")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
A Review of Recommendations for Routine Immunization Services During COVID-19 Pandemic That are Relevant for Nursing Personnel Involved in the Implementation of Immunoprophylaxis
Authors Bednarek A, Klepacz R
Received 9 July 2020
Accepted for publication 10 August 2020
Published 7 October 2020 Volume 2020:13 Pages 1099—1105
DOI https://doi.org/10.2147/JMDH.S271182
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anna Bednarek,1 Robert Klepacz2
1Chair and Department of Paediatric Nursing, Faculty of Health Sciences, Medical University of Lublin, Poland; 2Department of Clinical Pathomorphology, Medical University of Lublin, Poland
Correspondence: Anna Bednarek Email [email protected]
Abstract: Immunization programmes are of key importance for maintaining good health and protecting life. Disruption to routine immunization may increase the incidence of diseases that can be prevented by vaccinations. The aim of this review is to present the current recommendations on immunization services during the COVID-19 pandemic that are relevant for the nursing practice. It contains an overview of recommended guidelines published in March and April 2020, and of scientific publications on immunizations for children and adults, taking into account recommendations related to the new epidemiological risk caused by SARS-CoV-2 infections. The ongoing global pandemic of COVID-19 calls for changes in the organization of health care and puts an additional burden on all resources forming the healthcare system. The COVID-19 pandemic poses a particular challenge to public health, as active immunoprophylaxis should make it possible to control other infectious diseases. Protection against the spread of SARS-CoV-2 may hamper routine immunization services, which must be administered with particular regard to epidemiological safety. Nurses have always had an important role to play in the implementation and promotion of vaccinations and in emphasizing their importance for public health. Therefore, it is crucial that they have up-to-date information on vaccinological interventions that reduce the risk of transmission of SARS-CoV-2 infections.
Keywords: immunization, COVID-19 pandemic, nursing practice of vaccinology
Introduction
Immunization programmes are an important element of the national health policy in every country. Disruption in the systematic immunization services can have an adverse effect on health and on the maintenance of herd immunity against many infectious diseases. The increase in the number of unvaccinated people increases the risk of VPD outbreaks.1
The pandemic caused by SARS-CoV-2 resulted in an unexpected public health emergency. As of 19 March 2020, 51 out of 53 countries of the WHO European Region reported confirmed SARS-CoV-2 infections. Each of these countries initiated a range of measures to mitigate the transmission of SARS-CoV-2 infections. Healthcare resources have been shifted to the prevention and treatment of COVID-19 in order to reduce the impact of the outbreak on national healthcare systems.2,3
On 20 March 2020 the WHO issued guidance on routine immunization services during the COVID-19 pandemic in the WHO European Region. The WHO emphasized that immunization services are an essential component of healthcare services in every country. Routine immunization sessions should be adapted to the current epidemiological situation of COVID-19 and the capacity of the healthcare system. Through these measures, the risk of increased incidence and mortality due to VPDs shall be mitigated.4
Aim
The aim of this review is to present the current recommendations on immunization services during the COVID-19 pandemic that are relevant for the nursing practice in the field of vaccinology.
Review Methods
Compilation of source data selected on a subjective basis by the authors as part of the standard literature review of Medline, Cochrane, and Scopus databases. The paper is a review of the guidelines published in March and April 2020 and of scientific publications on immunization services for children and adults, which take account of the recommendations related to the epidemiological risk during the pandemic.
