")
Back to Journals » Journal of Pain Research » Volume 15
A Systematic Review and Meta-Analysis Protocol on How Best to Use Non-Pharmacologic Therapies to Manage Chronic Low Back Pain and Associated Depression
Authors Guo Y, Ma Q , Zhou X , Yang J , He K, Shen L, Zhao C , Chen Z, Tan CIC, Chen J
Received 29 June 2022
Accepted for publication 15 October 2022
Published 4 November 2022 Volume 2022:15 Pages 3509—3521
DOI https://doi.org/10.2147/JPR.S380058
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Yu Guo,1,* Qingyu Ma,1,* Xuan Zhou,1 Juan Yang,2 Kejie He,3 Longbin Shen,4 Canghuan Zhao,3 Zhuoming Chen,4 Celia Ia Choo Tan,5 Jiaxu Chen1
1Guangzhou Key Laboratory of Formula-Pattern of Traditional Chinese Medicine, School of Traditional Chinese Medicine, Jinan University, Guangzhou City, People’s Republic of China; 2Division of General Internal Medicine, Mayo Clinic, Rochester, MN, USA; 3Department of Acupuncture, First Affiliated Hospital of Jinan University, Guangzhou City, People’s Republic of China; 4Rehabilitation Medicine Center, First Affiliated Hospital of Jinan University, Guangzhou City, People’s Republic of China; 5Department of Physiotherapy, Singapore General Hospital, Singapore, Singapore
*These authors contributed equally to this work
Correspondence: Jiaxu Chen, Guangzhou Key Laboratory of Formula-Pattern of Traditional Chinese Medicine, School of Traditional Chinese Medicine, Jinan University, No. 601 Huangpu Road West, Tianhe District, Guangzhou City, People’s Republic of China, Email [email protected]
Purpose: To evaluate the efficacy of different non-pharmacologic therapies (NPTs) on relieving depressive symptoms and pain intensity in individuals living with chronic low back pain (LBP) and associated depression.
Methods: A comprehensive search of seven English databases and two Chinese databases from inception to the search date will be undertaken. The reference lists of previously published relevant reviews and included trials will also be searched. Only peer-reviewed and published moderate-to-high quality randomized controlled trials (RCTs) for chronic LBP and associated depression treated with NPTs will be considered. Two independent reviewers will identify studies, extract data, assess risk of bias, and evaluate the strength of evidence using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. Meta-analysis will be conducted to estimate the treatment effect of various NPTs. Heterogeneity will be assessed using Cochrane’s Q and the I-squared statistics. Subgroup and sensitivity analyses will be performed to assess the robustness of findings. A funnel plot will be developed to evaluate reporting bias, and Begg’s and Egger’s tests will be used to assess funnel plot symmetries.
Results: This protocol outlines the planned scope and methodology for an upcoming systematic review and meta-analysis, which will provide up-to-date evidence on 1) which NPTs are associated with improvements in depressive symptoms and pain intensity and 2) whether the effects of NPTs on chronic LBP and associated depression vary according to clinical condition, participant, and treatment characteristics.
Conclusion: Our meta-analyses of moderate-to-high quality RCTs will help to develop specific recommendations on prescribing NPTs in patients with chronic LBP and associated depression.
Study Registration: This protocol is registered on the International Platform of Registered Systematic Review and Meta-analysis (INPLASY) protocols platform as record No. INPLASY202260055.
Keywords: non-pharmacologic therapies, chronic low back pain and associated depression, meta-analysis, randomized controlled trial, protocol
Introduction
Low back pain (LBP) is recognized by the World Health Organization as a global health problem, and it is one of the commonest reasons that patients seek healthcare and nursing services worldwide.1,2 LBP is the most prevalent disorder in every country, regardless of income, and it affects all age groups and almost every individual during their lifetimes, either acutely or chronically.3 The number of prevalent cases, incident cases, and years lived with disability (YLD) of LBP have increased substantially from 1990 to 2019, and it remains the leading cause of productivity loss measured in years and was the top cause of YLDs in 2019 worldwide.4 Recent analyses of Global Burden of Disease (GBD) data in 204 countries and territories showed that LBP accounts for the highest burden of 150 musculoskeletal disorders, with approximately 568.4 million prevalent cases, 223.5 million incident cases, and 63.7 million YLDs globally.4 Moreover, GBD data show that the national economic burden from LBP was similar to that of high-cost diseases such as cardiovascular disease, cancer, and autoimmune disease.4 Although the financial and disability costs attributable to LBP substantially differ between countries, a significant and incremental impact on global health-care systems is expected over the coming decades in every country.1,5
With growing concerns about the number of people living with chronic LBP, research efforts have revealed that chronic LBP is a consequence of complex biological, psychological, and social interactions.2,6,7 Many patients with chronic LBP have ongoing and recurrent complaints, with the effects of chronic LBP extending beyond pain and resulting in significant mental health difficulties, including depression;1,8 indeed, people suffering from chronic LBP have a higher prevalence of depression than the general population.9–11 A retrospective cohort study found that those with chronic LBP and comorbid depression used more health-care resources and had more comorbidities such as diabetes, hypertension, chronic obstructive pulmonary disease, and anxiety.12 A one-year prospective cohort study concluded that several psychological features are risk factors for persistent, severe LBP and disability, especially depression and catastrophization.13 In addition, converging evidence indicates that depressive symptoms may aggravate pain intensity, amplify disability, and worsen treatment outcomes in patients with chronic LBP, triggering a vicious cycle of LBP and depression.9 These studies highlight that therapeutic regimens that consider the patient’s psychological profile may be more effective than those that focus on physical symptoms such as pain and disability alone when managing chronic LBP.
