")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
A Theoretically Informed Approach to Support the Implementation of Pre-Operative Anemia and Iron Deficiency Screening, Evaluation, and Management Pathways: Protocol for a Type Two Hybrid-Effectiveness Study
Authors Delaforce A , Duff J , Munday J , Farmer S, Miller K , Glover L, Corney C, Hurst C , Ansell G, Gutta N, Tuffaha H, Hardy J
Received 31 March 2021
Accepted for publication 16 April 2021
Published 6 May 2021 Volume 2021:14 Pages 1037—1044
DOI https://doi.org/10.2147/JMDH.S313309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alana Delaforce,1– 3 Jed Duff,1,4 Judy Munday,3– 5 Shannon Farmer,6,7 Kristin Miller,2 Lynne Glover,2 Christopher Corney,2 Cameron Hurst,8 Gareth Ansell,2,9 Naadir Gutta,2,9 Haitham Tuffaha,10 Janet Hardy2,3
1School of Nursing and Midwifery, The University of Newcastle, Callaghan, NSW, Australia; 2Mater Health Services, South Brisbane, QLD, Australia; 3Mater Research Institute-UQ, South Brisbane, QLD, Australia; 4Centre for Healthcare Transformation/School of Nursing, Queensland University of Technology, Kelvin Grove, QLD, Australia; 5Faculty of Health and Sport Science, The University of Agder, Kristiansand, Norway; 6Department of Haematology, Royal Perth Hospital, Perth, Western Australia, Australia; 7Medical School and Division of Surgery, The University of Western Australia, Perth, Western Australia, Australia; 8QIMR Berghoffer Medical Research Institute, Brisbane, QLD, Australia; 9School of Clinical Medicine - Mater Clinical Unit, The University of Queensland, St Lucia, QLD, Australia; 10Centre for the Business and Economics of Health, The University of Queensland, St Lucia, QLD, Australia
Correspondence: Alana Delaforce Level 6, Duncombe Building, Mater Hospital Brisbane, South Brisbane, QLD, 4101, Australia
Tel +61 7 3163 2853
Email [email protected]
Introduction: Blood transfusions are a risk factor for increased morbidity, mortality, and length of hospital stay. Patient blood management guidelines provide guidance to reduce risk and improve patient outcomes. They outline steps to help prevent transfusions and considerations for when deciding to transfuse. One recommendation to prevent unnecessary transfusion is to optimize patients using Pre-operative Anemia and Iron Deficiency Screening, Evaluation and Management Pathways (PAIDSEM-P). The uptake of these recommendations is highly variable, and an effective approach to implementing them in a tailored and context-specific manner remains elusive.
Method and Design: A mixed-methods, interventional study, using a type two-hybrid effectiveness-implementation design, will evaluate the impact of a change package to improve the uptake of PAIDSEM-P. The change package consists of the intervention (PAIDSEM-P) supported by theoretically informed implementation strategies. Pre- and post-implementation, retrospective health record reviews will determine the effect of the change package on provider outcomes, including compliance with guideline recommendations as measured by the proportion of patients who have the appropriate tests performed, and, if required, appropriate treatment and/or referrals. Patient outcomes will be measured by checking for any difference in the proportion of patients with anemia on the day of surgery and the proportion of patients who receive a blood transfusion during the peri-operative period. An economic evaluation will be conducted to compare health outcomes and costs. The feasibility, acceptability and appropriateness of the PAIDSEM-P will be assessed using a quantitative, validated survey to measure implementation outcomes.
Discussion: Testing of implementation theory is required to advance understanding of what works, in what context, and the impact on implementation success. This study aims to evaluate the impact of a theoretically informed change package on improving the uptake of PAIDSEM-P. If successful, it will also provide a framework for health care facilities to follow when addressing other evidence-practice gaps.