Results
Guidelines on Routine Immunization Services for Children and Adults During the COVID-19 Pandemic
The WHO presents six key principles for immunization services during the COVID-19 pandemic (Table 1). These recommendations will be regularly updated depending on the epidemiological situation related the spread of SARS-CoV-2 infections.5
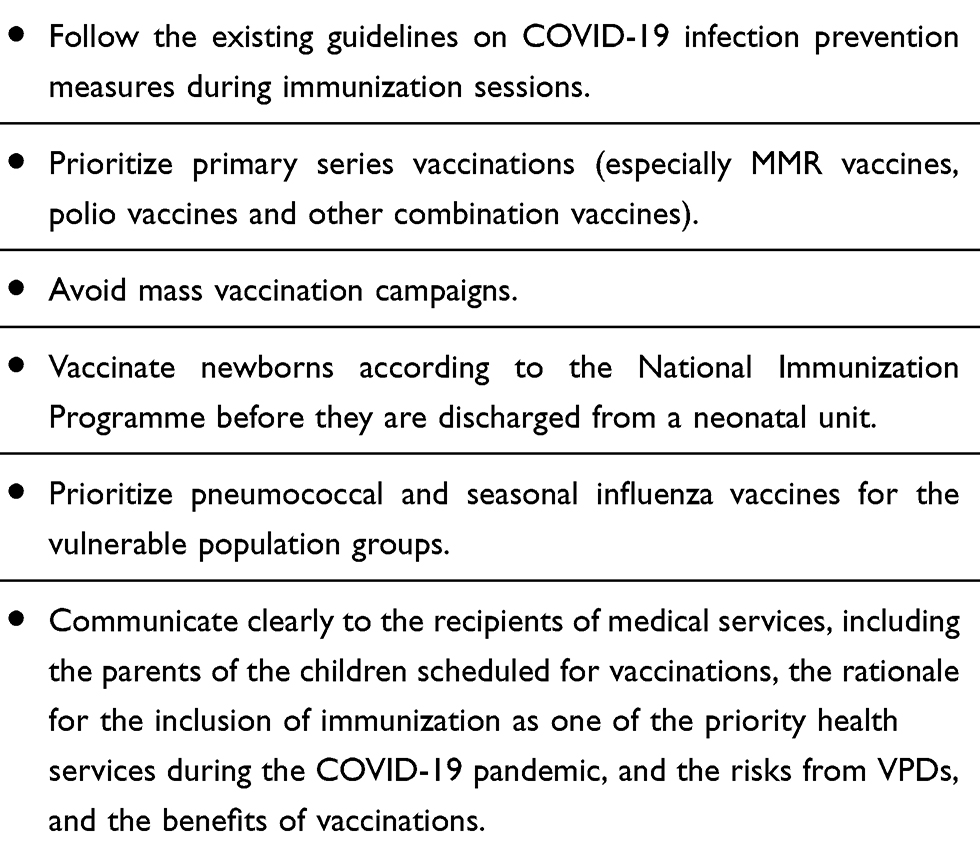 |
Table 1 New Guiding Principles for Immunization Programmes During the COVID-19 Pandemic |
Considerations for Decision Making on Immunization Services in a Given Country
The current COVID-19 situation is rapidly evolving, which directly translates into the organization of the healthcare system and its capacity in the individual countries of the WHO European Region. Differences in the methods of sustaining high levels of routine immunization coverage depend primarily on the incidence of COVID-19. This creates temporary changes in the organization of health care, and transformations in the treatment and prevention needs of the society. Overflow of data (or rather ‘information noise’) during an epidemic can lead to a decrease in public confidence, affecting active immunoprophylaxis and the healthcare system as a whole. Therefore, the Ministry of Health of each individual country should make every possible effort to sustain constant high population immunity.6
During a pandemic, it is important to monitor the level of immunization services and to analyse all signals of reduction in the vaccination coverage rate among the general population and in specific vulnerable groups. The immunization service providers should start preparing lists of children who have missed their vaccine doses and develop an action plan for tailormade catch-up immunization.7
Consideration of immunization options during the COVID-19 pandemic should be guided by a detailed assessment of the following local data on:
- Epidemiological risks of VPDs (vaccine-preventable diseases) among the general population and in specific vulnerable groups. Special emphasis should be given to epidemic-prone VPDs and to halting any backslide in the achievement of measles elimination and polio eradication.
- Epidemiological situation of COVID-19 and related mitigation measures in place. The need to divert resources to reduce the impact of COVID-19 on the healthcare system must be weighed against the risk of increased morbidity and mortality of VPDs resulting from any change to immunization services, which may cause a potential additional burden to the healthcare system. In accordance with the WHO Strategic Preparedness and Response Plan for COVID-19 all countries should be prepared to respond to all the transmission scenarios.
- Characteristics and constraints of the healthcare system and immunization services. Countries in the European Region have different healthcare systems and legislative frameworks for immunization.