According to American College of Physicians guidelines, pharmacologic therapies such as non-steroidal anti-inflammatory drugs (NSAIDs) or muscle relaxants are recommended to manage chronic LBP.14 However, their effect is limited when used long-term, and they are associated with gastrointestinal and cardiovascular adverse events and potential addiction.14 Due to ongoing concerns about the risk to benefit ratio and suboptimal results in clinical trials evaluating pharmacological agents in chronic LBP, recently published guidelines have proposed non-pharmacologic therapies (NPTs) such as exercise and physical therapy as first-line treatments for chronic LBP.15,16 Faced with various NPTs, however, day-to-day clinical decision-making often involves consideration of “effective available treatment options” for the depressive symptoms of individuals living with chronic LBP. For this population with chronic LBP and associated depression, clinical decision-making is hampered by a lack of robust evidence to inform the choice of therapy. Recent reviews have investigated a few selected NPTs for depressive symptoms of individuals living with chronic LBP,17,18 and the effectiveness of many NPTs for this specific patient group remains uncertain. There is therefore a need to provide individuals living with prolonged and persistent LBP with a tailored NPT program when they have depressive symptoms.
Therefore, this systematic review and meta-analysis will not only summarize a variety of NPTs but also evaluate their efficacy in relieving depressive symptoms and pain intensity in individuals living with chronic LBP and associated depression. We will also perform subgroup analyses to identify possible confounders of the effects of NPTs including participant characteristics (eg, gender, age, nationality, occupation, depression severity), chronic LBP characteristics (eg, cause, subtypes, duration, frequency, pain severity), and treatment characteristics (eg, form, duration, and frequency), which would help to establish patient-centered management and recovery.
Materials and Methods
Study Registration
This protocol was developed following guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) statement19 as displayed in the PRISMA-P checklist (Supplementary Table 1). Reporting of the systematic review and meta-analysis itself will adhere to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 guidance.20 To improve transparency, we also registered this protocol in the International Platform of Registered Systematic Review and Meta-analysis (INPLASY) protocols platform (https://inplasy.com/inplasy-2022-6-0055/; DOI: 10.37766/inplasy2022.6.0055) on June 13, 2022. Important protocol amendments, their date, and explanations and reasons for the modification will be documented and justified alongside the results of the final study.
Eligibility Criteria for Study Selection
Eligibility criteria will be established according to the review objectives and the participants, intervention, comparison, outcome, and study design (PICOS) approach.
Study Design
As randomized controlled trials (RCTs) represent the highest level of evidence for unbiased information, only full text articles of peer-reviewed and published moderate-to-high quality RCTs for chronic LBP and associated depression treated with NPTs in English and Chinese, including all relevant parallel-group RCTs including the first phase of crossover trials and cluster-randomized trials, will be considered eligible for this review. Where several publications report findings for the same population, the most comprehensive report including the largest sample size, longest follow-up, complete methods section, and comprehensive reporting of results report will be chosen.
Participants
The study participants of interest will be adult patients (aged ≥18 years) with a definitive diagnosis suggesting chronic LBP and associated depression. Chronic LBP is usually defined as a primary area of pain, stiffness, or muscle tension located typically below the costal margin and above the inferior gluteal folds lasting 12 weeks or more, with or without sciatica (pain radiating from the buttock and downward along the course of the sciatic nerve).1,2 In addition, study participants will also need to meet at least one of the standardized international or domestic approved diagnostic criteria of depression in the original RCT, such as criteria presented in the Diagnostic and Statistical Manual of Mental Disorders (DSM),21,22 International Statistical Classification of Diseases and Related Health Problems (ICD),23 or Chinese Classification of Mental Disorders (CCMD).24 We will not apply restrictions regarding gender, ethnicity, education, nationality, occupation, and economic status and cause, subtypes, duration, intensity, frequency, and severity of chronic LBP.
Interventions
Any NPT commonly used to treat chronic LBP and associated depression will be eligible for this review. According to current American College of Physicians Clinical Practice Guidelines and the Cochrane Back and Neck Group, eligible non-pharmacologic therapies include but are not limited to non-specific exercise and related therapies (eg, walking, swimming, running, stretching, aerobics), mind-body and body awareness exercise (eg, yoga, tai chi, Qigong, Pilates, motor control exercise, the Alexander technique, mindfulness-based stress reduction), manual therapy (eg, spinal manipulation and spinal mobilization), acupuncture (eg, manual acupuncture, electroacupuncture, laser acupuncture, scalp acupuncture, dry needling), massage/Tuina (eg, soft tissue massage, acupressure), physical therapies (eg, interferential therapy, low-level laser therapy, lumbar support, shortwave diathermy, superficial heat, traction, transcutaneous electric nerve stimulation, ultrasonography), psychological therapies (eg, cognitive-behavioral therapy, operant therapy, behavioral therapy, self-regulatory therapy), basic patient education (eg, back school, brief educational intervention, advice on importance of staying active, reassurance, McKenzie therapy), patient pain neuroscience education (educational sessions that describe the neurobiology and neurophysiology of pain), or multidisciplinary rehabilitation (packages that include coordinated delivery of interventions from across different disciplinary practices/clinics, typically consisting of physical and psychological therapy, eg, education + physiotherapy + exercise + counselling).15,16
Comparators
Control interventions will be no treatment, waiting lists, or pharmacological therapies. The following comparisons will be considered: (1) NPT alone versus no treatment or waiting lists; (2) NPT alone versus pharmacological therapy alone; (3) NPT plus pharmacological therapy versus non-pharmacologic therapy alone; and (4) NPT plus pharmacological therapy versus pharmacological therapy alone. We will exclude trials comparing only different types of NPT or different treatment doses with the same intervention.
