")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 12
A Single- and Multiple-Dose Study to Evaluate the Pharmacokinetics of Fixed-Dose Grazoprevir/Elbasvir in Healthy Chinese Participants
Authors Li H, Yang Z, Zhang S, Xu L, Wei Y, Jiang J , Caro L, Feng HP, McCrea JB , Li M, Xie S, Wang J, Zhao XM, Mu S
Received 25 July 2019
Accepted for publication 11 December 2019
Published 11 February 2020 Volume 2020:12 Pages 1—11
DOI https://doi.org/10.2147/CPAA.S224662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Haiyan Li,1 Zhenhua Yang,1 Shuang Zhang,1 Lin Xu,1 Yudong Wei,1 Jun Jiang,2 Luzelena Caro,3 Hwa-Ping Feng,3 Jacqueline B McCrea,3 Meng Li,2 Shuang Xie,2 Jiangdian Wang,2 Xu Min Zhao,2 Shengmei Mu2
1Drug Clinical Trial Center, Peking University Third Hospital, Beijing, People’s Republic of China; 2Department of Infectious Diseases, MSD (China) R&D, Beijing, People’s Republic of China; 3Department of Infectious Diseases, Merck & Co., Inc., Kenilworth, NJ, USA
Correspondence: Haiyan Li
Drug Clinical Trial Center, Peking University Third Hospital, 49 North Garden Road, Haidian District, Beijing 100191, People’s Republic of China
Tel +86 108 226 6226
Email [email protected]
Purpose: The burden of hepatitis C virus infection is particularly high in Asian countries, and new treatments are urgently needed. The purpose of this study was to characterize the pharmacokinetics (PK) and safety of the fixed-dose combination tablet of elbasvir/grazoprevir in healthy Chinese participants.
Patient and Methods: In this Phase I, single-site, open-label, 3-period study in healthy Chinese adults, participants received a single tablet of elbasvir 50 mg/grazoprevir 100 mg, followed by blood sampling for up to 96 hrs (http://www.chinadrugtrials.org.cn/ CTR20160034; Protocol PN071). Participants then received 1 tablet daily for 10 days, followed by a minimum 10-day washout, after which participants received a single dose of 2 tablets (elbasvir 100 mg/grazoprevir 200 mg). Elbasvir and grazoprevir PK were assessed following single and multiple doses. Safety and tolerability were also evaluated.
Results: Twelve participants (50% male) were enrolled in and completed the study. Following single-dose oral administration of elbasvir 50 mg/grazoprevir 100 mg or elbasvir 100 mg/grazoprevir 200 mg, the median Tmax was 3– 4 hrs and elimination half-life was 18 hrs (elbasvir) and 30 hrs (grazoprevir). Multiple-dose administration resulted in AUC0– 24 accumulation ratios of 1.58 (elbasvir) and 2.35 (grazoprevir). Both elbasvir 50 mg/grazoprevir 100 mg and 100 mg/200 mg regimens were generally well tolerated.
Conclusion: Single-dose administration of elbasvir 50 mg/grazoprevir 100 mg or 100 mg/200 mg and once-daily administration of elbasvir 50 mg/grazoprevir 100 mg for 10 days has been adequately characterized, with PK values within the expected range, and was generally well tolerated in healthy Chinese male and female participants.
Keywords: elbasvir, grazoprevir, healthy volunteers, hepatitis C virus, pharmacokinetics
Introduction
Hepatitis C virus (HCV) infection has become a worldwide pandemic, with approximately 150 million people infected globally.1 Across Asia, the burden of disease is particularly high, with prevalence estimates ranging from 0.6% to 1.9% in Japan, 1.0% to 1.9% in China, and up to 5.5% in Taiwan.2,3 However, the prevalence of HCV infection in China is likely to be underestimated due to a lack of national data; most studies to date have been performed in regional cohorts or voluntary blood donor populations.2,3
Epidemiologic studies have indicated that HCV genotype 1 is the most common genotype in Chinese patients, although there is a wide diversity across the country.4,5 The mainstay of treatment in China is pegylated interferon and ribavirin (PEG-IFN/RBV), but both sofosbuvir and the combinations of daclatasvir/asunaprevir, ombitasvir, paritaprevir/ritonavir/dasabuvir, and sofosbuvir/velpatasvir have also received approvals.6–12
Another direct-acting antiviral agent (DAA) is the fixed-dose combination of elbasvir (EBR) and grazoprevir (GZR), approved in the United States, Europe, and Canada for the treatment of HCV genotype 1 and 4 infection, in Japan for the treatment of HCV genotype 1 infection, and in Canada for use in combination with sofosbuvir for the treatment of HCV genotype 3 infection.13–16 The combination of GZR, a once-daily nonstructural protein (NS)3/4A protease inhibitor,17 and EBR, a once-daily NS5A inhibitor,18 has potent antiviral activity in vitro17,18 and has demonstrated high efficacy and favorable tolerability in the treatment of HCV infection in Phase II and Phase III studies, both in treatment-naive and treatment-experienced participants and in participants with or without cirrhosis, with or without chronic kidney disease stage 4/5, and with or without HIV coinfection.19–22 However, EBR and GZR have some established differences in their pharmacokinetics (PK), with drug exposures known to be higher in Asian than in Caucasian people14 and higher in Japanese than in non-Japanese individuals.23 Therefore, the purpose of this study was to characterize the pharmacokinetics of GZR and EBR following single- and multiple-dose administration of the fixed-dose combination tablet (EBR 50 mg/GZR 100 mg) in healthy Chinese participants.
Methods
Ethics
The study was conducted in accordance with principles of Good Clinical Practice and the ethical principles that have their origin in the Declaration of Helsinki, and was approved by the Independent Ethics Committee of Peking University Third Hospital. All patients were required to provide written informed consent to participate in the study.
Study Design and Treatment
This was a Phase I, single-site, open-label, 3-period study (http://www.chinadrugtrials.org.cn/ CTR20160034; Merck protocol MK-5172-071), conducted in China between February and July 2016.
In Period 1, participants received a single tablet of EBR 50 mg/GZR 100 mg on day 1. These doses were selected for assessment because they are the doses contained in the fixed-dose, single-tablet regimen of EBR/GZR that is used clinically for the treatment of HCV infection. Period 2 followed immediately after Period 1 (day 5). In Period 2, participants received 1 tablet of EBR 50 mg/GZR 100 mg daily for 10 days. After a minimum 10-day washout, during Period 3 participants received a single dose of 2 tablets of EBR 50 mg/GZR 100 mg (total of EBR 100 mg/GZR 200 mg). A 2-fold higher dose was used in Period 3 because GZR plasma concentrations are approximately 2-fold higher in HCV-infected people than in non–HCV-infected healthy individuals at steady-state.
All doses of study drug were administered in the fasted (following at least a 10-hr overnight fast) state, in the morning. Each oral dose was administered with approximately 240 mL of room-temperature water.
Participants
Male or female healthy participants aged 18–45 years (inclusive), of Chinese descent (defined as having both biological parents and all 4 biological grandparents born in China and of Chinese descent) and living in China, were eligible for enrollment. Key inclusion criteria were good health with no clinically significant abnormalities, based on medical history and physical and laboratory tests, and body mass index (BMI) between 18 and 24 kg/m2. Participants of reproductive potential were required to remain abstinent or use acceptable methods of birth control throughout the study and for 2 weeks after the study end.
