")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
A Retrospective Time Trend Study Of Diabetes Overtreatment In Geriatric Patients
Authors Wojszel ZB , Kasiukiewicz A
Received 1 July 2019
Accepted for publication 13 September 2019
Published 4 October 2019 Volume 2019:12 Pages 2023—2032
DOI https://doi.org/10.2147/DMSO.S221179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Zyta Beata Wojszel,1,2 Agnieszka Kasiukiewicz1,2
1Department of Geriatrics, Medical University of Bialystok, Bialystok, Poland; 2Department of Geriatrics, Hospital of the Ministry of Interior in Bialystok, Bialystok, Poland
Correspondence: Zyta Beata Wojszel
Department of Geriatrics, Medical University of Bialystok, Fabryczna street 27, Bialystok 15-471, Poland
Tel +48 85 8694 982
Fax +48 85 8694974
Email [email protected]
Purpose: We assessed changes in diabetes mellitus (DM) overtreatment prevalence in geriatric patients that had taken place after the introduction of the rule of therapy individualization in the Polish diabetes treatment guidelines.
Patients and methods: This time-trend assessment comprised two retrospective cross-sectional cohort studies of type 2 DM patients admitted to a geriatric ward in 2009–2010 (1st round) and in 2014–2015 (2nd round). A high-risk group was defined as patients on antihyperglycemic medications prior to admission, who were 80+ years old, diagnosed with dementia, end-stage renal disease, or had a history of macrovascular complications. The primary outcome measure was glycosylated A1C hemoglobin (HbA1C) ≤7.0% (53 mmol/mol).
Results: 213 patients in the 1st round and 83 in the 2nd round were included. Groups did not differ in age, gender, health and functional characteristics. The percentage of dementia (36.1% versus 18.8%, P=0.002) and of the high-risk cases (79.3% versus 67.7%, P=0.05) was higher in the 2nd round of the study. During the study, tight glycemic control prevalence in the high-risk group decreased significantly from 73.1% to 58.5%, P=0.04 (odds ratio 0.68, 95% CI 0.47–0.97), and the median value of HbA1c increased significantly from 6.4%, IQR 5.7–7.3 (46 mmol/mol, IQR 39–56) to 6.7%, IQR 6.1–7.9 (50 mmol/mol, IQR 43–63), P=0.03.
Conclusion: Despite the principle of individualization of DM therapy that was in force, after a five-year observation, the problem of DM overtreatment still concerned a large percentage of geriatric patients, although a positive trend was noted in this respect.
Keywords: type 2 diabetes, older people, therapy individualization, glycosylated A1C hemoglobin, HbA1c, tight control
Introduction
Diabetes mellitus (DM) is a common health condition in old age, connected with the higher rates of cardiovascular diseases, increasing risk of premature death and negatively effecting patients’ functional abilities and quality of life.1–5 There is no doubt at the moment that glycemic control targets in older patients with DM should be individualized, according to their functional status and comorbidities.6–8 The necessity of therapy individualization is extremely important in case of patients with limited ability to identify and manage hypoglycemia, with limited life expectancy, and especially in terminally ill patients. Therefore, in case of patients with multiple chronic illnesses, cognitive impairment, or functional dependence, less stringent glycemic goals are recommended.7,9
In spite of this recommendation, the problem of DM overtreatment in geriatric patients was described in some studies.10–12 We also observed a high prevalence of DM overtreatment in our previous cross-sectional study of the population of patients admitted to the geriatric ward in 2009–2010. The study was carried out just before the introduction of the principle of individualization of DM therapeutic goals for older people burdened with multimorbidity, and with short life expectancy.13 This principle was literally included in the guidelines of the Diabetes Poland Association (PTD) regarding DM treatment only in 2011.14 The lower glycemic goal (glycosylated A1C hemoglobin (HbA1C) ≤7% [53 mmol/mol]) was recommended for otherwise healthy, with few coexisting chronic illnesses, older patients with DM, whereas the new DM treatment goal, i.e. HbA1C <8% [64 mmol/mol], was proposed for older patients with long-term DM and vascular complications. This recommendation was retained in issued annual PTD guidelines, up to the last ones.8
Our aim was to assess whether the principle of individualization of DM therapy in the PTD guidelines was related to any change in DM overtreatment in patients with type 2 DM admitted to the geriatric ward, after five years of observation. To the authors’ knowledge, this is the first publication addressing the issue of implementation of the principle of DM therapy individualization in older patients in Poland from a long-term perspective.
