")
Back to Journals » Clinical Optometry » Volume 12
A Review of Contact Lens Dropout
Authors Pucker AD , Tichenor AA
Received 17 April 2020
Accepted for publication 10 June 2020
Published 25 June 2020 Volume 2020:12 Pages 85—94
DOI https://doi.org/10.2147/OPTO.S198637
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Andrew D Pucker,1 Anna A Tichenor2
1School of Optometry, University of Alabama at Birmingham, Birmingham, AL, USA; 2School of Optometry, Indiana University, Bloomington, IN, USA
Correspondence: Andrew D Pucker
School of Optometry, University of Alabama at Birmingham, 1716 University Blvd, Birmingham, AL 35233, USA
Tel +1 920 579-2900
Email [email protected]
Purpose: Contact lens (CL) dropout is likely a major factor contributing to the near stagnant growth in the CL market. The purpose of this review is to summarize the current state of knowledge related to the frequency of CL dropout and the factors associated with it.
Methods: PubMed.gov was searched on or before March 22, 2020, with the terms “contact lens” with “dropout” or “cessation” or “disruption” or “discomfort”. Pertinent articles were collected. The references from these articles were likewise searched to identify additional relevant articles. Only manuscripts written in English were included. No study design or date exclusions were imposed on this review.
Results: This literature review found that CL dropout was frequent across developed countries, with a CL dropout frequency that ranged between 12.0% and 27.4% (pooled mean = 21.7%). The top cited reason for CL dropout in established CL wearers was discomfort, while vision was the top reason in neophyte CL wearers. If given the chance, CL dropouts are often able to successfully resume CL wear up to 74% of the time. While the literature is mixed with regard to factors promoting CL dropout, meibomian gland dysfunction appears to promote CL dropout.
Conclusion: CL dropout is a frequently encountered condition that may be curtailed by early detection, patient education, alterative CL options, or early treatment of underlying ocular surface diseases such as meibomian gland dysfunction.
Keywords: contact lens dropout, contact lens cessation, contact lens dry eye, ocular surface
Introduction
Successful contact lens wear has been defined as being able to comfortably wear one’s contact lenses for at least 12 hours per day for at least six days per week while still being able to see at least as well as while wearing spectacles.1 Contact lenses have a number of benefits for both children and adults, which include improving one’s overall visual satisfaction, ability to play sports, and one’s overall self-perception.2,3 Mounting evidence also suggests that two contact lens-based options, soft multi-focal and overnight orthokeratology contact lenses are able to slow a child’s myopic progression,4,6 which is potentially a major public health victory since reducing one’s overall amount of myopia may improve one’s overall visual experience, and it might reduce one’s chances of developing vision threatening conditions later in life.7 Thus, ensuring that patients are successful contact lens wearers is now more important than ever.
Unfortunately, a large percent of contact lens wearers each year cease wearing their contact lenses on a regular basis and many even permanently stop wearing their contact lenses because of various reasons, which include discomfort, vision, cost, and convenience.8 The cessation of contact lens use is also commonly referred to in the literature as contact lens dropout.9 Contact lens dropout has historically plagued market growth, especially since the inception of daily wear, reusable contact lenses.8,10 Likewise, the introduction of better contact lens designs and materials have failed to curb contact lens dropout rates across the world.11,12 Since contact lens dropout is a worldwide issue,11,12 fully understanding its frequency and associated factors is imperative to devising strategies for moving past the pitfalls of modern contact lenses. Therefore, the purpose of this review is to summarize the current state of knowledge related to contact lens dropout and its associated factors, so better contact lens designs, materials, and fitting/management strategies can be employed to keep patients in contact lenses longer each day and for more years. This will subsequently allow practitioners to better meet the refractive and health needs of their patients.
Methods
The aim of this review was to gain a better understanding of the frequency of contact lens dropout (cessation of contact lenses) and factors associated with it. A PubMed.gov search was conducted on or before March 22, 2020 by entering the term “contact lens” with “dropout” or “cessation” or “disruption” or “discomfort”. All recovered abstracts were reviewed by the authors (ADP and AAT), and the text of articles of interest were analyzed to determine if the studies aligned with this review. Additional texts were recovered by searching the references of the recovered manuscripts. This review had no restrictions on study designs or dates. Only manuscripts published in English were included. Special attention was given to publication date when describing the frequency of contact lens dropout, so the readers could keep the available materials in mind when considering the frequency of contact lens dropout.
