")
Back to Journals » Nature and Science of Sleep » Volume 12
A Systematic Review of Instruments for the Assessment of Insomnia in Adults
Authors Ali RM, Zolezzi M , Awaisu A
Received 22 February 2020
Accepted for publication 26 May 2020
Published 2 July 2020 Volume 2020:12 Pages 377—409
DOI https://doi.org/10.2147/NSS.S250918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Sutapa Mukherjee
Raja Mahamade Ali, Monica Zolezzi, Ahmed Awaisu
College of Pharmacy, QU Health, Qatar University, Doha 2713, Qatar
Correspondence: Monica Zolezzi
College of Pharmacy, QU Health Qatar University, PO Box 2713, Doha, Qatar
Tel +974 4403 5623
Fax +974 4403 5551
Email [email protected]
Introduction: Self-reported sleep instruments remain the most practical methods for the assessment of insomnia in clinical practice. This systematic review aims to identify, describe and summarize the psychometric properties of questionnaires available for the assessment of insomnia in the adult population. In addition, the review also aimed to identify sleep instruments available in the Arabic language.
Methods: A systematic literature search was conducted using the following electronic databases: PubMed, EMBASE, ProQuest Central, SCOPUS, and Google Scholar. The quality assessment of the instruments was conducted using two established international criteria.
Results: One hundred and seven articles were selected for inclusion, from which 31 instruments were identified and categorized based on the constructs they assess as: (1) screening for insomnia (n=14); (2) measuring the consequences of insomnia (n=8); (3) assessing the cognitive aspects of insomnia (n= 5); and (4) assessing sleep hygiene (n= 4). The review of the psychometric properties showed that the Insomnia Severity Index and the Functional Outcomes of Sleep Questionnaire were the most extensively evaluated instrument. Criterion validity and reliability measures were the most commonly reported properties. Only four of the identified instruments were available in Arabic.
Discussion: Overall, the findings of this study indicate ample availability of sleep instruments. However, psychometric testing for several of the available sleep instruments remains incomplete, particularly responsiveness and interpretability. Our findings suggest that future studies should focus on reporting more psychometric measures to ensure the trustworthiness of these instruments.
Keywords: insomnia, sleep hygiene, sleep quality, questionnaires, psychometric properties
Introduction