Outcome Measures
The primary outcome will be a reduction in the degree of depressive symptoms and pain intensity at the end of the treatment period. Degree of depressive symptoms will be measured as a continuous variable according to the Hamilton Depression Rating Scale (HAMD),25 Beck Depression Inventory (BDI),26 Self-Rating Depression Scale (SDS),27 Montgomery-Åsberg Depression Rating Scale (MADRS),28 Patient Health Questionnaire-9 (PHQ-9),29 or any other depressive symptoms rating scale with evidence of adequate validity and reliability. Pain intensity will be measured as a continuous variable on any validated scale such as a Visual Analogue Scale (VAS),30 Numeric Rating Scale (NRS),30 McGill Pain Questionnaire (MPQ),31 or other rating scale with evidence of adequate validity and reliability.
The secondary outcomes will include:
- Total effective rate (as a dichotomous outcome): defined as the proportion of participants with a clinically relevant improvement according to a predefined change in validated depressive symptom and pain intensity rating scales at the end of the treatment period.
- Back pain-related function: measured as a continuous variable on any validated scale such as the Roland-Morris Disability Questionnaire (RMDQ),32 Oswestry Disability Index (ODI),33 Hanover Functional Ability Questionnaire (HFAQ),34 or other rating scale with evidence of adequate validity and reliability at the end of the treatment period.
- Health-related Quality of Life (HRQoL): measured as a continuous variable on any validated HRQoL scale such as the Medical Outcomes Study 36/12-Item Short-Form Health Survey (SF-36/12),35,36 Brief Form of the World Health Organization’s Quality of Life Questionnaire (WHOQOL-BREF),37 Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q),38 Nottingham Health Profile (NHP),39 or other well-recognized HRQoL scales with evidence of adequate validity and reliability at the end of the treatment period.
- Acceptability (dichotomous outcome): defined as the proportion of participants who drop out of the study for any reason during treatment delivery.
- Tolerability (dichotomous outcome): defined as the proportion of participants who discontinued treatment due to any adverse events during treatment delivery.
- Safety (dichotomous outcome): defined as the proportion of participants who experienced at least one adverse effect during treatment delivery.
When available, we will extract data obtained at baseline, after the intervention, and at all reported follow-up time points classified as short-term (0–3 months post-intervention), intermediate-term (3–6 months post-intervention), and long-term (>6 months post-intervention).
The exclusion criteria will be: (1) studies not published in English or Chinese; (2) studies with vague diagnostic or evaluation criteria; (3) studies with missing or incomplete data and duplicate publications; (4) the intervention was not an NPT; (5) studies with other designs or publication types such as quasi-RCTs, retrospective studies, cohort studies, case series or reports, animal model studies, laboratory studies, reviews, commentaries, editorials, letters, expert experience, practice guidelines, abstracts, study protocols, and conference articles; (6) trials in which the sample size is unknown or the total sample size is <20.
Data Sources and Search Strategy
Studies will be identified through a literature search from inception to search date in the following seven English electronic databases: 1) PubMed; 2) Embase; 3) Scopus; 4) Web of Science; 5) Cumulative Index to Nursing and Allied Health Literature (CINAHL); 6) Cochrane Library; and 7) Physiotherapy Evidence Database and two Chinese electronic databases: 1) China National Knowledge Internet (CNKI) and 2) Wanfang Data. To obtain more comprehensive evidence, three main subject heading domains will be combined with the AND operator: one to designate the clinical LBP condition (chronic LBP), the second to designate the depression condition (depression), and the third to designate the study type (RCT). To retrieve all potentially relevant studies, a combination of medical subject headings (MeSH) and free-text words related to chronic LBP, depression, and RCTs will be used. Keywords and subject terms will be customized for each database and any necessary adjustments made prior to running the search. The retrieval will be conducted with no restrictions regarding the year but limited to English or Chinese. If discrepancies occur, a consensus will be reached through consultation. The details of the search strategy for PubMed and EMBASE database are shown in Supplementary Tables 2 and 3.
In addition, the reference lists of previously published relevant reviews and included RCTs will be manually searched to identify any other eligible publications missed by electronic searching. We will not include grey literature due to the high risk of bias from a lack of peer review. The search will be repeated prior to the publication of the review in an aim to include any potentially eligible study that might have been published after the initial search.
Study Selection
Considering that there may be some differences between two independent reviewers in the understanding of eligibility criteria for study selection, calibration exercises and inter-rater agreement analysis (Cohen’s kappa (κ)) will be conducted to evaluate consistency and accuracy of study selection between reviewers using SPSS v26.0 software (IBM Statistics, Armonk, NY, USA). The chi-squared test will be used to analyze and obtain kappa (κ) values. Statistically, a κ value between 0.75 and 1 indicates high consistency and, to ensure high consistency, when the κ value is ≥0.8, study selection will be carried out by the two independent reviewers. Two reviewers (YG and YQM) will independently use EndNote X20 citation management software (Thomson Reuters, New York, USA) to identify all potentially relevant clinical studies and sequentially screen their titles, abstracts, and keywords for eligibility after removing duplicates and apparently irrelevant studies. Studies will be excluded if both reviewers consider that the study does not meet eligibility criteria. Comprehensive reading of the full text will be conducted for further assessment if there are studies that cannot clearly be included based on the title, abstract, and keywords. Full-text versions of all relevant studies will be obtained and reviewed to ensure that the studies meet the inclusion criteria. After ensuring that the RCTs meet the eligibility criteria, we will further exclude low-quality RCTs that scored <4 on the improved Jadad scale (0–3 indicating low quality, 4–5 moderate quality, and 6–7 high quality).40 Any discrepancies will be resolved through discussion between the two reviewers, and any ongoing disagreement will be adjudicated by a third reviewer (XZ). According to the PRISMA 2020 guidance,38 the study selection procedure flow diagram is summarized in Figure 1.