Results
Frequency of Contact Lens Dropout
Several key factors related to the frequency of contact lens dropout have been explored in the literature since the introduction of reusable soft contact lenses. The following section will explore these topics by first discussing the frequency of contact lens dropout in early reusable hydrogel soft contact lenses. It will next describe how there has been a lack of change in the frequency of contact lens dropout with the introduction of silicone hydrogel contact lenses. This section will then conclude with a description of key differences related to contact lens dropout in neophytes (new) or established contact lens wearers. Information related to rigid contact lens wearers will be included where appropriate, though limited information related to this contact lens modality was detected during this review likely because there are far fewer rigid contact lens wearers in the current market.13
Early Soft Contact Lenses (1999 and Before)
Modern, reusable, soft contact lenses were introduced back in the late 1980s,8 and daily disposable soft contact lenses were introduced into the market in 1994.14 While these wear modalities have somewhat simplified the contact lens wearing experience, not all wearers have been able to achieve complete contact lens satisfaction. This is highlighted by an early, commonly cited meeting abstract by Weed et al (1993) who surveyed established contact lens wearers in Ontario, Canada to determine the frequency of contact lens dropout.15 This university-based survey received responses from 568 subjects, and found that a staggering percentage (51%) of the subjects had a past history of contact lens dropout and that of these subjects only 48% of them tried to return to contact lenses; the primary reason for returning to contact lenses was because of cosmetic purposes.15 This study furthermore found that if a subject dropped out of contact lenses, they typically did so within the first 2 years of contact lens wear.15 The authors lastly found that the top two reasons for contact lens dropout were ocular discomfort and irritation.15 Briggs (1996) later performed a survey of 200 self-reported contact lens dropouts from Saudi Arabia who dropped out of contact lenses within the past 10 years, and the authors likewise found that the top reason for contact lens dropout was ocular discomfort (61.0%).12 This reason was followed by inconvenience (30.5%), poor vision (5.5%), cost (2.0%), and refractive surgery (1.0%).12
Pritchard et al (1999) later published their seminal survey on soft and rigid contact lens dropouts.8 This Canadian-based study received 1444 completed surveys from subjects who completed 5 ± 6 years of contact lens wear and found that 34% of the surveyed subjects had ceased contact lens wear at least once during that time period.8 While some of these subjects returned to contact lenses at a later date, this survey found that 12% of subject permanently dropped out of contact lenses.8 Pritchard et al like Weed et al and Briggs found that the top reason for contact lens dropout was ocular discomfort (49%).8,12,15 In fact, ocular discomfort was nearly equal to all of the other reasons for dropping out of contact lenses combined: experienced dry eye (9%), needed to replace lenses (6%), lens cleaning too much bother (5%), experienced red eye (5%), poor vision (4%), advised to do so by eyecare provider (4%), insertion/removal too much bother (3%), pregnancy (3%), and near vision problems (3%).8 Pritchard et al interestingly found that the contact lens dropouts wore their contact lenses fewer days per week than subjects who did not dropout of contact lenses.8 This result has since been confirmed by Pucker et al who found that contact lens dropouts were significantly more likely to wear their contact lenses fewer days per week and fewer hours per day than successful contact lens wearers.9 These results further support comfort being an issue for many wearers. Lastly, Pritchard et al found that subjects who resumed contact lens wear primarily did so for cosmetic reasons (23%) and because the discomfort/irritation symptoms that they were experiencing had resolved (23%).8 Thus, the overall data from early reusables soft contact studies suggest a permanent dropout rate between 12% and 27% (Table 1).
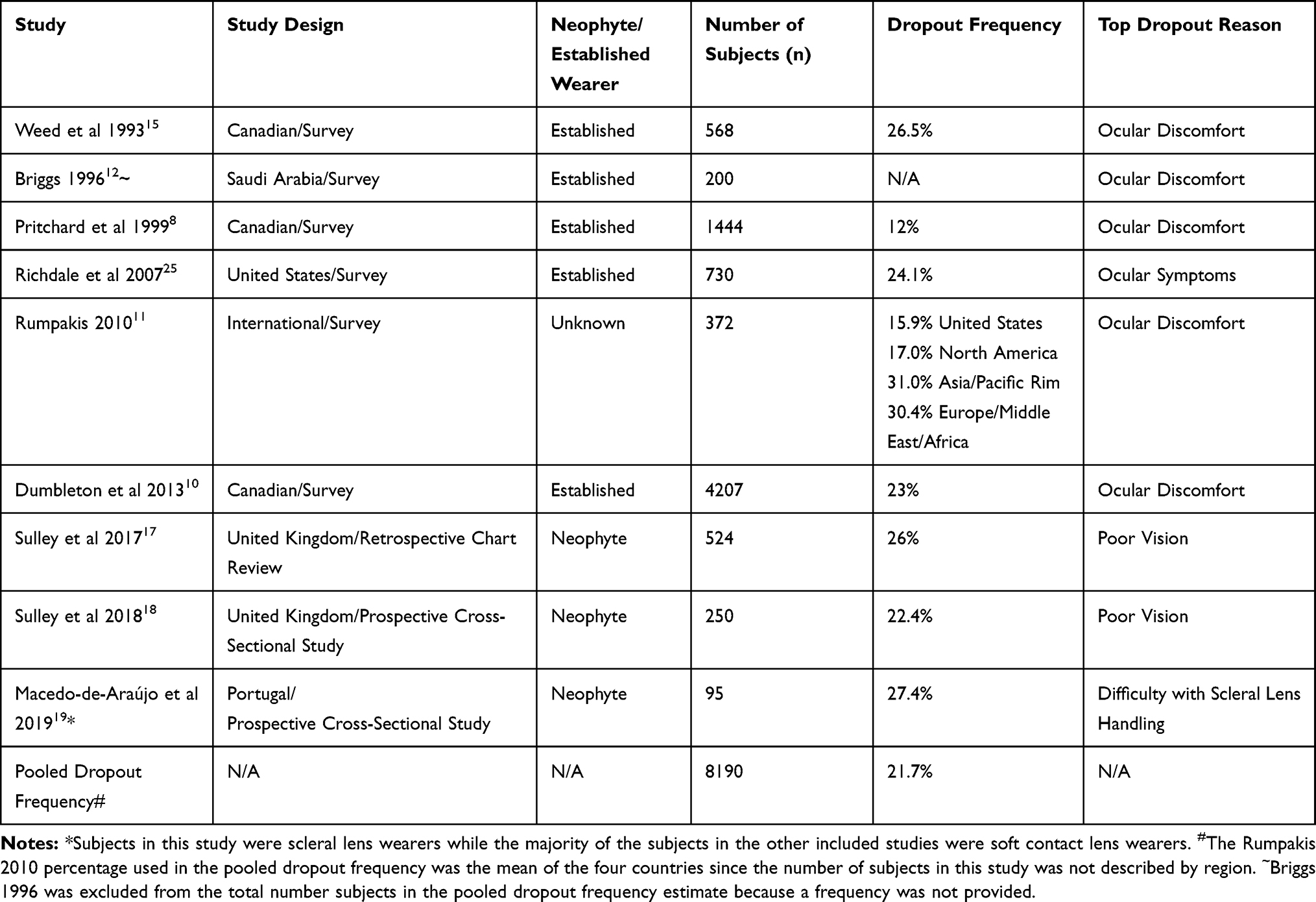 |
Table 1 Summary of the Frequency of Contact Lens Dropout by Study and for All Studies |
Modern Soft Contact Lenses (After 1999)
With the introduction of silicone hydrogel contact lenses into the market, there were high hopes related to improved ocular health, comfort, and overall contact lens success,10 yet multiple studies have failed to provide support for silicone hydrogel contact lenses yielding higher contact lens retention rates. Richdale et al (2007) were among the first groups to analyze contact lens dropout in a sample that contained silicone hydrogel contact lens wearers (hydrogel, silicone hydrogel, and rigid contact lens wearers) in the United States.16 The authors accomplished this task by surveying 730 subjects who were between the ages of 18 and 88 years.16 Of the subjects who completed the survey 62.0% of them had a history of wearing contact lenses, and 75.9% of these subjects were still wearing contact lenses (frequency of dropout = 24.1%).16 Subjects in this study who dropped out of contact lenses again reported (multiple responses allowed) that their top reason for dropping out of contact lenses was ocular symptoms (64%). The following specific symptoms were noted by the subjects: discomfort (69%), dryness (59%), grittiness (37%), itchiness (21%), photophobia (21%), soreness (24%), and pain (21%).16 Subjects additionally indicated that they dropped out of contact lenses because of preference for other refractive error correction (50%), contact lens cost or convenience (33%), and poor vision (14%).16