Worldwide reports suggest that around one-third of the adult population complains of insomnia symptoms.1–2 Insomnia is characterized by persistent sleep difficulty despite adequate sleep opportunity and associated daytime dysfunction.3 Insomnia has been associated with increased rates of road accidents, lower productivity and work absenteeism.4,5 Several factors are known to contribute to the development or worsening of insomnia symptoms. Current findings from the literature suggest that negative cognitive processes including worry, rumination and catastrophizing thoughts are associated with worse sleep quality and insomnia.6 These processes have been shown to fuel anxiety and arousal resulting in delayed sleep onset and shorter sleep duration.7 Similarly, poor sleep hygiene, which consists of a combination of behavioral practices and environmental conditions which improves sleep, is common among insomniacs.8–11
Studies suggest that chronic insomnia is an independent risk factor for developing mental illnesses in otherwise healthy individuals.12,13 Chronic insomnia has also been reported to increase the probability of developing chronic medical conditions, such as hypertension, cardiovascular disease and type 2 diabetes.14,15 Therefore, early detection and management of insomnia is important to minimize these associated risks. Although polysomnography (PSG) is considered the gold standard method for evaluating insomnia, it is not routinely used as it requires a specialized setting and equipment, and it is often labour intensive. Wrist actigraphy is another objective tool for the assessment of insomnia, but is limited by its lack of specificity.16,17 Consequently, self-reported sleep instruments remain the most practical methods for the assessment of insomnia in clinical practice.16,18 There are several systematic reviews on a range of sleep instruments utilized for the assessment of sleep dysfunction in a variety of medical and neuropsychiatric disorders, or in specialized populations.19–21 In these reviews, there was insufficient evaluation of the psychometric properties of the instruments that were identified, and none of them included instruments which assess sleep hygiene practices in the adult population. Therefore, the main objective of this study is to present an updated systematic review of the literature on validated self-reported instruments used for the assessment of different dimensions of sleep in the adult population. In addition, the review also aimed to identify sleep instruments available in Arabic language.
Methods
Search methods
Data Sources and Search Strategy
A comprehensive systematic search was conducted to identify studies reporting the development and/or validation of instruments for the assessment of self-reported sleep and sleep hygiene in the adult population. The five databases and search engines utilized included PubMed (1966 - April 2018), EMBASE (1980 - April 2018), ProQuest Central (1947–2018), SCOPUS (1966 - April 2018), and Google Scholar (till April 2018). Grey literature was also searched by reviewing conference proceedings and abstracts of the Canadian Sleep Society and the American Academy of Sleep Medicine published in the period from January 2014 to December 2017. Additionally, a hand search of the bibliographies of the articles identified through the electronic databases search