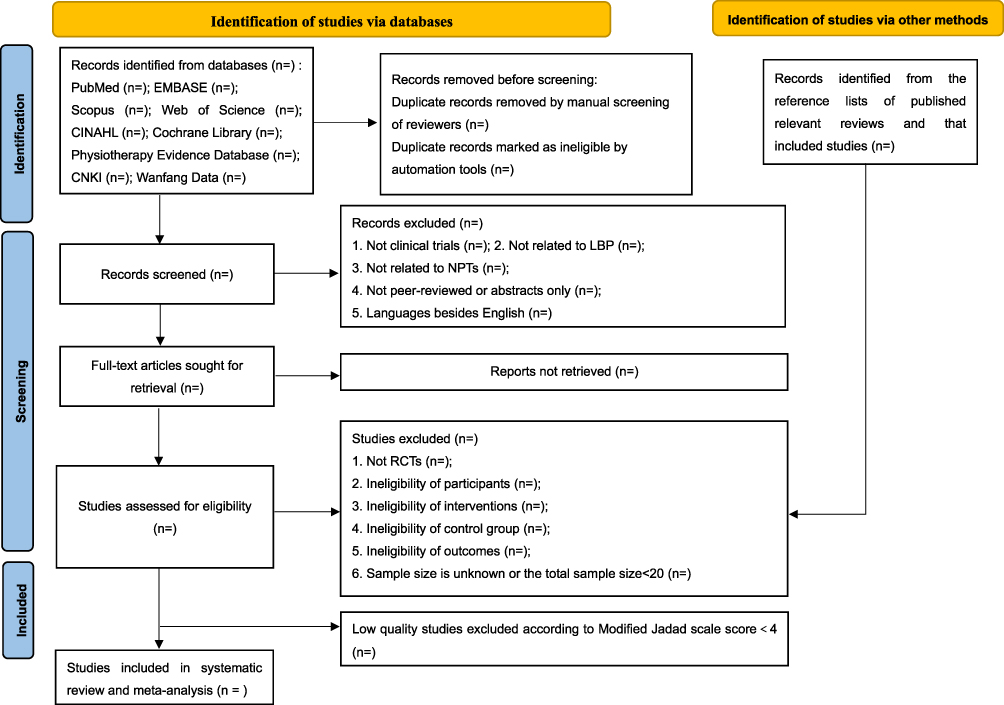 |
Figure 1 Study selection procedure of flow diagram. |
Data Extraction and Collection
According to the inclusion criteria, a standardized electronic data extraction form will be prepared prior to data extraction. For studies fulfilling the inclusion criteria, two reviewers (YG, QYM) will independently extract data from the included RCTs, including study details (article title, first author, publication year, publication source, publication language, country, setting), study design (eligibility criteria, recruitment method, randomization method, allocation concealment method, blinding method, measuring time points, follow-up period), notes (financial source, competing interests), participant characteristics (number of arms, sample size, gender proportion, mean age, diagnostic criteria, baseline chronic LBP condition, baseline degree of depressive symptoms), intervention and comparison characteristics (type, frequency, number of sessions, session duration, total period in the intervention, type of comparison, details of comparison), outcome data (methods of outcome assessment, primary outcomes, secondary outcomes), and conclusions (key findings of the study). These are illustrated in Tables 1–4.
 |
Table 1 Basic Characteristics of the Included RCTs |
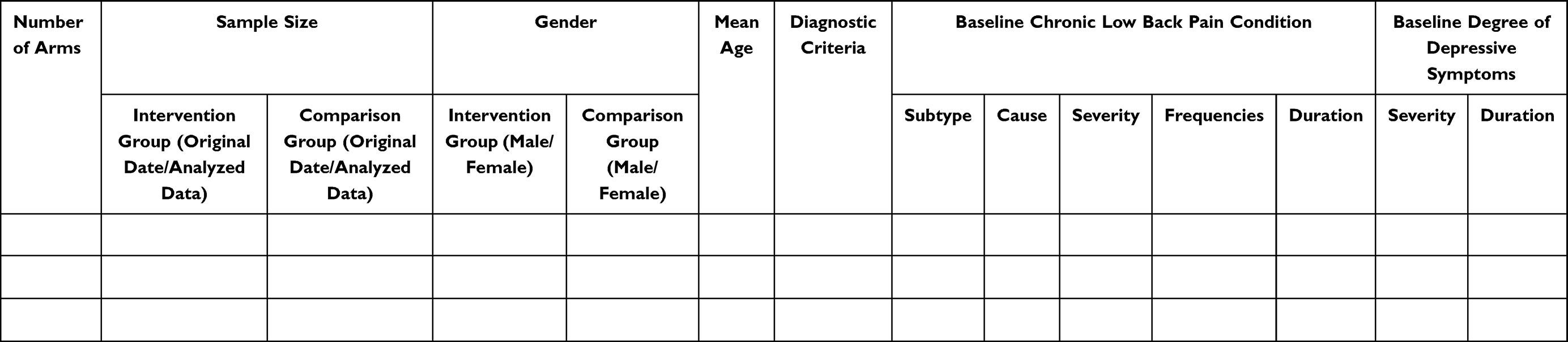 |
Table 2 Summary of the Participant Characteristics |
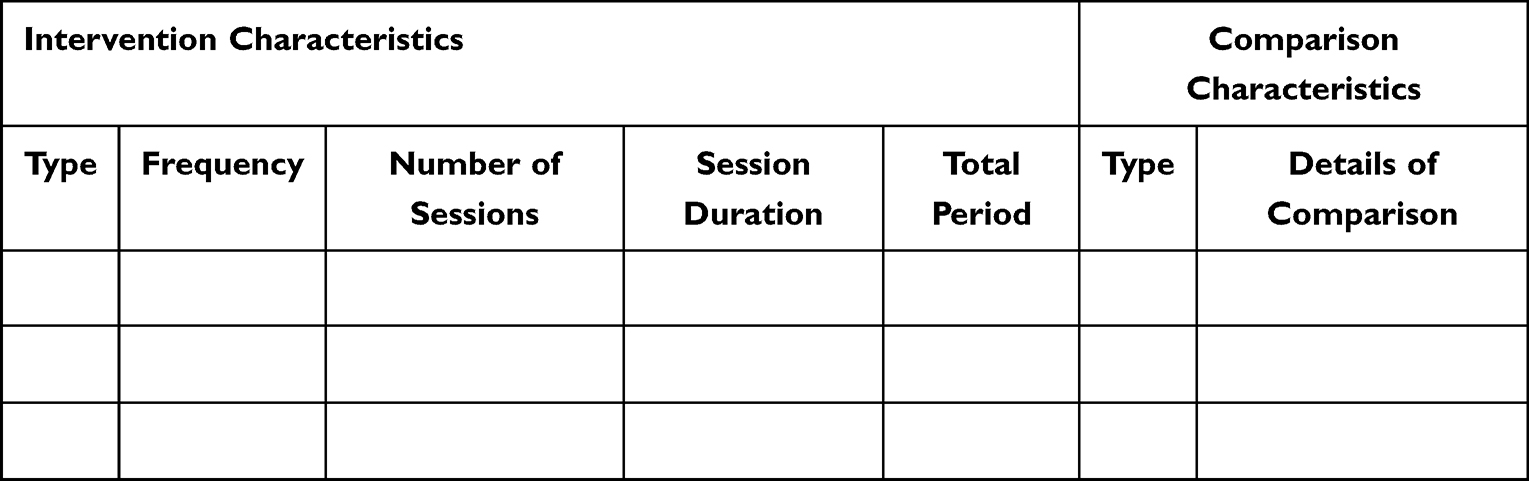 |
Table 3 Summary of the Intervention/Comparison Characteristics |
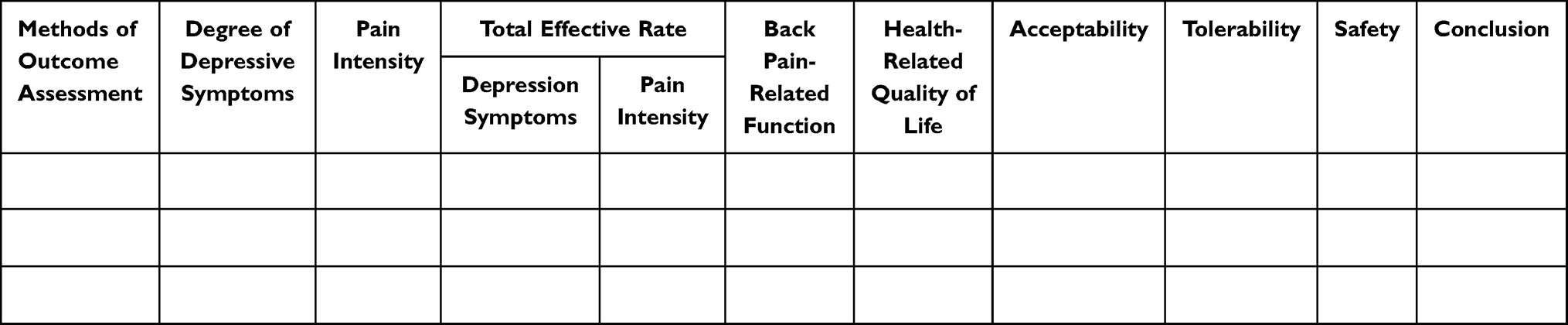 |
Table 4 Summary of the Outcome Characteristics |
Where study reports allow, we will use data from the intention-to-treat analysis. Any disagreements will be resolved through discussion between the two reviewers (YG and YQM), with discrepancies and uncertainties resolved by consulting a third reviewer (YZ). In cases of missing data, the authors of eligible studies will be contacted to obtain complete information. All data will be cross-checked and transferred into Review Manager (RevMan) software version 5.4 software (Cochrane, London, UK).
Risk of Bias Assessment
The methodological quality of each eligible study will be assessed by two independent reviewers (YG and YQM) according to the Revised Cochrane Collaboration’s Risk of Bias (RoB) v2.0 tool.41 This version is structured into five domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. Each domain includes several signaling questions that elicit information relevant to an assessment of risk