Keywords: patient blood management, implementation, anemia, iron deficiency, surgery
Introduction
Blood transfusions present an increased risk of mortality, infection and coagulopathy, and should be avoided where possible.1–3 Patient Blood Management (PBM) guidelines provide support to clinicians when considering treatment options for preserving and managing a patient’s own blood and guidance when transfusion is a treatment option.4–7 The guidelines consider three fundamental principles, or “pillars”: the maximization of a patient’s red cell mass before invasive procedures, the minimization of iatrogenic and coagulopathic blood losses, and that patients are supported to tolerate anemia in the short term rather than automatically resorting to red blood cell transfusion.8,9 When implemented effectively, the guidelines can significantly improve patient care, health outcomes and reduce costs.8,10–12
Pillar one, which focuses on the maximization of a patient’s red cell mass recommends that elective surgical patients at risk of losing >500 mL of blood are screened and treated according to Preoperative Anemia and Iron Deficiency Screening, Evaluation and Management Pathways (PAIDSEM-P).7 Multiple models are used to deliver PAIDSEM-P in Australia and internationally. Some examples include the minimal staffing model (whereby anesthetists take carriage of the screening and treatment),13 the introduction of staff whose role is specifically to screen and refer anemic or iron deficient patients for treatment,14 the inclusion of the screening and treatment into the existing preadmission team responsibilities,15 and finally, creation of a hybrid model where a nurse oversees and manages the pre-operative anemia and iron deficiency screening and treatment.16 The success of these models remains highly variable, and it is unclear how facilities can best support this intervention.
Implementation strategies that support the uptake of PADISEM-P are reported in the literature. However, it is unclear how and why they are selected, and the language describing them is highly variable.8 Implementation strategies previously used to improve uptake of PAIDSEM-P include local consensus processes, audit and feedback, providing education, and identifying and preparing champions.17,18 A systematic review found that behavioral implementation strategies reduced blood product utilization, but due to heterogeneity across studies, no specific recommendations as to which are more effective than others could be made.19 Another review noted that many studies inadequately report the process of implementation.20 These difficulties are not unique to PAIDSEM-P implementation. Much research has been undertaken to improve evidence translation into clinical practice through the development of theoretical frameworks to support implementation strategy selection.21,22
This study uses a theoretically informed change package that consists of an intervention and supporting implementation strategies.23 The intervention is the implementation of a Preoperative Anemia and Iron Deficiency Screening, Evaluation and Management Pathway (PAIDSEM-P), delivered by a Pre-operative Anemia Care Coordinator (PACC). This intervention will be supported by implementation strategies that were selected in a previously reported study. The study identified barriers using the Consolidated Framework for Implementation Research (CFIR), which were then mapped to the Expert Recommendations for Implementing Change (ERIC) framework.23–25
Method and Design
Aim
To test the effectiveness, feasibility, appropriateness, and acceptability of a change package (consisting of the intervention (PAIDSEM-P) supported by theoretically informed implementation strategies).
Design
A mixed-methods, interventional study, using a type two-hybrid effectiveness-implementation design.26 Type two-hybrid effectiveness designs evaluate both the effect of an intervention and the implementation strategies that support it.26 They are appropriate when utilizing interventions that have been proven to be effective but require further investigation regarding the context and implementation strategies that best support delivery.26 A pre- and post-implementation retrospective health record review will be undertaken to determine effectiveness and a validated survey will be used to measure acceptability, appropriateness and feasibility.27
Setting: The study will be undertaken in a large, metropolitan, tertiary referral hospital that provides services for public and privately insured patients over a wide range of specialties. For this study, the focus is on public patients only. Approximately 1400 major surgeries (eligible for the PAIDSEM-P) are undertaken annually in this public facility. A Pre-operative Anemia Care Coordinator (PACC) will deliver the intervention, overseen by an implementation facilitator.
Ethics: Ethical approval was granted by the Mater Misericordiae Ltd Human Research Ethics Committee (HREC), and administrative approval from the University of Newcastle HREC (reference: AM/MML/47826) in accordance with the Declaration of Helsinki. The screening tests outlined in the PAIDSEM-P occur in the scope of hospital policy. Any treatment that arises as a consequence will be provided in the setting of fully informed consent – eg, where intravenous iron is required.28 A waiver of consent has been granted for the collection of deidentified data to be obtained from retrospective medical chart reviews. All survey participants will be provided with a participant information and consent form prior to entering the survey.
Funding: Funding for this study has been provided by the Mater Research Foundation.
Change Package
The Intervention
The intervention is a Preoperative Anemia and Iron Deficiency Screening, Evaluation and Management Pathway (PAIDSEM-P) delivered by a Pre-operative Anemia Care Coordinator (PACC) (Figure 1). The intervention is described in Table 1 using the Template for Intervention Description and Replication (TIDieR) checklist.29 The checklist enables standardized reporting of intervention components to enhance replicability.29 Detailed information about the intervention delivery is outlined in Table 2.