was undertaken. Search terms used in the electronic databases search were classified into three categories related to: sleep dysfunction (Category A), the instrument for assessment (Category B), and validation and psychometric properties (Category C). Terms from Category C were not used in databases such as PubMed which offered “validation studies” as one of the limits or filters. Publication language was limited to English and no limits were imposed on the publication year. Examples of full search strategies for two of the electronic databases can be found under the supplementary material. In addition to the English search, two separate searches were conducted to identify sleep instruments developed in Arabic language or translated into Arabic. The first used the same search terms as those used in the original search, in addition to the word “Arabic”. The second was conducted in Arabic language in the following databases: PubMed, Google Scholar and Dar Al-mandumah using the same search terms as those used in the original search.
Inclusion Criteria
Articles selected for full review were those providing results of validation studies or reporting psychometric properties of instruments and questionnaires assessing characteristics of sleep (quality, quantity, nocturnal awakenings), daytime consequences of poor sleep, or sleep hygiene in the adult population. The inclusion criteria were limited to instruments completed by self-report and to instruments written in English or Arabic.
Exclusion Criteria
Studies were excluded from the review if they included evaluating instruments designed to measure sleep disorders other than insomnia (eg obstructive sleep apnea, restless leg syndrome, etc.), those using sleep items as subdomains of an instrument assessing a condition other than insomnia, studies which focused on pediatric/geriatric populations, studies describing instruments designed to be completed by clinician or caregiver and not by the patient, using instruments developed in languages other than English or Arabic, or describing instruments not psychometrically validated.
Data Collection and Analysis
Data Collection Process and Data Extraction
Duplicate citations were removed after obtaining the initial records of relevant articles from different databases. Titles and abstracts of the articles were then screened for relevance. Full-text of eligible articles were obtained and screened against the inclusion and exclusion criteria. Data were extracted from the eligible studies according to eight key attributes, as established by the Scientific Advisory Committee, Medical Outcomes Trust (SAC-MOT).22 The extraction tool used in this study included the following elements: instrument’s name, authors, conceptual framework (domains and purpose), psychometric properties, validation population, general description of the instrument (number of items, scale, scoring, response format, burden), and cultural and linguistic