Key exclusion criteria were positivity for hepatitis B virus (HBV) surface antigen or HCV antibodies, or documented human immunodeficiency virus or HBV or HCV infection; any medical condition or prestudy laboratory abnormality that might confound the results of the study or pose unnecessary risk to the patient; estimated creatinine clearance of ≤80 mL/min based on the Cockcroft-Gault equation; use of any medication, including prescription and nonprescription drugs or herbal remedies (such as St. John’s Wort), from 2 weeks prior to study initiation until the final follow-up visit; excessive alcohol or caffeine consumption; smoking or drug abuse within 6 months of screening; and major surgery or blood loss/donation within 4 weeks prior to screening.
Assessments and Analyses
PK parameters following single and multiple doses of EBR 50 mg/GZR 100 mg were assessed in healthy Chinese participants. We also performed a comparison of the pharmacokinetics of EBR (50 mg) and GZR (100 mg) in Chinese individuals from the present study after multiple-dose administration of the EBR/GZR fixed-dose combination versus that in healthy Caucasian individuals receiving single-entity formulations of EBR or GZR in the MK-8742-PN001 and MK-5172-PN001 studies (data on file). These were two Phase I studies (EudraCT numbers 2011-003060-71 and 2009-011502-42) comprising sequential single ascending dose and subsequent multiple ascending dose panels. Both studies were approved by the University of Ziekenhuis ethics committee, Ghent, Belgium, and conducted in accordance with the Declaration of Helsinki and the principles of Good Clinical Practice. All participants provided written informed consent. MK-5172-PN001 was initiated in June 2009 and completed in April 2010, and MK-8742-PN001 was initiated in September 2011 and completed in February 2012. All participants were nonsmoking adult males aged ≥18 years with BMI ≤32 kg/m2 who were in good health based on medical history, physical examination, vital sign measurements, and laboratory safety tests.
For evaluation of pharmacokinetics, blood samples were taken predose, and at 0.5, 1, 2, 3, 4, 6, 8, 12, 16, 24, 48, 72, and 96 hrs postdose in Periods 1, 2, and 3. Plasma GZR concentrations were determined using a validated high-performance liquid chromatographic tandem mass spectrometric (LC-MS/MS) method. The lower limit of quantitation (LLOQ) was 1.0 ng/mL (1.30 nM), and analytical range was 1.00–1000.00 ng/mL (1.30–1300 nM). Assay precision was 3.5%, and accuracy ranged from 95.7% to 102%. Plasma EBR concentrations were also determined using a validated high-performance LC-MS/MS method with an LLOQ of 0.25 ng/mL (0.283 nM) and analytical range of 0.25–500.00 ng/mL (0.283–567 nM). Assay precision was 6.5%, and accuracy ranged from 97.9% to 105.5%. The PK parameters for EBR and GZR were calculated using noncompartmental analysis and included the plasma concentration profile; area under the curve (AUC) from time 0 to infinity (AUC0-∞), AUC from time 0 to 24 hrs (AUC0–24), maximum concentration of the drug (Cmax), concentration of the drug at 24 hrs after dosing (C24), time of maximum concentration (Tmax), apparent total body clearance, volume of distribution/bioavailability, and apparent terminal half-life (t1/2) for single dose; and AUC0–24, Cmax, C24, Tmax, t1/2, and accumulation ratio for multiple-dose administration. Descriptive statistics were provided for each PK parameter. A 95% 2-sided confidence interval (CI) based on t-distribution was constructed for the geometric means of AUC0-∞, AUC0-last, AUC0–24, Cmax, and C24. Accumulation ratios were estimated using Period 1, Day 1, and Period 2, Day 10 data; a 90% 2-sided CI was constructed for the accumulation ratio of AUC0–24, Cmax, and C24 based on a linear mixed-effects model containing a fixed effect for day and a random effect for participant. Individual trough concentration values were natural log-transformed and evaluated with a repeated measures analysis of variance (ANOVA), with time as the repeated (categorical) measure.
Safety was assessed via reporting of adverse events (AEs) and clinical and laboratory evaluations.
Analysis populations included all participants as treated (APaT; participants who received at least 1 dose of study drug), and per protocol (PP; participants who complied with the study protocol). APaT data were used for demographic and baseline information and all safety variables; PP data were used for the PK analyses.
Results
Participant Demographics
A total of 12 healthy Chinese participants were enrolled in the study; all 12 received the assigned study drugs and completed the study per protocol. The APaT and PP populations were identical and comprised all 12 participants. Of these 12 participants, 6 (50%) were men and 6 (50%) were women. Baseline demographics and characteristics are reported in Table 1; the mean age was 33 years, and mean BMI was 22.4 kg/m2.
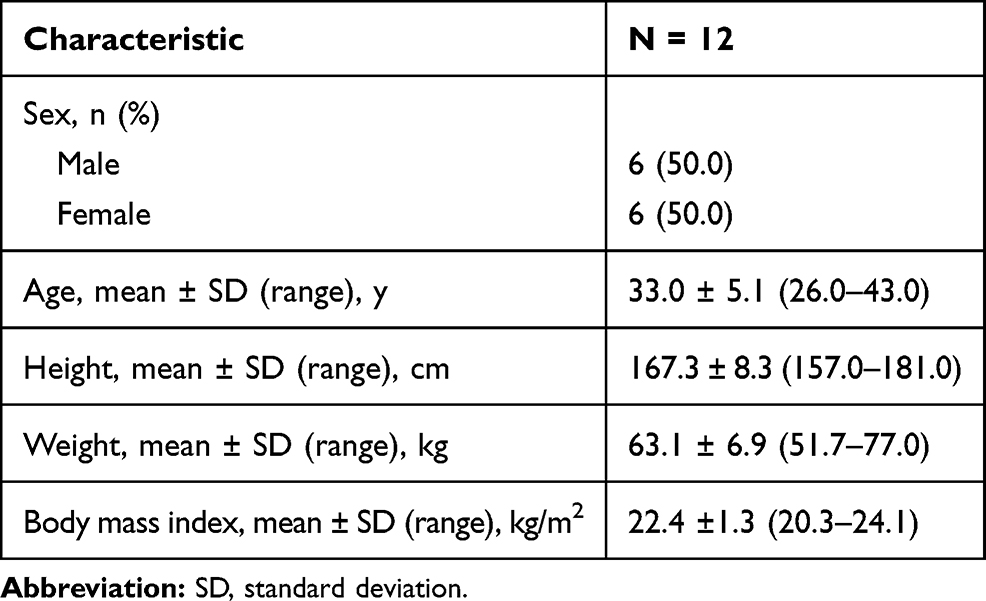 |
Table 1 Participant Demographics and Baseline Characteristics (All Participants as Treated) |
PK Following Single-Dose Administration of Grazoprevir/Elbasvir
Following single-dose administration of EBR 50 mg/GZR 100 mg or EBR 100 mg/GZR 200 mg in healthy Chinese participants, both EBR and GZR were absorbed with a median Tmax of 3–4 hrs (Table 2). Plasma concentrations of EBR and GZR declined bi-exponentially with a geometric mean t1/2 of approximately 18 hrs for EBR and 30 hrs for GZR. Mean t1/2 levels were similar at both dose levels for both drugs. For EBR, the geometric mean values of AUC0-∞ and Cmax were 2.69 h·μM and 0.14 μM, respectively, after administration of EBR 50 mg/GZR 100 mg, and 4.36 h·μM and 0.23 μM after EBR 100 mg/GZR 200 mg. For GZR, the geometric mean values of AUC0-∞ and Cmax were 0.68 h·μM and 0.04 μM, respectively, after administration of EBR 50 mg/GZR 100 mg, and 1.16 h·μM and 0.08 μM after administration of EBR 100 mg/GZR 200 mg. Mean plasma concentration versus time profiles are shown in Figure 1.
