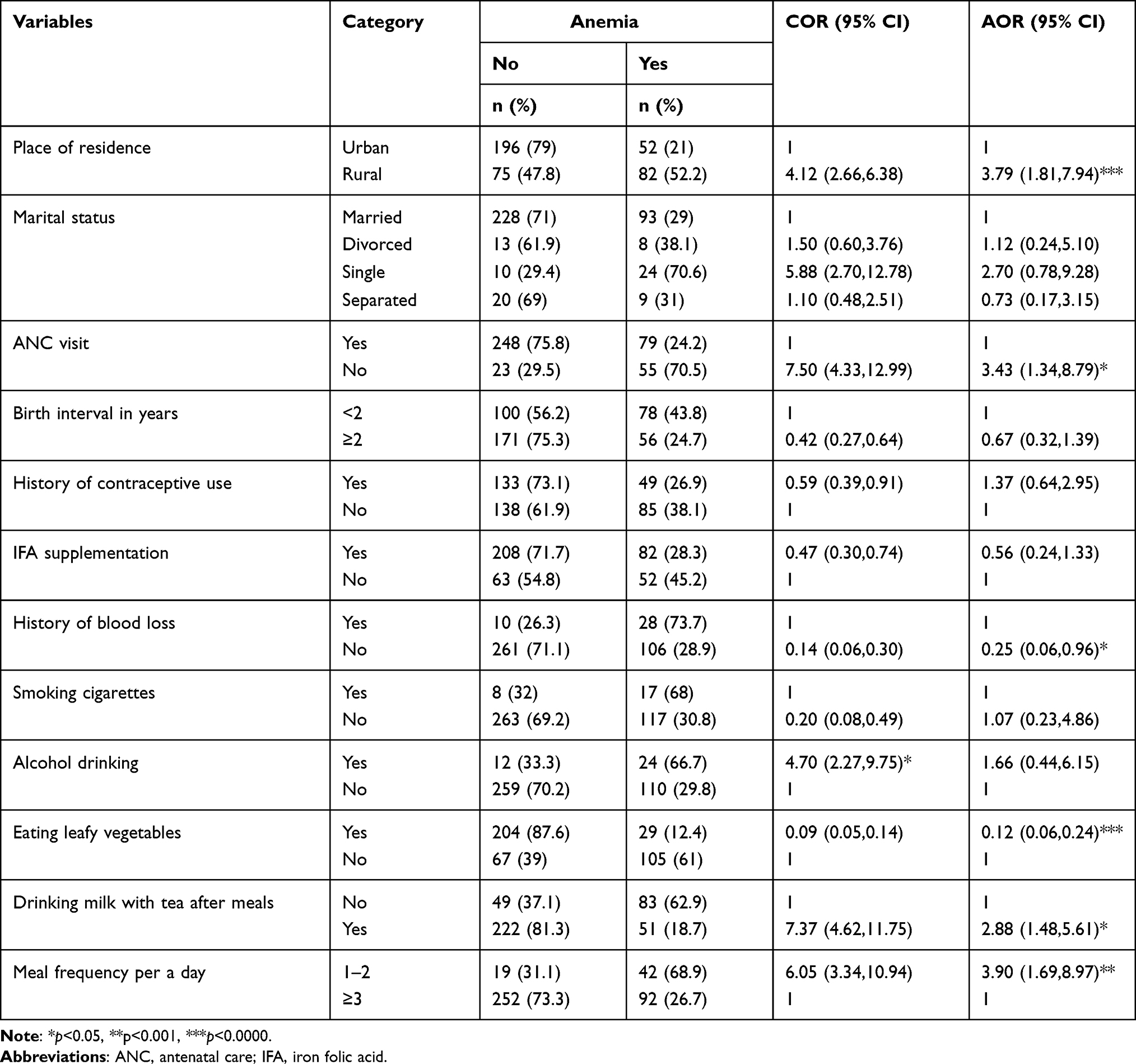 |
Table 3 Factors Associated with Anemia Among Pregnant Women Admitted to Labor Wards of Public Hospitals in Eastern Ethiopia, 2018 (N=405) |
Discussion
This study assessed the magnitude of anemia among pregnant women admitted to labor wards of four public hospitals in eastern Ethiopia. It revealed that about one in three pregnant women were anemic. Women from rural areas, who had no ANC visit, who had a habit of drinking milk with tea after meals and who had meal frequency of 1–2 times per day were more likely to be anemic than their counterparts. Pregnant women who did not experience blood loss in their current pregnancy and who had a habit of eating leafy vegetables were less likely to be anemic.