Materials And Methods
This time-trend assessment comprised two retrospective cross-sectional cohort studies of type 2 DM patients; admitted to the geriatric ward between 1st January 2009 and 31st December 2010 (1st round),13 and between 1st September 2014 and 30th April 2015 (2nd round) – a secondary analysis of the study on frailty syndrome in patients of the geriatric ward.15 The study population included patients with type 2 DM, on antihyperglycemic medications (insulin and/or oral glucose-lowering agents) prior to admission, who were tested for Hb A1c during a stay in the ward. Medical records of all consecutive patients were analyzed.
The geriatric ward of the Hospital of the Ministry of Interior in Bialystok, Poland, is a sub-acute department. Older people with multimorbidity and physical/mental disability are referred to it by general practitioners or other specialists, and are admitted in a planned manner. A mean length of stay is 7 days, and a comprehensive geriatric assessment carried out by a multidisciplinary team, including reviewing and modifying patient’s pharmacotherapy, is one of the goals of hospitalization. Most often, therefore, it was not possible to indicate a single reason for hospitalization.
Classification Of Groups
The subjects were classified into two groups:
- A “high-risk group” was defined as patients on antihyperglycemic medications prior to admission, who were 80+ years old, diagnosed with dementia, end-stage renal disease or had a history of macrovascular complications.
- A “low-risk group” was defined as patients who did not meet the abovementioned criteria.
Study Parameters
End-stage stage chronic kidney disease (CKD) was defined as stage 4 and 5 CKD according to the Kidney Disease Outcome Quality Initiative (KDOQI)-glomerular filtration rate (GFR) <30 mL/min/1.73 m2. GFR was counted using the Cockcroft-Gault formula.16 Dementia diagnosis was based on the clinical neuropsychologist’s examination. Macrovascular complications included history of myocardial infarction (MI), coronary artery bypass graft (CABG), percutaneous transluminal coronary angioplasty (PTCA), stroke and transient ischemic attack (TIA). Only confirmed in medical records diagnoses were included.
Information on patients’ age, gender, place of residence (urban/rural), functional status (basic activities of daily living (ADL) assessed with the Barthel Index17 [range 0–100 points]; instrumental activities of daily living (IADL) assessed with the 6-item scale derived from the Duke OARS assessment that included activities such as housework, preparing own meals, using the telephone, handling money, shopping and taking medicines [range 0–12 points];18 risk of pressure sores assessed with the Norton scale [range 5–20 points; the score ≤14 points pointed to the increased risk]),19 on nutritional health (body mass index (BMI), number of lymphocytes in blood), depression, hypertension, orthostatic hypotension (diagnosed if systolic pressure decreased by 20 mm Hg or diastolic pressure decreased by 10 mmHg in the first or the third minute of the active standing test) and serum creatinine level were also collected. Hypoglycemic medications use (insulin, sulfonylurea, metformin or others) both prior to admission and recommended at discharge was evaluated. HbA1C measurements were made with the immunoinhibition method using an Olympus AU400 analyzer (Beckman-Coulter, Brea, CA, USA).
Outcome Measures
The primary outcome measure was HbA1C ≤7.0% (53 mmol/mol). We defined also three different thresholds of HbA1C:
- ≤7.0% [53 mmol/mol] and >6.5% [48 mmol/mol];
- ≤6.5% [48 mmol/mol] and >6.0% [42 mmol/mol];
- and ≤6.0% [42 mmol/mol]
that reflected increasingly tight glycemic control, and had been confirmed as connected with the increasing risk of hypoglycemia in older diabetic patients.20
Statistical Methods
IBM SPSS Version 18 Software suit (SPSS, Chicago, IL, USA) and STATISTICA 13.3 software package (TIBCO Software, Palo Alto, CA, USA) were used to analyze data collected. Shapiro–Wilk test was used to assess the distribution of variables. Data were presented as means and standard deviation for normally distributed, as medians and interquartile range for not normally distributed continuous variables, and as the number of cases and percentage for categorical variables. Proportions were compared using χ2 tests or Fisher exact test, as appropriate, while the independent samples Student’s t-test and Mann–Whitney U-test were used to compare means and medians. To assess differences between two dependent samples, Wilcoxon signed-rank test was used. Odds ratio for DM overtreatment in the 2nd round of the study, comparing to its 1st round, was calculated. Missing values were omitted and statistics in such cases were calculated for the adequately reduced groups. A P value of less than 0.05 was regarded as significant.