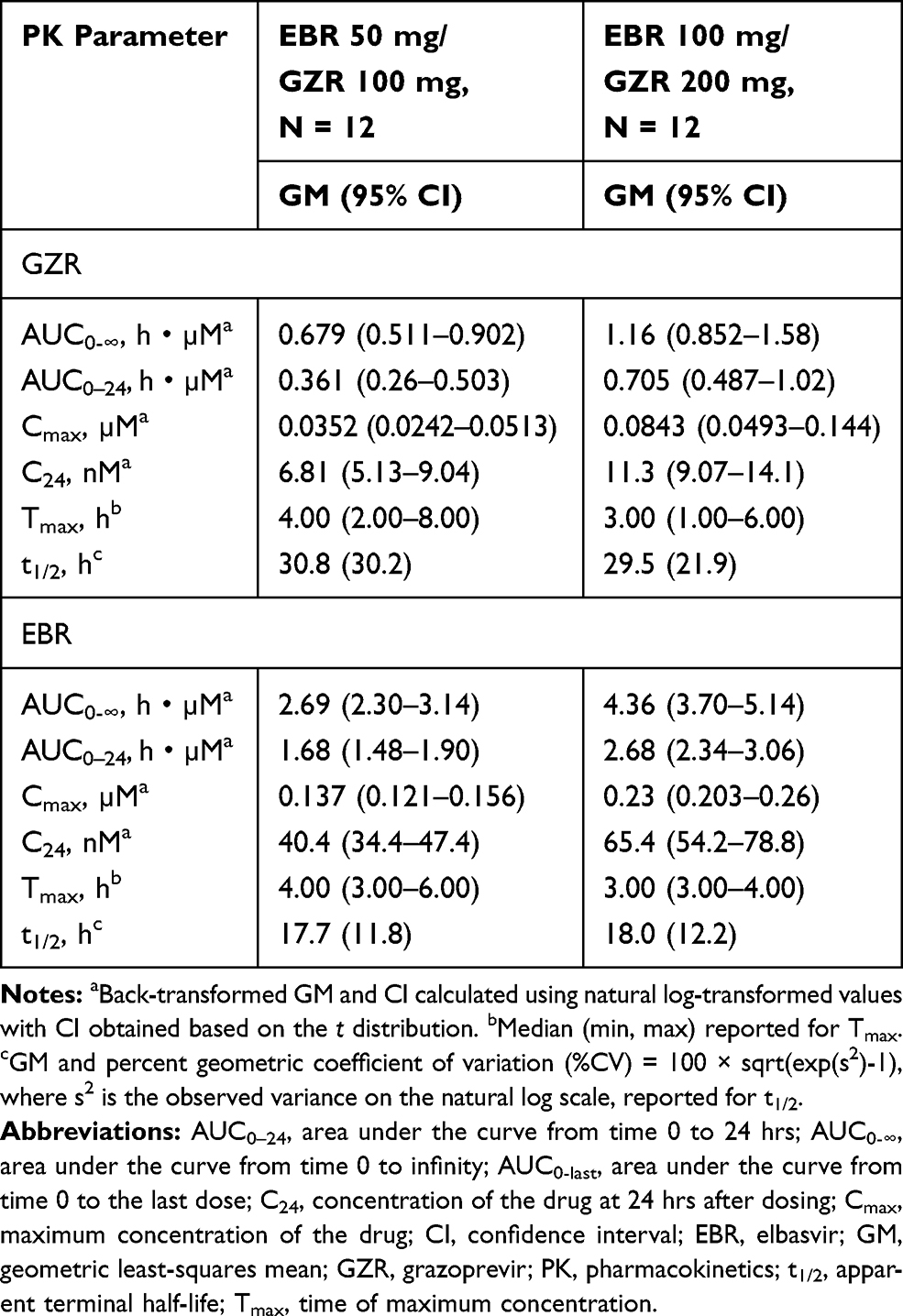 |
Table 2 Pharmacokinetic Parameters of Grazoprevir and Elbasvir Following Single-Dose Oral Administration of Elbasvir 50 mg/Grazoprevir 100 mg or Elbasvir 100 mg/Grazoprevir 200 mg in Healthy Chinese Participants (Per-Protocol Population) |
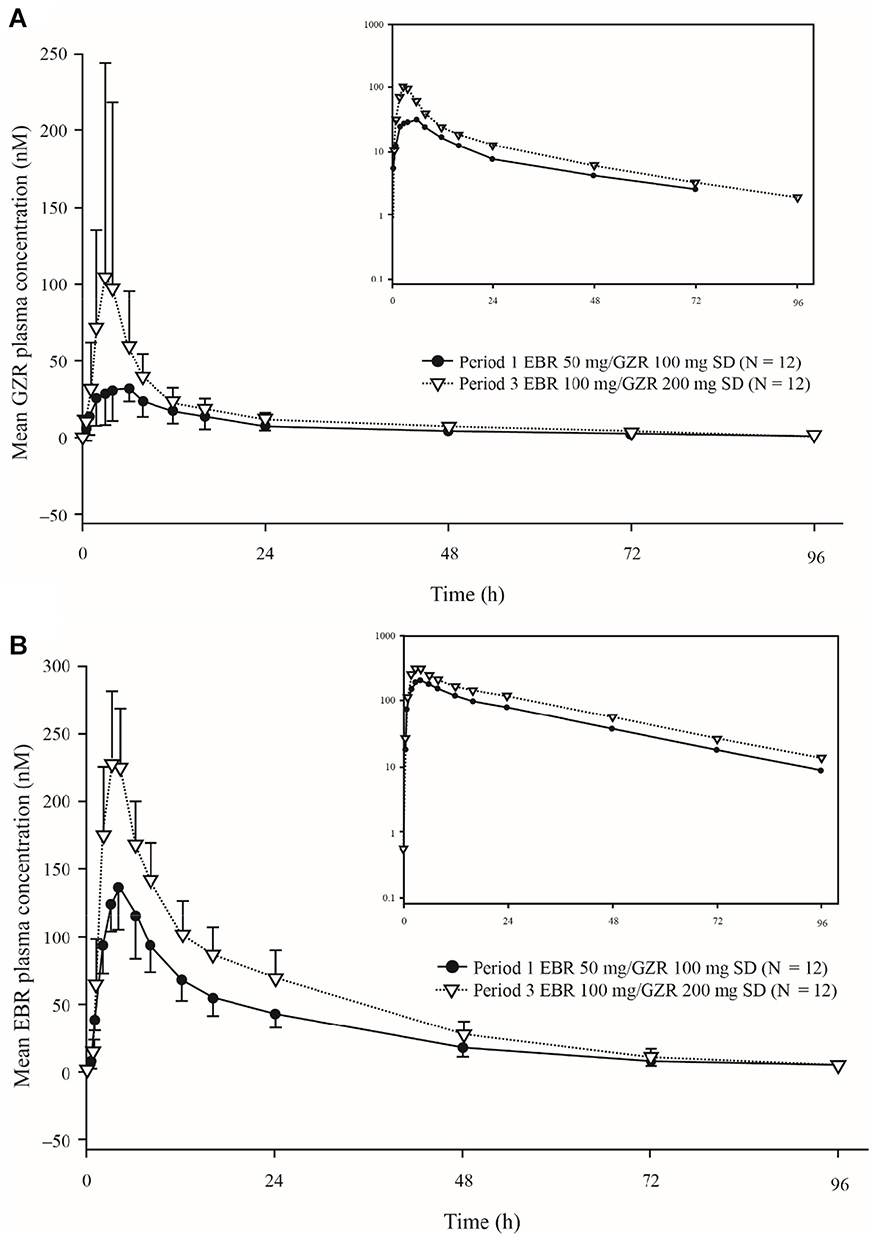 |
Figure 1 Arithmetic mean plasma concentration versus time profiles following single-dose oral administration of elbasvir/grazoprevir on day 1 of Period 1 or on day 1 of Period 3 in healthy Chinese participants (per-protocol population). (A) Grazoprevir; (B) elbasvir. Error bars represent standard deviation. Inset: semi-log scale. Abbreviations: EBR, elbasvir; GZR, grazoprevir. |
PK Following Multiple-Dose Administration of Grazoprevir/Elbasvir
Mean plasma concentration versus time profiles of EBR and GZR following once-daily administration of EBR 50 mg/GZR 100 mg for 10 days are shown in Figure 2.