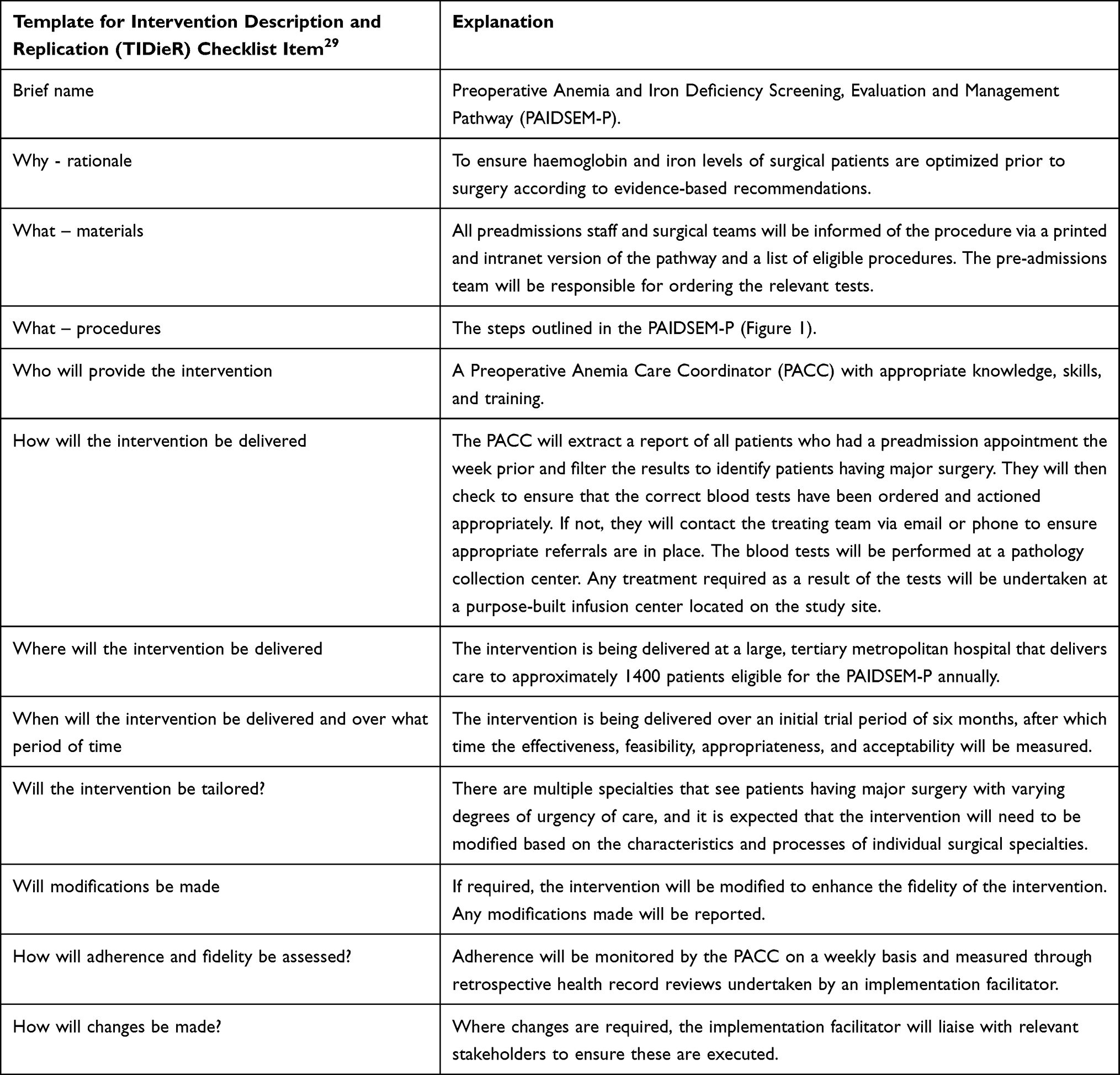 |
Table 1 Detailed Intervention Description |
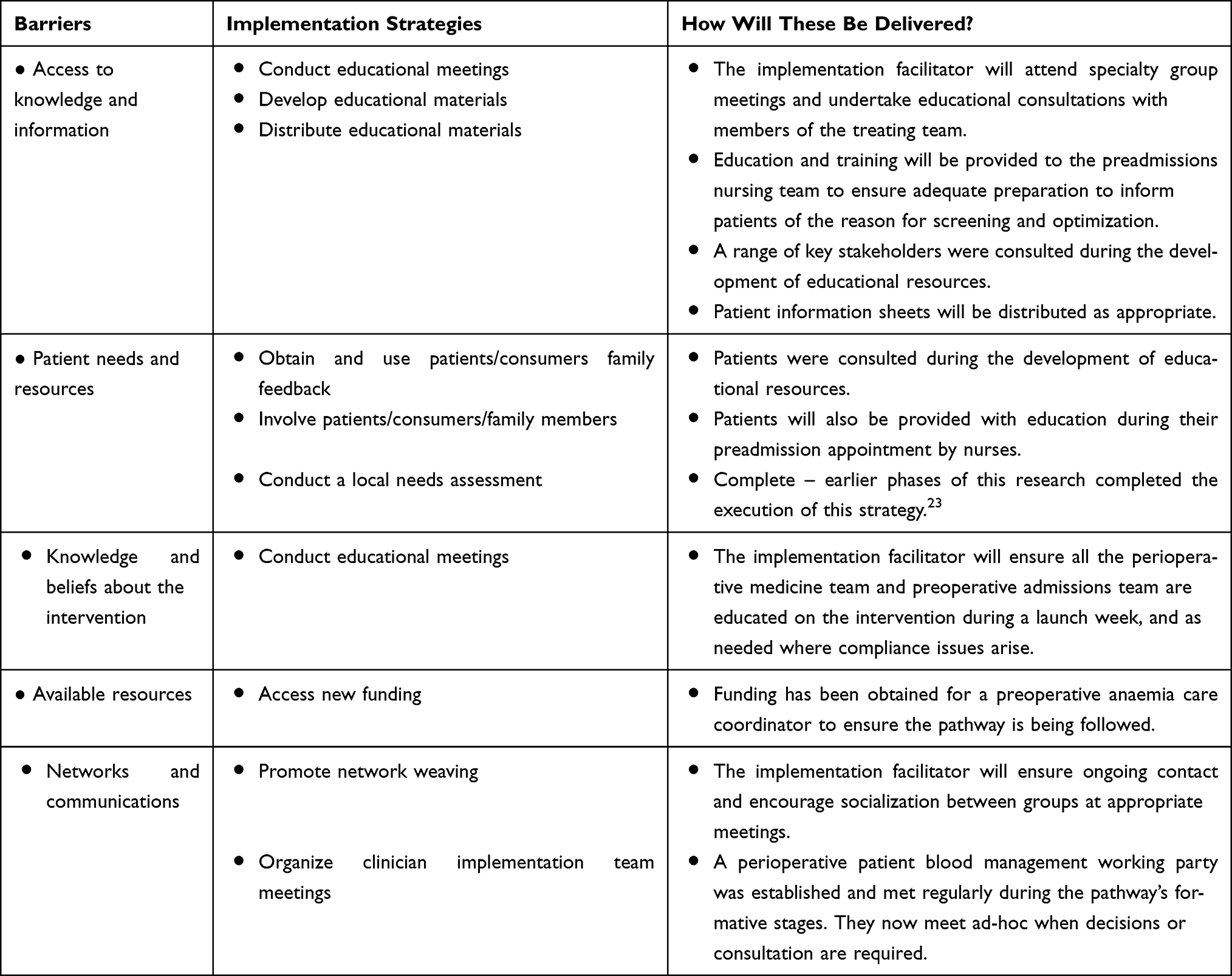 |
Table 2 Barriers, Implementation Strategies and Method of Delivery |
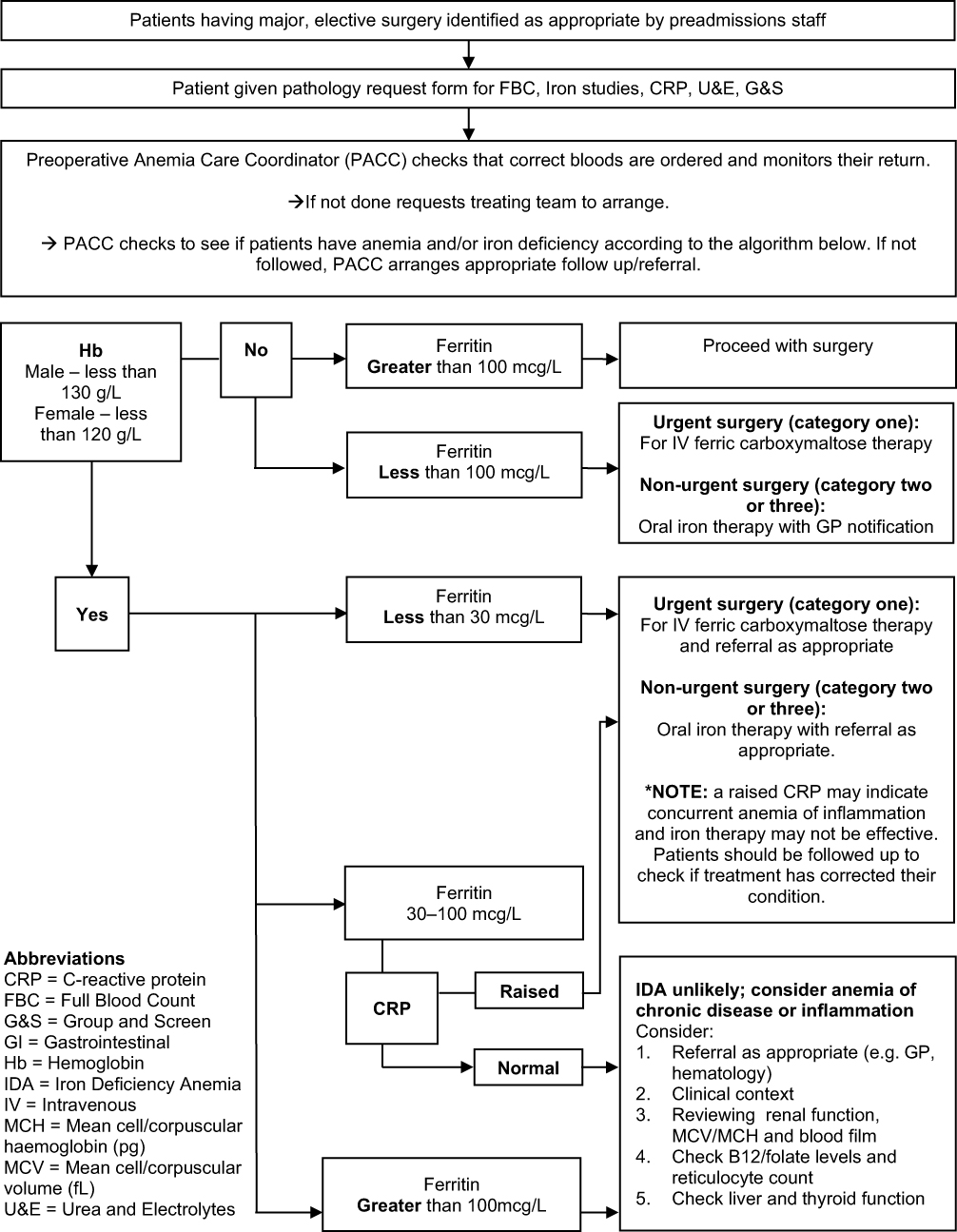 |
Figure 1 Pre-operative Anemia and Iron Deficiency Screening, Evaluation and Management Pathway (PAIDSEM-P) and Preoperative Anemia Care Coordinator (PACC) steps. |
Implementation Strategies
The intervention delivery will be further supported using theoretically informed implementation strategies selected based on results from a previously described qualitative investigation.23 The summarised results and delivery of the implementation strategies are outlined in Table 2, below:
Outcomes
The impact of this study will be measured at the provider, patient and health service levels.
- Provider outcomes are compliance with the National Blood Authority Patient Blood Management Guidelines7 which will be measured by the proportion of patients that receive recommended care including the performance of appropriate tests and provision of appropriate treatment and/or referral.