adaptation. The psychometric properties were extracted from studies describing the validation of the original (English or Arabic) version of the instruments. The psychometric properties extracted from the validation studies included validity, reliability, responsiveness, and interpretability. In addition, instruments’ attributes related to the validation sample were extracted. Data extraction was done by one reviewer (RA) and reviewed by a second author (MZ). The psychometric properties for instruments validated in specific populations were not extracted.
Quality Assessment
A modified version of the criteria developed by Terwee et al23 was used to assess the quality of the sleep instruments. The Terwee at al. criteria evaluates 8 psychometric properties including validity (content, construct and criterion), reliability (internal consistency and reproducibility), responsiveness, interpretability and floor and ceiling effects.23 For the purposes of this study, the criteria for the floor and ceiling effects and the agreement component of the reproducibility were not used, primarily because, for the most part, these measures were not reported in the validation studies included in this review. In addition, Pearson’s Correlation Coefficient was used for rating the reliability, responsiveness, criterion and construct validity.
Results
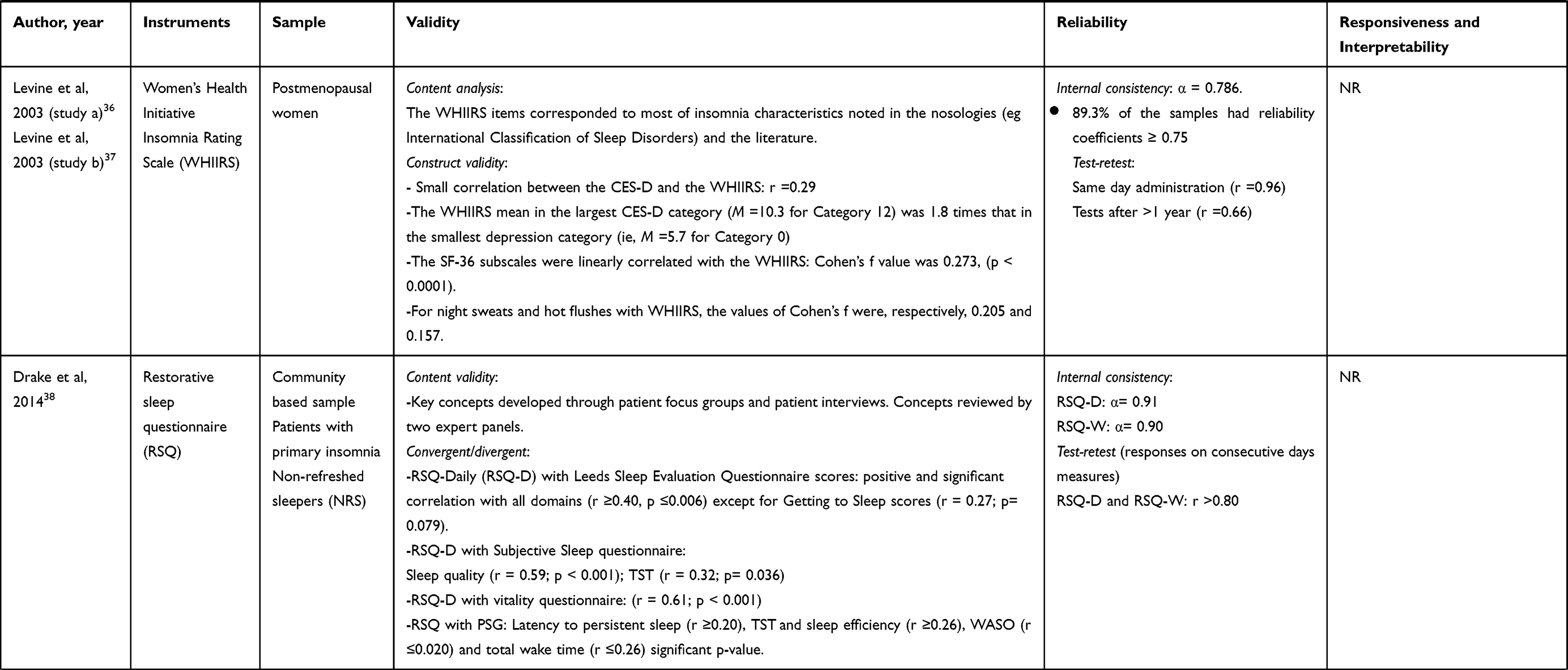
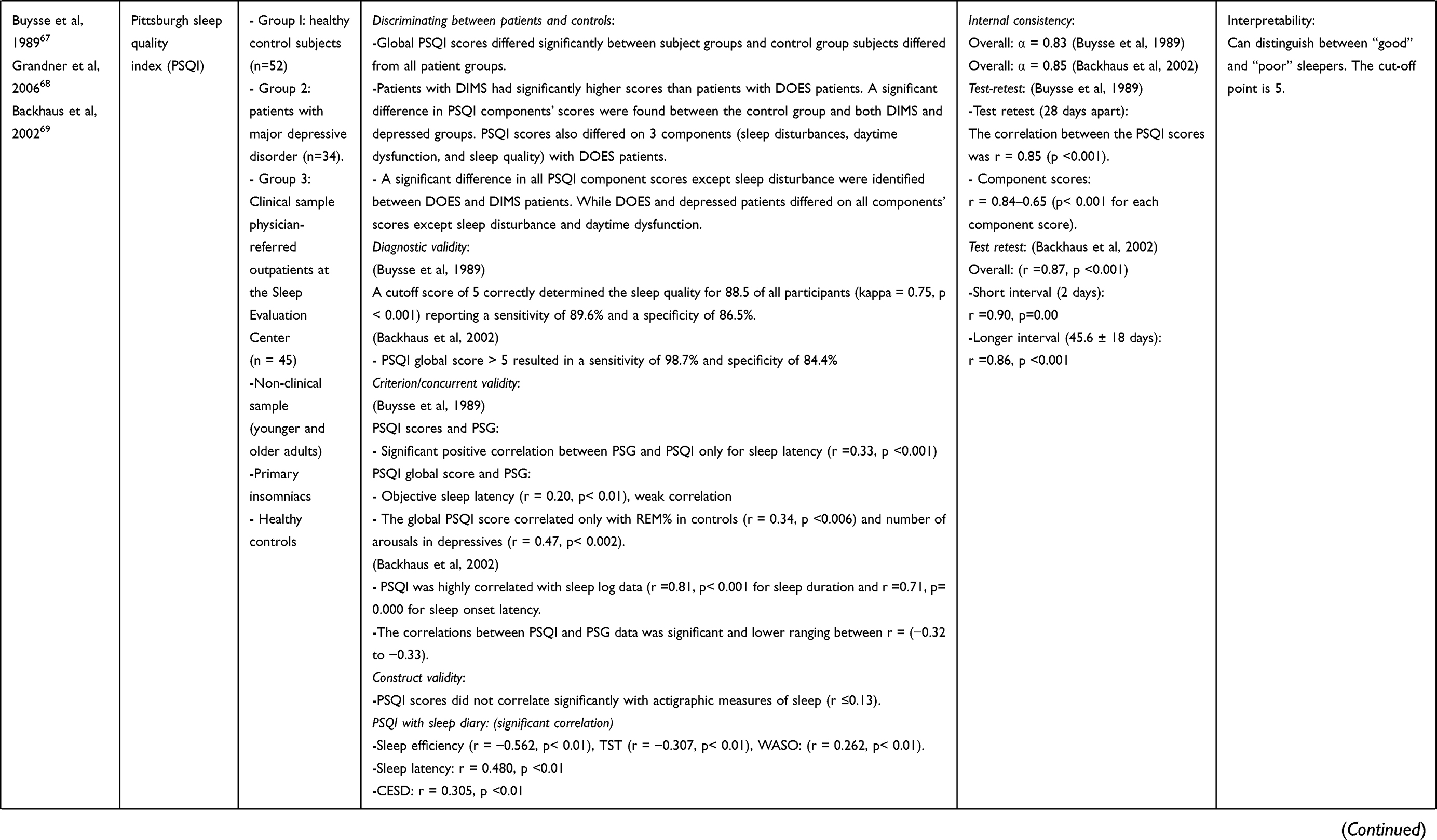
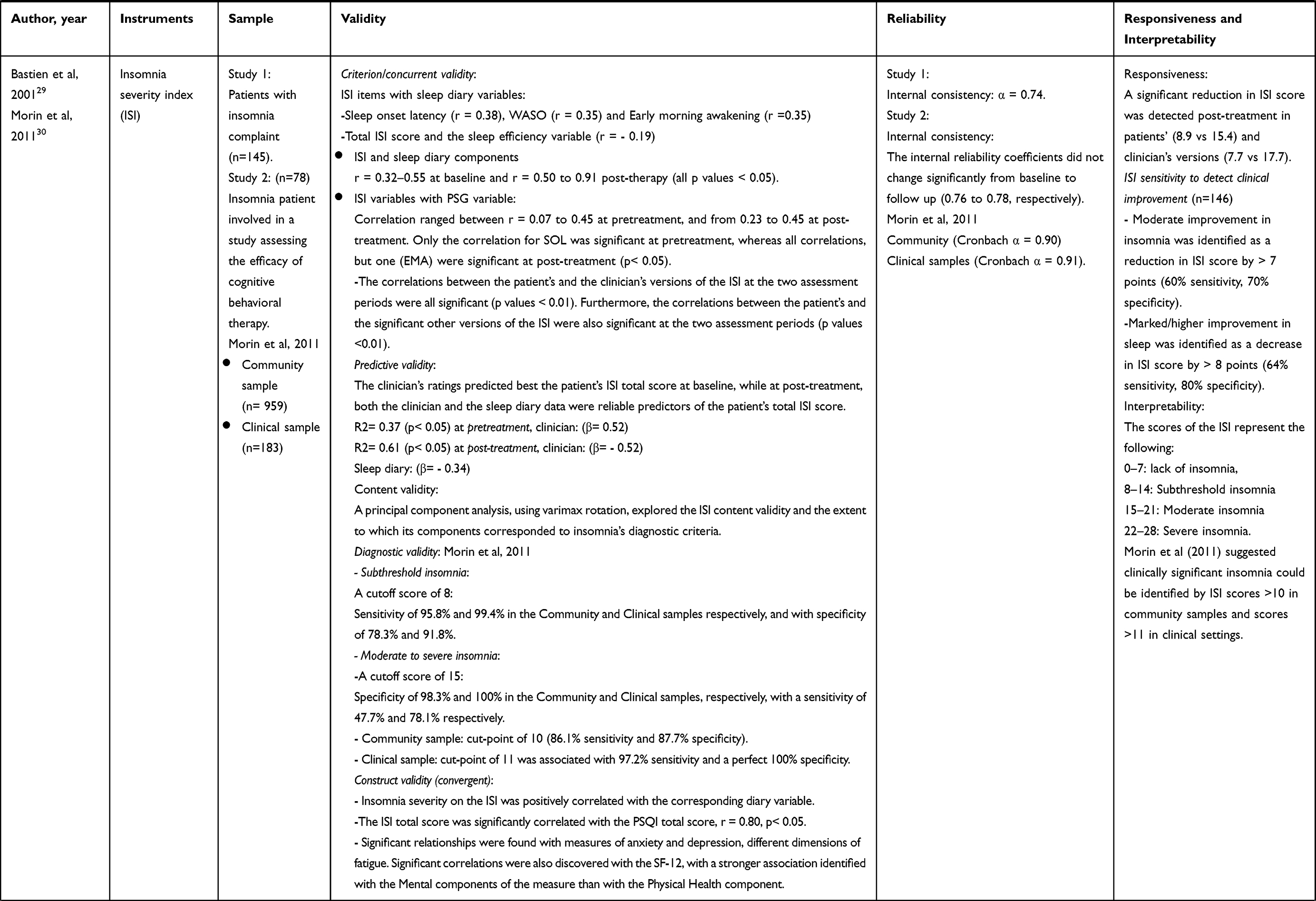
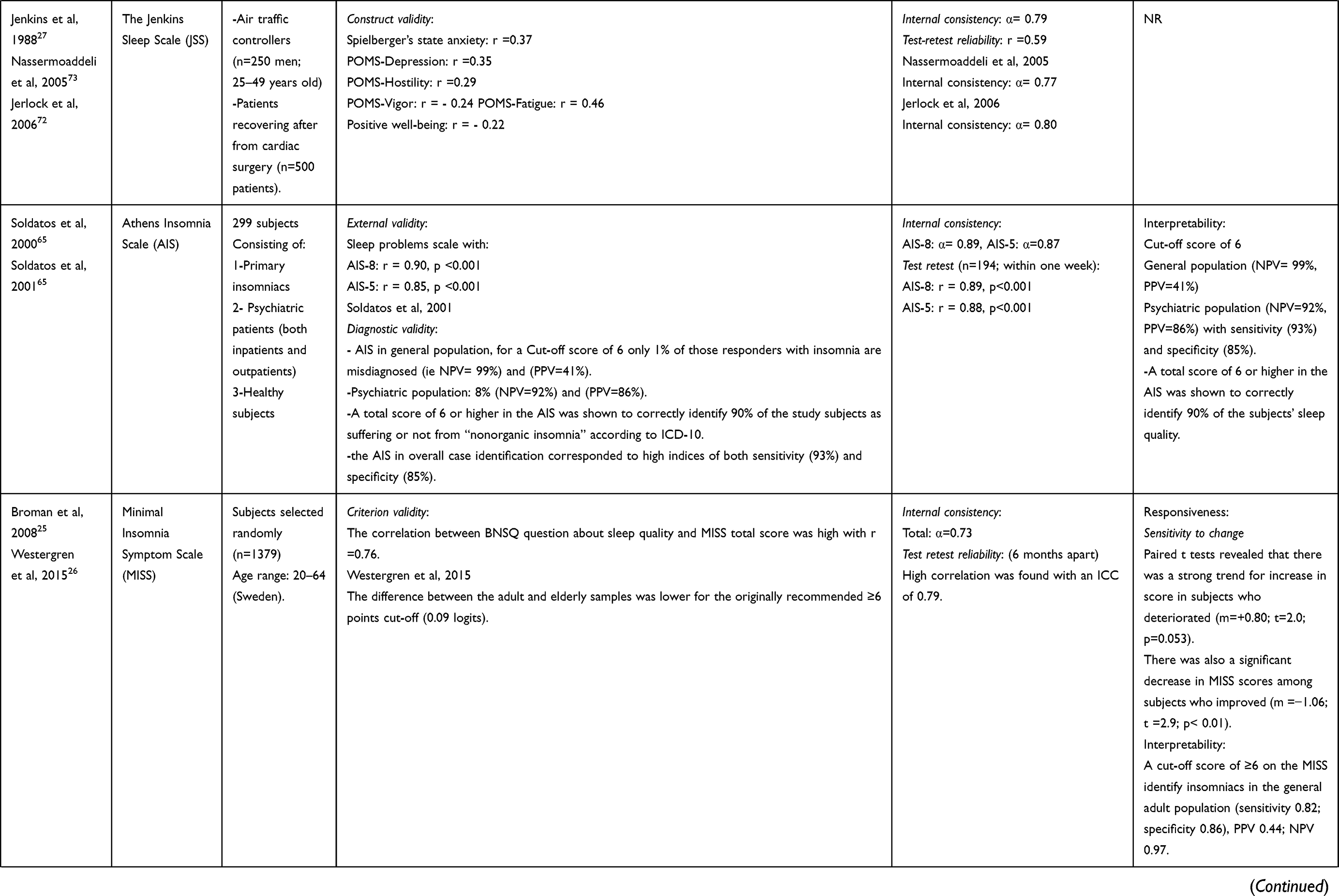
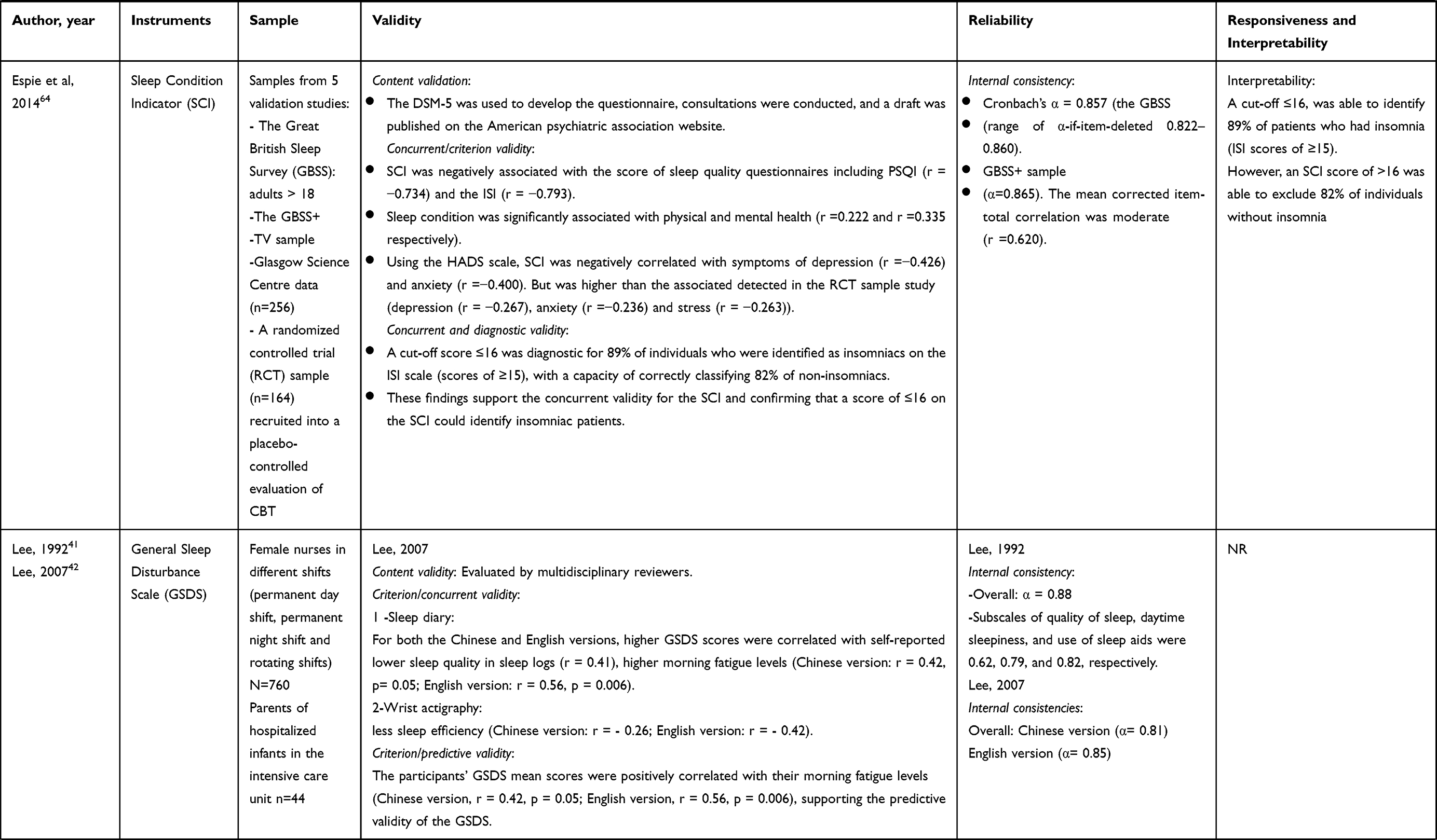
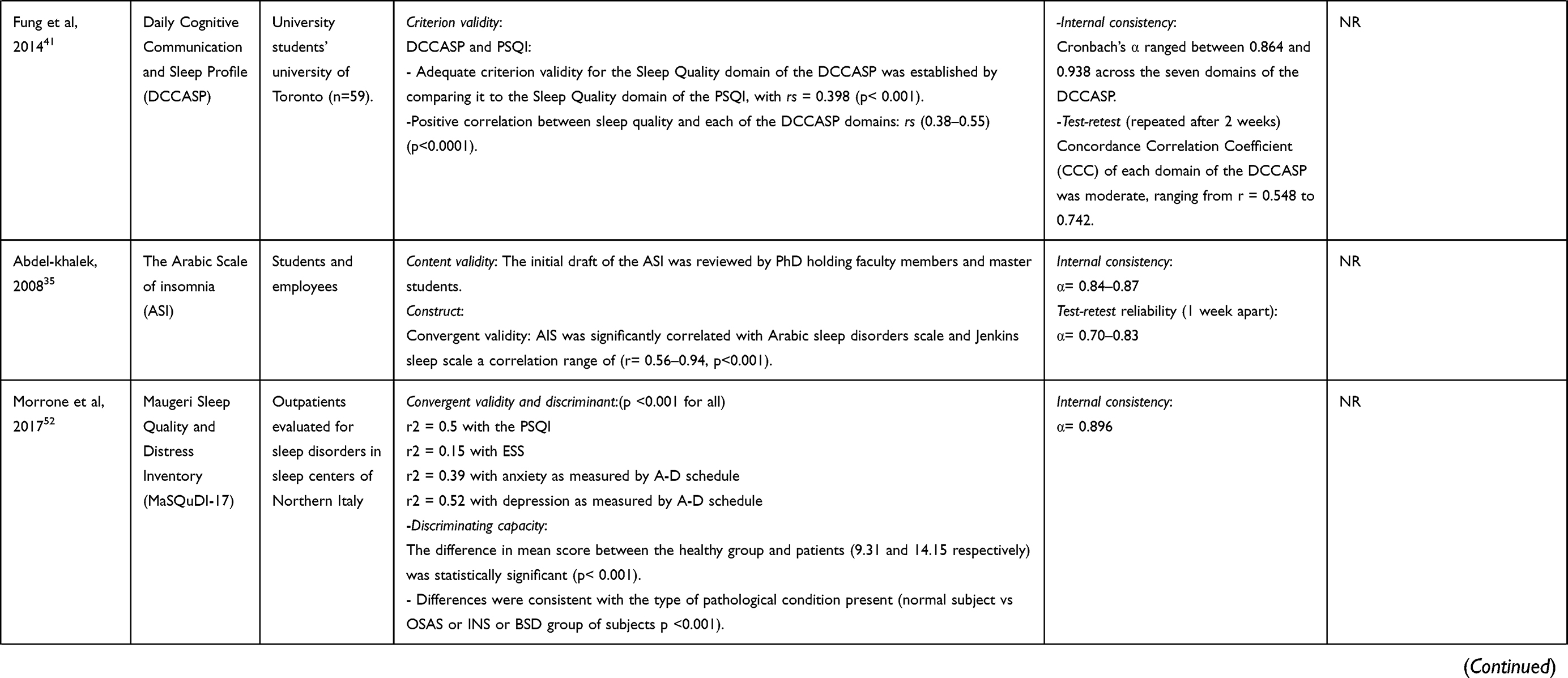
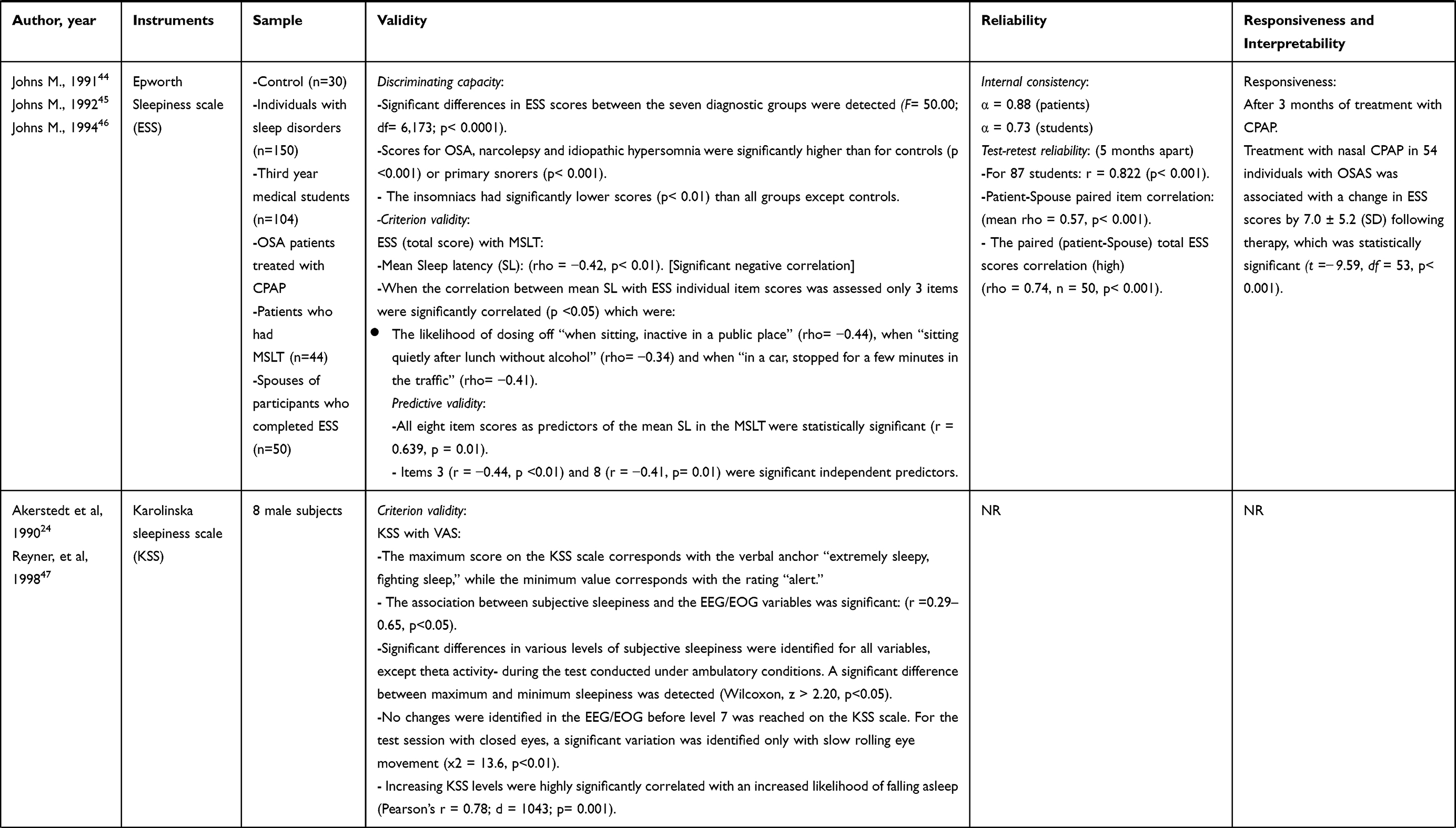
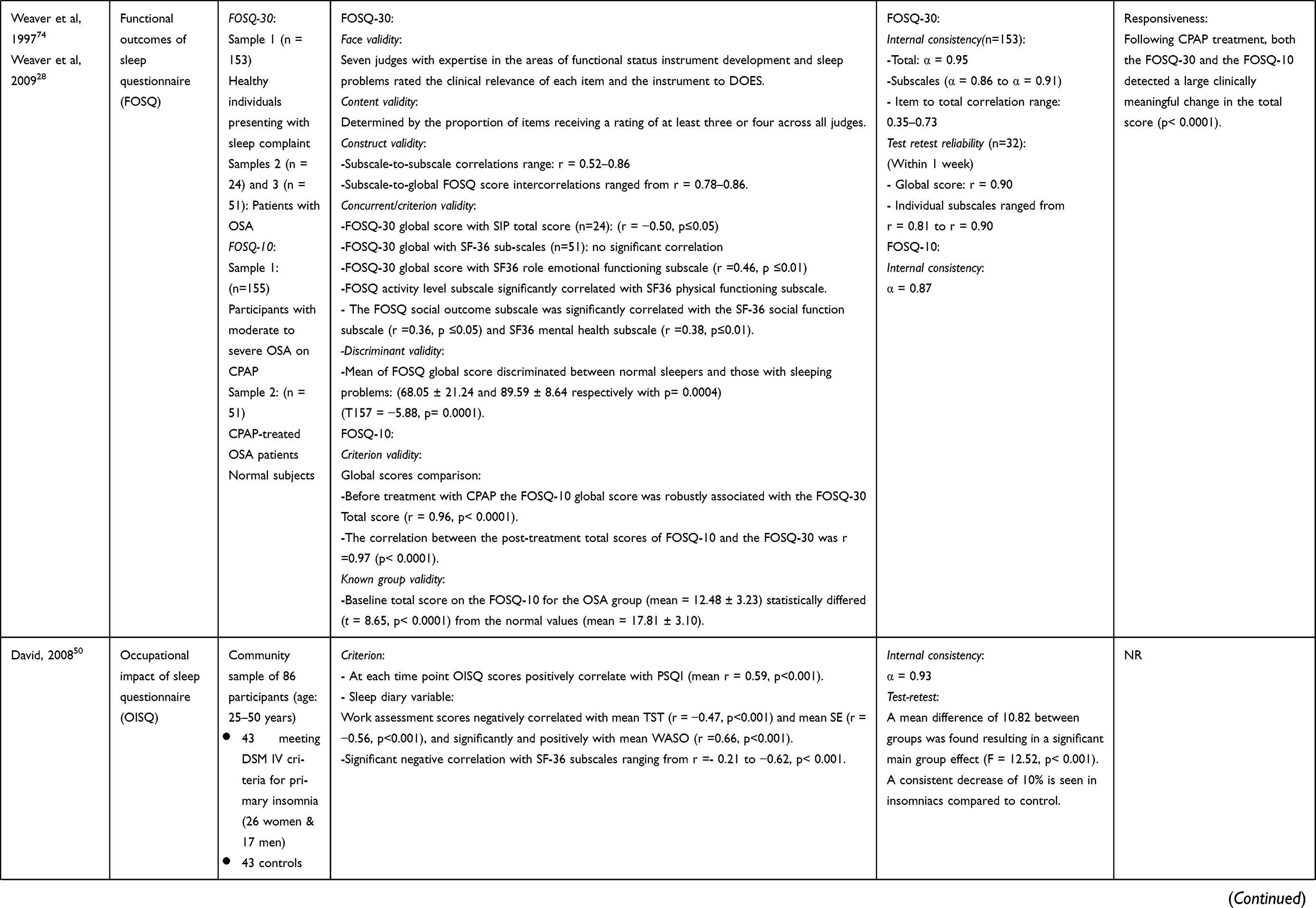
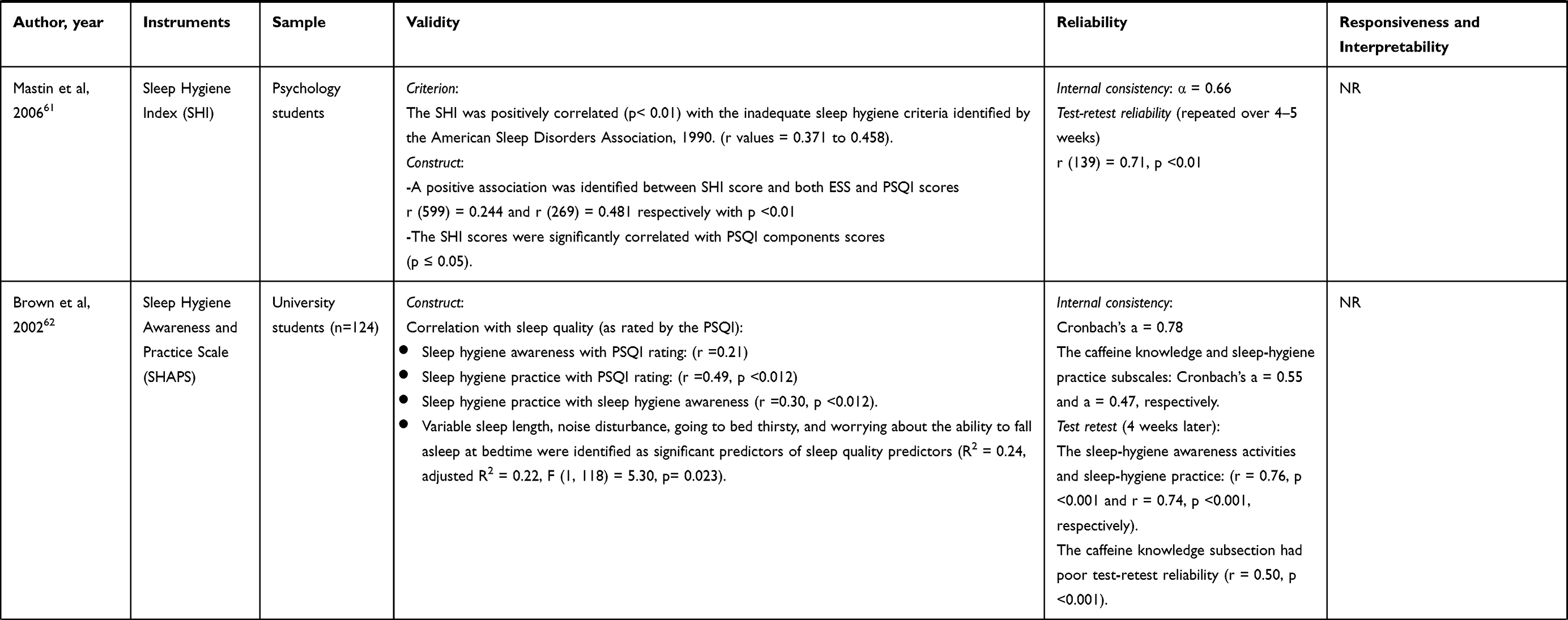
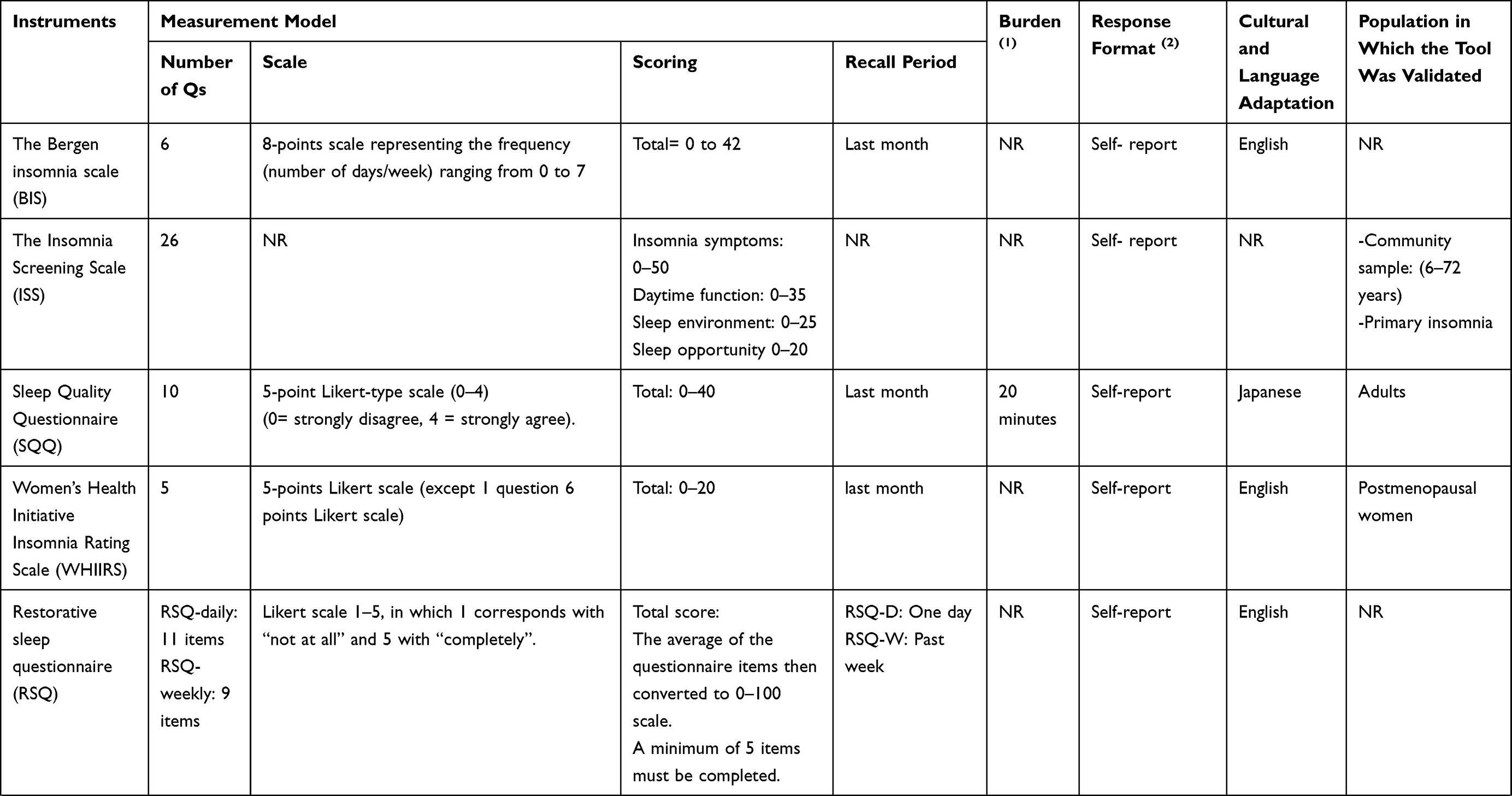
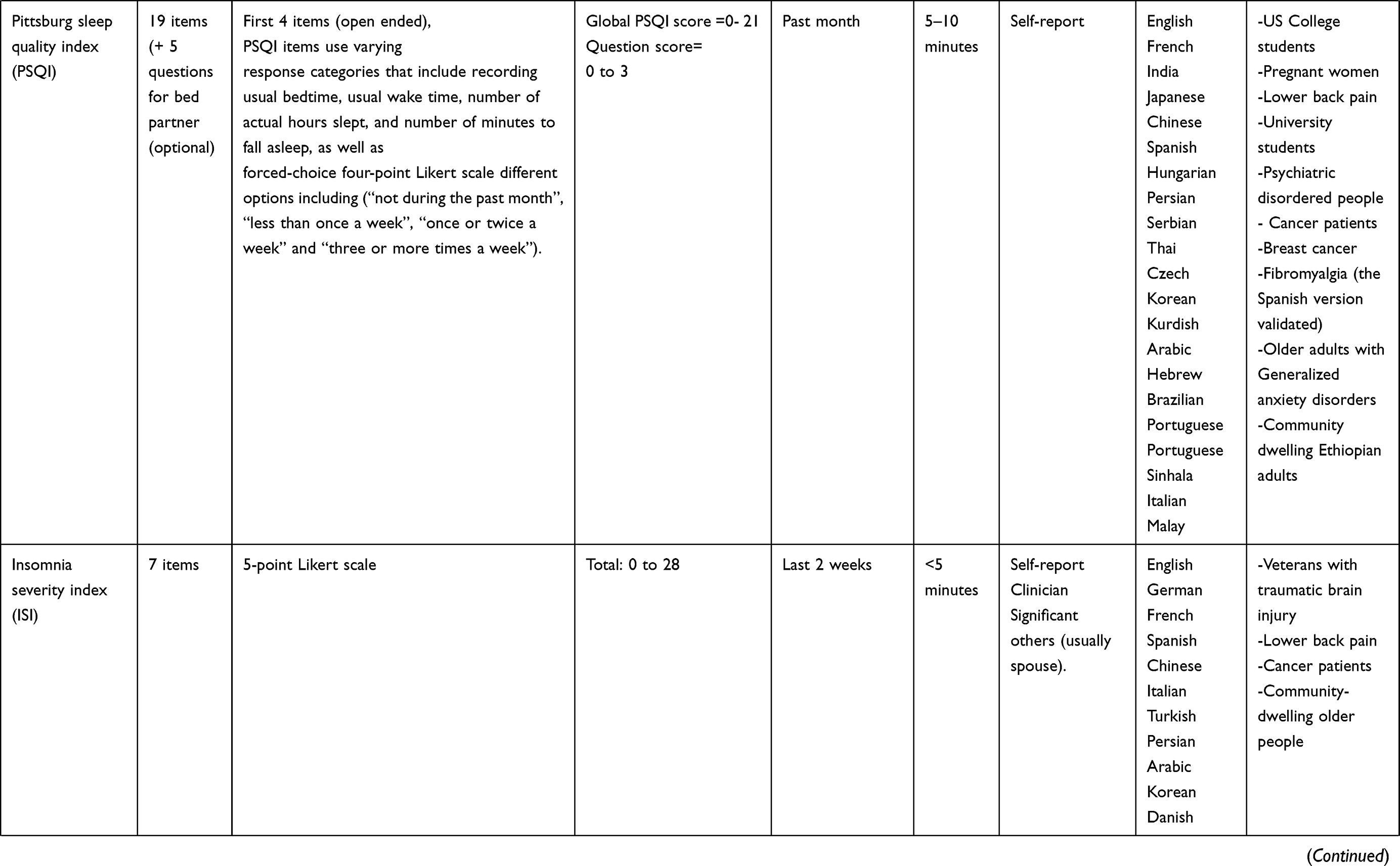
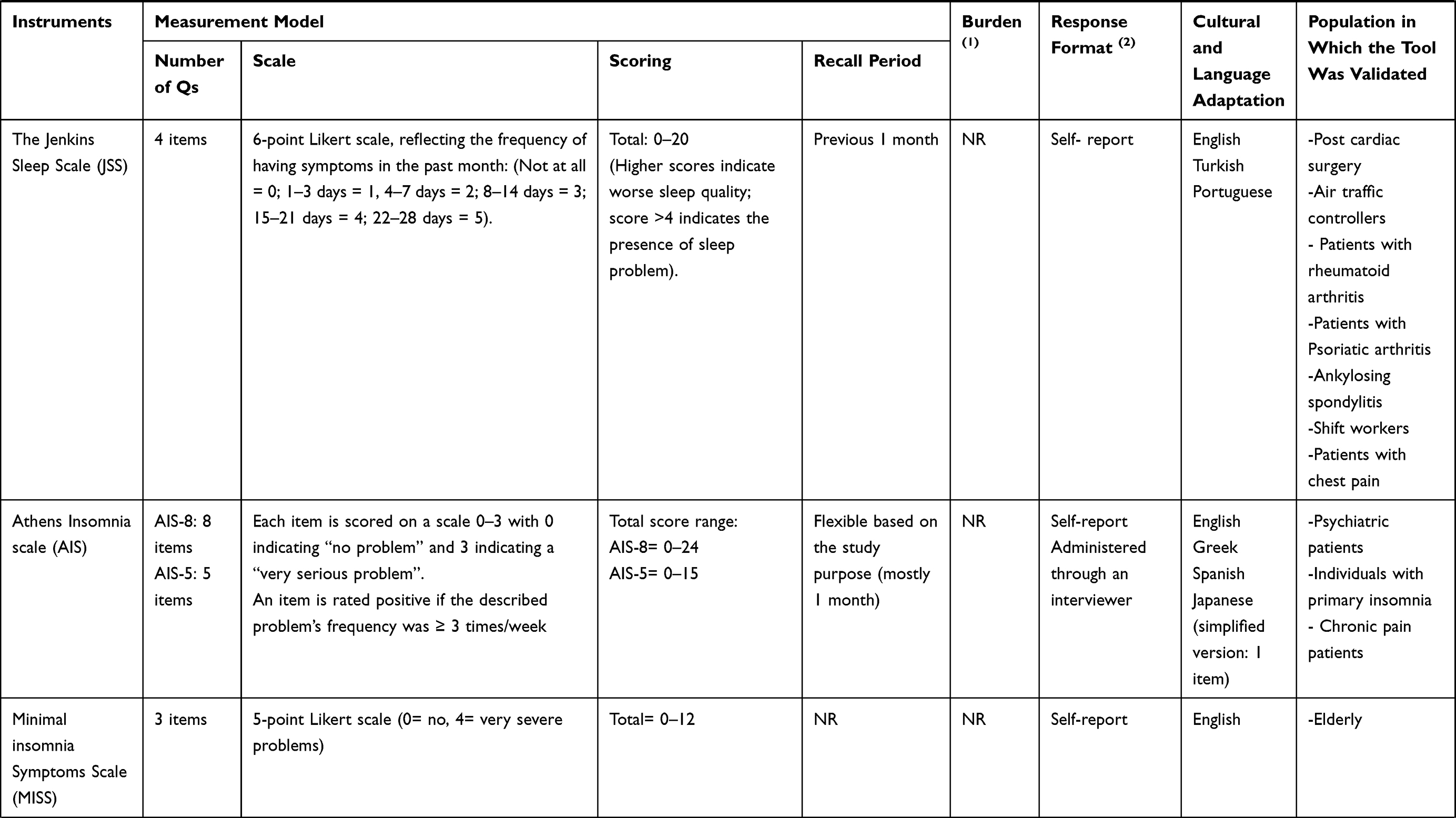
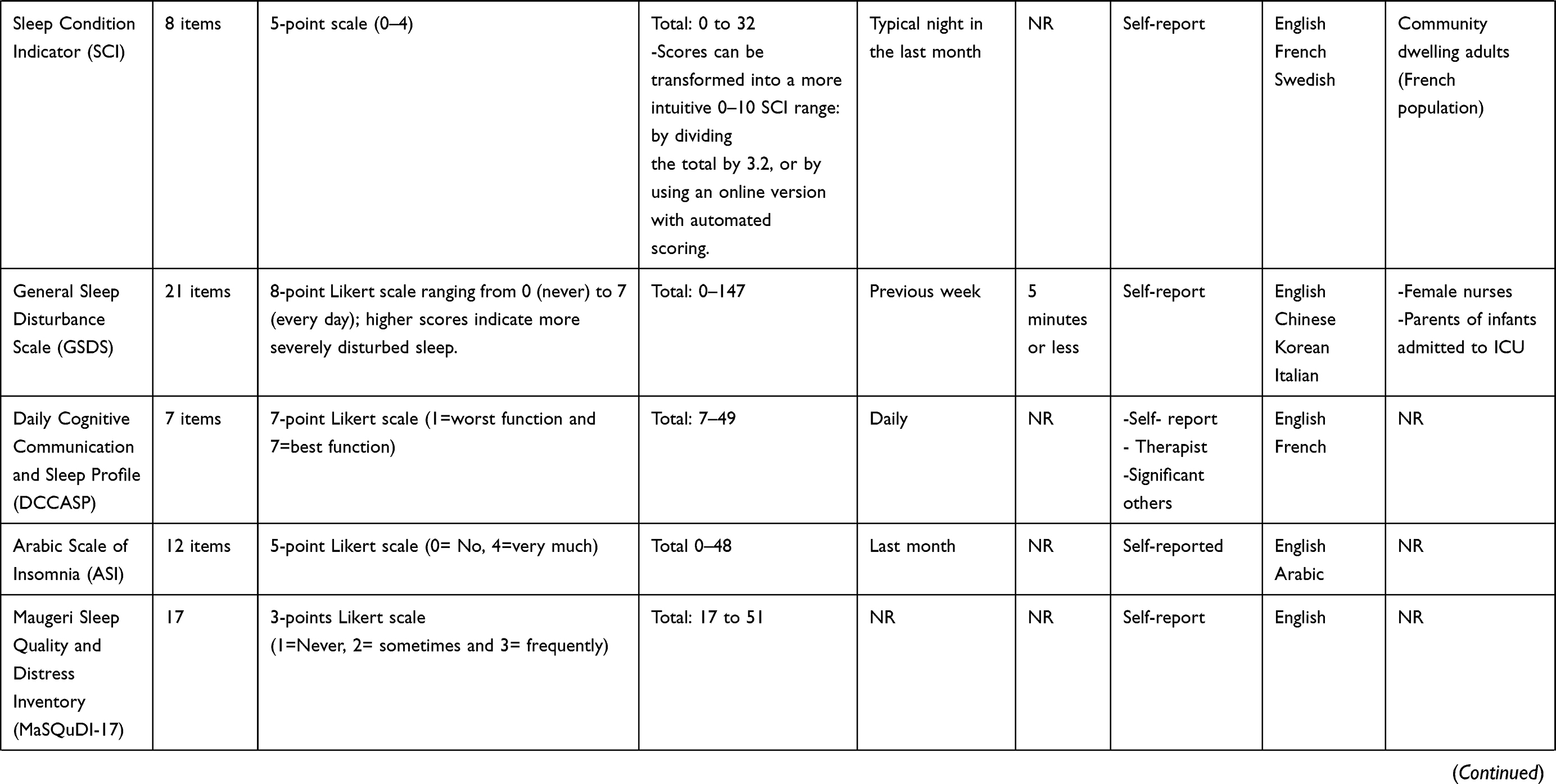
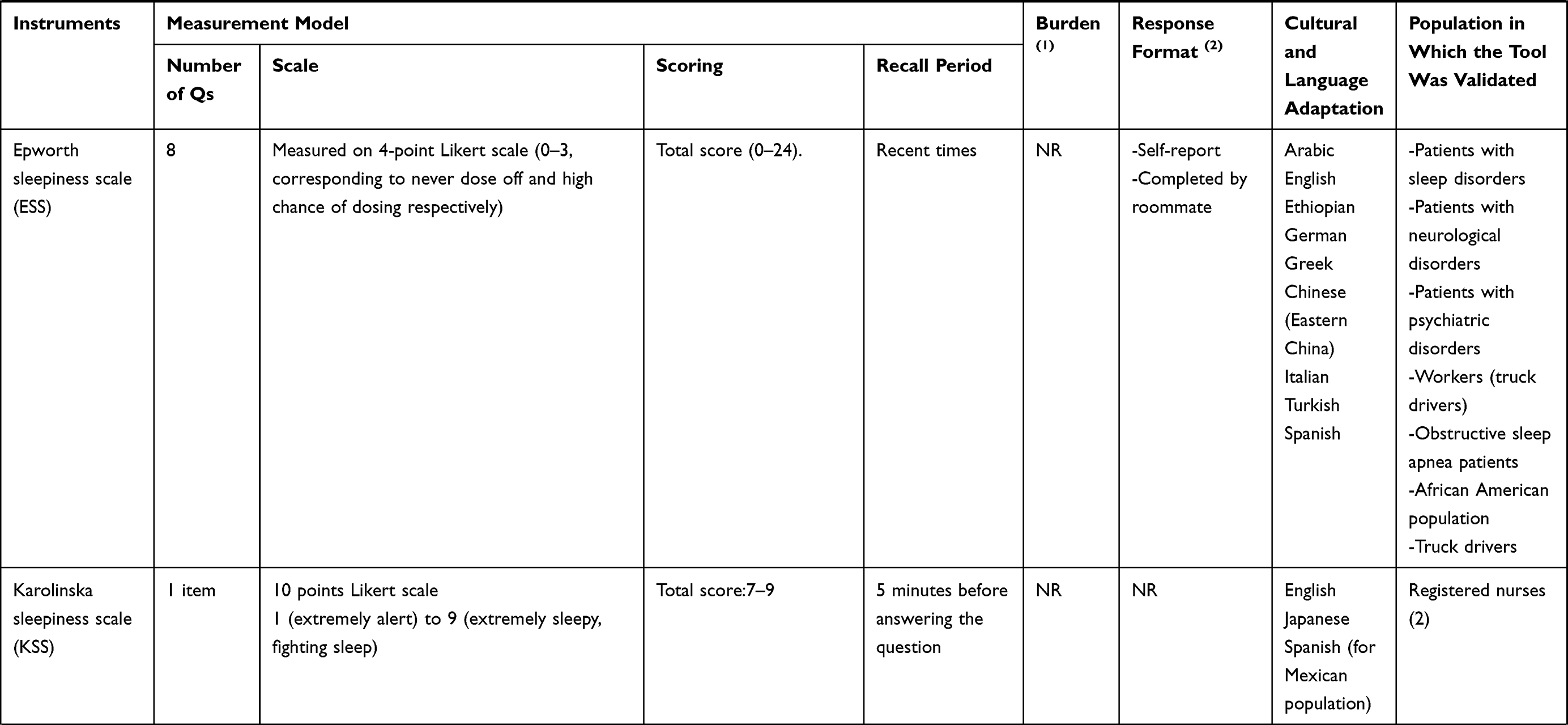
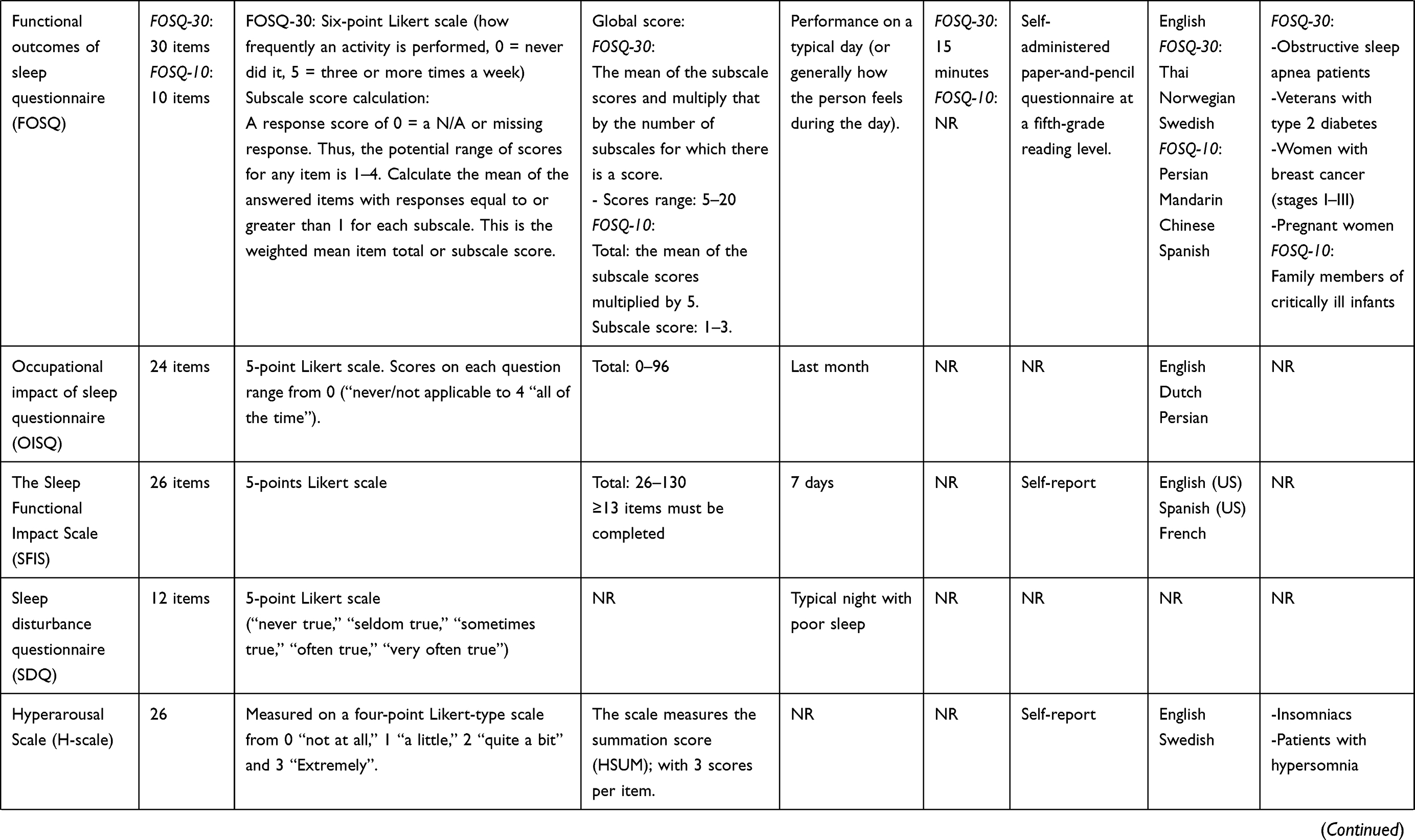
As illustrated in Figure 1, a total of 4453 citations were retrieved from the search. One hundred and seven articles were deemed suitable for inclusion in the review. These articles included 31 distinct sleep instruments. Of the 107 articles included, 47 discussed the validation process of the instruments in English, while the remaining 60 articles reviewed the translation and cultural adaptation of these instruments into a variety of languages and populations. The two additional searches to identify sleep instruments in the Arabic language did not identify any additional results than those derived from the original search. Table 1 summarizes the results of the validation studies (n=47) related to the 31 sleep instruments included in this review. The table also describes the psychometric properties of the instruments and the characteristics of the populations in which they were validated. Table 2 provides a detailed description of the characteristics of the 31 instruments.