In a more recent and comprehensive study, Dumbleton et al (2013) investigated the frequency and reasons for contact lens dropout via an online survey in Canada.10 A total of 4207 of the completed surveys were deemed eligible for the study with the subjects ranging in age from 17 and 77 years with 64% of these subjects being female.10 This study found that 60% of the subjects were current wearers while 40% of the subjects had a history of contact lens dropouts.10 While 62% of the contact lens dropouts did resume contact lens wear, 23% of the subjects were permanent contact lens dropouts.10 Reasons for returning to contact lenses included cosmetic (32%), convenience (21%), and being offered an alternative type of contact lens (14%).10 The top reasons for contact lens dropout were discomfort (24.4%) and dryness (19.9%), though subjects noted other factors such as ocular redness (6.8%), cost (6.8%), and handling issues (6.3%). If subjects dropped out of contact lenses, 27% of the subjects dropped out within six months, 38% of the subjects dropped out within six to 12 months, and 35% of the subjects dropped out after one year.10
Dumbleton et al’s data are supported by a related Rumpakis (2010) study.10,11 While the article from Rumpakis was published in Review of Optometry (trade journal), it is still commonly cited in the peer-reviewed literature because it offers an international perspective on contact lens dropout.11 This study was a 27-country survey (n = 372) of wearers, which found that contact lens dropout rates were between 16% and 30% worldwide. Rumpakis estimated that each contact lens dropout could translate to $24,000 ($19,497 to $24,556 depending on country; US = $21,695) worth of lost revenue to a clinical practice over a patient’s lifetime.11 The author like the above studies found that the top reason for contact lens dropout was ocular discomfort.11 Thus, data from Rumpakis, Richdale et al, and Dumbleton et al all suggest that the introduction of silicone hydrogel materials has not curbed the frequency of contact lens dropout.10,11,16
Neophyte vs Established Wearers
Historically, the top cited reason for contact lens dropout has been ocular discomfort, yet recent research has caused the community to qualify this conclusion. More specifically, investigators have attempted to analyze the frequency of contact lens dropout in neophyte contact lens wearers. This point is highlighted by a 2017 study by Sulley et al who analyzed the one-year retention rates of neophyte contact lens wearers.17 This United Kingdom-based retrospective chart review analyzed 524 charts from patients with a known fitting outcome (wearing contact lenses or not).17 This study of predominantly soft contact lens wearers (98%) found that 74% of the subjects were still wearing contact lenses one year after being originally fit in lenses (26.0% dropout rate).17 Of the subjects who had a known dropout date, 25.4% of subjects dropped out within one month, 46.7% dropped out within two months, and 75.0% dropped out within six months.17 Of the subjects with a known contact lens dropout reason (more than one reason allowed), the top reasons were poor vision (47%), discomfort (25%), and lack of motivation (18%).17 This study interestingly found that only 29% of contact lens dropouts were offered an alternative contact lens option, which indicates that practitioners should more actively investigate and try to solve the problems of contact lens wearers.17 The above data from Dumbleton et al likewise suggests that patients should be reminded of the many benefits (eg, cosmetic) offered by contact lenses to help them rekindle their motivation to wear contact lenses.10
Sulley et al (2018) later attempted to answer the same question in a different manner by prospectively enrolling 531 neophyte subjects (250 fully completing study) and fitting them in appropriate soft contact lens. Retention rates were then analyzed over one year.18 Sulley et al’s prospective study came to a similar conclusion to their chart review with regards to dropout rates (22.4%), time to contact lens discontinuation, and primary reason for contact lens dropout.18 Macedo-de-Araújo et al (2019) likewise completed a prospective study of contact lens retention rates over a one year time period; however, Macedo-de-Araújo et al specifically studied scleral lens wearers (large dimeter gas permeable lenses).19 While Macedo-de-Araújo’ et al’s prospective study found a similar contact lens dropout rate (27.4%) compared to Sulley et al’s perspective study (22.4%), Macedo-de-Araújo’ et al found that the top reasons for subjects to drop out of scleral lenses were that 35% of the dropouts experienced handling issues and 19% of the dropouts experienced ocular discomfort.18,19 The primary difference between Macedo-de-Araújo’ et al’s work and Sulley et al’s work is likely related to the unique issues associated with applying scleral lenses (eg, most scleral lens wearers need to use application devices to apply the lens) compared to soft contact lens wearers who typically just apply the their contact lenses with their fingers.19 These data suggest that early in a contact lens wearer’s life acceptable vision is one of the most important factors for contact lens success while after wearing lenses for one or more years, many contact lens wearers begin to experience contact lens discomfort, which eventually results in contact lens dropout.20 These data furthermore indicate that the frequency of contact lens dropout across a contact lens wearers’ life (neophyte vs established contact lens wearers) is relatively stable, so contact lens practitioners should be regularly monitoring for issues. A summary of studies related to the frequency of contact lens dropout can be found in Table 1. Data from this table has been subsequently used to estimate an across study frequency of contact lens dropout (pooled mean = 21.7%).