- Patient outcomes include the proportion of patients who are anemic on the day of surgery defined by World Health Organization haemoglobin levels (males <130g/L, females <120g/L);30–35 and, the proportion of patients who receive a blood transfusion during the peri-operative period.7,20,36
- An economic evaluation will be conducted to compare the costs and effects of the program to the health service.
- Implementation outcomes will measure the acceptability, appropriateness and feasibility of the PAIDSEM-P.27
Data Collection and Analysis
Retrospective Health Record Review
Using the pilot tested data collection tool in Supplementary File 1, a before and after implementation health record review will be conducted using hospital administrative data to identify a random sample of patients eligible for inclusion. Patients eligible for inclusion must be aged 18 years or older, and have undergone elective, major surgery where there was a risk of blood loss >500mL (see Supplementary File 1 for list of surgeries). Revision surgeries are excluded. Assuming a baseline (pre-implementation) level of compliance of 5% during sample size calculations, 400 patients (200 pre and 200 post implementation) are needed to detect a 20% absolute improvement in compliance (ie, Post-stage compliance of 25%).31,32 Data will be described using means and standard deviations, for continuous variables, and counts and percentages, for categorical data. Statistical analysis for the patient outcomes (proportion of patients anemic on the day of surgery, and proportion of patients who receive a blood transfusion during the peri-operative period) will involve using binary logistic regression. We will investigate whether there may be other differences in the pre-and post-populations, which will be controlled for using stratified propensity score analysis. General linear modelling will be utilized for the other continuous outcomes and logistic regression methods for categorical outcomes. All analysis will be conducted using the R statistical package, and propensity score analysis will be performed using the R library Matching.