Results
213 patients in the 1st round and 83 in the 2nd round were included. Figure 1 shows patients’ enrolment in the study. Groups did not differ significantly in age, gender and in the majority of health and functional characteristics analyzed. The majority of them were women (165; 77.5% in the 1st round and 58; 69.9% in the 2nd one), aged 80 years or more (105; 49.3% in the 1st round and 49; 59% in the 2nd one). In the 2nd round of the study, the higher percentage of dementia (36.1% versus 18.8%, P=0.002) and of the “high-risk” cases (78.3% versus 61.0%, P=0.05) was observed (Table 1). A relatively small part of patients admitted to the geriatric ward (16% in the 1st round and 21.7% in the 2nd one) had HbA1C above 8% [64 mmol/mol]. In the majority of cases (69.5% in the 1st round and 56.6% in the 2nd one), HbA1C level was ≤7% [53 mmol/mol].
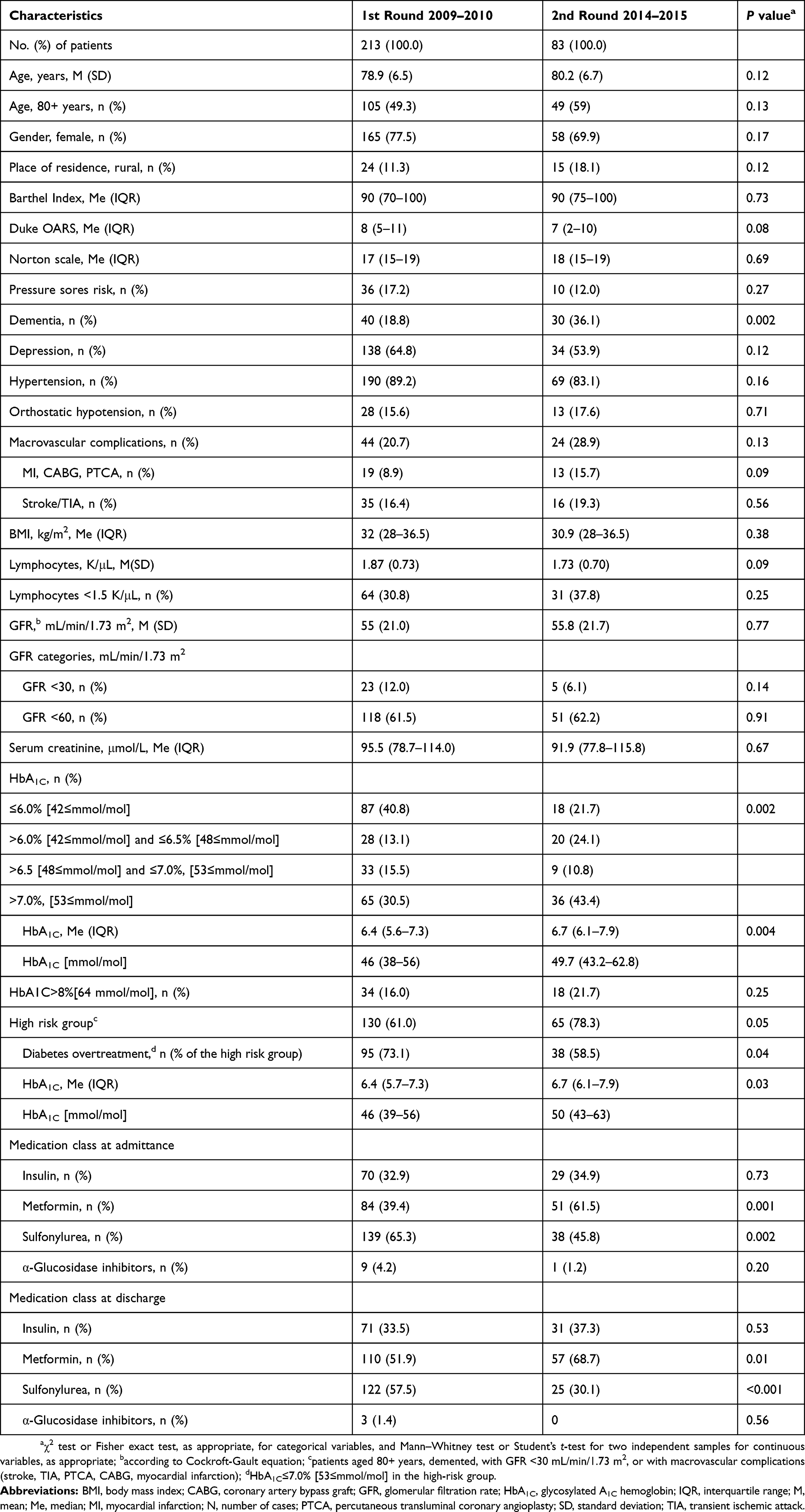 |
Table 1 Characteristics Of Patients In Two Rounds Of The Study |
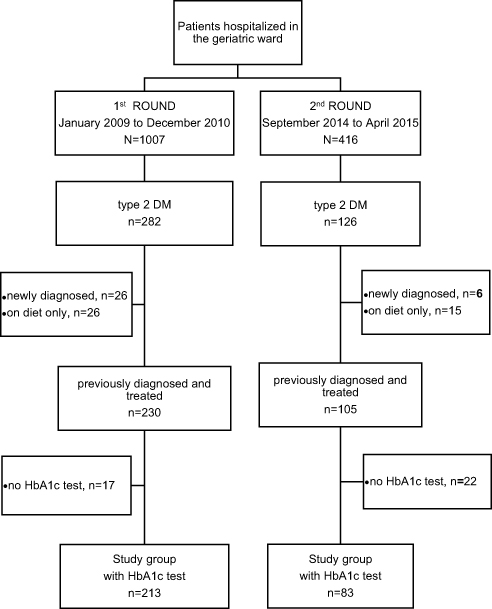 |
Figure 1 Flow chart of diabetes (DM) patients’ enrollment. |
We identified 130 (61%) patients in the 1st round and 65 (78.3%) patients in the 2nd round as the “high-risk” cases. Over the study period, tight glycemic control prevalence in the high-risk group decreased significantly from 73.1% to 58.5%, P=0.04 (odds ratios 0.68, 95% CI 0.47–0.97), and the median value of HbA1c increased significantly from 6.4%, IQR 5.7–7.3 [46 mmol/mol, IQR 39–56] to 6.7%, IQR 6.1–7.9 [50 mmol/mol, IQR 43–63], P=0.03. But still, very frequently very low values of HbA1C were observed in the high-risk population (Figure 2).