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
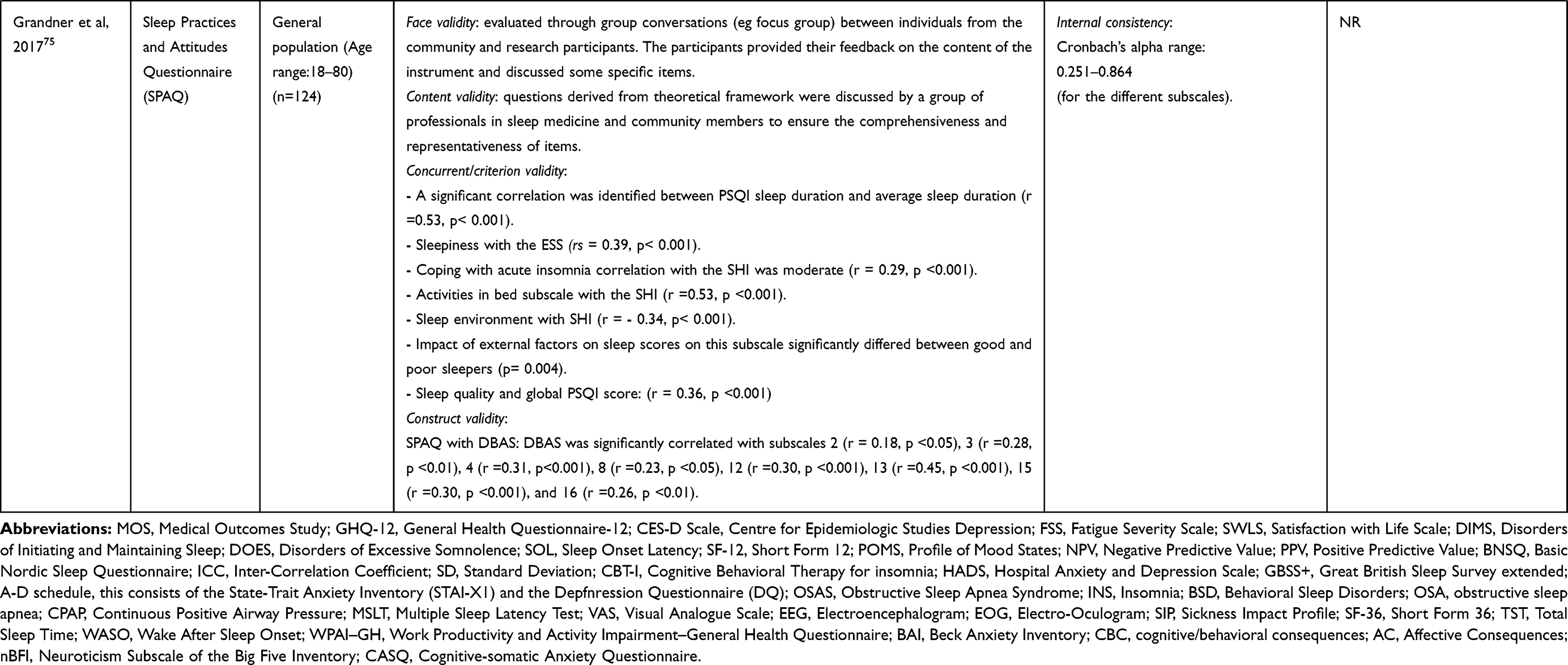 |
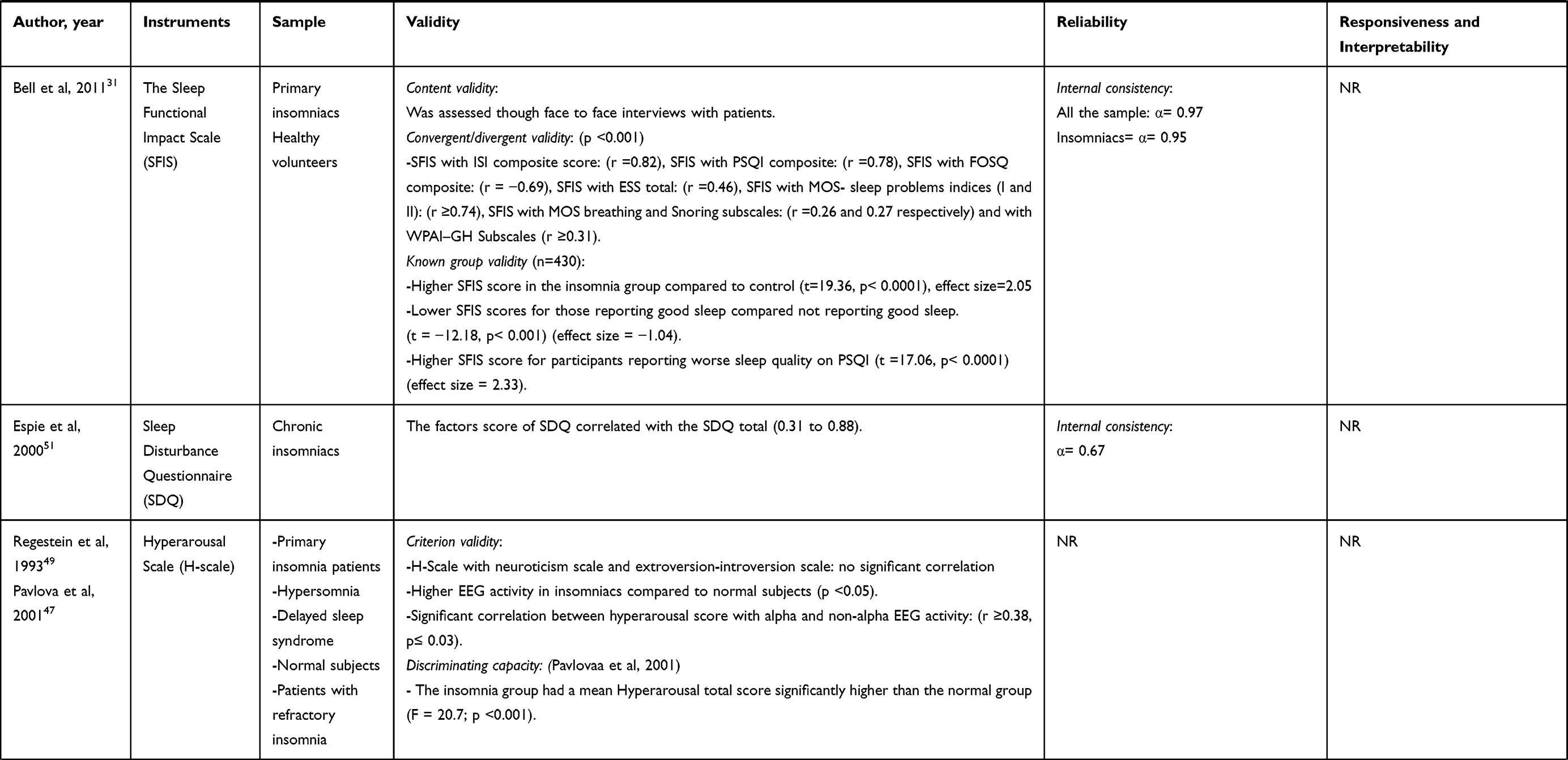
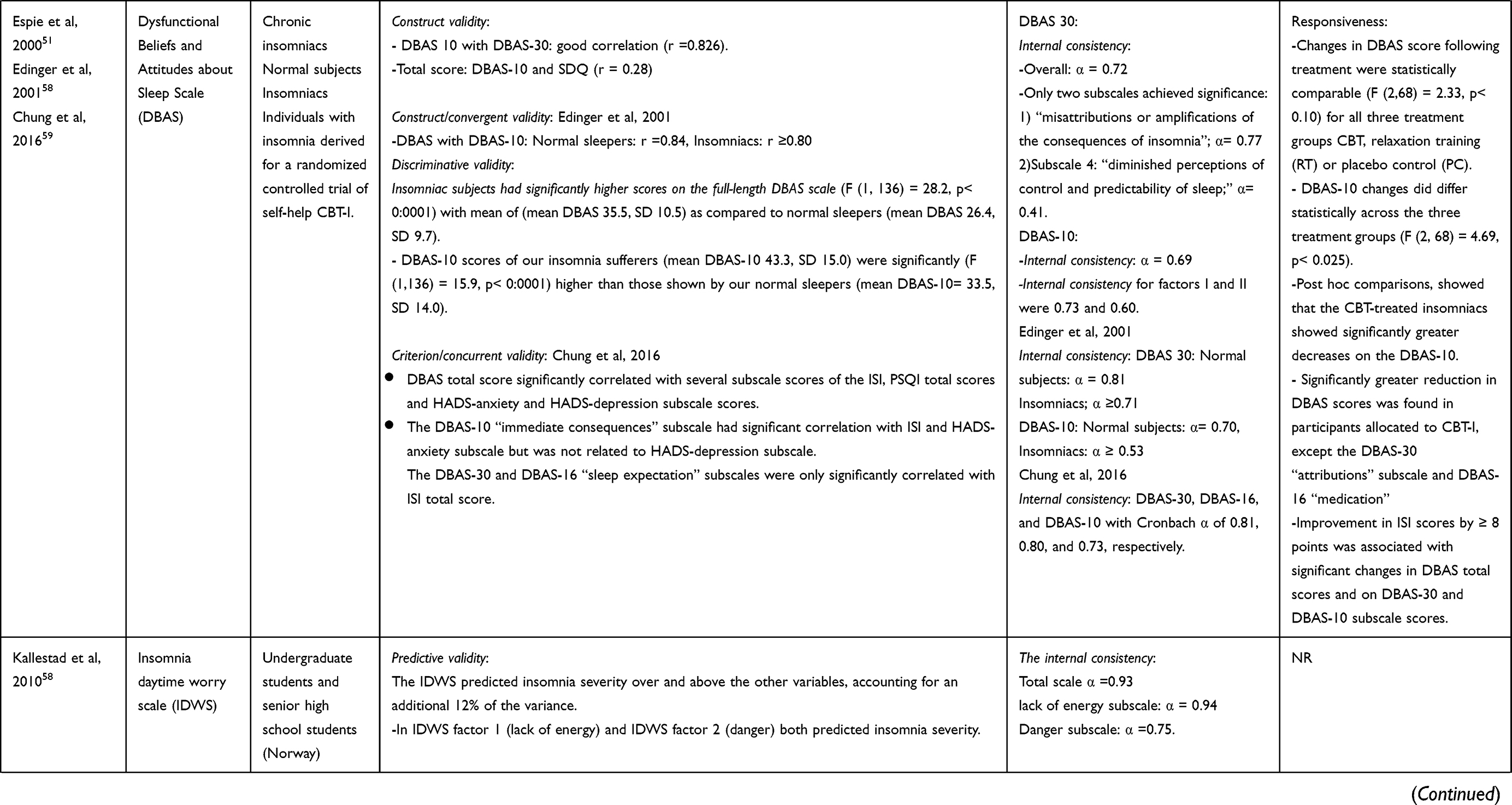
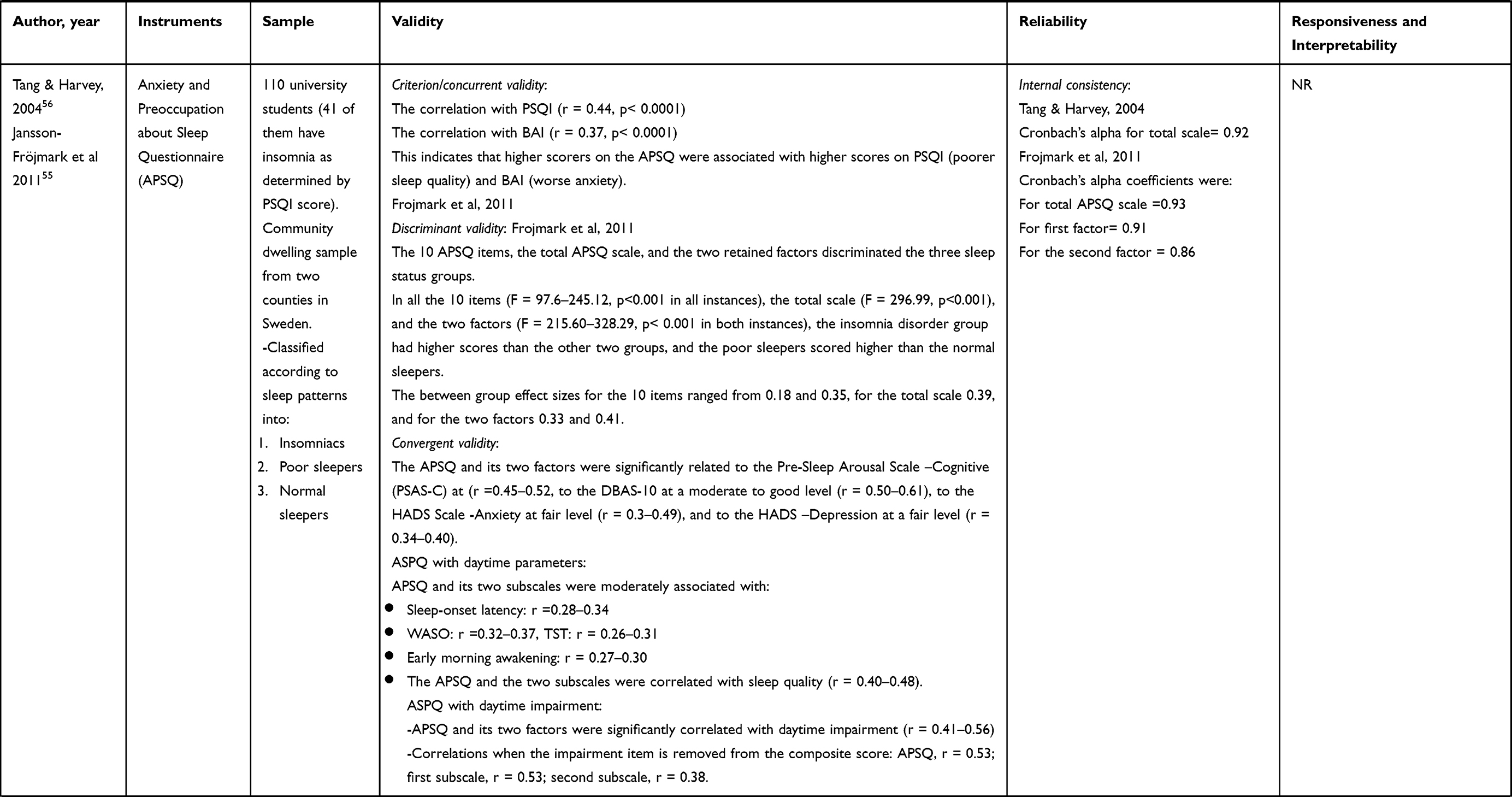
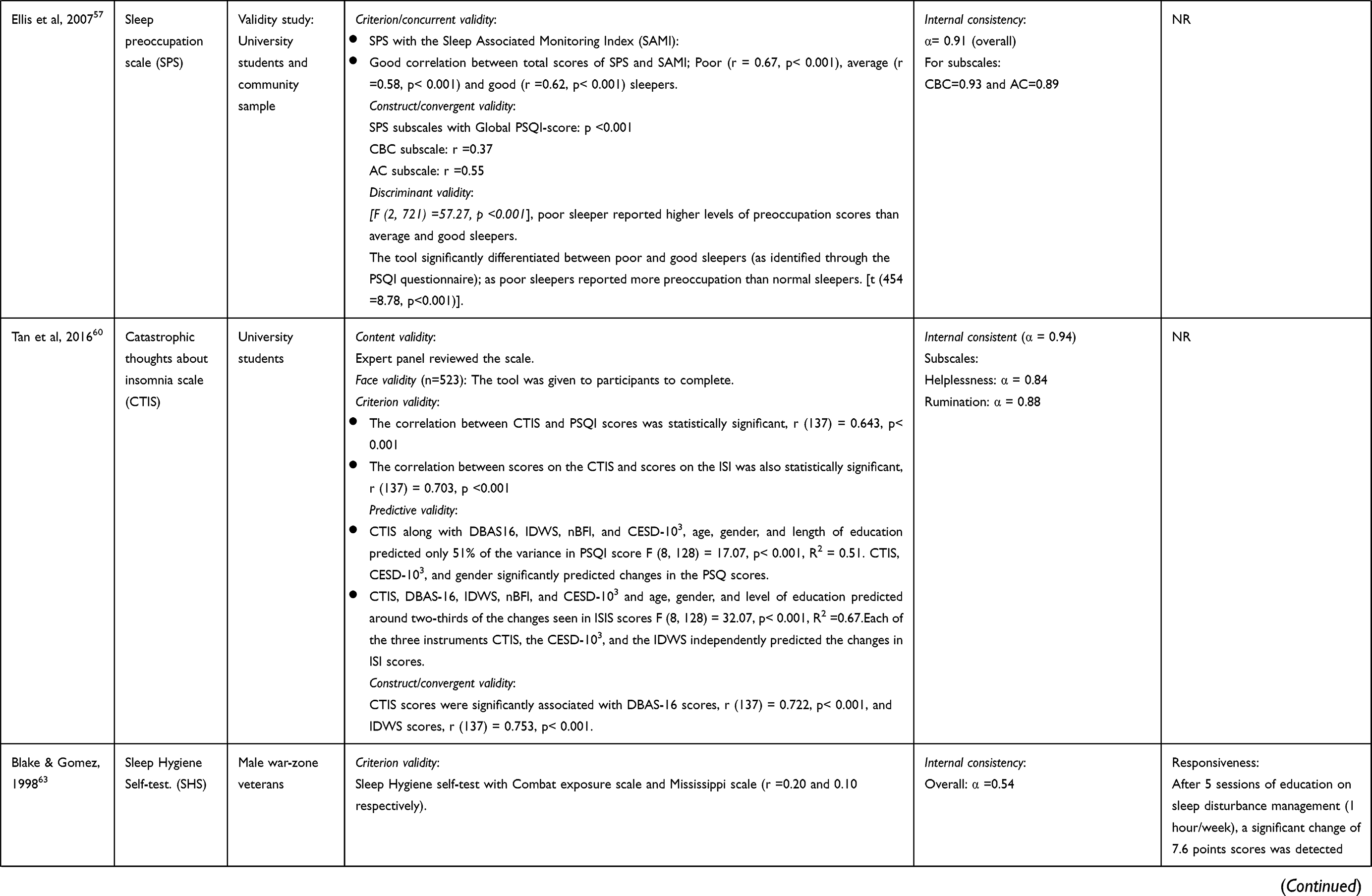
Table 1 Studies Testing the Psychometric Properties of Extracted Sleep Instruments |
 |
 |
 |
 |
 |
 |
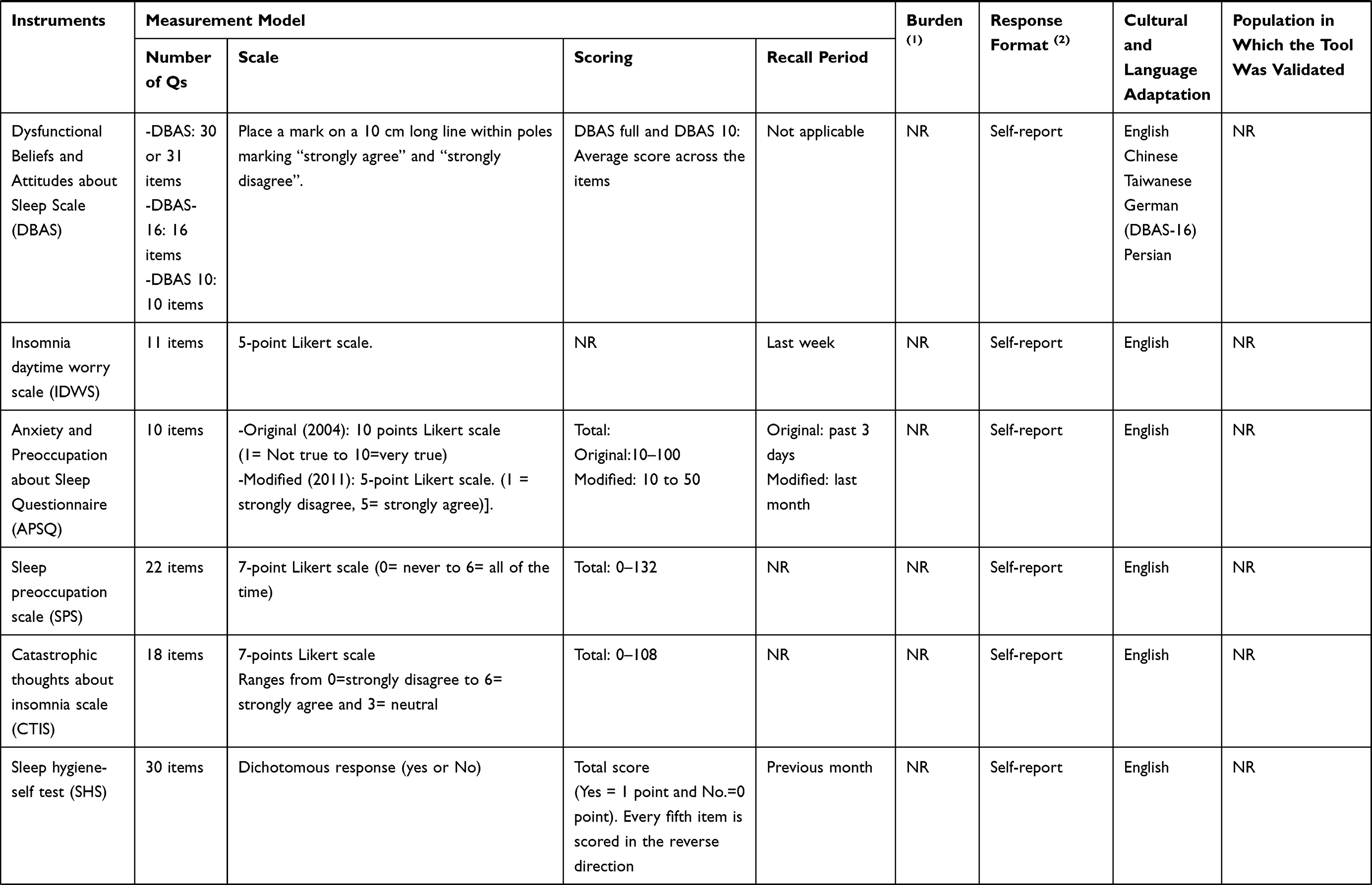 |
Table 2 Characteristics of Sleep Instruments Extracted from Selected Studies (n=112) |
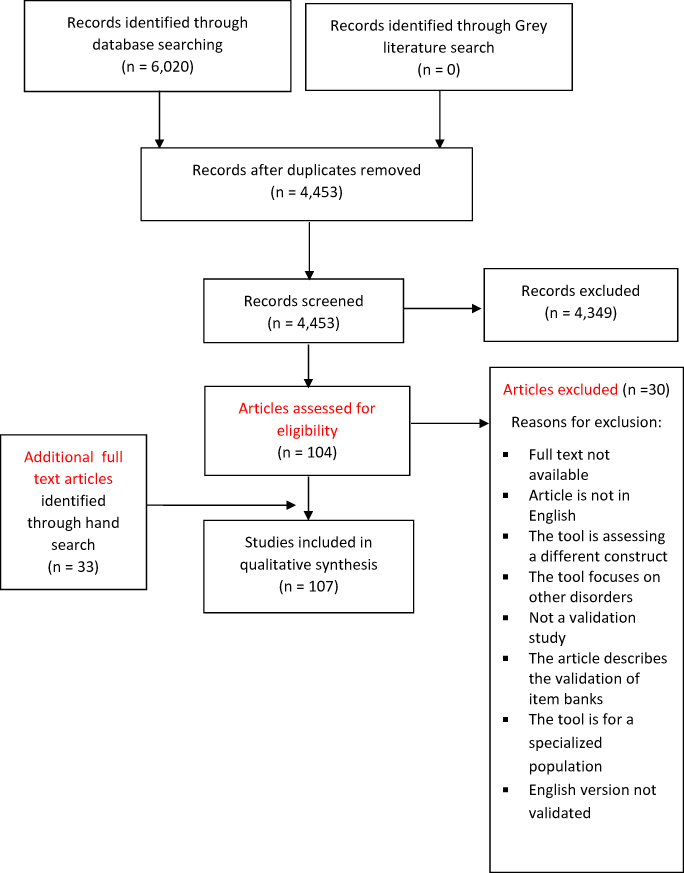 |
Figure 1 Flow chart of the systematic review process. |
As summarized in Tables 1 and 2, the majority of the instruments identified contain less than 20 items. The longest of these instruments is the Sleep Practices and Attitudes Questionnaire (SPAQ), which contains 151 questions divided into 16 different domains.75 While the Karolinska Sleepiness Scale (KSS),24 the Minimal Insomnia Symptoms Scale (MISS),25,26 and the Jenkins Sleep Scale (JSS)27–73 are the shortest instruments identified, consisting of one, three, and four questions, respectively. Some of the instruments have multiple versions, each consisting of a different number of questions [eg, the Functional Outcomes of Sleep Questionnaire (FOSQ)-30 and the FOSQ-10 have 30 and 10 questions, respectively].74,28 The majority of the instruments use Likert-type scales as response options to generate scores. The time needed to complete an instrument was not reported in the majority of the studies reviewed. However, the response burden, wherever reported, did not exceed 10 minutes. The recall period for the majority of the instruments was one month, except for the Insomnia Severity Index (ISI)29,30 and the the Sleep Functional Impact Scale (SFIS)31 which had a recall period of 2 weeks and 1 week, respectively. Only four of the identified instruments were available in Arabic, three of which (PSQI,32 ISI,33 and ESS34) were originally developed in English, but translated and validated in Arabic-speaking populations. The Arabic Scale of Insomnia (ASI)35 is the only instrument which was originally developed in Arabic.