Economic Analysis
A cost-effectiveness analysis will be undertaken from a health payer perspective using data from the retrospective health record reviews. We will also access general hospital administrative data through a formal request to quantify and value health resources consumed including medications, pathology tests, transfusions and other resources required to manage complications. We will also include the cost of delivering the project using this method (costs associated with a project coordinator) using the incremental cost effectiveness ratio, which is the difference in cost divided by the difference in effects with and without the PADISEM-P. A health economist (HT) will oversee the analysis process.
Survey
A range of multidisciplinary, peri-operative team members will be invited to participate in a survey measuring acceptability, appropriateness, and feasibility of the change package. Invitations will be made verbally or through individual email after the study has been running for six months. The online survey will be administered through REDCapR and is based on an existing validated tool27 (see Supplementary File 2), with additional space for qualitative responses. The survey form has been pilot tested for content and face validity by three research team members. All participants will be presented with a participant information sheet and informed that completion of the survey confirms consent. Following agreement to participate reminder emails will be sent at one, two, and four-week intervals unless sufficient responses are received prior. Analysis of categorical data will use a descriptive statistical analysis, including counts and percentages. For qualitative data, a thematic analysis will be conducted using an iterative approach, as described by Braun and Clarke.37 Free text data will be analyzed and coded with recurring themes. All coded data will be sent to at least two other authors to check for agreement. Where disagreement occurs, it will be resolved by consensus.
Discussion
Consensus among experts that pre-operative anemia should be identified and addressed before elective surgery has been in existence since 2005.38 Since that time, multiple studies have shown that pre-operative anemia and/or iron deficiency is an independent risk factor for blood transfusion, increased length of stay and increased risk of blood transfusion.7,39,40 Based on the results of these studies, patient blood management guidelines have been developed that recommend the implementation of PAIDSEM-P.5,7,41 Despite evidence to support the implementation, there remains high variability in the uptake of PAIDSEM-P.20 A systematic review previously undertaken by the study authors revealed that there is high variability in the approaches used for the implementation of PAIDSEM-P, which are also poorly described and do not appear to leverage available theoretical frameworks.20
Thorough reporting of theoretical frameworks may help improve the uptake of PAIDSEM-P and assist in addressing other evidence-practice gaps. A cluster randomized controlled trial that sought to evaluate the use of the Capability, Opportunity, Motivation, Behavior (COM-B) and the behavior change wheel, on reducing sitting time in the workplace demonstrated a significant result when using this approach (−83.28 min/workday, 95% CI −116.57 to −49.98 (in favor of the intervention group).41 Studies such as this demonstrate the impact of theoretically informed approaches on achieving change. This study will be the first (to the author’s knowledge) to use an approach informed by the CFIR and ERIC frameworks, and apply a theoretical approach in the context of PAIDSEM-P implementation.
Implications for Practice
If this study is successful, there is potential for replication of the model, which includes barrier identification, strategy mapping and utilization of tailored implementation strategies.24,42 The package has the potential to assist health facilities with decision-making regarding suitable approaches to embed PAIDSEM-P in addition to other evidence-based problems.
Conclusion
Pre-operative anaemia and iron deficiency screening evaluation and management pathways should be the standard of care adopted in hospitals. Developing context-specific change packages using theoretically informed frameworks to select tailored implementation strategies may help improve uptake. This study aims to evaluate if a theoretically informed change package can help improve the utilization of evidence-based practice.
What this paper adds:
- This protocol outlines a theoretically informed approach to addressing healthcare problems which can be generalized to other implementation challenges.
Disclosure
The authors JD, JH, KM, LG, NG, GA, HT report no conflicts of interest in this work.
AD is the recipient of funding for the study from the Mater Foundation. AD also gratefully acknowledges assistance received from the Australian Government Research Training Program Scholarship.
JM attended a meeting with other health care professionals organised by the company 3M.
SF reports personal fees for travel, accommodation and meeting support as member of Working Group and Clinical Reference Group developing National Patient Blood Management Guidelines from National Blood Authority (Australia), personal fees from Ethicon Biosurgery, personal fees from Baxter, honorarium for book chapter from Thieme (Stuttgart), non-financial support from Health Round Table (Australia), and Member of WHO Working Group developing Guidance for PBM Implementation into Health Care (non-renumerated) for World Health Organization, outside the submitted work.