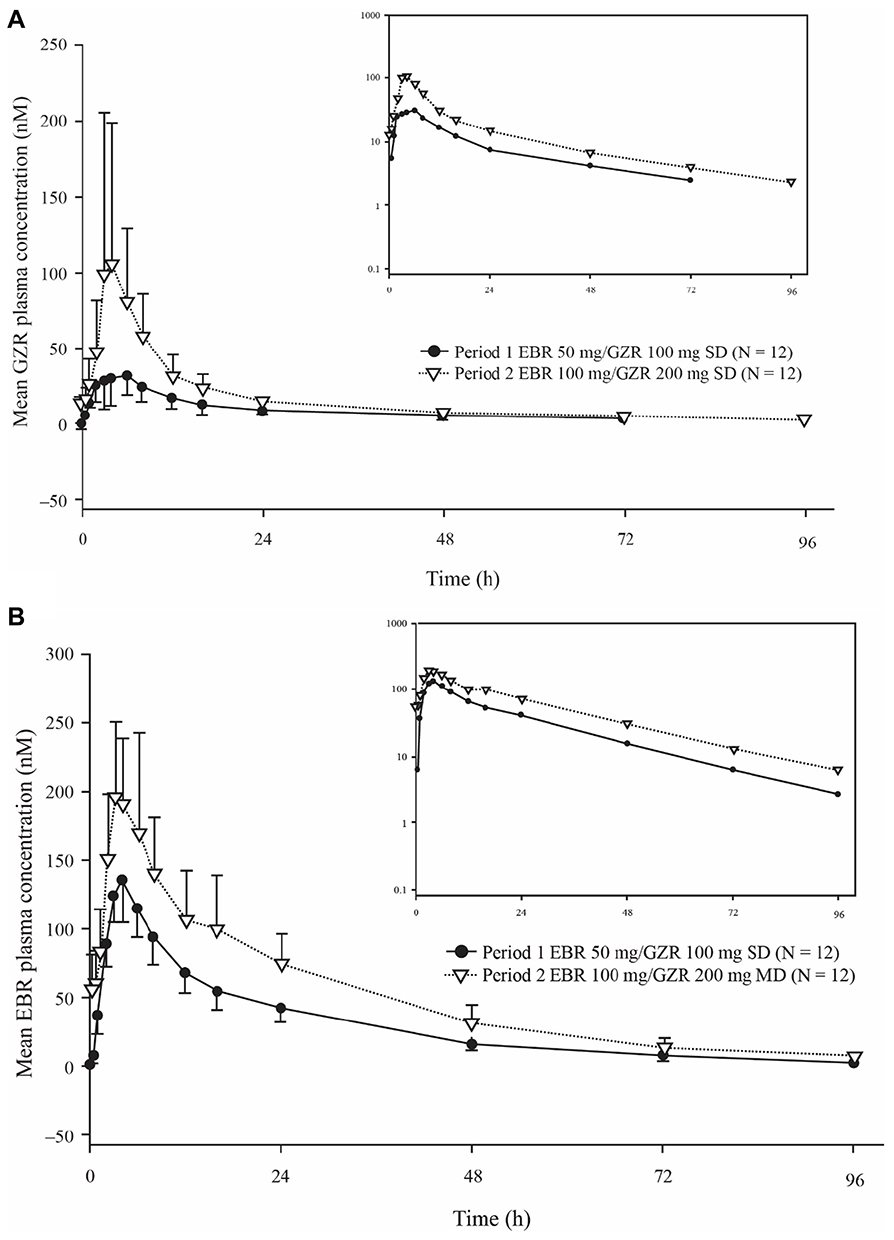 |
Figure 2 Arithmetic mean plasma concentration versus time profiles following once-daily multiple-dose administration of elbasvir 50 mg/grazoprevir 100 mg on day 1 of Period 1 or on day 10 of Period 2 in healthy Chinese participants (per-protocol population). Error bars represent standard deviation. (A) Grazoprevir; (B) elbasvir. Inset: semi-log scale. Abbreviations: EBR, elbasvir; GZR, grazoprevir. |
PK parameter values for EBR and GZR after multiple doses are summarized in Table 3. Both EBR and GZR were absorbed with a median Tmax of 4–5 hrs. Both compounds accumulated following multiple-dose administration, which is consistent with their estimated t1/2, with an AUC0–24 accumulation ratio of 1.58 (EBR; 95% CI = 1.37–1.83) and 2.53 (GZR; 95% CI = 1.79–3.09) (Figure 3).