of bias. Based on the answers to all signaling questions, we will obtain an overall risk of bias judged as low risk of bias, some concerns, or a high risk of bias considering the risk of bias judgement in five domains.41 Any discrepancy in the methodological quality assessment between the two reviewers (YG and YQM) will be resolved through arbitration by discussion. If the disagreement persists, a third reviewer (XZ) will be consulted to reach consensus.
Dealing with Missing Data
If any data are missing from the included studies, we will first contact the first and/or corresponding authors by email, telephone, or other means to request missing data and/or additional information. If sufficient information remains unobtainable in this way, we will try to use the available coefficients to calculate the data. The potential impact of missing data on the results will be tested in sensitivity analyses and will be explained in the final review.
Data Analysis
Eligible RCTs and results will be qualitatively summarized. If more than three studies evaluate similar treatments and outcomes, a meta-analysis will be performed using RevMan v5.4 software (Cochrane, London, UK) to estimate the treatment effect.42,43 For meta-analyses, we will include studies that score ≥4 on the improved Jadad scale (range 0–7),40 since these studies can be regarded as having sufficient similarity in clinical characteristics and high methodological quality. We will adopt the Mantel-Haenszel random-effects model for all meta-analyses due to the broad spectrum of non-pharmacologic intervention components in the included studies.42,43
The pooled estimates of the weighted mean difference (WMD) or the standard mean difference (SMD) with 95% confidence intervals (CIs) will be calculated for continuous outcomes. WMD will be used for data measured on the same scales and for which the same assessment instrument is used. SMD will be used if all studies assess the same outcome but measure it in various ways.42,43 For dichotomous outcomes, data will be analyzed using the risk ratio (RR) with 95% CIs.42,43 Throughout the analyses, two-sided tests will be used, and a P-value <0.05 will be considered statistically significant.42,43 Between-group effect sizes will be calculated using Hedges’ g statistic, the magnitude of which can be interpreted as small (0.2), medium (0.5), or large (0.80).42 If data are not available or insufficient for quantitative analysis, the evidence and findings will be summarized in a written narrative.