References
1. Goel R, Patel EU, Cushing MM, et al. Association of perioperative red blood cell transfusions with venous thromboembolism in a north american registry. JAMA Surg. 2018;153(9):826–833. doi:10.1001/jamasurg.2018.1565
2. Hill GE, Frawley WH, Griffith KE, Forestner JE, Minei JP. Allogeneic blood transfusion increases the risk of postoperative bacterial infection: a meta-analysis. J Trauma Injury, Infect Critical Care. 2003;54(5):908–914. doi:10.1097/01.TA.0000022460.21283.53
3. Trentino KM, Leahy MF, Sanfilippo FM, et al. Associations of nadir haemoglobin level and red blood cell transfusion with mortality and length of stay in surgical specialties: a retrospective cohort study. Anaesthesia. 2019;74(6):726–734. doi:10.1111/anae.14636
4. Munoz M, Acheson AG, Auerbach M, et al. International consensus statement on the peri-operative management of anaemia and iron deficiency. Anaesthesia. 2017;72(2):233–247. doi:10.1111/anae.13773
5. Vaglio S, Gentili S, Marano G, et al. The Italian Regulatory Guidelines for the implementation of patient blood management. Blood Transfus. 2017;15(4):325–328. doi:10.2450/2017.0060-17
6. Gammon HM, Waters JH, Watt A, Loeb JM, Donini-Lenhoff A. Developing performance measures for patient blood management. Transfusion. 2011;51(11):2500–2509. doi:10.1111/j.1537-2995.2011.03406.x
7. National Blood Authority, National Health Medical Research Council. Patient blood management guidelines: module 2 - Perioperative. Canberra, ACT: National Blood Authority; 2012.
8. Althoff FC, Neb H, Herrmann E, et al. Multimodal patient blood management program based on a three-pillar strategy: a systematic review and meta-analysis. Ann Surg. 2019;269(5):794–804. doi:10.1097/SLA.0000000000003095
9. Meybohm P, Fischer DP, Weber CF, et al. Safety and effectiveness of a Patient Blood Management Programme in surgical patients - the study design for a multicentre epidemiological non-inferiority trial by the German PBM network. ISBT Sci Series. 2015;10(S1):141–145. doi:10.1111/voxs.12146
10. Whitney G, Daves S, Hughes A, et al. Implementation of a transfusion algorithm to reduce blood product utilization in pediatric cardiac surgery. Paediatr Anaesth. 2013;23(7):639–646. doi:10.1111/pan.12126
11. Zuckerberg GS, Scott AV, Wasey JO, et al. Efficacy of education followed by computerized provider order entry with clinician decision support to reduce red blood cell utilization. Transfusion. 2015;55(7):1628–1636. doi:10.1111/trf.13003
12. Trentino K, Mace H, Symons K, et al. Screening and treating pre-operative anaemia and suboptimal iron stores in elective colorectal surgery: a cost effectiveness analysis. Anaesthesia. 2020;76:357–365. doi:10.1111/anae.15240
13. Mabry C, Perelman S, Kim J, Blitz J. Implementation of a pre-operative anemia clinic utilizing a minimal staffing model. A & a Practice. 2019;14:1.