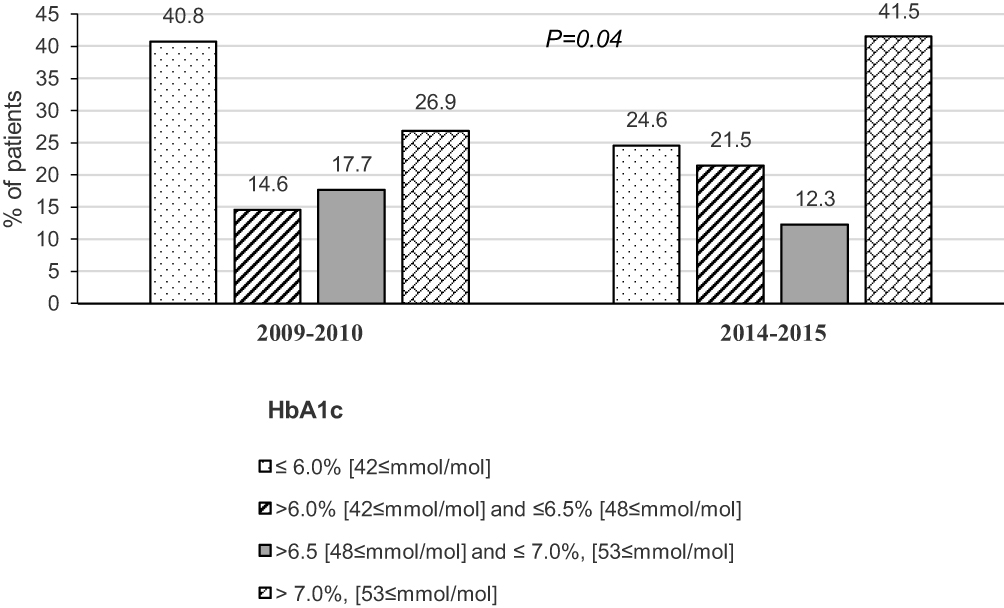 |
Figure 2 A distribution of HbA1c values in the high-risk group, in two rounds of the study. |
Sulfonylurea was the most frequently used hypoglycemic agent at admission to the ward in the 1st round of the study (65.3%), but its use at admittance decreased significantly in the study period to 45.8%, P=0.002. Metformin use in admittance increased significantly in the study period from 39.4% to 61.5%, P=0.001, and it was the most frequently used hypoglycemic agent at admittance in the 2nd round of the study. The study rounds did not differ in the frequency of insulin and α-glucosidase inhibitors usage. Other therapeutic options were absent in both rounds of the study. Metformin was used more frequently at discharge than at admission, and this change was significant only in the 1st round of the study, whereas sulfonylurea was used significantly less frequently at discharge than at admission in both rounds of the study (Table 2). Antidiabetic medications used by patients of the high-risk group before hospitalization, by level of glycemic control, are presented in Table 3. In two rounds of the study, tightly treated patients of the high-risk group did not differ in the percentage of patients taking metformin, sulfonylureas or α-Glucosidase inhibitors, but significantly less frequently were on insulin in the 1st round of the study, and the similar trend was observed in the 2nd round of the study.