In this study, the magnitude of anemia among pregnant women is in harmony with findings from similar studies in Arba Minch,17 northwest Tigray20 and Shalla-West Arsi.22 However, it is higher than reports of other previous studies.15,18,23–28 On the contrary, the current magnitude is lower than similar previous studies.13,14,19,29,30 These differences might be due to variations in the socio-economic characteristics, study settings and periods, dietary habits and health seeking behaviors across the towns with a community of relatively different lifestyle, feeding practices and social norms.
Pregnant women who lived in rural areas were more likely to be anemic as compared to those who lived in urban areas. This is in line with the study from Tigray.20 The possible reason for this higher burden of anemia among pregnant women from rural areas could be related to inaccessibility of health care facilities and/or low health seeking behavior of the rural women, lack of information about causes of anemia, as well as accessibility and affordability of possible methods to prevent the risk factors of anemia. Additionally, women who had no ANC follow-up were more likely to be anemic than their counterparts. This result is consistent with previous findings.18 This might be due to the fact that pregnant women who attend ANC follow-up are counseled about appropriate feeding practices and supported by the maternity care providers to take IFA supplementation to prevent or reduce the occurrence of anemia.
Furthermore, pregnant women who have a habit of drinking milk with tea after meals had higher likelihood of getting anemia than those who did not have such habit. This is similar to findings from a study in Addis Ababa18 and this might be due to the inhibition effect of tea and calcium on iron absorption resulting in low bioavailability of iron.31–34 The risk of anemia was higher among pregnant women who had a meal frequency of 1–2 times per day than those who had three or more times. This is in line with the finding from Tigray20,28 and it might be because taking meals frequently helps to meet the increased demands for nutrients during pregnancy.
On the other hand, pregnant women who did not experience blood loss in the current pregnancy were 75% less likely to be anemic. This might be because blood loss would result in lower circulating serum iron with lower hemoglobin level. Similarly, women who had a habit of eating leafy vegetables were 88% less likely to experience anemia than those who did not. The possible reason for this might be feeding on different leafy vegetables could increase the folate/folic acid levels that are important to produce normal cells including red blood cells that aids in increasing the availability of hemoglobin.
We used standardized medical equipment and procedures to measure anemia. But, variables such as meal frequency and other lifestyle factors were prone to social desirability bias. In addition, the study was cross-sectional study and could not establish cause and effect relationship between anemia and the associated factors.
Conclusion
This study indicated that about one in three pregnant women were anemic and anemia was a moderate public health problem in the study settings. Interventions targeting reduction or prevention of anemia should focus on pregnant women in rural areas, promoting the use of ANC visits, reducing the habit of drinking milk with tea after meals, encouraging the consumption of leafy vegetables and increasing meal frequency per day to minimize the risk of anemia and its consequences.
Data Sharing Statement
The data sets used for this study are available from the corresponding author on reasonable request.