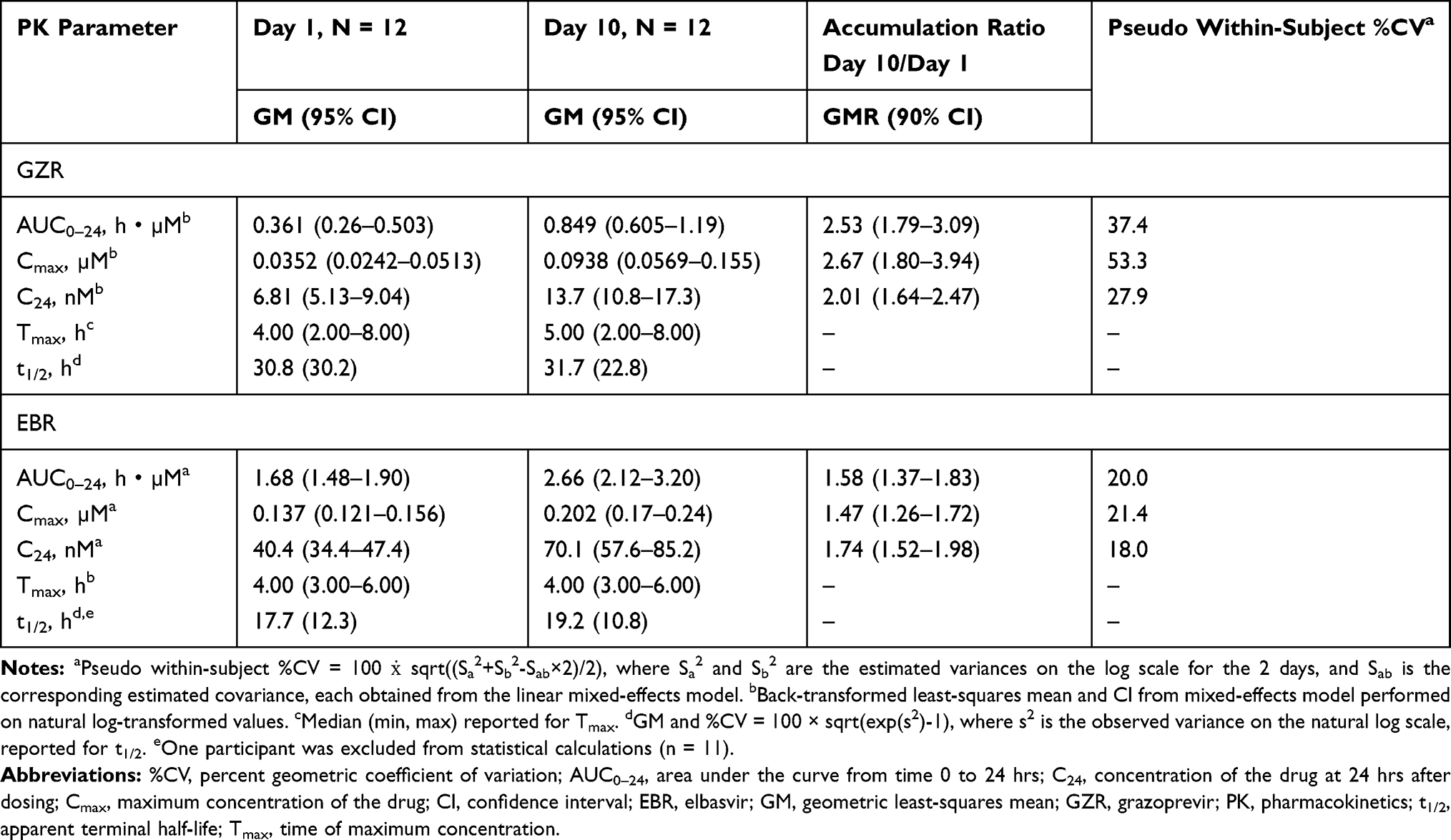 |
Table 3 Pharmacokinetic Parameters of Grazoprevir and Elbasvir Following Multiple-Dose Administration of One Tablet of Elbasvir 50 mg/Grazoprevir 100 mg Daily for 10 Days in Healthy Chinese Participants (Per-Protocol Population) |
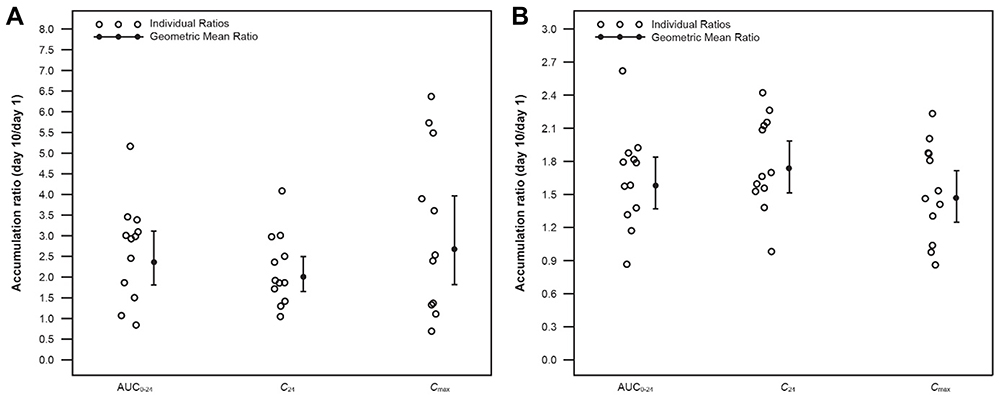 |
Figure 3 Individual accumulation ratio (day 10/day 1): geometric mean ratio and 95% confidence interval following multiple-dose administration of oral elbasvir 50 mg/grazoprevir 100 mg in healthy Chinese participants (per-protocol population). (A) Grazoprevir; (B) elbasvir. Abbreviations: AUC0–24, area under the curve from time 0 to 24 hrs; C24, concentration of the drug at 24 hrs after dosing; Cmax, maximum concentration of the drug. |
The pharmacokinetics of EBR (50 mg) and GZR (100 mg) in Chinese individuals in the present study after multiple-dose administration with the EBR/GZR fixed-dose combination were also compared with PK values from healthy, Caucasian males receiving single-entity EBR or GZR in the MK-8742-PN001 and MK-5172-PN001 studies (Table 4). GZR pharmacokinetics were generally similar in Chinese and Caucasian individuals, with geometric mean ratios (GMRs; (90% CI) of 1.19 (0.755–1.88) for AUC0–24 and 0.99 (0.711, 1.38) for C24. The GMR (90% CI) for Cmax was 1.27 (0.646–2.50) and median Tmax was 4 hrs for GZR in both Chinese and Caucasian participants. EBR exposure was slightly higher in healthy Chinese individuals than in their Caucasian counterparts, with GMRs (90% CI) for AUC0–24 of 1.76 (1.31–2.37) and 1.84 (1.35–2.51) for C24. The GMR (90% CI) for Cmax of EBR was 1.88 (1.36–2.58), and median Tmax was 4 hrs in Chinese and Caucasian participants.