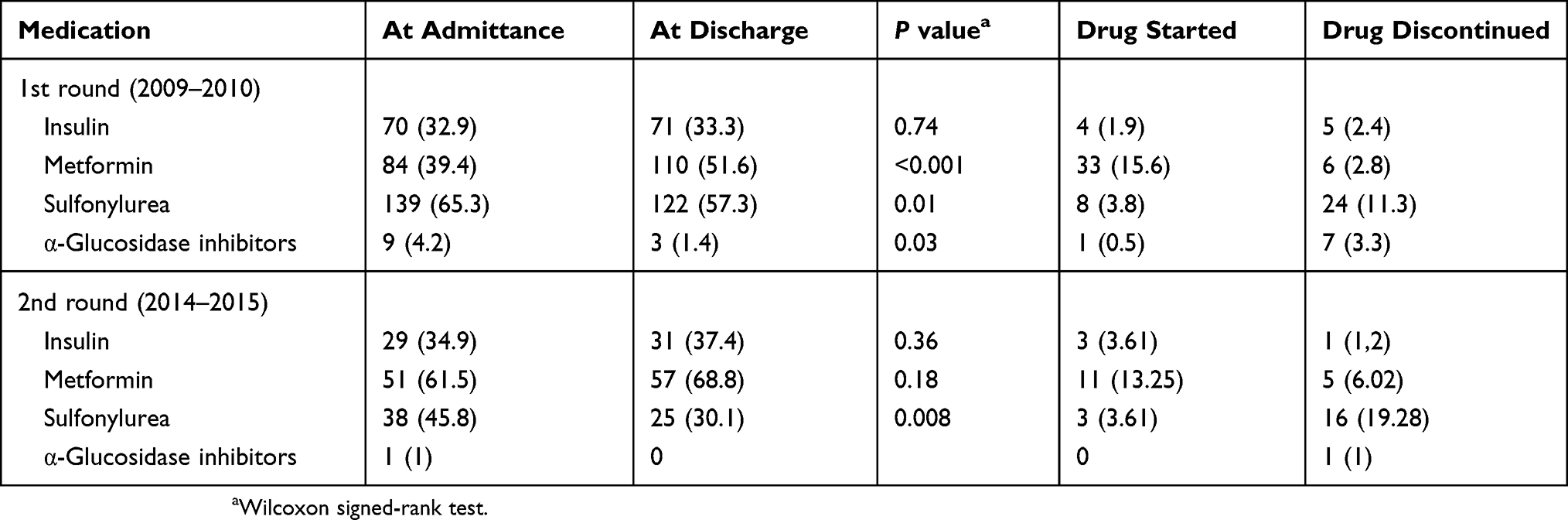 |
Table 2 Glucose-Lowering Medications Use At Admittance, And At Discharge From The Geriatric Ward, In Two Rounds Of The Study |
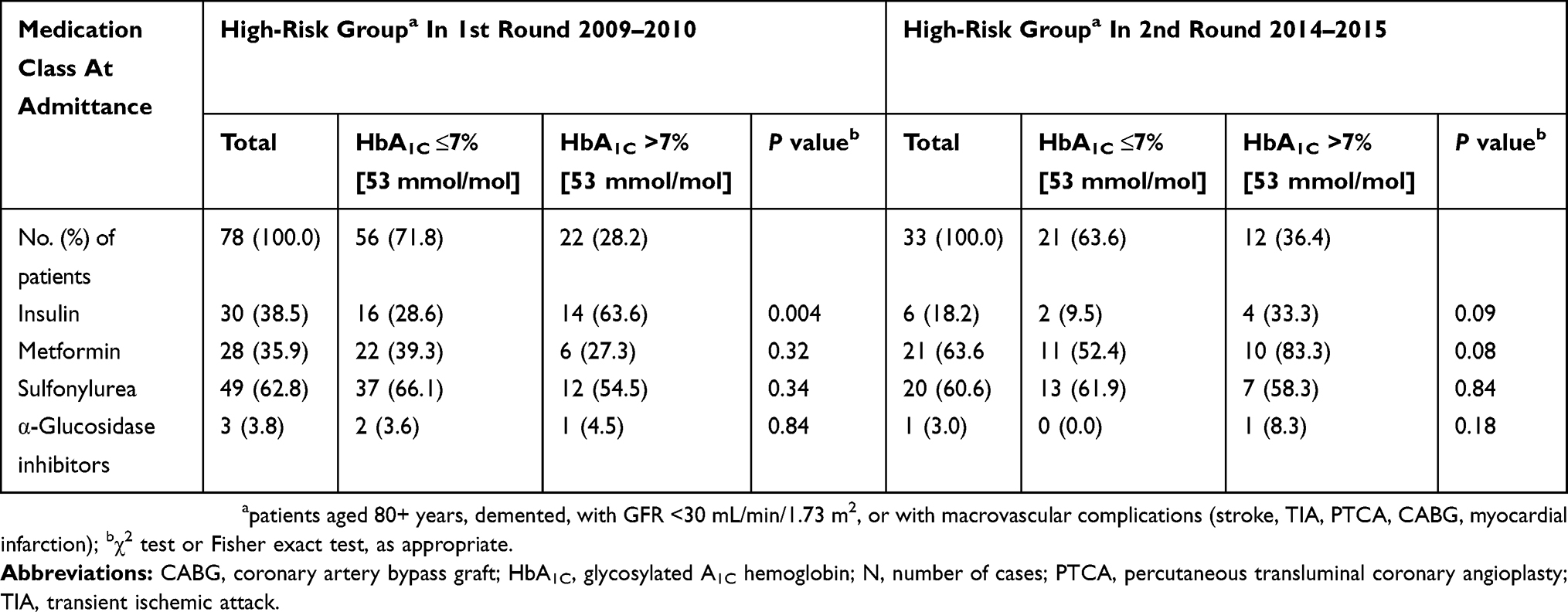 |
Table 3 Antidiabetic Medications At Admittance To The Geriatric Ward In The High-Risk Group In Two Study Rounds By Level Of Glycemic Control |
Discussion
Different studies highlighted the importance of recognizing frailty, or limited life expectancy, and supported the individualization of care in older people with DM.21 Despite clear guidelines recommending the higher glycemic targets in certain subgroups of older people, too tight glycemic control was noticed in some studies.10,11 It concerned also a high proportion of patients admitted to our geriatric ward in 2009–2010.13,22
In 2011, PTD guidelines on the management of diabetic patients in Poland literally took into account the earlier recommendations of international societies.14 Despite this change in the Polish guidelines, the current study confirmed that tight DM control was still a far more common in the group of older patients admitted to the geriatric ward than insufficient control of the disease. The HbA1C ≤7% [53 mmol/mol] was observed in almost 70% of the study participants in the 1st round (2009–2010) and in almost 60% of the 2nd round (2014–2015), but HbA1C below 6.5% [48 mmol/mol] had 53.9% and 45.8% patients in these rounds, respectively. In many studies, such low levels of HbA1C were associated with the increased risk of hypoglycemic episodes,23–25 although severe hypoglycemia was common among patients with type 2 DM across all levels of glycemic control in the Diabetes and Aging Study. Risk tended to be higher in patients with either near-normal glycaemia or very poor glycemic