Resuming Contact Lens Wear
While investigators such as Pritchard et al and Dumbleton et al have used surveys to investigate subjects returning to contact lens use after dropout,8,10 others have prospectively studied this topic in an attempt to see if contact lens dropouts could successfully resume contact lens wear if given an alternative contact lens option. Schlanger (1993) was the first to attempt this approach by recruiting 199 subjects from the United States who self-identified as contact lens dropouts within the past 10 years.21 Schlanger’s study found that if given the option to try an alternative contact lens, 82% of subjects could wear their contact lenses at least on the weekends and 64.5% of subjects could wear their contact lenses on a daily basis for at least 10 hours per day.21 Unfortunately, this study only had a one week follow up time period.21 Young et al (2002) later completed a similar, yet more comprehensive study of subjects who dropped out of contact lenses at least one year ago.16 Young et al’s 6-month multi-center study, which was conducted in the United Kingdom, recruited 236 contact lens dropouts who were refit into an alternative contact lens.16 The top reason subjects had originally dropped out of contact lenses was because of discomfort (51%) and poor vision (13%). Of the included subjects 96% of them were dispensed lenses and of these subjects 77% of them were still wearing contact lenses at the one-month visit.16 Nevertheless, by the six-month evaluation, 26% of the subject who were able to be contacted (214/236) indicated that they were contact lens dropouts.16 Therefore, these data overall suggest that while not all subjects are able to wear contact lenses when given an additional opportunity, up to 74% of subjects may be able to successfully resume contact lens wear at least part time.16,21 These results from Young et al’s study are similar to Dumbleton et al’s survey of lapsed wearers study (77% vs 74%), though differences in study design (prospective vs retrospective) and sample size (236 subjects vs 4207 subjects) prevent a true comparison between studies.10,16
Factors Associated with Contact Lens Dropout
With over 140 million contact lens wearers worldwide and over 45 million wearers in the United States alone, there is clearly a high demand for contact lenses.22,23 Unfortunately, these numbers are relatively small in comparison to the estimated 2.5 billion myopes in the world who could benefit from contact lenses and the many other patients who suffer from refractive error issues such as presbyopia who could also benefit.24 These data suggest that there a number of factors that are either inhibiting patients from trying contact lenses or from being a successful contact lens wearer. The following section describes the known factors that are associated with contact lens dropout (inability to succeed with contact lenses) with hope that future strategies can be devised to help mitigate the shortcomings of contact lenses.
Patient Factors (Sex, Age)
There is limited evidence in the literature to support that sex or age influences the frequency of contact lens dropout. During the above mentioned Richdale et al (n = 730) study on contact lens dropout and dissatisfaction,25 the authors determined that contact lens dropout was about two times more likely with males than females. However, other studies have failed to show a significant association between sex and dropping out of contact lenses. This claim is supported by Pritchard et al (n = 1444) and Dumbleton et al (n = 4207) who all failed to find an association between sex and being a contact lens dropout.8,10
The literature likewise suggests that age is another factor that may or may not be associated with contact lens dropout. Richdale et al found in their study of established wearers that contact lens dropouts were more likely to be older when first starting to wear contact lenses and more likely to have worn lenses for a longer period in their lifetime.25 Pritchard et al likewise found that contact lens dropouts started wearing lenses at an older age than successful lens wearers.8 However, while Young et al also found contact lens dropouts to have worn lenses for a longer time period in their lifetime, they found conflicting evidence that contact lens dropouts started wearing lenses at a younger age.16 In addition, Pucker et al did not find a difference in age when starting contact lens wear between successful contact lens wears and contact lens dropouts, but the authors note that successful contact lens wears had worn lenses longer than the dropouts which conflicts with the results from other studies.9 Thus, based on the above work, there are no definitive associations between sex nor age and contact lens dropout. Unfortunately, the data on age is muddied by patients becoming presbyopic, which has the potential to cause some patients to drop out of contact lenses because of the visual changes associated with advancing age.9
Contact Lens Factors
Exploring more modifiable factors associated with contact lens dropout has the potential to provide insight into methods for reducing the frequency of contact lens dropout. One area of interest is the parameters of contact lenses; however, very few direct and definitive associations have been found between contact lens dropout and factors such as contact lens material, modulus, and lens design. One study of note is Pucker et al (2019) who recruited a group of subjects who dropped out of contact lenses because of discomfort within the past six to 12 months and compared these subjects to successful contact lens wearers (n = 112).9 The investigators of this study found a non-significant association (p = 0.05; odds ratio = 2.5) between hydrogel contact lens wearers and silicone hydrogel contact lens wearers for contact lens dropout. This finding is corroborated by Sulley et al (2018) who found that material (silicone hydrogel vs hydrogel) had no impact on contact lens retention rates.18 Nevertheless, the above described Dumbleton et al (2013) study found that lapsed contact lens wearers were more likely to wear hydrogel contact lenses than silicone hydrogel contact lenses,10 and because of this there is still no consensus on the effects of contact lens material on contact lens dropout. The difference between Pucker et al’s, Dumbleton et al’s, and Sulley et al’s studies that may be leading to this lack of clarity include that Sulley et al’s work focused on neophyte contact lens wearers whereas the other two studies focused on established wearers.9,10,18 Pucker et al’s and Sulley et al’s were likewise prospective studies while Dumbleton et al’s study was a retrospective study. Lastly, Dumbleton et al’s study was considerably larger than the other two studies, which may have made it easier for these investigators to have found a significant result.