- Specific vaccines and available logistics. The availability of routine vaccines and the possibility of procurement and administration, in the current context, of all scheduled vaccine doses should be analysed according to the National Immunization Programme and the local guidelines on logistic operations. In addition, it should be taken into consideration that a ‘stop–start’ policy might have to be adopted, whereby the target population would receive the required vaccine doses at irregular intervals over a longer period of time.8
As the epidemiological and operational status is different in each country, a single vaccination strategy cannot be provided in the current situation. The algorithm proposed by the WHO may provide guidance to national public health authorities in taking decisions related to the continuing operation of immunization services (Figure 1).4,9
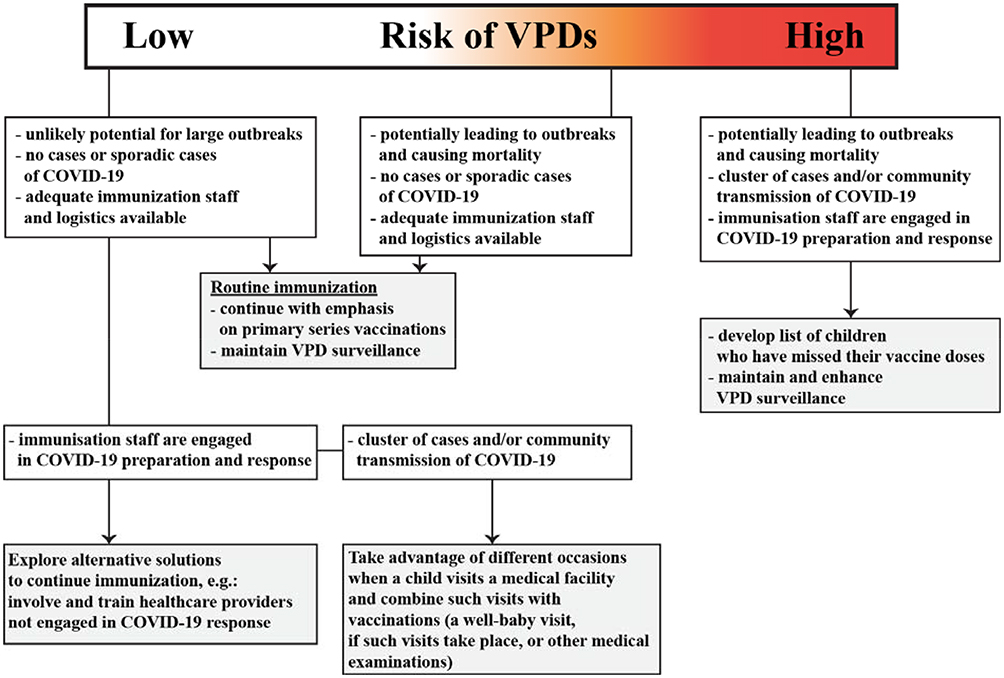 |
Figure 1 Decision-making algorithm for immunization services in the general population. |
The WHO draws attention to the key principles for immunization services during the COVID-19 pandemic, which should include measures to limit the risk of SARS-CoV-2 transmission during immunization sessions. Provision of immunization services should be aligned with the national guidelines and with the principles of anti-epidemic procedures concerning prevention and control of infections in healthcare facilities (Table 2).10
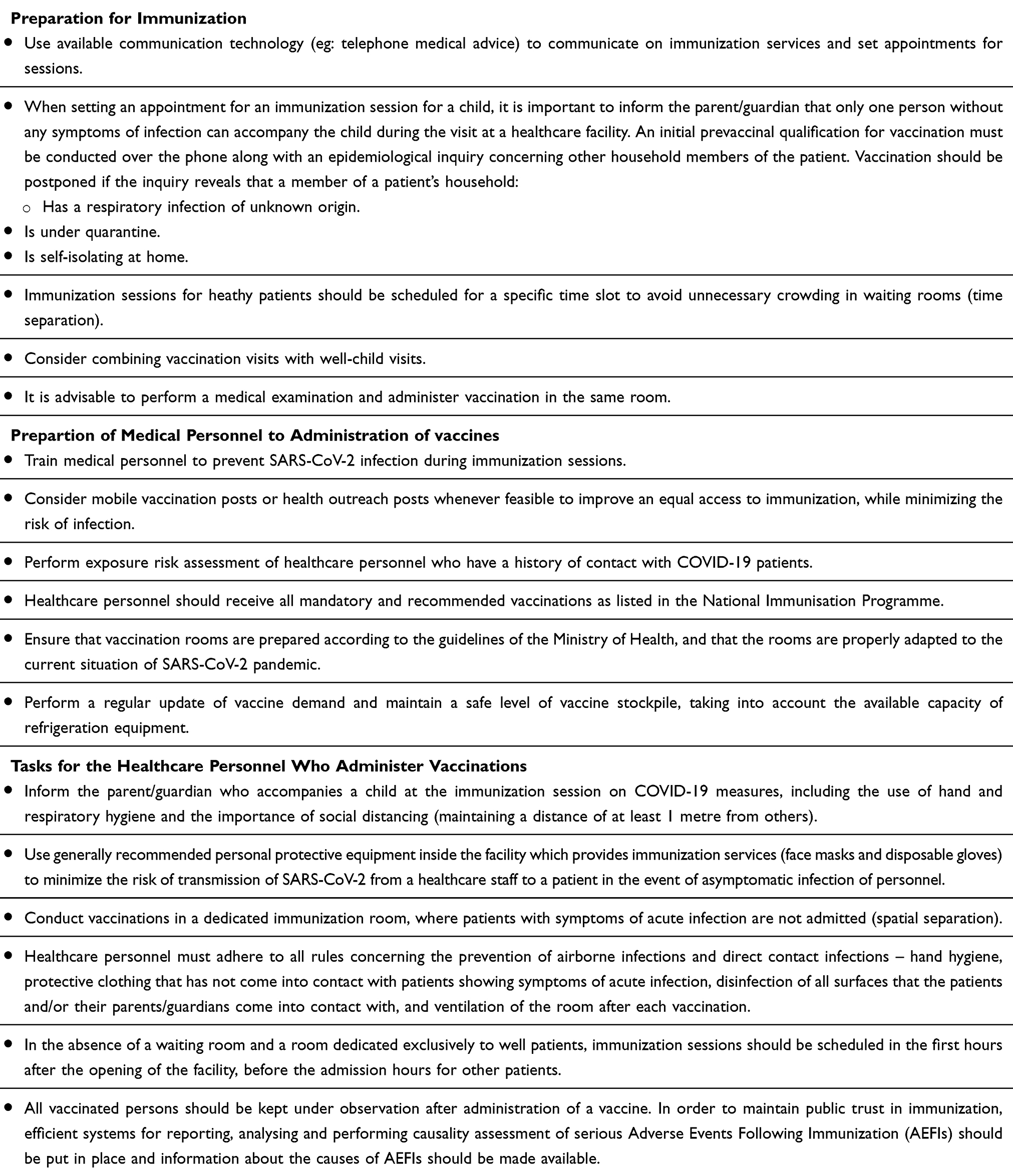 |
Table 2 Organization of Immunization Services and Vaccination Procedures During the COVID-19 Pandemic – Guidelines for Doctors and Nurses |
In times of the COVID-19 pandemic immunization services for healthy children and adults remain a very important issue and they are recommended to be carried out, provided the required level of epidemiological safety described above is maintained.4,11
First of all, immunization services should be carried out in neonatal wards in accordance with the National Immunization Programme. Immunization services should also be provided as soon as possible in the group of children under 24 months of age, as infants and young children are most vulnerable to all kinds of infections, and in this age group, the risk of developing infectious diseases is the highest. Chronically ill children, for whom there are often special medical indications for immunization, require individual attention. When medical indications require, post-exposure vaccinations against rabies, tetanus, measles, varicella and hepatitis B should be carried out systematically in all age groups. At the same time, it is advisable to carry out other immunization services, whose administration or completion is necessary due to the characteristics of the medicinal product. In addition, it is recommended to promote vaccinations against pertussis for pregnant women, and vaccinations against pneumococcus and seasonal flu for adults in risk groups and for people over 60 years of age.5