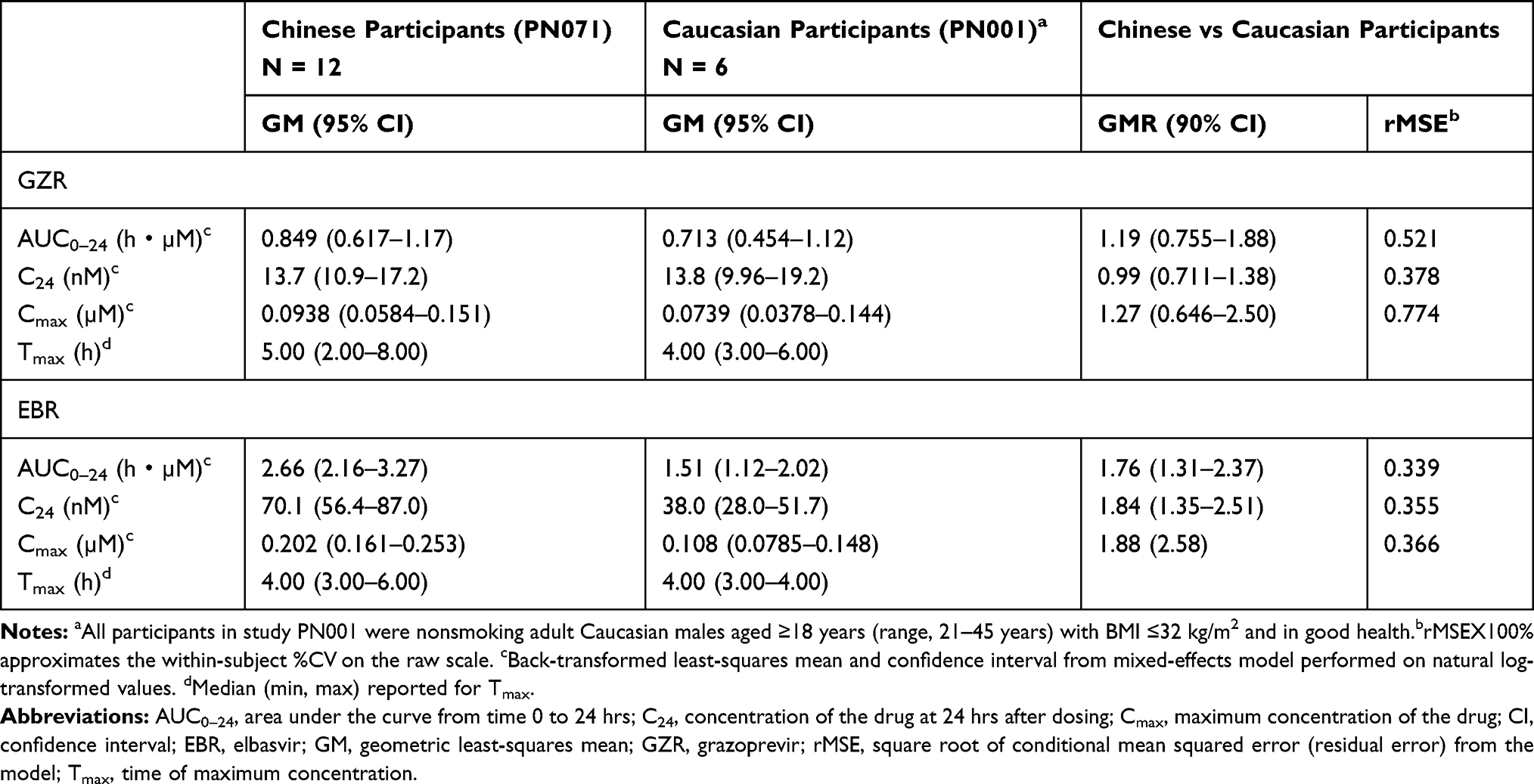 |
Table 4 Summary Statistics and Statistical Comparison of Pharmacokinetic Parameters Following Multiple-Dose Oral Administration of Elbasvir 50 mg/Grazoprevir 100 mg Fixed-Dose Combination in Healthy Chinese Participants (MK-5172-PN071) versus Grazoprevir (100 mg) or Elbasvir (50 mg) as Single-Entity Formulations in Healthy Caucasian Participants (MK-5172-PN001 and MK-8742-PN001) |
Safety
EBR 50 mg/GZR 100 mg and EBR 100 mg/GZR 200 mg were generally well tolerated in healthy Chinese male and female participants in this study. A summary of AEs is shown in Table 5. In total, 5 of the 12 enrolled participants experienced 5 AEs in Period 2 (multiple dose), and no AEs were reported in Period 1 or Period 3 (single dose). Just 1 AE (decreased appetite, mild in intensity) was considered by the investigator to be drug-related. One AE was moderate in intensity (dizziness), the remaining AEs were mild; all AEs resolved spontaneously without treatment. No deaths or serious AEs were reported, and no participants discontinued the study because of an AE. There were no clinically meaningful changes in laboratory safety test results, electrocardiograms, vital signs, or physical examination findings.
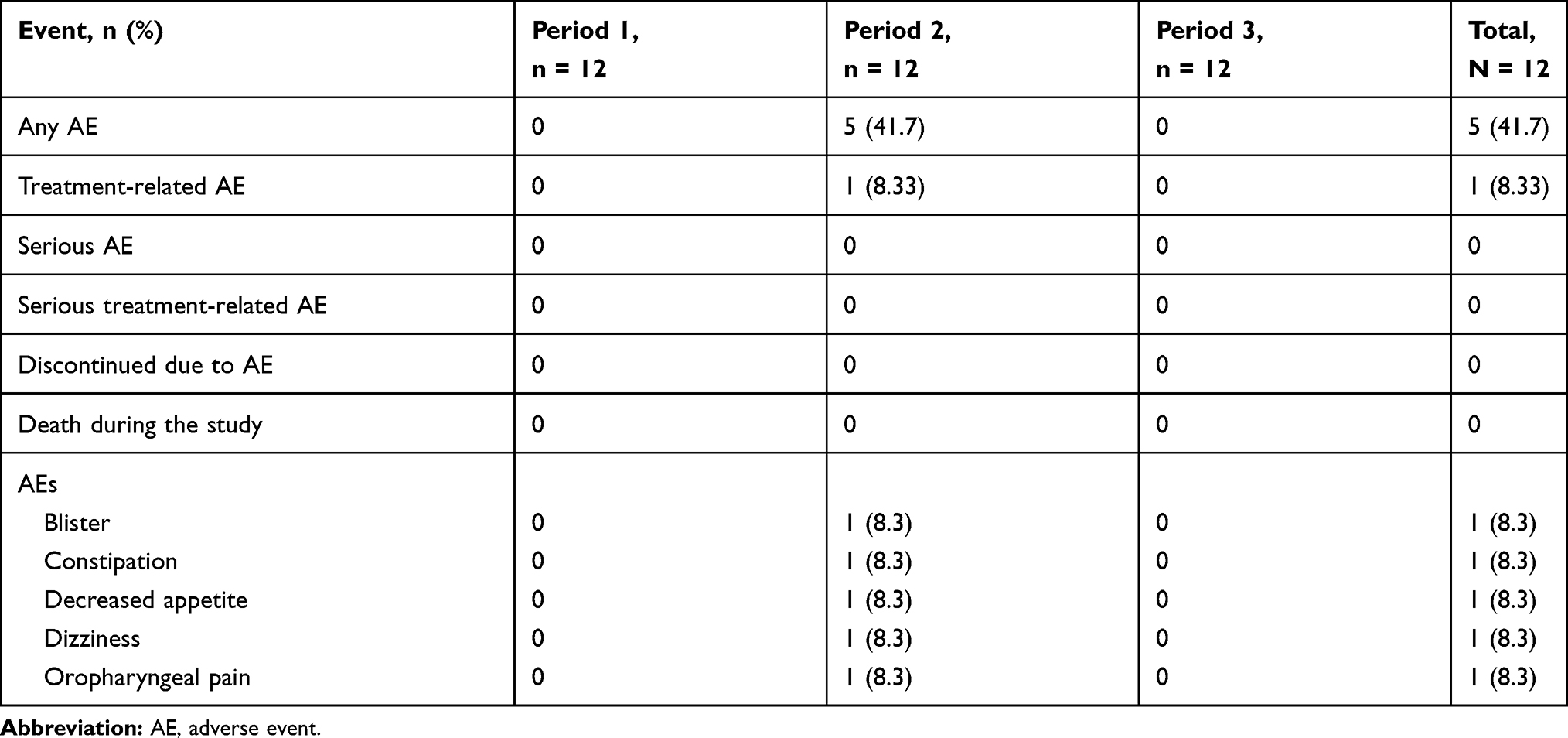 |
Table 5 Summary of Adverse Events During Treatment Periods (All Patients as Treated) |
Discussion
In this Phase I, open-label, 3-period study, the pharmacokinetics of single- and multiple-dose EBR/GZR in healthy Chinese volunteers have been characterized. The exposures observed in this study were within exposure ranges previously demonstrated to be efficacious and well tolerated. Following single-dose administration of EBR 50 mg/GZR 100 mg or EBR 100 mg/GZR 200 mg of study drug, the AUC0-∞ and Cmax of EBR increased as the dose increased, with a median Tmax of 3–4 hrs and t1/2 of approximately 18 hrs. Similarly, the AUC0-∞ and Cmax of GZR increased as the dose increased, with a median Tmax of 3–4 hrs and t1/2 of approximately 30 hrs. Once-daily administration of EBR 50 mg/GZR 100 mg for 10 days resulted in AUC0–24 accumulation ratios of 1.58 and 2.35 for EBR and GZR, respectively.