The instruments were classified into four categories based on the outcomes that were assessed in the 107 studies, as follows: (1) instruments screening for insomnia symptoms (n=14); (2) instruments assessing consequences of poor sleep (n=8); (3) instruments assessing the cognitive aspect of insomnia (n=5) and; (4) instruments evaluating sleep hygiene (n=4). A detailed description of the reported psychometric properties for the four categories of sleep instruments retrieved from the studies included in this review is provided in Table 3.
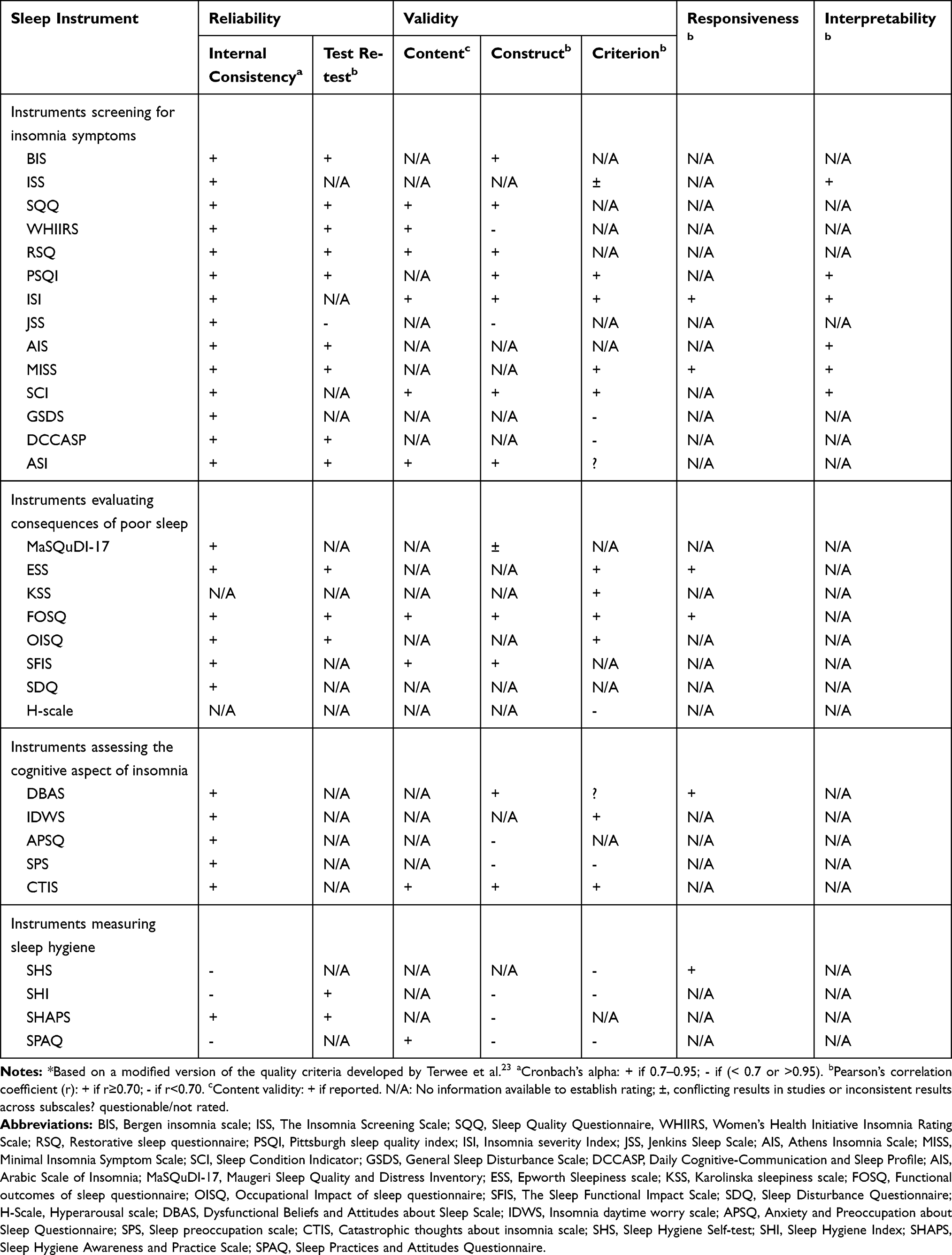 |
Table 3 Quality Assessment of Extracted Sleep Instruments* (n=31) |
Instruments Screening for Insomnia Symptoms
From the 14 instruments screening for insomnia symptoms, two [the Women’s Health Initiative Insomnia Rating Scale (WHIIRS)36,37 and the Restorative Sleep Questionnaire (RSQ)38] were dimension-specific and focus on evaluating the sleep quality through assessing problems with initiation and maintenance of sleep. The remaining 12 instruments were multidimensional, assessing sleep quality and consequences of poor sleep. Some of the identified instruments also measure other specific dimensions such as satisfaction with sleep in the Bergen Insomnia Scale (BIS)39 and sleep environment in the Insomnia Screening Scale (ISS).40 While the Daily Cognitive-Communication and Sleep Profile (DCCASP)41 measures the daily fluctuation in sleep quality and evaluates the impact of these fluctuations on the individual’s cognitive functioning and communication, while the General Sleep Disturbance Scale (GSDS)42,43 assesses sleeping patterns and the use of sleep aids during the past month.