Patients should be reminded that lung diseases, cardiovascular diseases, cancer, diabetes, kidney failure and immune disorders make them prone to pneumonia. It is particularly important when we think of prophylaxis against SARS-CoV-2 infection.7,12
It is recommended to administer the maximum number of vaccinations which are included the National Immunization Programme (in accordance with the summary of product characteristics of the particular vaccine) during one immunization session. Such a procedure eliminates the unnecessary additional contact between the vaccinated person and the medical facility which provides immunization services.10,13 The first step is to vaccinate children, whose immunization has already been delayed due to factors not related to their general health condition. Since the most common generalized postvaccination reaction is fever, in time of the current epidemic it is recommended to administer a prophylactic dose of paracetamol to children who have been vaccinated.14–16
In view of the COVID-19 pandemic and the spread of SARS-CoV-2 infections, it is important to demonstrate understanding towards parents and adults who often have strong reservations or unfounded fears related to immunization services, which may result in a temporary vaccine refusal.1,17
In 1974 the WHO initiated the Expanded Program on Immunization (EPI), which resulted in an increase in the percentage of children who received four core EPI vaccines, ie vaccines preventing tuberculosis (BCG), diphtheria, tetanus and pertussis (DTP), poliomyelitis and measles, from <5% to 86%. As a follow-up to this program in 2012, the WHO approved the Global Vaccine Action Plan (GVAP). The main objective of this project is to increase to at least 90% the proportion of children vaccinated with vaccines used routinely in national immunization programmes in all WHO regions, and to reduce inequalities in access to these vaccines. The WHO had planned to achieve these objectives in 2020.18
According to preliminary reports published by the WHO, even before the COVID-19 pandemic, every year 20 million children under the age of 1 did not receive vaccinations against measles or poliomyelitis. In 2019 over 13 million of the youngest children were not given any vaccine. Most of these children live in countries with an inefficient healthcare system. The lowest vaccination coverage rates are in the WHO African Region and, taking into account the whole population of incompletely vaccinated children, more than half of them (60%) live in only 10 countries (Nigeria, India, Pakistan, Indonesia, Ethiopia, Philippines, Democratic Republic of Congo, Brazil, Angola, Vietnam).19