The fixed-dose combinations of EBR 50 mg/GZR 100 mg and EBR 100 mg/GZR 200 mg were generally well tolerated in healthy Chinese male and female participants in this study. All AEs were reported in Period 2 (multiple-dose administration), and all resolved spontaneously without treatment. Although it has been reported that Asian participants experienced a slightly higher rate of late alanine aminotransferase elevations in clinical trials owing to higher plasma PK exposure,14 no clinically meaningful laboratory abnormalities were observed in this analysis.
The PK properties of EBR and GZR have previously been evaluated in non–HCV-infected and in HCV-infected adult participants, and population PK analyses estimated the AUCs for EBR and GZR to be 15% and 50% higher, respectively, for Asians compared with Caucasians.6,14 Broadly similar results were obtained when data from the current multiple-dose study were compared with data from previous Phase I studies in Caucasian participants (MK-5172-001 and MK-8742-001). This comparison showed 76% and 19% increases in AUC0–24 values for EBR and GZR in Chinese compared with Caucasian individuals. The differences between the population PK results and data from the present study may be attributable to several factors related to the present analyses. Participants in the present study received the fixed-dose combination of EBR/GZR, whereas participants in the historical Phase I studies received single-entity EBR or GZR. However, the in vivo performances of the fixed-dose combination versus the single-entity formulations have been demonstrated to be similar, and thus any PK differences between Chinese and Caucasian populations are unlikely to be attributable to the different formulations. Other notable differences between the study populations were the inclusion of Caucasian male participants in the Phase I studies versus male and female Chinese participants in the present study. Smaller sample sizes of the population in these Phase I studies and large variability in GZR pharmacokinetics may also contribute to the differences. In both the present study and the MK-8742-PN001 and MK-5172-PN001 studies, EBR and GZR were administered under fasted conditions and the same PK sampling schedules were used for both agents.
Regardless of these slight differences, both the present analysis and previous population PK analyses demonstrate small increases in EBR and GZR exposure in Asian compared with Caucasian individuals. The PK of EBR and GZR when administered as single entities have also been assessed in healthy Chinese participants.24 In this study, EBR AUC0-∞ and Cmax increased in a dose-proportional manner, whereas GZR AUC0-∞ and Cmax increased in a greater-than-dose-proportional manner. A comparison with PK in healthy Caucasian participants indicated that EBR and GZR exposures may trend higher in healthy Chinese participants relative to healthy Caucasian participants.24 In addition, both compounds have moderate to high PK variability, and the PK variability in the present study is also consistent with that previously reported.24 Increased drug exposure in Asian compared with Caucasian participants has also been reported for other HCV DAAs such as simeprevir and asunaprevir.25,26 These increases may be due to race-related differences in liver size, hepatic blood flow, or cytochrome P450 3A expression. Overall, based on the accumulated safety data from previous EBR and GZR studies, together with the comparable efficacy and safety of EBR 50 mg/GZR 100 mg in Asian and non-Asian participants in Phase III studies, the magnitude of these PK differences is not considered clinically relevant. The data from the present study therefore support the dosing recommendation of EBR 50 mg/GZR 100 mg for Chinese people with HCV infection. In the Phase III C-CORAL study, high rates of sustained virologic response 12 weeks after the completion of therapy were achieved in Asian participants with HCV genotype 1 or 4 infection receiving EBR 50 mg/GZR 100 mg for 12 weeks.27 Rates of SVR12 were 96.7% in participants enrolled at Chinese study centers (146/151), similar to SVR12 rates attained by Australian (92.9% [26/28]) and Russian (99.2% [117/118]) individuals.27
With the recent release (November 2017) and worldwide implementation of ICHE17 guidelines on multi-regional clinical trials (MRCT),28 it has become increasingly important that internal and external factors are taken into consideration during the planning and design of MRCTs. The present study illustrates that uniform dose recommendations can be applied across different geographic regions, despite racial differences in the PK profile. In the future, Asian countries, including China, could become increasingly involved in early-stage drug development, enabling the generation of Asian/Chinese-specific pharmacologic data that can then be used to support late-stage MRCTs across diverse geographic regions.
Conclusion
Single-dose administration of 1 or 2 tablets of the fixed-dose combination of EBR 50 mg/GZR 100 mg and once-daily administration of 1 tablet of the fixed-dose combination for 10 days was generally well tolerated in healthy Chinese male and female participants, with PK values within the expected range.
Abbreviations
AE, adverse event; ANOVA, analysis of variance; APaT, all participants as treated; AUC, area under the curve; AUC0-∞, area under the curve from time 0 to infinity; AUC0–24, area under the curve from time 0 to 24 hrs; BMI, body mass index; C24, concentration of the drug at 24 hrs after dosing; CI, confidence interval; Cmax, maximum concentration of the drug; CV, coefficient of variation; DAA, direct-acting antiviral agent; EBR, elbasvir; GM, geometric least-squares mean; GZR, grazoprevir; HBV, hepatitis B virus; HCV, hepatitis C virus; LC-MS/MS, liquid chromatographic tandem mass spectrometric; LLOQ, lower limit of quantitation; MRCT, multi-regional clinical trials; NS, nonstructural protein; PEG-IFN, pegylated interferon; PK, pharmacokinetics; PP, per protocol; RBV, ribavirin; rMSE, square root of conditional mean squared error (residual error) from the model; t1/2, apparent terminal half-life; Tmax, time of maximum concentration.
Ethics Statement
The study was conducted in accordance with principles of Good Clinical Practice and the ethical principles that have their origin in the Declaration of Helsinki, and was approved by the Independent Ethics Committee of Peking University Third Hospital.
Consent for Publication
All patients were required to provide written informed consent to participate in the study.
Data Sharing Statement
Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA’s data sharing policy, including restrictions, is available at http://engagezone.msd.com/ds_documentation.php. Requests for access to the clinical study data can be submitted through the EngageZone site or via email to [email protected].
Acknowledgments
The study was conducted in the Drug Clinical Trial Center, Peking University Third Hospital, Peking, China. Medical writing support was provided by Sally Mitchell, PhD, and Tim Ibbotson, PhD, of ApotheCom, Yardley, PA, USA. This assistance was funded by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA.
Author Contributions
All authors made substantial contributions to the conception and design of the study, the acquisition of data, or analysis and interpretation of data; took part in drafting the manuscript or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
L.C. and J.B.M. are employees of and hold stock in Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA. H-P.F. is an employee and stockholder of Merck Sharp & Dohme Corp., a subsidiary of Merck and Co., Inc., Kenilworth, NJ, USA. J.J., M.L., S.M., J.W., and S.X. are employees of Merck, Sharp & Dohme Ltd, Beijing, China. X.M.Z. is an employee of and holds stock in Merck, Sharp & Dohme Ltd, Beijing, China. H.L., Y.W., L.X., Z.Y., and S.Z. have no conflicts of interest to declare. Funding for this research was provided by Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA. The authors report no other conflicts of interest in this work.