control.26 It is well known that not only lower average glucose levels, but also higher glucose variability indicate a greater hypoglycemia risk.27 Additionally, taking into consideration some authors’ observations, indicating that HbA1c levels may increase with age in patients without DM,28 the results of our study – pointing to the overtreatment of DM in geriatric patients – are even more alarming.
The “high-risk group” (“age 80+ years” or “end-stage renal disease”, or “dementia”, or “macrovascular complications”) constituted 67.7% of patients in 1st round and 79.3% in the 2nd round of our study. The abovementioned patients’ profile was connected with the limited life expectancy and the higher hypoglycemia risk.29–32 For these patients, less stringent glycemic goals were recommended,9 but 73.1% of them in the 1st round and 58.5% in the 2nd round had values of HbA1C ≤7.0% [53 mmol/mol]. It was confirmed in some studies that the prevalence of hypoglycemia increased significantly as HbA1C decreased.33 In both rounds of our study, a high percentage of patients had HbA1C values below 6.0% [42 mmol/mol]. Therefore, we can assume that episodes of hypoglycemia might have occurred frequently in the study groups before admission to the hospital, and might have been one of the reasons for the changes that were introduced in the treatment of DM during the stay of patients in the geriatric ward. Unfortunately, the retrospective nature of the study did not allow to assess this problem. However, it should be noted that over the course of 5 years of follow-up the decrease in the prevalence of too tight DM treatment was statistically significant, confirming that the principle of individualization of DM therapy in the elderly population had been better adhered to.