In poorer regions of the world immunization services are often carried out in unconventional places that gather a large number of people (schools, religious facilities). Educational methods and incentives are effective strategies to support vaccination systems. However, vaccination campaigns pose a huge logistical challenge, requiring the involvement of tens of thousands of healthcare workers. The task is further complicated by the need to maintain the cold chain and to administer the vaccine by injection.20
The WHO recommends that the governments of developing countries perform their own assessment of the risk that may be associated with temporary suspension of immunization services, and that state authorities financially support immunization programmes. In this current difficult pandemic situation, it is recommended that efforts be made to continue basic immunization programmes while maintaining adequate safety for medical personnel and local communities through appropriate procedures and equipment. The WHO also calls on partner organizations, European governments and donors to financially support immunization programmes in developing countries and thus reduce vaccination inequalities.4
It is undisputable that vaccinations are the most effective public health intervention aimed to reduce the incidence and mortality of infectious diseases. Unfortunately, a number of prevention programmes in developing countries are not implemented or do not achieve the required population coverage due to specific circumstances, especially economic conditions. Lack of awareness and limited resources of qualified personnel should also be identified as obstacles to this form of immunoprophylaxis. Moreover, it should always be noted that the WHO only recommends certain measures and rules of conduct, but their introduction into the healthcare system is a sovereign decision of each individual country.5
Conclusion
Immunization affects many aspects of health at a global level, no matter at what stage of life it is done. Therefore, immunization services should be carried out on a continuous basis. During the epidemic of SARS-CoV-2 infections vaccinations should be administered with a particular regard to epidemiological safety. Nurses have an important role to play in promoting knowledge about immunization. Especially during the COVID-19 pandemic, it is important that nurses have up-to-date information on immunization services. It is important for building a relationship based on mutual trust with parents of vaccinated children and with vaccinated adults, which is a basic condition for a proper vaccination procedure.