References
1. WHO World Health Organization. Hepatitis C: key facts. [
2. Bennett H, Waser N, Johnston K, et al. A review of the burden of hepatitis C virus infection in China, Japan, South Korea and Taiwan. Hepatol Int. 2015;9(3):378–390. doi:10.1007/s12072-015-9629-x
3. Sievert W, Altraif I, Razavi HA, et al. A systematic review of hepatitis C virus epidemiology in Asia, Australia and Egypt. Liver Int. 2011;31(Suppl 2):61–80. doi:10.1111/liv.2011.31.issue-s2
4. Zhang Y, Chen L-M, Miao H. Hepatitis C virus in mainland China with an emphasis on genotype and subtype distribution. Virol J. 2017;14:41. doi:10.1186/s12985-017-0710-z
5. Messina JP, Humphreys I, Flaxman A, et al. Global distribution and prevalence of hepatitis C virus genotypes. Hepatology. 2015;61(1):77–87. doi:10.1002/hep.27259
6. Lu Y, Jin X, Duan CA, Chang F. Cost-effectiveness of daclatasvir plus asunaprevir for chronic hepatitis C genotype 1b treatment-naïve patients in China. PLoS One. 2018;13(4):e0195117. doi:10.1371/journal.pone.0195117
7. Li JP, Feng WT, Xie ZW, et al. [Real-world study of daclatasvir and asunaprevir combination in Chinese patients with HCV genotype 1b infection]. Zhonghua Gan Zang Bing Za Zhi. 2018;26(12):951–954. Chinese. doi:10.3760/cma.j.issn.1007-3418.2018.12.014
8. Han Q, Fan X, Wang X, et al. High sustained virologic response rates of sofosbuvir-based regimens in Chinese patients with HCV genotype 3a infection in a real-world setting. Virol J. 2019;16(1):74. doi:10.1186/s12985-019-1184-y
9. Hu P, Ren H. [Current status of treatment of chronic hepatitis C and related challenges in the “Pre-DAA era” in China]. Zhonghua Gan Zang Bing Za Zhi. 2016;24(11):869–873. Chinese. doi:10.3760/cma.j.issn.1007-3418.2016.11.015
10. Lim SG, Dan YY. A 2015 roadmap for the management of hepatitis C virus infections in Asia. Korean J Intern Med. 2015;30(4):423–433. doi:10.3904/kjim.2015.30.4.423
11. Wei L, Cheng J, Luo J, et al. [Efficacy and safety of paritaprevir/ritonavir/ombitasvir combined with dasabuvir in non-cirrhotic Asian adult patients with newly diagnosed and treated chronic HCV genotype 1b infection: a randomized, double-blind, placebo-controlled study – China data]. Zhonghua Gan Zang Bing Za Zhi. 2018;26(5):359–364. Chinese. doi:10.3760/cma.j.issn.1007-3418.2018.05.009
12. Zhang QF, Zhang DZ. [Potential application of sofosbuvir-based treatment for chronic hepatitis C in China]. Zhonghua Gan Zang Bing Za Zhi. 2018;26(3):233–237. Chinese. doi:10.3760/cma.j.issn.1007-3418.2018.03.012
13. Health Canada. Product Monograph Including Patient Medication Information: Zepatier. Kirkland, QC, Canada: Merck Canada Inc.; 2017. Available from: https://pdf.hres.ca/dpd_pm/00039964.PDF.
14. Zepatier [perscribing information]. Whitehouse Station, NJ: Merck Sharp & Dohme, Corp.; 2018.
15. Zepatier [Summary of Product Characteristics]. Hoddesdon, Hertfordshire: Merck Sharp & Dohme Ltd.; 2018.
16. Kumada H, Suzuki Y, Karino Y, et al. The combination of elbasvir and grazoprevir for the treatment of chronic HCV infection in Japanese patients: a randomized phase II/III study. J Gastroenterol. 2017;52(4):520–533. doi:10.1007/s00535-016-1285-y
17. Harper S, McCauley JA, Rudd MT, et al. Discovery of MK-5172, a macrocyclic hepatitis C virus NS3/4a protease inhibitor. ACS Med Chem Lett. 2012;3(4):332–336. doi:10.1021/ml300017p
18. Coburn CA, Meinke PT, Chang W, et al. Discovery of MK-8742: an HCV NS5A inhibitor with broad genotype activity. ChemMedChem. 2013;8(12):1930–1940. doi:10.1002/cmdc.v8.12
19. Kwo P, Gane E, Peng CY, et al. Effectiveness of elbasvir and grazoprevir combination, with or without ribavirin, for treatment-experienced patients with chronic hepatitis C infection. Gastroenterology. 2017;52(1):164–175. doi:10.1053/j.gastro.2016.09.045
20. Roth D, Nelson DR, Bruchfeld A, et al. Grazoprevir plus elbasvir in treatment-naive and treatment-experienced patients with hepatitis C virus genotype 1 infection and stage 4-5 chronic kidney disease (the C-SURFER study): a combination phase 3 study. Lancet. 2015;386(10003):1537–1545. doi:10.1016/S0140-6736(15)00349-9
21. Rockstroh JK, Nelson M, Katlama C, et al. Efficacy and safety of grazoprevir (MK-5172) and elbasvir (MK-8742) in patients with hepatitis C virus and HIV co-infection (C-EDGE CO-INFECTION): a non-randomised, open-label trial. Lancet HIV. 2015;2(8):e319–e327. doi:10.1016/S2352-3018(15)00114-9
22. Zeuzem S, Ghalib R, Reddy KR, et al. Grazoprevir-elbasvir combination therapy for treatment-naive cirrhotic and noncirrhotic patients with chronic HCV genotype 1, 4, or 6 infection: a randomized trial. Ann Intern Med. 2015;163(1):1–13. doi:10.7326/M15-0785
23. Caro L, Lee J, Feng E, et al. II-37 population pharmacokinetics modeling characterizes the higher grazoprevir exposure in Japanese compared to non-Japanese HCV-infected patients.
24. Cheung TT, Yan Chiu JW, Yuen MF, et al. A phase I, single- and multiple-dose study to evaluate the pharmacokinetics of elbasvir and grazoprevir in healthy Chinese participants. Clin Ther. 2018;40(5):719–732. doi:10.1016/j.clinthera.2018.03.014
25. Eley T, Garimella T, Li W, Bertz RJ. Asunaprevir: a review of preclinical and clinical pharmacokinetics and drug–drug interactions. Clin Pharmacokinet. 2015;54(12):1205–1222. doi:10.1007/s40262-015-0299-6
26. Ramamoorthy A, Pacanowski MA, Bull J, Zhang L. Racial/ethnic differences in drug disposition and response: review of recently approved drugs. Clin Pharmacol Ther. 2015;97(3):263–273. doi:10.1002/cpt.61
27. Wei L, Zhdanov K, Burnevich E, et al. Efficacy and safety of elbasvir/grazoprevir in treatment-naïve patients with chronic HCV GT 1, GT 4 and GT 6 infection (C-CORAL): a phase III randomized multinational clinical trial 2017. J Hepatol. 2017;66:S529. doi:10.1016/S0168-8278(17)31460-5
28. U.S. Department of Health and Human Services. Food and Drug Administration. General principles for planning and design of Multi-Regional Clinical Trials. 2018. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/e17-general-principles-planning-and-design-multi-regional-clinical-trials. Accessed
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.