Research studies have also focused on investigating the relationship between contact lens parameters and ocular discomfort. There is likewise conflicting evidence showing a relationship between contact lens discomfort and material. Several large, cross-sectional studies have reported either greater comfort with silicone hydrogel,26 equal or greater comfort to silicone hydrogel compared to traditional hydrogel lenses,27 or that hydrogel lenses has less comfort or no difference in hydrogel lenses compared to silicone hydrogel lenses.28 Based on these studies, while there are ocular surface health benefits from silicone hydrogel contact lenses compared to traditional hydrogels (eg increased oxygen transmissibility leading to less corneal edema),29 it is difficult to ascertain a significant relationship between lens material and contact lens dropout. Nevertheless, a better understanding of how contact lens material affects contact lens comfort and dropout would greatly benefit the community because this knowledge could lead to customized treatments and more biocompatible materials. These advancements will likely only be achieved by completing well-designed, prospective, randomized trials that pit a number of materials against each other and include molecular endpoints that can determine the biological impact of individual materials.
Sphere, Toric, and Presbyopic Lenses
There may be an association between the type of refractive lens needed and contact lens dropout. Sulley et al (2018) reported retention rates for the first year of wear for neophytes and found these rates to be highest in spherical lens wearers (81%), followed by toric lenses (75%), and multifocal lenses worn by presbyopes (69%).18 Likewise, Young et al reported high success rates in spherical wearers, with lower rates in toric wearers followed by multifocal wearers.16 These studies suggest an association between contact lens dropout rates and refractive design of the contact lens. Furthermore, contact lens wearers of these different designs may report different reasons for dropping out of contact lens wear. While new wearers of spherical lenses may discontinue due to handling of the lens and discomfort, those fit in toric and multifocal lenses are more likely to discontinue due to poor vision.16,18,30 Therefore, it may be especially important to have toric and multifocal contact lens wearers return for a follow up visit to ensure that all of their visual needs are being met.
Wear Schedule
Reusable contact lenses are now frequently prescribed meaning that the contact lenses are usually worn on a monthly or biweekly basis, removed nightly and disinfected with care systems, reapplied during the day, and discarded after the wear period. Daily disposable contact lenses are also frequently prescribed; these wearers discard their contact lenses each day after the wear cycle. Daily disposable contact lenses have gained popularity since their inception because of the many benefits of a daily disposable contact lenses such as ease of use and increased compliance due to the limited need for contact lens care products like multipurpose solutions or cases.31–33 Therefore, it seems prudent to investigate whether this simplified modality has influenced the frequency of contact lens dropout.
In a 2013 Dumbleton et al survey, 24% of the discontinued contact lens wearers had worn daily disposable contact lenses while only 19% of the successful contact lens wearers were wearing daily disposable lenses.10 In contrast, the same survey found that 71% of the discontinued contact lens wearers had worn frequent replacement soft lenses while 76% of the successful wearers wore frequent replacement soft lenses. These results, suggesting that a higher proportion of daily disposable lens wearers discontinued lens wear, are surprising and may be explained by clinicians’ prescribing tendencies. Chalmers et al found that clinicians tend to prescribe daily disposable contact lenses to their more challenging/dissatisfied patients.27 Therefore, more dropouts in the daily disposable modality may have been artificially skewed by using daily disposable lenses as a problem solver. Other more recent studies have also investigated daily disposable wear and contact lens dropout. A study by Sulley et al (2018) found no difference in the one year retention rate between new contact lens wearers wearing daily disposable lenses and reusable lenses.18 Pucker et al (2019) likewise evaluated clinical factors associated with contact lens dropout and failed to find an association between wear schedule and being a contact lens dropout.9 Finally, when considering comfort as a reason for contact lens dropout, Chalmers et al found no difference in comfort between daily disposable and reusable contact lens wear,30 although others report an increase in reported comfort by reusable contact lens wearers fit into daily disposable lenses suggesting greater comfort with daily disposable contact lenses.16,34 These data overall suggests that it is currently unclear how wear schedule affects the frequency of contact lens dropout in reusable contact lens wearers.
Ocular Surface Factors
A contact lens placed on the eye’s surface interacts directly with the cornea, conjunctiva, tear film, and eyelids.35 Any homeostatic imbalance caused by ocular surface conditions, such as dry eye or meibomian gland dysfunction, can become exacerbated by a contact lens and lead to contact lens discomfort or contact lens-induced dry eye.23,36 This issue as it relates to contact lens dropout has been specifically analyzed by Giannaccare et al (2016) via a retrospective analysis (n = 87).37 The authors found that compared to controls, subjects who had discontinued contact lens wear had lower/worse tear break up time and Schirmer test values, and higher/worse ocular surface disease index (OSDI) and corneal staining scores. These results suggest that patients with signs of dry eye such as quick tear film evaporation, poor tear production, and corneal irritation may be more likely to drop out of contact lenses.
To further elucidate clinical parameters that may be predictive of a contact lens wearer developing symptoms of discomfort, and thus having an increased risk of dropping out of contact lenses, Siddireddy et al enrolled 30 healthy, established contact lens wearers and performed assessments of ocular surface signs and symptoms.38 The investigators determined that worse tear film evaporation rate without contact lenses, palpebral conjunctival staining scores, and lid-parallel conjunctival folds were all acceptable predictors of contact lens discomfort. Furthermore, they concluded that evaluating the secretions of the meibomian glands (volume, quality, and expressibility) were strong predictors of contact lens discomfort. This agrees with Pucker et al (2019) who concluded that those successfully wearing contact lenses had less upper eyelid meibomian gland tortuosity whereas contact lens dropouts had more meibomian gland plugging in upper and lower eyelids and worse meibum quality in upper eyelids than successful wearers.9,39 Nevertheless, Pucker et al did not find any difference in meibomian gland atrophy grades between successful and lapsed contact lens wearers, and they did not find any significant differences in any other ocular surface factors such as tear break up time, tear meniscus height, or blepharitis when comparing successful and unsuccessful wearers. Consequently, based on these studies, one can conclude that evaluation of meibum quality in both upper and lower eyelids may be predictive of intolerant contact lens wear and that meibomian gland dysfunction should be regularly screened for and treated when managing contact lens wearers to help avoid contact lens dropout.