Instruments Assessing Consequences of Poor Sleep
These instruments measure an individual’s functioning and daytime performance. Two of these instruments [the Epworth Sleepiness Scale (ESS44–46 and the KSS)24,47 focus on assessing sleepiness only, whereas the Hyperarousal Scale (H-Scale)48,49 also assesses daytime alertness. Three instruments, the FOSQ,74,28 Occupational Impact of Sleep Questionnaire (OISQ),50 and the Sleep Functional Impact Scale (SFIS),31 evaluate the effects of insomnia on overall functioning. Conversely, the Sleep Disturbance Questionnaire (SDQ)51 evaluates factors which contribute to poor sleep, and the Maugeri Sleep Quality and Distress Inventory (MaSQuDI-17)52 measures the emotional burden of insomnia.
Instruments Assessing Cognitive Aspects of Insomnia
These were in line with the ICD-10 criteria which identifies preoccupation with sleepiness and excessive worry about the consequences of insomnia during the day as one of the clinical features for insomnia.53 Four of these instruments [Insomnia Daytime Worry Scale (IDWS),54 Anxiety and Preoccupation about Sleep Questionnaire (APSQ),55,56 Sleep Preoccupation Scale (SPS)57] evaluate the extent of worry about insomnia. The Dysfunctional Beliefs and Attitudes about Sleep Scale (DBAS) explores individuals’ perceptions and beliefs regarding insomnia.51,58,59 While the Catastrophic Thoughts about Insomnia Scale (CTIS)60 assess exaggerated thinking about insomnia and the severity of the consequences.
Instruments Assessing Sleep Hygiene
Out of the four instruments included under this category [Sleep Hygiene Index (SHI),61 Sleep Hygiene Awareness and Practice Scale (SHAPS),62 Sleep Hygiene Self-test (SHS)63 and the SPAQ75], only the SPAQ is a comprehensive instrument which evaluates sleep quality, quantity, consequences of poor sleep, and sleep hygiene. The SHS also evaluates the effects of interventions which are expected to improve sleep hygiene, and is the only sleep-hygiene instrument which has been validated for responsiveness. The SHAPS measures knowledge about sleep hygiene in addition to behaviors surrounding sleep.
Some of the sleep instruments which were validated in the 107 articles included in this review, such as the BIS,39 Sleep Condition Indicator (SCI),64 ISS, Athens Insomnia Scale (AIS)65,66 and Sleep Hygiene Index (SHI)61 were developed in accordance with international diagnostic criteria for insomnia such as the International Classification of Sleep Disorders 2nd edition (ICSD-II), International Classification of Diseases 10th edition (ICD-10), and the Diagnostic and Statistical Manual of Mental Disorders (DSM). The majority of these instruments were validated among university students and in primary insomniacs.
Many of the identified sleep instruments have been translated and culturally adapted in variety of languages, such as the Pittsburgh Sleep Quality Index (PSQI),67–69 ISI, and ESS which are available in 18, 10, and 6 languages, respectively.
Quality Assessment
The majority of the instruments used in the 107 studies included in this review did not meet all of the eight criteria set by the SAC-MOT.22 However, the conceptual and measurement models were specified for all instruments.Additionally, the reliability of sleep measures was usually reported in the validation studies, particularly the internal consistency reliability was reported for all instruments, except for the H-scale and the KSS. The reported internal consistency values for the sleep and sleep hygiene instruments across the studies included in this systematic review ranged between 0.53 and 0.97.
As outlined in Table 3, the test-retest reliability was only reported for 15 of the 31 instruments. Validity measures were reported for almost all of the instruments identified (29 out of 31), of which criterion validity was the most commonly reported and content validity the least reported validity measure. The generalizability of the psychometric properties reported was examined for three instruments (ISS, ISI and AIS) in community samples and primary insomniacs. Only six instruments (MaSQuDI-17, ESS, FOSQ, DBAS, APSQ, SPS) provided evidence of discriminating capacity between healthy individuals and poor sleepers. As summarized in Table 1, some of the sleep instruments were tested for other validity measures such as incremental validity, diagnostic validity, and external validity.40,64-67,70,76 Additionally, the SHS was the only instrument that was assessed for responsiveness to change in sleep hygiene after interventions.46 With the exception of SHAPS, all of these instruments had low internal consistency (α < 0.7) and only the SHI and the SHAPS were evaluated for their reproducibility.75,61–63
Discussion
This study identified 31 sleep instruments and described in detail their psychometric properties as described in 107 validation and cultural adaptation studies. In the validation studies included in this review, only the ISI, FOSQ and MISS were evaluated for all four psychometric properties such as responsiveness, interpretability, reliability and validity.25,73-28,69,76 Because most validation studies try measuring the same construct in different settings, it was expected that the sleep instruments in these studies were mostly tested for their reliability. For the most part, the sleep instruments identified in this systematic review had good internal consistency with Cronbach’s alpha values ≥0.7, which is in line with the recommended threshold for adequate reliability reported in the literature.77 However, overall lower Cronbach’s alpha values were reported for instruments measuring sleep hygiene. It has been suggested that the low internal consistency identified for sleep hygiene measures could be due to the definition of sleep hygiene, which consists of different factors (not necessarily related) that have the potential for negatively affecting sleep.61 Thus, items in sleep hygiene instruments may appear to be poorly related in the internal consistency test. This suggests that when assessing the psychometric properties of sleep hygiene instruments, the use of other validity and reliability measures is recommended to avoid depending on Cronbach’s alpha values alone.
The validation studies included in this systematic review reported on the reproducibility of only 15 out of the 31 instruments identified. Mostly were assessed through the test-retest reliability method. However, the time frame between the two measurements was highly variable, ranging between 2 days and 6 months.27,69 There is still no consensus in the literature on the best time interval for reproducibility tests. Findings from studies that compared between different time intervals suggests that test results from an interval of 2 days and 2 months are similar to those resulting from a 2-weeks’ interval.78,79
Criterion validity was the most commonly reported validity measure in the studies included in this review. Concurrent validity (which compares the score of the instrument to that of a gold standard which assesses the same construct) was evaluated for 18 out of the 31 sleep instruments identified, whereas the predictive validity (which provides evidence of an instrument’s ability to forecast a particular outcome in the future) was assessed only for 5 instruments. Considering that most of the validation studies included in this review were done on newly developed instruments, not prioritizing on assessing their predictive validity is understandable. Some of the validation studies such as those done on ISI, RSQ and PSQI, compared the scores generated by the instruments to non-subjective assessment tools such as the PSG.29,37,65 The quality criteria for questionnaires developed by Terwee et al recommends providing the reasons for selecting a measure to be a gold standard in a validation study.23 However, in the studies included in this systematic review, the choice of the instrument to be used as a comparator or as a gold standard was rarely justified. In situations where a gold standard measure is not available, construct validity could be used to assess the instrument’s validity.80 This is the case for some of the instruments included in this review, such as the RSQ, APSQ and SHAPS, which evaluate new sleep-related concepts for which gold standards are not available.
The diagnostic validity of an instrument is an important measure, particularly for clinicians, as it examines the extent to which the instrument can accurately differentiate between healthy individuals and insomniacs at a specific score.81 Diagnostic validity was reported for only five of the instruments identified in this review (specifically the PSQI, ISI, AIS, MISS and the SCI). Incremental validity (which describes the ability of an instrument to predict a variable of interest beyond what is possible by other existing instruments) was only tested for the Sleep Quality Questionnaire (SQQ).62 This measure is important as it facilitates the comparison between different instruments and provides evidence of which instrument is superior.
The selection of an insomnia instrument in practice is also affected by factors such as the length of the instrument, the time required for completion and the languages in which it is available. Around half of the instruments identified in this review consisted of ten questions or less, and those assessing the cognitive aspects of insomnia or sleep hygiene were usually longer. However, the duration required for completion was not commonly reported. Only six instruments were available in more than three languages, and only four in Arabic language.34 The limited availability of instruments in Arabic language offers a valuable opportunity for researchers interested in sleep medicine in the Arab region to translate and validate these instruments.
Despite the comprehensiveness of this systematic review, the time elapsed between the initial database search and the publication of the results is an important limitation. To address this, a supplementary literature search using the same search strategy and databases was undertaken in April 2020, which identified additional validation studies and 7 new instruments including: the Insomnia Catastrophising Scale (ICS),82,83 the Single-item sleep quality scale (SQS),84 the Lebanese insomnia scale (LIS-18),85 the Daytime Sleepiness Perception Scale-4 (DSPS-4),86 the Indian Sleepiness Scale (InSS),87 Athlete Sleep Behavior Questionnaire (ASBQ),88 and the Non-restorative Sleep Scale (NRS)89. These findings are indicative that the improvement in scientists’ understanding of insomnia pathophysiology has been associated with a parallel increase in the development of instruments which measure different aspects of sleep dysfunction and related risk factors. Researchers also appear to be acknowledging the cultural effects on sleep behaviors and insomnia perception, as two of the newly developed instruments (LIS-18 and InSS) were developed to describe sleep from a non-Western perspective. Comparing between the psychometric properties of insomnia instruments across different populations is interesting and could be the focus of a future investigation. In addition, because this systematic review was focused on identifying instruments that assess the symptoms of insomnia, daytime consequences and those related to sleep hygiene, instruments assessing arousal before sleep only such as the Pre-Sleep Arousal Scale (PSAP)90,91 were excluded.
Conclusion
Different instruments are available for evaluating various aspects of sleep and sleep hygiene. The validity and reliability of most of these instruments have been tested and are well established. However, psychometric testing for several of the available sleep instruments remains incomplete, particularly responsiveness and interpretability. Our findings suggest that future studies should focus on reporting more psychometric measures to ensure the trustworthiness of the findings generated by these instruments. The number of sleep instruments available in languages other than English including Arabic are limited, indicating a need to translate and culturally adapt many of these instruments into various languages to be available for use in clinical practice and research in different populations.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hirshkowitz M, Whiton K, Albert SM, et al. National sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Heal J Natl Sleep Found. 2014;1(1):40–43. doi:10.1016/j.sleh.2014.12.010
2. Roth T. Insomnia: definition, prevalence, etiology, and consequences. J Clin Sleep Med. 2007;3(5Suppl):S7–S10.
3. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387–1394. doi:10.1378/chest.14-0970
4. Ferrie JE, Kumari M, Salo P, Singh-Manoux A, Kivimaki M. Sleep epidemiology-a rapidly growing field. Int J Epidemiol. 2011;40:1431–1437. doi:10.1093/ije/dyr203
5. Wong WS, Fielding R. Prevalence of insomnia among Chinese adults in Hong Kong: a population‐based study. J Sleep Res. 2011;20(1pt1):117–126. doi:10.1111/j.1365-2869.2010.00822.x
6. Hiller RM, Johnston A, Dohnt H, Lovato N, Gradisar M. Assessing cognitive processes related to insomnia: a review and measurement guide for Harvey’s cognitive model for the maintenance of insomnia. Sleep Med Rev. 2015;23:46–53. doi:10.1016/j.smrv.2014.11.006
7. Pillai V, Drake CL. Sleep and repetitive thought: the role of rumination and worry in sleep disturbance. In: Babson KA, Feldne M, editors. Sleep and Affect: Assessment, Theory, and Clinical Implications. San Diego: Elsevier Academic Press; 2015:201–225. doi:10.1016/B978-0-12-417188-6.00010-4
8. Jefferson CD, Drake CL, Scofield HM, et al. Sleep hygiene practices in a population-based sample of insomniacs. Sleep. 2005;28(5):611–615. doi:10.1093/sleep/28.5.611
9. Gellis LA, Park A, Stotsky MT, Taylor DJ. Associations between sleep hygiene and insomnia severity in college students: cross-sectional and prospective analyses. Behav Ther. 2014;45(6):806–816. doi:10.1016/j.beth.2014.05.002
10. Brick CA, Seely DL, Palermo TM. Association between sleep hygiene and sleep quality in medical students. Behav Sleep Med. 2010;8(2):113–121. doi:10.1080/15402001003622925
11. Seun-Fadipe CT, Aloba OO, Oginni OA, Mosaku KS. Sleep hygiene index: psychometric characteristics and usefulness as a screening tool in a sample of Nigerian undergraduate students. J Clin Sleep Med. 2018;14(8):1285–1292. doi:10.5664/jcsm.7256
12. Krystal AD. Sleep and psychiatric disorders: future directions. Psychiatr Clin North Am. 2006;29(4):
13. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135(1):10–19. doi:10.1016/j.jad.2011.01.011
14. Meng L, Zheng Y, Hui R. The relationship of sleep duration and insomnia to risk of hypertension incidence: a meta-analysis of prospective cohort studies. Hypertens Res. 2013;36(11):985–995. doi:10.1038/hr.2013.70
15. Cappuccio FP, D’Elia L, Strazzullo P, Miller MA. Quantity and quality of sleep and incidence of type 2 diabetes: a systematic review and meta-analysis. Diabetes Care. 2010;33(2):414–420. doi:10.2337/dc09-1124
16. Van de Water A, Holmes A, Hurley DA. Alternatives to polysomnography objective measurements of sleep for non-laboratory settings as alternatives to polysomnography – a systematic review. J Sleep Res. 2011;20(1pt2):183–200. doi:10.1111/j.1365-2869.2009.00814.x
17. Martin JL, Hakim AD. Wrist actigraphy. Chest. 2011;139(6):1514–1527. doi:10.1378/chest.10-1872
18. Buysse DJ, Yu L, Moul DE, et al. Development and validation of patient-reported outcome measures for sleep disturbance and sleep-related impairments. Sleep. 2010;33(6):29–33. doi:10.1093/sleep/33.6.781
19. Klingman KJ, Jungquist CR, Perlis ML. Questionnaires that screen for multiple sleep disorders. Sleep Med Rev. 2016;1–8. doi:10.1016/j.smrv.2016.02.004
20. Ji X, Liu J. Subjective sleep measures for adolescents: a systematic review. Child Care Heal Dev. 2016;42(6):825–839. doi:10.1111/cch.12376
21. Devine EB, Hakim Z, Green J. A systematic review of patient-reported outcome instruments measuring sleep dysfunction in adults. Pharmacoeconomics. 2005;23(9):889–912. doi:10.2165/00019053-200523090-00003
22. Lohr KN. Assessing health status and quality-of-life instruments: attributes and review criteria. Qual Life Res. 2002;11(3):193–205. doi:10.1023/A:1015291021312
23. Terwee CB, Bot SDM, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
24. Akerstedt T. Subjective and objective sleepiness in the active individual. Intern J Neurosci. 1990;52:29–37. doi:10.3109/00207459008994241
25. Broman JE, Smedje H, Mallon L, Hetta J. The minimal insomnia symptom scale (MISS): a brief measure of sleeping difficulties. UPS J Med Sci. 2008;113(2):131–142. doi:10.3109/2000-1967-221
26. Westergren A, Broman JE, Hellstrom A, Fagerstrom C, Willman A, Hagell P. Measurement properties of the minimal insomnia symptom scale as an insomnia screening tool for adults and the elderly. Sleep Med. 2015;16(3):379–384. doi:10.1016/j.sleep.2014.10.016
27. Jenkins CD, Stanton BA, Niemcryk SJ, Rose RM. A scale for the estimation of sleep problems in clinical research. J Clin Epidemiol. 1988;41(4):313–321. doi:10.1016/0895-4356(88)90138-2
28. Weaver TE, Chasens ER, Ratcliffe SJ, Development of the FOSQ-10: a short version of the functional outcomes of sleep questionnaire. Sleep. 2009;32(7):915–919. doi:10.1093/sleep/32.7.915
29. Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/S1389-9457(00)00065-4
30. Morin CM, Belleville G, Bélanger L, Ivers H, The insomnia severity index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601–608.