The type of agents used to treat DM may contribute to the risk of hypoglycemia. A patient-centered approach is recommended to guide the choice of pharmacologic treatment, and the medication regimen should be reevaluated at regular intervals, and adjusted as needed to incorporate new patient’s factors.34,35 Since many years now, metformin has been the preferred initial pharmacologic agent for the treatment of type 2 DM, and once initiated it was recommended to continue it as long as it was tolerated, and not contraindicated. The study showed that the frequency of metformin use in patients admitted to the geriatric ward had increased significantly over the years of follow-up, and changes in metformin prescribing during the hospital stay were no longer significant in the 2nd round of the study. The approval for metformin up to GFR of 30 mL/min/1.73 m2 that took place between the study rounds certainly could have contributed to this. Contrary to that, although the frequency of sulfonylurea use had decreased significantly over the study period, the sulfonylurea was still often discontinued during patients stay in the geriatric ward. It had been confirmed that sulfonylurea was associated with the high risk of hypoglycemia and alternative hypoglycemic agents should be considered rather, when metformin was not tolerated or contraindicated in the older patient.36 In the last PTD recommendations for the treatment of DM, sulfonylureas were placed at a distant place in the treatment regimen,8 but they were one of the foremost groups of drugs in DM in the period covered by our study. Some studies revealed that the highest risk of hypoglycemia is under intensive insulin therapy;37 however, this treatment strategy is not very common in patients of advanced old age.38 Moreover, tightly treated patients less frequently were on insulin, and our previous analysis of the first round of the study had confirmed that insulin intake was a negative predictor of low HbA1C values in our patients.13 This could have been the result of a large variation in glycemic values in these patients, but also the consequence of a different level of care (including medical) provided to these patients, although data gathered in our study did not allow us to verify that.
In patients with established atherosclerotic cardiovascular disease, or CKD, sodium–glucose cotransporter 2 (SGLT2) inhibitors, or glucagon-like peptide 1 (GLP1) receptor agonists are safer, and their use brings additional benefits and improves prognosis.39–41 These drug groups were not completely taken by our patients in both rounds of our study. We can assume that it was largely due to financial constraints, as SGLT2 inhibitors and GLP1 receptor agonists were (and still are) rather expensive, and not refunded in the Polish health care system. For many years now, the PTD has been unsuccessfully made efforts to include these drugs on the reimbursement lists. Inadequate management of DM is more common in patients with poor societal conditions,42 so screening for that is recommended.43 Unfortunately, the study design did not allow to analyze social determinants of health in our patients. But we should be aware that each of the new groups of antidiabetic medications also comes with its own unique advantages and safety profile, so a personalized case by case approach should be adopted while establishing treatment strategy for older patients, after weighing the overall risks and benefits of therapy. Therefore, for instance, treatment with SGLT 2 inhibitors in elderly people may be problematic, as it requires a special body hygiene, which is often difficult to keep for patients with physical disability or dementia.
Limitations And Strengths
The strength of this study is the use of the real-world data. It was not based on administrative claims, but we have evaluated the problem of DM treatment in old age from the perspective of everyday clinical practice. Our study was not a randomized clinical trial, but included older patients burdened with disability and multimorbidity, usually excluded from most clinical trials. Furthermore, this is the first study to investigate the problem of implementation of the principle of DM therapy individualization in older patients in Poland from a long-term perspective.
However, some limitations of this study are worth mentioning. First of all, it was performed not in the sample randomly selected from the general population of older people, but in the convenient sample of patients admitted to one geriatric ward, so the results can be generalized for the patients of similar characteristics (in more advanced age, more disabled and with different geriatric syndromes, such as dementia, depression, malnutrition, dependence on others in activities of daily living). The multicenter study would increase the external validity of the results. Some limitations of our study resulted from its retrospective design and secondary analysis of data collected in previously conducted studies. Thus, we were unable to determine, for example, how the dose of hypoglycemic medications was modified, or what the specific reason for the absence of new, safer drug groups in treatment regimens was. The availability of data on the frequency of hypoglycaemia in the last year was also limited, so there was no possibility to analyze that. The consequence of the secondary analysis of earlier studies was also the different number of patients recruited for them.