Combatting Contact Lens Dropout
Ensuring successful contact lens wear and reducing the chances of contact lens dropout can be beneficial for both patients and clinicians.11 Various targeted strategies can be used to help promote contact lens success, and these strategies should be employed in at least three different timepoints in a contact lens wearer’s life: first fitting, established wearer, and presbyopia. At these different stages, practitioners can employ evidenced-based strategies to target patients and help them avoid dropping out of contact lenses. The following section includes strategies based on the findings of the current review, which may be supported by mitigating factors that can contribute to discomfort symptoms. A full description of treating contact lens discomfort is outside of the scope of this manuscript, though a summary of the currently accepted treatment methods can be found in the Tear Film and Ocular Surface Society’s report on contact lens discomfort management and therapies.40
A study by Sulley et al (2017) found that after reviewing patient records, practitioners reported a dropout rate of 26% at 1 year of contact lens wear with close to 50% of those dropping out in the first two months.17 Prior to the first fitting, a thorough evaluation of the health of the ocular surface is necessary to determine potential risk factors for future dropout. These risk factors include signs of dry eye disease and meibomian gland dysfunction, which may increase the likelihood dropping out of contact lenses.9 After fitting a patient in a contact lens, regular follow up visits or calls can improve retention.17 Once the patient is an established wearer, identifying that the contact lens wearer is symptomatic is the first step in determining the likelihood of a patient dropping out of contact lenses. Established, psychometrically validated questionnaires such as the Contact Lens Dry Eye Questionnaire (CLDEQ)-8 or Standardized Patient Evaluation of Eye Dryness (SPEED) can be utilized to screen patients for the development of contact lens related dry eye and contact lens discomfort.41–43 However, pointed questions directed towards discerning hours of comfortable wear time may also prove useful in determining whether a management strategy is needed to prevent discontinuation of lens wear.10 With new wearers, handling and vision are primary reasons for contact lens dropout.18 Thus, picking lenses with an improved edge design and higher modulus may provide benefit.44 Practitioners should also consider fitting patients with low cylinder in toric lens designs to improve vision now that they are widely available since the top complaint of neophyte toric contact lens wearers who have dropped out of contact lenses is poor vision.17,18
One of the most common problems of patients struggling with soft contact lens wear is reduced end-of-day comfort; therefore, this topic should be regularly probed during patient history.14 Contact lens discomfort, encompassing symptoms such as discomfort, dryness, irritation, fatigue, etc, is the most common reason for contact lens dropout in established wearers and addressing the contributing factors may prevent contact lens dropout. Factors contributing to ocular discomfort can include contact lens parameters such as material, design, wear modality, and lens care solution, in addition to patient and environmental factors like age, gender, medications, and ocular surface health.23 A thorough review of these factors can be found in the Tear Film and Ocular Surface Society International Workshop on Contact Lens Discomfort: report of the contact lens materials, design, and care subcommittee.45
Presbyopia is a common condition that typically characterizes individuals over the age of 40 years and may necessitate correction of vision using multifocal contact lenses.46 These contact lenses have varying designs to provide correction at distance, near, and sometimes intermediate ranges. Poor vision and discomfort are often the primary reasons for discontinuation of contact lens wear in the presbyopic population.47–49 While there are large scale studies that failed to show a significant difference in success rates between presbyopic and non-presbyopic contact lens wearers,16 setting realistic expectations with “real world” testing of multifocal contact lenses and using the latest multifocal designs and materials may prove to be uniquely successful when fitting presbyopic patients. Unfortunately, conditions such as dry eye are more common in this group of patients,50 which is an additional hurdle that may promote contact lens dropout in presbyopic patients.51 Again, as described above, early treatment may promote additional years of comfortable contact lens use.9 Nevertheless, at every state of a contact lens wearer’s life, they should be offered an alternative contact lens option if they are struggling or if they have dropped out of lenses because research suggests that they may be able to resume contact lens wearer if they are given additional opportunities.16
Conclusions
Contact lens dropout is a highly prevalent condition that is most commonly attributed to discomfort in established contact lens wearers while new wearers most frequently dropout of contact lenses because of poor vision. While silicone hydrogel and daily disposable lenses are now easily available to practitioners, these innovations have not altered the frequency of contact lens dropout.10,13, 16–19 The literature provides convincing evidence that many contact lens dropouts can resume contact lens wear if they are simply offered an alternative contact lens modality; therefore, wearers should be closely followed-up to ensure adequate contact lens satisfaction, especially within the first two months of contact lens wear.17
Although factors such as age, sex, and wear schedule do not appear to clearly influence the frequency of contact lens dropout, meibomian gland dysfunction has been consistently found to promote contact lens dropout. Therefore, it should be screened for and treated when found to help mitigate the number of patients dropping out of contact lenses. Overall, this review indicates that while contact lens dropout is frequent, there are numerous options and strategies available for combating contact lens dropout.
Acknowledgments
No funding was specifically provided for the completion of this work.
Commercial Relationship Disclosures
The authors have received financial support from Alcon Research, LLC (ADP), Bausch & Lomb (ADP), Euclid Systems (ADP), Contamac (ADP), National Eye Institute (ADP, AAT), and Paragon Vision Sciences (ADP), and consulted for Alcon Research, LLC (ADP), CooperVision (ADP), EpiTech (ADP), EyeGate Pharmaceuticals, Inc (ADP), and Optikal Care Inc (ADP) over the past three years.