Ethical Approval
Ethical approval was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Haramaya University, College of Health and Medical Sciences. Support letters from the College of Health and Medical Sciences were submitted to the selected hospitals where the study was conducted. After getting all permission letters from the responsible body, an informed voluntary written consent was signed by study participants. For study participants under the age of 18 years, we got informed written consent from parents or family before the data collection. Confidentiality was maintained by using codes instead of participant’s name. Participants were also informed that they have full right to refuse participation or withdraw at any time from the research. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgment
The authors are very thankful to Haramaya University, heads and staff of the selected hospitals, the study participants, data collectors and field supervisors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Haramaya University provided the financial supports for this study. But, the funding body had no role in the collection, analysis and interpretation of the data as well as the write up and publication of this article.
Disclosure
The authors have no competing interests to declare in this work.
References
1. WHO (World Health Organization). The global prevalence of anaemia in 2011; 2015.
2. WHO (World Health Organization). Worldwide prevalence of anaemia 1993–2005. WHO global database on anaemia; 2008.
3. Stevens GA, Finucane MM, De-Regil LM, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Glob Health. 2013;1(1):e16–e25. doi:10.1016/S2214-109X(13)70001-9
4. Rahman M, Abe SK, Rahman S, et al. Maternal anemia and risk of adverse birth and health outcomes in low-and middle-income countries: systematic review and meta-analysis, 2. Am J Clin Nutr. 2016;103(2):495–504. doi:10.3945/ajcn.115.107896
5. Van DB, Nynke R, Letsky EA. Etiology of anemia in pregnancy in South Malawi. Am J Clin Nutr. 2000;72(1):247S–256S.
6. Crawley J. Reducing the burden of anemia in infants and young children in malaria-endemic countries of Africa: from evidence to action. Am J Trop Med Hyg. 2004;71(2_suppl):25–34. doi:10.4269/ajtmh.2004.71.25
7. Banhidy F, Acs N, Puho EH, et al. Iron deficiency anemia: pregnancy outcomes with or without iron supplementation. Nutrition. 2011;27(1):65–72. doi:10.1016/j.nut.2009.12.005
8. Kalaivani K. Prevalence & consequences of anaemia in pregnancy. Indian J Med Res. 2009;130(5):627–633.
9. Levy A, Fraser D, Katz M, et al. Maternal anemia during pregnancy is an independent risk factor for low birthweight and preterm delivery. Eur J Obstet Gynecol Reprod Biol. 2005;122(2):182–186. doi:10.1016/j.ejogrb.2005.02.015
10. Chang S, Zeng L, Brouwer ID, et al. Effect of iron deficiency anemia in pregnancy on child mental development in rural China. Pediatrics. 2013;131(3):e755–e763. doi:10.1542/peds.2011-3513
11. CSA-Ethiopia, I.C.F. International. Ethiopia Demographic and Health Survey 2016: Key Indicators Report. USA: CSA and ICF; 2016.
12. CSA. Population Projection of Ethiopia for All Regions at Wereda Level from 2014–2017. Addis Ababa: CSA; 2013.
13. Brhanie T, Sisay H. Prevalence of iron deficiency anemia and determinants among pregnant women attending antenatal care at Woldia Hospital, Ethiopia. J Nutr Dis Ther. 2016;6(4).
14. Getachew M, Yewhalaw D, Tafess K, et al. Anaemia and associated risk factors among pregnant women in Gilgel Gibe dam area, Southwest Ethiopia. Parasit Vectors. 2012;5(1):296. doi:10.1186/1756-3305-5-296
15. Getahun W, Belachew T, Wolide AD. Burden and associated factors of anemia among pregnant women attending antenatal care in southern Ethiopia: cross sectional study. BMC Res Notes. 2017;10(1):276. doi:10.1186/s13104-017-2605-x
16. Gupta A. Prevalence of maternal anemia and its impact on perinatal outcome in a rural area of Dakshina Kannada. Int J Med Sci Public Health. 2017;6(7):1209–1214. doi:10.5455/ijmsph.2017.0410803052017
17. Bekele A, Tilahun M, Mekuria A. Prevalence of anemia and its associated factors among pregnant women attending antenatal care in health institutions of Arba Minch town, Gamo Gofa Zone, Ethiopia: a Cross-sectional study. Anemia. 2016;2016:1–9. doi:10.1155/2016/1073192
18. Jufar AH, Zewde T. Prevalence of anemia among pregnant women attending antenatal care at tikur anbessa specialized hospital, Addis Ababa Ethiopia. J Hematol Thromboembolic Dis. 2014.