14. Bielby L, Akers C, Francis S, et al. The role of the transfusion safety coordinator in Australia. ISBT Sci Series. 2016;11(S1):118–125. doi:10.1111/voxs.12201
15. Munting KE, Klein AA. Optimization of pre-operative anaemia in patients before elective major surgery - why, who, when and how? Anaesthesia. 2019;74(Suppl 1):49–57. doi:10.1111/anae.14466
16. Leahy MF, Mukhtar SA. From blood transfusion to patient blood management: a new paradigm for patient care and cost assessment of blood transfusion practice. Intern Med J. 2012;42(3):332–338. doi:10.1111/j.1445-5994.2012.02717.x
17. Rineau E, Chaudet A, Chassier C, Bizot P, Lasocki S. Implementing a blood management protocol during the entire peri-operative period allows a reduction in transfusion rate in major orthopedic surgery: a before-after study. Transfusion. 2016;56(3):673–681. doi:10.1111/trf.13468
18. Kumar A, Figueroa PI, Gowans KL, et al. An evolution in blood management: past, present, and future. Qual Manag Health Care. 2011;20(4):311–321. doi:10.1097/QMH.0b013e3182315ad9
19. Tinmouth A, Macdougall L, Fergusson D, et al. Reducing the amount of blood transfused: a systematic review of behavioral interventions to change physicians’ transfusion practices. Arch Intern Med. 2005;165(8):845–852. doi:10.1001/archinte.165.8.845
20. Delaforce A, Duff J, Munday J, Hardy J. Overcoming barriers to evidence-based patient blood management: a restricted review. Implement Sci. 2020;15(1):6. doi:10.1186/s13012-020-0965-4
21. Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10(1):53. doi:10.1186/s13012-015-0242-0
22. Wensing M, Grol R. Knowledge translation in health: how implementation science could contribute more. BMC Med. 2019;17(1):88. doi:10.1186/s12916-019-1322-9
23. Delaforce A, Duff J, Munday J, Hardy J. Preoperative anemia and iron deficiency screening, evaluation and management: barrier identification and implementation strategy mapping. J Multidiscip Healthc. 2020;13:1759–1770. doi:10.2147/JMDH.S282308
24. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50. doi:10.1186/1748-5908-4-50
25. Waltz TJ, Powell BJ, Fernandez ME, Abadie B, Damschroder LJ. Choosing implementation strategies to address contextual barriers: diversity in recommendations and future directions. Implement Sci. 2019;14(1):42. doi:10.1186/s13012-019-0892-4
26. Curran GM, Bauer M, Mittman B, Pyne JM, Stetler C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med Care. 2012;50(3):217–226. doi:10.1097/MLR.0b013e3182408812
27. Weiner BJ, Lewis CC, Stanick C, et al. Psychometric assessment of three newly developed implementation outcome measures. Implementation Sci. 2017;12(1):108. doi:10.1186/s13012-017-0635-3
28. Mater Misericordiae. Pre-operative anaemia and iron deficiency screening and treatment (excluding pregnant women) procedure. In: Internal Hospital Document. Brisbane, Australia; 2020.
29. Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348(mar073):g1687–g1687. doi:10.1136/bmj.g1687
30. World Health Organisation. Haemoglobin concentrations for diagnosis of anaemia and assessment of severity. In: Vitamin and Mineral Nutrition Information System. Vol. 2018. Geneva: World Health Organization; 2011.
31. Poon E, Pache D, Delaforce A, Abdalla L, McGuire T. Anaemia in patients undergoing major bowel surgery – prevalence and current practice: a public and private institution experience. J Perioper Pract. 2020;1750458920934321. doi:10.1177/1750458920934321
32. Delaforce A, Galeel L, Poon E, et al. Pre-operative anemia screening and treatment practices in patients having total joint replacement surgery: a retrospective, observational audit. J Blood Med. 2020;11:259–265. doi:10.2147/JBM.S254116
33. Delaforce A, Moore D, Duff J, Munday J, Hardy J. Assessing transfusion practice in elective surgical patients: a baseline audit. ISBT Sci Series. 2019;14(4):415–422. doi:10.1111/voxs.12496
34. Delaforce A, Duff J, Ralph N. Changing the standard of blood management in Australia: an overview. J Perioperative Nurs. 2018;31(2):15–17. doi:10.26550/2209-1092.1026
35. Australian Commission on Safety & Quality in Health Care. National Safety and Quality Health Service Standards.
36. Morgan PN, Coleman PL, Martinez-Garduno CM, Gunaratne AW, McInnes E, Middleton S. Implementation of a patient blood management program in an Australian private hospital orthopedic unit. J Blood Med. 2018;9:83–90. doi:10.2147/JBM.S157571
37. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
38. Goodnough LT, Shander A, Spivak JL, et al. Detection, evaluation, and management of anemia in the elective surgical patient. Anesth Analg. 2005;101(6):1858–1861. doi:10.1213/01.ANE.0000184124.29397.EB
39. Fowler AJ, Ahmad T, Phull MK, Allard S, Gillies MA, Pearse RM. Meta-analysis of the association between pre-operative anaemia and mortality after surgery. BJS. 2015;102(11):1314–1324.
40. Rössler J, Schoenrath F, Seifert B, et al. Iron deficiency is associated with higher mortality in patients undergoing cardiac surgery: a prospective study. Br J Anaesth. 2020;124(1):25–34. doi:10.1016/j.bja.2019.09.016
41. Edwardson CL, Yates T, Biddle SJH, et al. Effectiveness of the Stand More AT (SMArT) Work intervention: cluster randomized controlled trial. BMJ. 2018;363:k3870. doi:10.1136/bmj.k3870
42. Powell BJ, Waltz TJ, Chinman MJ, et al. A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project. Implementation Sci. 2015;10(1):21. doi:10.1186/s13012-015-0209-1
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.