Disclosure
Dr Andrew D Pucker reports grants, personal fees from Alcon Research, LLC, grants from Bausch & Lomb, grants, personal fees from Euclid Systems, grants from Contamac, grants from National Eye Institute, grants from Paragon Vision Sciences, personal fees from CooperVision, personal fees from EpiTech, personal fees from EyeGate Pharmaceuticals, Inc, personal fees from Optikal Care Inc, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Terry RL, Schnider CM, Holden BA, et al. CCLRU standards for success of daily and extended wear contact lenses. Optom Vis Sci. 1993;70(3):234–243. doi:10.1097/00006324-199303000-00011
2. Walline JJ, Jones LA, Sinnott L, et al. Randomized trial of the effect of contact lens wear on self-perception in children. Optom Vis Sci. 2009;86(3):222–232. doi:10.1097/OPX.0b013e3181971985
3. McMonnies CW. Improving patient education and attitudes toward compliance with instructions for contact lens use. Cont Lens Anterior Eye. 2011;34(5):241–248. doi:10.1016/j.clae.2011.06.007
4. Smith MJ, Walline JJ. Controlling myopia progression in children and adolescents. Adolesc Health Med Ther. 2015;6:133–140. doi:10.2147/AHMT.S55834
5. Cho P, Cheung SW, Edwards M. The longitudinal orthokeratology research in children (LORIC) in Hong Kong: a pilot study on refractive changes and myopic control. Curr Eye Res. 2005;30(1):71–80. doi:10.1080/02713680590907256
6. Walline JJ, Greiner KL, McVey ME, Jones-Jordan LA. Multifocal contact lens myopia control. Optom Vis Sci. 2013;90(11):1207–1214. doi:10.1097/OPX.0000000000000036
7. Bullimore MA, Brennan NA. Myopia control: why each diopter matters. Optom Vis Sci. 2019;96(6):463–465. doi:10.1097/OPX.0000000000001367
8. Pritchard N, Fonn D, Brazeau D. Discontinuation of contact lens wear: a survey. Int Contact Lens Clin. 1999;26:157–162. doi:10.1016/S0892-8967(01)00040-2
9. Pucker AD, Jones-Jordan LA, Marx S, et al. Clinical factors associated with contact lens dropout. Cont Lens Anterior Eye. 2019;42(3):318–324.
10. Dumbleton K, Woods CA, Jones LW, Fonn D. The impact of contemporary contact lenses on contact lens discontinuation. Eye Contact Lens. 2013;39(1):93–99. doi:10.1097/ICL.0b013e318271caf4
11. Rumpakis JMB. New data on contact lens dropouts: an international perspective. Rev Optom. 2010;147:37–42.
12. S. B. Profile of contact lens failures in Saudi Arabia. Clin Exp Optom. 1996;79:255–259.
13. Nichols JJ. 2017 annual report: contact lenses 2016. Contact Lens Spectrum. 2018;33:22–25.
14. Hickson-Curran S, Spyridon M, Hunt C, Young G. The use of daily disposable lenses in problematic reusable contact lens wearers. Cont Lens Anterior Eye. 2014;37(4):285–291. doi:10.1016/j.clae.2014.03.002
15. Weed K, Fonn D, Potvin R. Discontinuation of contact lens wear. Optom Vis Sci. 1993;70(Suppl):140.
16. Young G, Veys J, Pritchard N, Coleman S. A multi-centre study of lapsed contact lens wearers. Ophthalmic Physiol Opt. 2002;22(6):516–527. doi:10.1046/j.1475-1313.2002.00066.x
17. Sulley A, Young G, Hunt C. Factors in the success of new contact lens wearers. Cont Lens Anterior Eye. 2017;40(1):15–24. doi:10.1016/j.clae.2016.10.002
18. Sulley A, Young G, Hunt C, McCready S, Targett M-T, Craven R. Retention rates in new contact lens wearers. Eye Contact Lens. 2018;44(Suppl 1):S273–S282. doi:10.1097/ICL.0000000000000402
19. Macedo-de-Araujo RJ, van der Worp E, Gonzalez-Meijome JM. A one-year prospective study on scleral lens wear success. Cont Lens Anterior Eye. 2019. doi:10.1016/j.clae.2019.10.140
20. Nichols JJ, Willcox MD, Bron AJ, et al. The TFOS international workshop on contact lens discomfort: executive summary. Invest Ophthalmol Vis Sci. 2013;54(11):TFOS7–TFOS13.
21. Schlanger JL. A study of contact lens failures. J Am Optom Assoc. 1993;64(3):220–224.
22. Cope JR, Collier SA, Nethercut H, Jones JM, Yates K, Yoder JS. Risk behaviors for contact lens-related eye infections among adults and adolescents - United States, 2016. MMWR Morb Mortal Wkly Rep. 2017;66(32):841–845. doi:10.15585/mmwr.mm6632a2
23. Nichols JJ, Willcox MDP, Bron AJ, et al. The TFOS International Workshop on contact lens discomfort: executive summary. Invest Ophthalmol Vis Sci. 2013;54(11):TFOS7–TFOS13.
24. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
25. Richdale K, Sinnott LT, Skadahl E, Nichols JJ. Frequency of and factors associated with contact lens dissatisfaction and discontinuation. Cornea. 2007;26(2):168–174. doi:10.1097/01.ico.0000248382.32143.86
26. Ramamoorthy P, Sinnott LT, Nichols JJ. Treatment, material, care, and patient-related factors in contact lens-related dry eye. Optom Vis Sci. 2008;85(8):764–772. doi:10.1097/OPX.0b013e318181a91f
27. Chalmers RL, Hunt C, Hickson-Curran S, Young G. Struggle with hydrogel CL wear increases with age in young adults. Cont Lens Anterior Eye. 2009;32(3):113–119. doi:10.1016/j.clae.2008.12.001
28. Young G, Chalmers R, Napier L, Kern J, Hunt C, Dumbleton K. Soft contact lens-related dryness with and without clinical signs. Optom Vis Sci. 2012;89(8):1125–1132. doi:10.1097/OPX.0b013e3182640af8
29. Stapleton F, Stretton S, Papas E, Skotnitsky C, Sweeney DF. Silicone hydrogel contact lenses and the ocular surface. Oculr Surf. 2006;4(1):24–43. doi:10.1016/S1542-0124(12)70262-8
30. Chalmers RL, Young G, Kern J, Napier L, Hunt C. Soft contact lens-related symptoms in North America and the United Kingdom. Optom Vis Sci. 2016;93(8):836–847. doi:10.1097/OPX.0000000000000927
31. Woods PBM, Tig CA, Efron N, Jones LW, Nelson L. International contact lens prescribing in 2019. Contact Lens Spectrum. 2020;35:26–32.