19. Addis AK, Mohamed DA. Prevalence of anemia and associated factors among pregnant women in an urban area of Eastern Ethiopia. Anemia. 2014.
20. Gebre A, Mulugeta A. Prevalence of anemia and associated factors among pregnant women in North Western zone of Tigray, Northern Ethiopia: a cross-sectional study. J Nutr Metab. 2015;2015:1–7. doi:10.1155/2015/165430
21. WHO (World Health Organization). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System; 2011. NMH/NHD/MNM/11.1. Available from: https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?sequence=22&isAllowed=y. Geneva, Switzerland.
22. Obse N, Mossie A, Gobena T. Magnitude of anemia and associated risk factors among pregnant women attending antenatal care in Shalla Woreda, West Arsi Zone, Oromia Region, Ethiopia. Ethiop J Health Sci. 2013;23((2):):165–173.
23. Alem M, Enawgaw B, Gelaw A, et al., Prevalence of anemia and associated risk factors among pregnant women attending antenatal care in Azezo Health Center Gondar town, Northwest Ethiopia. J Interdiscip Histopathol.2013.
24. Walelign F, Gariba E, Roba K. Prevalence of Anemia and associated factors among pregnant women in Ethiopia. Food Sci Nutri Res. 2018;1(1).
25. Berhe B, Mardu F, Legese H, et al. Prevalence of anemia and associated factors among pregnant women in Adigrat General Hospital, Tigrai, northern Ethiopia, 2018. BMC Res Notes. 2019;12(1):310. doi:10.1186/s13104-019-4347-4
26. Kitila KT, Tulu BL, Bedaso DG, Negwo DT, Gemeda MN. Prevalence of anemia and associated risk factors among pregnant women attending antenatal care in selected health centers in Addis Ababa, Ethiopia. J Womens Health Care. 2018;7(443):
27. Geleta W, Babure Z. Anemia and its determinant factors among pregnant women in Ebantu District, East Wollega zone, Ethiopia. J Womens Health Care. 2020;9(490):2167–2420.
28. Abriha A, Yesuf ME, Wassie MM. Prevalence and associated factors of anemia among pregnant women of Mekelle town: a cross sectional study. BMC Res Notes. 2014;7(1):888. doi:10.1186/1756-0500-7-888
29. Bereka SG, Gudeta AN, Reta MA, Ayana LA. Prevalence and associated risk factors of anemia among pregnant women in rural part of JigJiga City, Eastern Ethiopia: a cross sectional study. J Preg Child Health. 2017;4((337):):2.
30. Gedefaw L, Ayele A, Asres Y, Mossie A. Anaemia and associated factors among pregnant women attending antenatal care clinic in Walayita Sodo town, Southern Ethiopia. Ethiop J Health Sci. 2015;25(2):155–164. doi:10.4314/ejhs.v25i2.8
31. Disler P, Lynch SR, Charlton RW, et al. The effect of tea on iron absorption. Gut. 1975;16(3):193–200. doi:10.1136/gut.16.3.193
32. Fan FS. Iron deficiency anemia due to excessive green tea drinking. Clin Case Rep. 2016;4(11):1053. doi:10.1002/ccr3.707
33. Nelson M, Poulter J. Impact of tea drinking on iron status in the UK: a review. Journal of Hum Nut Dietetics. 2004;17(1):43–54. doi:10.1046/j.1365-277X.2003.00497.x
34. Lönnerdal B. Calcium and iron absorption - mechanisms and public health relevance. Int J Vitam Nutr Res. 2010;80(45):293–299. doi:10.1024/0300-9831/a000036
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.