Abbreviations
COVID-19, coronavirus disease 2019, a disease caused by infection with SARS-CoV-2; AEFI, adverse events following immunization; MMR, measles, mumps and rubella vaccine; SARS-CoV-2, severe acute respiratory syndrome coronavirus; VPD, vaccine-preventable diseases; WHO, World Health Organization.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Lieu TA, Zikmund-Fisher BJ, Chou C, Ray GT, Wittenberg E. Parents’ perspectives on how to improve the childhood vaccination process. Clin Pediatr. 2017;56(3):238–246. doi:10.1177/0009922816649001
2. Burke RM, Midgley CM, Dratch A, et al. Active monitoring of persons exposed to patients with confirmed COVID-19 — United States, January–February 2020. MMWR Morb Mortal Wkly Rep. 2020;69(9):245–246. doi:10.15585/mmwr.mm6909e1
3. Available from: who.maps.arcgis.com/apps/opsdashboard/index.html#/ead3c6475654481ca51c-248d52ab9c61.
4. WHO. Guidance on routine immunization services during COVID-19 pandemic in the WHO European region.
5. Centers for Disease Control and Prevention (CDC). Maintaining childhood immunizations during COVID-19 pandemic.
6. Ghinai I, McPherson TD, Hunter JC, et al. First known person-to-person transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in the USA. Lancet. 2020;395(10230):1137–1144.
7. Chen H, Guo J, Wang C, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet. 2020;395(10226):809–815. doi:10.1016/S0140-6736(20)30360-3
8. COVID-19: strategic planning and operational guidance for maintaining essential health services during an outbreak. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical guidance.
9. Chen Y, Peng H, Wang L, et al. Infants born to mothers with a new coronavirus (COVID-19). Front Pediatr. 2020;8. doi:10.3389/fped.2020.00104
10. Available from: www.who.int/publications-detail/critical-preparedness-readinessand-response-actions-for-covid-19.
11. Rose MA, Juergens C, Schmoele-Thoma B, Gruber WC, Baker S, Zielen S. An open-label randomized clinical trial of prophylactic paracetamol coadministered with 7-valent pneumococcal conjugate vaccine and hexavalent diphtheria toxoid, tetanus toxoid, 3-component acellular pertussis, hepatitis B, inactivated polio virus, and Haemophilus influenzae type b vaccine. BMC Pediatr. 2013;13:98.
12. Das RR, Panigrahi I, Naik SS. The effect of prophylactic antipyretic administration on post-vaccination adverse reactions and antibody response in children: a systematic review. PLoS One. 2014;9(9):e106629. doi:10.1371/journal.pone.0106629
13. Prymula R, Esposito S, Zuccotti GV, et al. A Phase 2 randomized controlled trial of a multicomponent meningococcal serogroup B vaccine (I). Hum Vaccin Immunother. 2014;10(7):1993–2004.
14. Manley J, Taddio A. Acetaminophen and ibuprofen for prevention of adverse reactions associated with childhood immunization. Ann Pharmacother. 2007;41(7–8):1227–1232. doi:10.1345/aph.1H647
15. Anderson BJ. Paracetamol (Acetaminophen): mechanisms of action. Paediatr Anaesth. 2008;18(10):915–921. doi:10.1111/j.1460-9592.2008.02764.x
16. Jackson LA, Dunstan M, Starkovich P, et al. Prophylaxis with acetaminophen or ibuprofen for prevention of local reactions to the fifth diphtheria-tetanus toxoids-acellular pertussis vaccination: a randomized, controlled trial. Pediatrics. 2006;117(3):620–625. doi:10.1542/peds.2005-1217
17. Kim HJ, Lee YH, Im SA, Kim K, Lee CHK. Cyclooxygenase inhibitors, aspirin and ibuprofen, inhibit MHC-restricted antigen presentation in dendritic cells. Immune Netw. 2010;10(3):92–98. doi:10.4110/in.2010.10.3.92
18. Peck M, Gacic-Dobo M, Diallo MS, Nedelec Y, Sodha SS, Wallace AS. Global routine vaccination coverage, 2018. Morb Mortal Wkly Rep. (MMWR). 2019;68(42):937–942. doi:10.15585/mmwr.mm6842a1
19. Casey RM, Hampton LM, Anya BM, Gacic-Dobo M, Diallo MS, Wallace AS. State of equity: childhood immunization in the World Health Organization African Region. Pan Afr Med J. 2017;21(Suppl 3):5.
20. Johri M, Pérez MC, Arsenault C, et al. Strategies to increase the demand for childhood vaccination in low-and middle-income countries: a systematic review and meta-analysis. Bull World Health Organ. 2015;93(5):339–346C. doi:10.2471/BLT.14.146951
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.