Statistical heterogeneity will be assessed based on Cochran’s Q statistic and its related P-value.42 Furthermore, the I-squared statistic (I2 index) will be used as a measure to categorize heterogeneity across the included RCTs, where I2 values range from 0% to 100%; studies with P-values >0.1 and I2 index values <50% will be regarded as having no statistical heterogeneity.42 When the P-value is ≤0.1 and I2 index is ≥50%, the study will be considered to have substantial heterogeneity.42 I2 indices of 75%, 50%, and 25% represent high, moderate, and low levels of heterogeneity, respectively.42
Subgroup Analysis
Where sufficient data are available in the included RCTs, RevMan version 5.4 (Cochrane, London, UK) and STATA version 14.0 (Stata Corp., College Station, TX) statistical software packages will be used to carry out subgroup analyses and multiple meta-regressions for relevant outcomes to investigate possible sources of heterogeneity including in the following characteristics: publication year; publication language; setting; sample size; gender; age; nationality; ethnicity; occupation; baseline degree of depressive symptoms; diagnostic criteria; cause, subtypes, severity, frequencies, and duration of chronic LBP; format, frequency, and number of sessions; session duration; total period of intervention, type of comparison; time-point of outcomes; duration of follow-up; and the methodological quality of the selected RCTs.
Sensitivity Analysis
Sensitivity analyses will be performed for relevant outcomes to explore the robustness and reliability of the review conclusions where feasible. Meta-analysis will be repeated by excluding each related study with a small sample size, a high risk of bias, and incomplete results one at a time and re-evaluating the effect size.42 If the results are inconsistent, they will be discussed, and caution will be taken when drawing conclusions.
Reporting Bias Assessment
RevMan version 5.4 (Cochrane, London, UK) and STATA version 14.0 (Stata Corp., College Station, TX) statistical software packages will be used to assess reporting bias. Potential reporting bias will be assessed by visually inspecting contour-enhanced funnel plots44 and with Begg’s and Egger’s tests45 if sufficient studies are included. A funnel plot is a graphical illustration showing the relationship between study size and effect size. In general, a plot that resembles a symmetrical inverted funnel suggests the absence of publication bias.44 Begg’s and Egger’s tests will be used to quantify the publication bias captured in the funnel plot. Two-sided P-values >0.05 in Begg’s and Egger’s tests indicate no publication bias.45 When Begg’s test and Egger’s test results are inconsistent, conclusions will be based on Egger’s test due to its higher sensitivity.45
Confidence Assessment
Two independent reviewers (YG and YQM) will utilize the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework to evaluate the overall quality of evidence.46 The strength of evidence will be judged as “high” (further research is unlikely to change our conclusion), “moderate” (further research is likely to alter our conclusion), or “low” and “very low” (further studies are required to answer the research question with a high degree of confidence/increase confidence) on the basis of limitations in study design and implementation, unexplained heterogeneity or inconsistency of effect results, indirectness of evidence, inaccuracies in the results, and a high probability of publication bias.46 These assessments will be cross-checked by two reviewers (YG and YQM) and will be generated in GRADEprofiler (GRADEpro) version 3.6.1 (Evidence Prime, Ontario, Canada). Any discrepancy will be resolved by consensus or consultation with a third reviewer (XZ).
Ethical Considerations
This study is being conducted using systematic review and meta-analysis methods with existing trial data. Since no private and confidential patient data will be contained in the reporting, there are no ethical considerations associated with this protocol.
Discussion
Previous reviews have compared the efficacy and safety of different NPTs in patients with chronic LBP. Their aim was to comprehensively and objectively guide clinical decision-making with respect to efficacy, harm reduction, and cost efficiency based on patient preference.15,16,47,48 Nevertheless, most of these studies focused on evaluating the effects of various NPTs on pain intensity, physical function, and HRQoL without considering heterogeneity in patient characteristics, not least with respect to the treatment and management of chronic LBP in the presence of associated depression, reducing the applicability of the results in practice. This review endeavors to overcome these problems by establishing: (1) whether to adopt NPTs in individuals living with chronic LBP and associated depression; (2) which types and characteristics of NPTs can improve depressive symptoms and pain intensity in individuals living with chronic LBP and associated depression; (3) whether the effects of NPTs on depressive symptoms and pain intensity vary according to baseline chronic LBP, associated depression, and participant and treatment characteristics. These results will guide precise decisions and facilitate clinical/shared decision-making between clinicians and patients on effective and appropriate strategies or interventions when using NPTs to manage chronic LBP and associated depression.
This study has a number of strengths. First, this review is being reported according to the PRISMA-P statement,19 and the consequent systematic review and meta-analysis will be conducted according to PRISMA 2020 guidance.20 Second, we will only include the “gold standard” of clinical trials – RCTs - and then use the improved Jadad scale to exclude low-quality RCT to improve the reliability of the conclusions. Third, our study will provide a comprehensive comparison of the effects of different NPTs on chronic LBP and associated depression and will provide subgroup analysis according to baseline characteristics, where available. Finally, we will analyze publication bias and use GRADE to provide more robust and targeted evidence in this field to help treatment decision-making.
Nevertheless, the proposed review may have limitations. First, we will rely on studies written in English and Chinese as well as peer-reviewed published data, making the review vulnerable to small-study effects and publication bias. Second, outcomes and measures will be vastly different across studies. However, to overcome this heterogeneity, we will make every effort to include all eligible studies with sufficient data and evaluate standardized mean differences and standardized values as well as compensate variables using meta-regression.