31. Bell C, McLeod LD, Nelson LM, Fehnel SE, Zografos LJ, Bowers B, Development and psychometric evaluation of a new patient-reported outcome instrument measuring the functional impact of insomnia. Qual Life Res. 2011;20(9):1457–1468. doi:10.1007/s11136-011-9885-8
32. Suleiman KH, Yates BC, Berger AM, Pozehl B, Meza J. Translating the pittsburgh sleep quality index into Arabic. West J Nurs Res. 2010;32(2):250–268. doi:10.1177/0193945909348230
33. Suleiman KH, Yates BC. Translating the insomnia severity index into Arabic. J Nurs Sch. 2011;43(1):49–53. doi:10.1111/j.1547-5069.2010.01374.x
34. Ahmed AE. Validation of Arabic versions of three sleep surveys. Qatar Med J. 2014;2014(2):130–136. doi:10.5339/qmj.2014.20
35. Abdel-Khalek AM. The development and validation of the Arabic scale of insomnia (ASI). Sleep Hypn. 2008;10(1):3–10.
36. Levine DW, Kaplan RM, Kripke DF, Bowen DJ, Naughton MJ, Shumaker SA. Factor structure and measurement invariance of the women’s health initiative insomnia rating scale (study a). Psychol Assess. 2003;15(2):123–136. doi:10.1037/1040-3590.15.2.123
37. Levine DW, Kripke DF, Kaplan RM, et al. Reliability and validity of the women’s health initiative insomnia rating scale (study b). Psychol Assess. 2003;15(2):137–148. doi:10.1037/1040-3590.15.2.137
38. Drake CL, Hays RD, Morlock R, et al. Development and evaluation of a measure to assess restorative sleep. J Clin Sleep Med. 2014;10(7):733–741. doi:10.5664/jcsm.3860
39. Pallesen S, Bjorvatn B, Nordhus IH, Sivertsen B, Hjornevik M, Morin CM. A new scale for measuring insomnia: the bergen insomnia scale. Percept Mot Ski. 2008;107(3):691–706. doi:10.2466/pms.107.3.691-706
40. Yeh ZT, Chiang RP, Kang SC, Chiang CH. Development of the insomnia screening scale based on ICSD-II. Int J Psychiatry Clin Pr. 2012;16(4):259–267. doi:10.3109/13651501.2011.640938
41. Fung CHL, Nguyen M, Moineddin R, Colantonio A, Wiseman-Hakes C. Reliability and validity of the daily cognitive–communication and sleep profile: a new instrument for monitoring sleep, wakefulness and daytime function. Int J Methods Psychiatr Res. 2014;23(2):217–228. doi:10.1002/mpr.1422
42. Lee KA. Self-reported sleep disturbances in employed women. Sleep. 1992;15(6):493–498. doi:10.1093/sleep/15.6.493
43. Lee SY, Validating the General Sleep Disturbance Scale among Chinese American parents with hospitalized infants. J Transcult Nurs. 2007;18(2):111–117. doi:10.1177/1043659606298502
44. Johns MW. A new method for measuring daytime sleepiness: the epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
45. Johns MW. Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep. 1992;15(4):376–381. doi:10.1093/sleep/15.4.376
46. Johns MW. Sleepiness in different situations measured by the epworth sleepiness scale. Sleep. 1994;17(8):703–710. doi:10.1093/sleep/17.8.703
47. Reyner L, Horne J. Falling asleep whilst driving: are drivers aware of prior sleepiness? Int J Leg Med. 1998;111(3):120–123. doi:10.1007/s004140050131
48. Pavlova M, Berg O, Gleason R, Walker F, Roberts S, Regestein Q. Self-reported hyperarousal traits among insomnia patients. J Psychosom Res. 2001;51(2):435–441. doi:10.1016/S0022-3999(01)00189-1
49. Regestein QR, Dambrosia J, Hallett M, Murauski B, Paine M. Daytime alertness in patients with primary insomnia. Am J Psychiatry. 1993;150:
50. David B. Sleep Quality and Daytime Functioning in Primary Insomnia: A Prospective Study. Loughbrgh Univ Institutional Repos; 2008.
51. Espie CA, Inglis SJ, Harvey L, Tessier S. Insomniacs’ attributions psychometric properties of the dysfunctional beliefs and attitudes about sleep scale and the sleep disturbance questionnaire. J Psychosom Res. 2000;48(2):141–148. doi:10.1016/S0022-3999(99)00090-2
52. Morrone E, Sguazzin C, Bertolotti G, et al. Development and validation of the Maugeri sleep quality and distress inventory (MaSQuDI-17). PLoS One. 2017;12(7):e0180743. doi:10.1371/journal.pone.0180743
53. World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: WHO; 1992.
54. Kallestad H, Hansen B, Langsrud K, Hjemdal O, Stiles TC. Psychometric properties and the predictive validity of the insomnia daytime worry scale: a pilot study. Cogn Behav Ther. 2010;39(2):150–157. doi:10.1080/16506070903115317
55. Jansson-Frojmark M, Harvey AG, Lundh LG, et al. Psychometric properties of an insomnia-specific measure of worry: the anxiety and preoccupation about sleep questionnaire. Cogn Behav Ther. 2011;40(1):65–76. doi:10.1080/16506073.2010.538432
56. Tang NKY, Harvey AG. Correcting distorted perception of sleep in insomnia: a novel behavioural experiment? Behav Res. 2004;42(1):27–39. doi:10.1016/S0005-7967(03)00068-8
57. Ellis J, Mitchell K, Hogh H. Sleep preoccupation in poor sleepers: psychometric properties of the sleep preoccupation scale. J Psychosom Res. 2007;63(6):579–585. doi:10.1016/j.jpsychores.2007.07.011
58. Edinger JD, Wohlgemuth WK. Psychometric comparisons of the standard and abbreviated DBAS-10 versions of the dysfunctional beliefs and attitudes about sleep questionnaire. Sleep Med. 2001;2(6):493–500. doi:10.1016/S1389-9457(01)00078-8
59. Chung KF, Ho FYY, Yeung WF. Psychometric comparison of the full and abbreviated versions of the dysfunctional beliefs and attitudes about sleep scale. J Clin Sleep Med. 2016;12(6):821–828. doi:10.5664/jcsm.5878
60. Tan LO, Hadjistavropoulos T, MacNab YC. The catastrophic thoughts about insomnia scale (CTIS): development and validation. Cognit Ther Res. 2016;41(1):143–154. doi:10.1007/s10608-016-9804-y
61. Mastin DF, Bryson J, Corwyn R. Assessment of sleep hygiene using the sleep hygiene index. J Behav Med. 2006;29(3):223–227. doi:10.1007/s10865-006-9047-6
62. Brown FC, Buboltz W
63. Blake DD, Gómez MH, A scale for assessing sleep hygiene: preliminary data. Psychol Rep. 1998;83(3 Pt 2):1175–1178. doi:10.2466/PR0.83.7.1175-1178
64. Espie CA, Kyle SD, Hames P, Gardani M, Fleming L, Cape J. The sleep condition indicator: a clinical screening tool to evaluate insomnia disorder. BMJ Open. 2014;4:3. doi:10.1136/bmjopen-2013-004183
65. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. Athens insomnia scale: validation of an instrument based on ICD-10 criteria. J Psychosom Res. 2000;48(6):555–560. doi:10.1016/S0022-3999(00)00095-7
66. Soldatos CR, Dikeos DG, Paparrigopoulos TJ. The diagnostic validity of the Athens Insomnia Scale. J Psychosom Res. 2001;55(3):263–267. doi:10.1016/S0022-3999(02)00604-9
67. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
68. Grandner MA, Kripke DF, Yoon IY, Youngstedt SD. Criterion validity of the pittsburgh sleep quality index: investigation in a non-clinical sample. Sleep Biol Rhythms. 2006;4(2):129–136. doi:10.1111/j.1479-8425.2006.00207.x
69. Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F. Test-retest reliability and validity of the pittsburgh sleep quality index in primary insomnia. J Psychosom Res. 2002;53(3):737–740. doi:10.1016/S0022-3999(02)00330-6
70. Kato T. Development of the sleep quality questionnaire in healthy adults. J Heal Psychol. 2013;19(8):977–986. doi:10.1177/1359105313482168
71. Ohayon MM, Smirne S. Prevalence and consequences of insomnia disorders in the general population of Italy. Sleep Med. 2002;3(2):115–120. doi:10.1016/S1389-9457(01)00158-7
72. Jerlock M, Gaston-Johansson F, Kjellgren KI, Welin C. Coping strategies, stress, physical activity and sleep in patients with unexplained chest pain. BMC Nurs. 2006;5(1):7. doi:10.1186/1472-6955-5-7
73. Nasermoaddeli A, Sekine M, Kumari M, Chandola T, Marmot M, Kagamimori S. Association of sleep quality and free time leisure activities in japanese and british civil servants. J Occup Health. 2005;47(5):384–390. doi:10.1539/joh.47.384
74. Weaver E, Laizner AM, Evans LK, et al. An instrument to measure functional status outcomes for disorders of excessive sleepiness. Sleep. 1997;20(10):835–843.
75. Grandner MA, Jackson N, Gooneratne NS, Patel NP. The development of a questionnaire to assess sleep-related practices, beliefs, and attitudes. Behav Sleep Med. 2014;12(2):123–142. doi:10.1080/15402002.2013.764530
76. Morin CM, Belleville G, Belanger L, Ivers H. The insomnia severity index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601–608.
77. Frost MH, Reeve BB, Liepa AM, Stauffer JW, Hays RD, Sloan JA. What is sufficient evidence for the reliability and validity of patient-reported outcome measures? Value Health. 2007;10(SUPPL.2):94–105. doi:10.1111/j.1524-4733.2007.00272.x
78. Marx RG, Menezes A, Horovitz L, Jones EC, Warren RF. A comparison of two time intervals for test-retest reliability of health status instruments. J Clin Epidemiol. 2003;56(8):730–735. doi:10.1016/S0895-4356(03)00084-2
79. Chmielewski M, Watson D. What is being assessed and why it matters: the impact of transient error on trait research. J Pers Soc Psychol. 2009;97(1):186–202. doi:10.1037/a0015618
80. Bannigan K, Watson R. Reliability and validity in a nutshell. J Clin Nurs. 2009;18(23):3237–3243. doi:10.1111/j.1365-2702.2009.02939.x
81. Smith GE, Cerhan JH, Ivnik RJ. Diagnostic validity. In: Clinical Interpretation of the WAIS-III and WMS-III. Minnesota: Elsevier Science (USA). 2003;273–300.
82. Jansson-Fröjmark M, Harvey AG, Flink IK. Psychometric properties of the Insomnia Catastrophizing Scale (ICS) in a large community sample. J ofSleep Res. 2012;21(Suppl1):168. doi:10.1080/16506073.2019.1588362
83. Jansson-fröjmark M, Harvey AG, Flink I. Psychometric properties of the Insomnia Catastrophizing Scale (ICS) in a large community sample. Cogn Behav Pract. 2020;49(2):120–136. doi:10.1080/16506073.2019.1588362
84. Snyder E, Cai B, DeMuro C, Morrison MF, Ball W. A new single-item sleep quality scale: results of psychometric evaluation in patients with chronic primary insomnia and depression. J Clin Sleep Med. 2018;14(11):1849–1857. doi:10.5664/jcsm.7478
85. Hallit S, Sacre H, Haddad C, et al. Development of the Lebanese insomnia scale (LIS-18): a new scale to assess insomnia in adult patients. BMC Psychiatry. 2019;19(1):1–11. doi:10.1186/s12888-019-2406-y
86. Marques DR, Gomes AA, de Azevedo MHP. DSPS-4: a brief measure of perceived daytime sleepiness. Curr Psychol. 2019;38(2):579–588. doi:10.1007/s12144-017-9638-0
87. Venkatnarayan K, Krishnaswamy UM, Ramachandran P, Devaraj U. Validation of the Indian sleepiness scale to assess excessive daytime somnolence. Sleep Med. 2019;64:S404. doi:10.1016/J.SLEEP.2019.11.1124
88. Driller MW, Mah CD, Halson SL. Development of the athlete sleep behavior questionnaire: a tool for identifying maladaptive sleep practices in elite athletes. Sleep Sci. 2018;11(1):37–44. doi:10.5935/1984-0063.20180009
89. Wilkinson K, Shapiro C. Development and validation of the Nonrestorative Sleep Scale (NRSS). J Clin Sleep Med. 2013;9(9):929–937. doi:10.5664/jcsm.2996
90. Nicassio FM, Mendlowitz DR, Fussell JJ, Petras L. The henomenology of the pre-sleep state: the development of the pre-sleep arousal scale *. Behav Res Ther. 1985;23(3):263–271. doi:10.1016/0005-7967(85)90004-X
91. Jansson-Fröjmark M, Norell-Clarke A, Jansson-Frojmark M, Norell-Clarke A. Psychometric properties of the Pre-Sleep Arousal Scale in a large community sample. J Psychosom Res. 2012;72(2):103–110. doi:10.1016/j.jpsychores.2011.10.005
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.