32. Sulley A, Dumbleton K. Silicone hydrogel daily disposable benefits: the evidence. Cont Lens Anterior Eye. 2020.
33. Stapleton F, Keay L, Edwards K, Holden B. The epidemiology of microbial keratitis with silicone hydrogel contact lenses. Eye Contact Lens. 2013;39(1):79–85. doi:10.1097/ICL.0b013e3182713919
34. Michaud L, Forcier P. Comparing two different daily disposable lenses for improving discomfort related to contact lens wear. Cont Lens Anterior Eye. 2016;39(3):203–209. doi:10.1016/j.clae.2015.11.002
35. Craig JP, Willcox MD, Argueso P, et al. The TFOS International Workshop on Contact Lens Discomfort: report of the contact lens interactions with the tear film subcommittee. Invest Ophthalmol Vis Sci. 2013;54(11):Tfos123–156. doi:10.1167/iovs.13-13235
36. Kojima T. Contact lens-associated dry eye disease: recent advances worldwide and in Japan. Invest Ophthalmol Vis Sci. 2018;59:DES102–DES108. doi:10.1167/iovs.17-23685
37. Giannaccare G, Blalock W, Fresina M, Vagge A, Versura P. Intolerant contact lens wearers exhibit ocular surface impairment despite 3 months wear discontinuation. Graefes Arch Clin Exp Ophthalmol. 2016;254(9):1825–1831. doi:10.1007/s00417-016-3400-4
38. Siddireddy JS, Tan J, Vijay AK, Willcox M. Predictive potential of eyelids and tear film in determining symptoms in contact lens wearers. Optom Vis Sci. 2018;95(11):1035–1045. doi:10.1097/OPX.0000000000001290
39. Pucker AD, Jones-Jordan LA, Marx S, et al. Clinical factors associated with contact lens dropout. Contact Lens Anterior Eye. 2019;42(3):318–324.
40. Papas EB, Ciolino JB, Jacobs D, et al. The TFOS International Workshop on Contact Lens Discomfort: report of the management and therapy subcommittee. Invest Ophthalmol Vis Sci. 2013;54(11):TFOS183–203. doi:10.1167/iovs.13-13166
41. Lopez-de la Rosa A, Arroyo-Del Arroyo C, Enriquez-de-Salamanca A, Pinto-Fraga J, Lopez-Miguel A, Gonzalez-Garcia MJ. The ability of the Contact Lens Dry Eye Questionnaire (CLDEQ)-8 to detect ocular surface alterations in contact lens wearers. Cont Lens Anterior Eye. 2019;42(3):273–277. doi:10.1016/j.clae.2018.11.012
42. Nichols JJ, Mitchell GL, Nichols KK, Chalmers R, Begley C. The performance of the contact lens dry eye questionnaire as a screening survey for contact lens-related dry eye. Cornea. 2002;21(5):469–475. doi:10.1097/00003226-200207000-00007
43. Pucker AD, Dougherty BE, Jones-Jordan LA, Kwan JT, Kunnen CME, Srinivasan S. Psychometric Analysis of the SPEED Questionnaire and CLDEQ-8. Invest Ophthalmol Vis Sci. 2018;59(8):3307–3313. doi:10.1167/iovs.18-24016
44. Tranoudis I, Efron N. Tensile properties of soft contact lens materials. Cont Lens Anterior Eye. 2004;27(4):177–191. doi:10.1016/j.clae.2004.08.002
45. Jones L, Brennan NA, Gonzalez-Meijome J, et al. The TFOS International Workshop on Contact Lens Discomfort: report of the contact lens materials, design, and care subcommittee. Invest Ophthalmol Vis Sci. 2013;54:TFOS37–70. doi:10.1167/iovs.13-13215
46. Wolffsohn JS, Davies LN. Presbyopia: effectiveness of correction strategies. Prog Retin Eye Res. 2019;68:124–143. doi:10.1016/j.preteyeres.2018.09.004
47. Rueff EM, Varghese RJ, Brack TM, Downard DE, Bailey MD. A survey of presbyopic contact lens wearers in a university setting. Optom Vis Sci. 2016;93(8):848–854. doi:10.1097/OPX.0000000000000881
48. Novillo-Diaz E, Villa-Collar C, Narvaez-Pena M, Martin JLR. Fitting success for three multifocal designs: multicentre randomised trial. Cont Lens Anterior Eye. 2018;41(3):258–262. doi:10.1016/j.clae.2017.12.012
49. Back A, Grant T, Hine N, Holden BA. Twelve-month success rates with a hydrogel diffractive bifocal contact lens. Optom Vis Sci. 1992;69(12):941–947. doi:10.1097/00006324-199212000-00006
50. de Paiva CS. Effects of aging in dry eye. International Ophthalmology Clinics. 2007;26(2):47–64. doi:10.1097/IIO.0000000000000170
51. Lafosse E, Wolffsohn JS, Talens-Estarelles C, Garcia-Lazaro S. Presbyopia and the aging eye: existing refractive approaches and their potential impact on dry eye signs and symptoms. Cont Lens Anterior Eye. 2020;43(2):103–114. doi:10.1016/j.clae.2019.08.005
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.