Conclusion
Recent clinical trials and guidelines show that NPTs are effective tools for treating individuals living with chronic LBP. However, there is limited evidence on the effectiveness of NPTs in patients with chronic LBP and associated depression. This systematic review and meta-analysis will provide up-to-date evidence on which NPTs are associated with improvements in depressive and pain symptoms and which patient populations living with chronic LBP and associated depression are more likely to respond to certain types of NPT.
Thus, this study will provide pragmatic support for clinical practice guideline recommendations regarding the use of various NPT-based programs. It will also assist health-care providers and clinical researchers to make effective and appropriate decisions when managing chronic LBP and associated depression, helping them adjust to each unique individual’s needs, characteristics, and functional status. Furthermore, current research gaps will be identified to inform future investigations.
Abbreviations
NPTs, Non-pharmacologic Therapies; LBP, Low Back Pain; RCTs, Randomized Controlled Trials; GRADE, Grading of Recommendations, Assessment, Development and Evaluation; INPLASY, International Platform of Registered Systematic Review and Meta-analysis; YLD, Years Lived with Disability; GBD, Global Burden of Disease; NSAIDs, Non-steroidal Anti-Inflammatory Drugs; PRISMA-P, Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols; PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis; PICOS, Participants, Intervention, Comparison, Outcome, and Study design; DSM, Diagnostic and Statistical Manual of Mental Disorders; ICD, International Statistical Classification of Diseases and Related Health Problems; CCMD, Chinese Classification of Mental Disorders; HAMD, Hamilton Depression Rating Scale; BDI, Beck Depression Inventory; SDS, Self-Rating Depression Scale; MADRS, Montgomery-Åsberg Depression Rating Scale; PHQ-9, Patient Health Questionnaire-9; VAS, Visual Analogue Scale; NRS, Numeric Rating Scale; MPQ, McGill Pain Questionnaire; RMDQ, Roland-Morris Disability Questionnaire; ODI, Oswestry Disability Index; HFAQ, Hanover Functional Ability Questionnaire; HRQoL, Health-related Quality of Life; SF-36/12, Study 36/12-Item Short-Form Health Survey; WHOQOL-BREF, Brief Form of the World Health Organization’s Quality of Life Questionnaire; Q-LES-Q, Quality of Life Enjoyment and Satisfaction Questionnaire; NHP, Nottingham Health Profile; SPSS, Statistical Product Service Solutions; CINAHL, Cumulative Index to Nursing and Allied Health Literature; CNKI, China National Knowledge Internet; MeSH, Medical Subject Headings; RoB, Risk of Bias; RevMan, Review Manager; WMD, Weighted Mean Difference; SMD, Standard Mean Difference; CIs, Confidence Intervals; RR, Risk Ratio; I2 index, I-squared statistic; STATA, Statistical Software for Data Science; GRADEpro, Grading of Recommendations, Assessment, Development and Evaluation Profiler.
Author Contributions
All authors made a significant contribution to this work, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all of these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by a grant from Key-Area Research and Development Program of Guangdong Province [grant number 2020B1111100001], China, and the HEAD Foundation, Singapore. The funding sources had no influence on the study design, data collection, analysis, and interpretation of data or the writing of the manuscript. The corresponding author had full access to all the data in the study and has final responsibility for the decision to submit for publication.
Disclosure
The authors have no conflicts of interest related to this work.
References
1. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–2367. doi:10.1016/S0140-6736(18)30480-X
2. Knezevic NN, Candido KD, Vlaeyen JWS, et al. Low back pain. Lancet. 2021;398(10294):78–92. doi:10.1016/S0140-6736(21)00733-9
3. Cieza A, Causey K, Kamenov K, et al. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2021;396(10267):2006–2017. doi:10.1016/S0140-6736(20)32340-0
4. Collaborators GDaI. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
5. Karran EL, Grant AR, Moseley GL. Low back pain and the social determinants of health: a systematic review and narrative synthesis. Pain. 2020;161(11):2476–2493. doi:10.1097/j.pain.0000000000001944
6. da Menezes Costa L, Maher CG, Hancock MJ, et al. The prognosis of acute and persistent low-back pain: a meta-analysis. Can Med Assoc J. 2012;184(11):E613–E624. doi:10.1503/cmaj.111271
7. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–747. doi:10.1016/S0140-6736(16)30970-9
8. Christe G, Crombez G, Edd S, et al. Relationship between psychological factors and spinal motor behaviour in low back pain: a systematic review and meta-analysis. Pain. 2021;162(3):672–686. doi:10.1097/j.pain.0000000000002065
9. Wong JJ, Tricco AC, Côté P, et al. Association between depressive symptoms or depression and health outcomes for low back pain: a systematic review and meta-analysis. J Gen Intern Med. 2022;37(5):1233–1246. doi:10.1007/s11606-021-07079-8
10. Fernandez M, Colodro-Conde L, Hartvigsen J, et al. Chronic low back pain and the risk of depression or anxiety symptoms: insights from a longitudinal twin study. Spine J. 2017;17(7):905–912. doi:10.1016/j.spinee.2017.02.009
11. Hu Y, Yang Z, Li Y, et al. Prevalence and associated factors of depressive symptoms among patients with chronic low back pain: a cross-sectional study. Front Psychiatry. 2021;12:820782. doi:10.3389/fpsyt.2021.820782
12. Bailes AH, Navlani R, Koscumb S, et al. Use of healthcare resources in patients with low back pain and comorbid depression or anxiety. Spine J. 2021;21(9):1440–1449. doi:10.1016/j.spinee.2021.03.031
13. Ranger TA, Cicuttini FM, Jensen TS, et al. Catastrophization, fear of movement, anxiety, and depression are associated with persistent, severe low back pain and disability. Spine J. 2020;20(6):857–865. doi:10.1016/j.spinee.2020.02.002
14. Chou R, Deyo R, Friedly J, et al. Systemic pharmacologic therapies for low back pain: a systematic review for an American College of physicians clinical practice guideline. Ann Intern Med. 2017;166(7):480–492. doi:10.7326/M16-2458
15. Chou R, Deyo R, Friedly J, et al. Nonpharmacologic therapies for low back pain: a systematic review for an American College of physicians clinical practice guideline. Ann Intern Med. 2017;166(7):493–505. doi:10.7326/M16-2459
16. Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
17. Hoffman BM, Papas RK, Chatkoff DK, et al. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol. 2007;26(1):1–9. doi:10.1037/0278-6133.26.1.1
18. Amaral LKB, Souza MB, Campos MGM, et al. Efficacy of conservative therapy in older people with nonspecific low back pain: a systematic review with meta-analysis and GRADE recommendations. Arch Gerontol Geriatr. 2020;90:104177. doi:10.1016/j.archger.2020.104177
19. Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;350:g7647. doi:10.1136/bmj.g7647
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
21. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).
22. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
23. World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders. Diagnostic Criteria for Research. Geneva, Switzerland: World Health Organization; 1993.
24. Chinese Psychiatric Society. The Chinese Classification of Mental Disorders (CCMD-3).
25. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56–62. doi:10.1136/jnnp.23.1.56
26. Richter P, Werner J, Heerlein A, et al. On the validity of the Beck Depression Inventory. A review. Psychopathology. 1998;31(3):160–168. doi:10.1159/000066239
27. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
28. Soron TR. Validation of Bangla Montgomery Asberg Depression Rating Scale (MADRSB). Asian J Psychiatr. 2017;28:41–46. doi:10.1016/j.ajp.2017.03.019
29. Costantini L, Pasquarella C, Odone A, et al. Screening for depression in primary care with Patient Health Questionnaire-9 (PHQ-9): a systematic review. J Affect Disord. 2021;279:473–483. doi:10.1016/j.jad.2020.09.131
30. Chiarotto A, Maxwell LJ, Ostelo RW, et al. Measurement properties of visual analogue scale, numeric rating scale, and pain severity subscale of the brief pain inventory in patients with low back pain: a systematic review. J Pain. 2019;20(3):245–263. doi:10.1016/j.jpain.2018.07.009
31. Hawker GA, Mian S, Kendzerska T, et al. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011;63(Suppl 11):S240–S252. doi:10.1002/acr.20543
32. Woiciechowsky C. Comparison of endoscopic facet joint denervation to the percutaneous technique regarding efficacy in patients with low back pain: a randomized controlled trial. Spine. 2022;47(17):1187–1193. doi:10.1097/BRS.0000000000004392
33. Rajfur J, Rajfur K, Kosowski Ł, et al. The effectiveness of dry needling in patients with chronic low back pain: a prospective, randomized, single-blinded study. Sci Rep. 2022;12(1):15803. doi:10.1038/s41598-022-19980-1
34. Leonhardt C, Kuss K, Becker A, et al. Graded exposure for chronic low back pain in older adults: a pilot study. J Geriatr Phys Ther. 2017;40(1):51–59. doi:10.1519/JPT.0000000000000083
35. Ware J, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
36. Brazier JE, Harper R, Jones NM, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ. 1992;305(6846):160–164. doi:10.1136/bmj.305.6846.160
37. Su C-T, Ng H-S, Yang A-L, et al. Psychometric evaluation of the Short Form 36 Health Survey (SF-36) and the World Health Organization Quality of Life Scale Brief Version (WHOQOL-BREF) for patients with schizophrenia. Psychol Assess. 2014;26(3):980–989. doi:10.1037/a0036764
38. Rapaport MH, Clary C, Fayyad R, et al. Quality-of-life impairment in depressive and anxiety disorders. Am J Psychiatry. 2005;162(6):1171–1178. doi:10.1176/appi.ajp.162.6.1171
39. Busija L, Pausenberger E, Haines TP, et al. Adult measures of general health and health-related quality of life: medical outcomes study Short Form 36-Item (SF-36) and Short Form 12-Item (SF-12) Health Surveys, Nottingham Health Profile (NHP), Sickness Impact Profile (SIP), Medical Outcomes Study Short Form 6D (SF-6D), Health Utilities Index Mark 3 (HUI3), Quality of Well-Being Scale (QWB), and Assessment of Quality of Life (AQoL). Arthritis Care Res. 2011;63(Suppl 11):S383–S412. doi:10.1002/acr.20541
40. Yeung W-F, Chung K-F, Ng K-Y, et al. A systematic review on the efficacy, safety and types of Chinese herbal medicine for depression. J Psychiatr Res. 2014;57:165–175. doi:10.1016/j.jpsychires.2014.05.016
41. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
42. Cheung MWL, Vijayakumar R. A guide to conducting a meta-analysis. Neuropsychol Rev. 2016;26(2):121–128. doi:10.1007/s11065-016-9319-z
43. Siddaway AP, Wood AM, Hedges LV. How to do a systematic review: a best practice guide for conducting and reporting narrative reviews, meta-analyses, and meta-syntheses. Annu Rev Psychol. 2019;70:747–770. doi:10.1146/annurev-psych-010418-102803
44. Peters JL, Sutton AJ, Jones DR, et al. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J Clin Epidemiol. 2008;61(10):991–996. doi:10.1016/j.jclinepi.2007.11.010
45. Sterne JA, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. 2000;53(11):1119–1129. doi:10.1016/s0895-4356(00)00242-0
46. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
47. Traeger A, Buchbinder R, Harris I, et al. Diagnosis and management of low-back pain in primary care. Can Med Assoc J. 2017;189(45):E1386–E1395. doi:10.1503/cmaj.170527
48. Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. 2018;391(10137):2368–2383. doi:10.1016/S0140-6736(18)30489-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.