Conclusion
Despite the principle of individualization of DM therapy that was in force, after five-year observation the problem of DM overtreatment still concerned a large percentage of geriatric patients, although a positive trend was noted in this respect.
This may indicate the need to further broaden the knowledge of doctors about the specificity of DM treatment in older patients, with particular emphasis on the high-risk of hypoglycemia groups. It is also worth considering changing system solutions in the care of these patients, taking also into account the social determinants of health. It seems that there is an urgent need to facilitate older patients access to new hypoglycemic medications associated with lower risk of hypoglycemia, by including them in the reimbursement lists.
Abbreviations
BMI, body mass index; CABG, coronary artery bypass graft; CKD, chronic kidney disease; GLP1, glucagon-like peptide-1; GFR, glomerular filtration rate; HbA1C, glycosylated A1C hemoglobin; IQR, interquartile range; KDOQI, the Kidney Disease Outcome Quality Initiative; M, mean; Me, median; MI, myocardial infarction; N, number of cases; OARS, Older Americans Resources and Services; PTCA, percutaneous transluminal coronary angioplasty; PTD, the Diabetes Poland association; SD, standard deviation; SGLT2, sodium/glucose cotransporter 2; TIA, transient ischemic attack.
Ethics Approval And Informed Consent
This was a secondary analysis of data collected in the previous studies, approved by the Ethics Committee at Medical University in Bialystok. The need to obtain participants consent in the first round of the study was waived by the ethics committee as it was a retrospective study and only medical records were analyzed. All study participants taking part in the second round gave their informed consent to participate. Permission for accessing patients’ medical records was granted by the Director of the Hospital of the Ministry of Interior in Bialystok, Poland. All procedures performed were in accordance with the ethical standards of the Medical University of Bialystok Research Committee and with the Helsinki Declaration, and its later amendments. The study can be classified as a study of “usual practice”.
Availability Of Data And Material
The data supporting the results in the current study are available from the corresponding author on reasonable request.
Acknowledgments
This work was supported in part by funds of the Medical University of Bialystok research projects: 123-01651 P/2012 (1st round of the study) and N/ST/ZB/15/001/3301 (2nd round of the study), both granted to ZBW. The study was designed and run independently of the funding body. An abstract of this work was submitted to the 15th International Congress of the European Geriatric Medicine Society; Cracow, Poland (September 25–27, 2019; published in Eur Geriatr Med, 2019;10(Suppl 1):147).
Author Contributions
Both authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McDonald M, Hertz RP, Unger AN, Lustik MB. Prevalence, awareness, and management of hypertension, dyslipidemia, and diabetes among United States adults aged 65 and older. J Gerontol A Biol Sci Med Sci. 2009;64(2):256–263. doi:10.1093/gerona/gln016
2. Du Y, Heidemann C, Gosswald A, Schmich P, Scheidt-Nave C. Prevalence and comorbidity of diabetes mellitus among non-institutionalized older adults in Germany - results of the national telephone health interview survey ‘German Health Update (GEDA)’ 2009. BMC Public Health. 2013;13:166. doi:10.1186/1471-2458-13-166
3. Sanchez Martinez M, Blanco A, Castell MV, et al. Diabetes in older people: prevalence, incidence and its association with medium- and long-term mortality from all causes. Aten Primaria. 2014;46(7):376–384. doi:10.1016/j.aprim.2013.12.004
4. Yang YC, Lin MH, Wang CS, et al. Geriatric syndromes and quality of life in older adults with diabetes. Geriatr Gerontol Int. 2019. doi:10.1111/ggi.13654
5. Espelt A, Borrell C, Palencia L, et al. Socioeconomic inequalities in the incidence and prevalence of type 2 diabetes mellitus in Europe. Gac Sanit. 2013;27(6):494–501. doi:10.1016/j.gaceta.2013.03.002
6. American Diabetes A. 6. Glycemic targets: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S61–S70. doi:10.2337/dc19-S006
7. American Diabetes A. 12. Older adults: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S139–S147. doi:10.2337/dc19-S012
8. Diabetes Poland. 2019 Guidelines on the management of diabetic patients. A position of Diabetes Poland. Clin Diabetol. 2019;8(1):1–97. doi:10.5603/DK.2019.0001
9. Yun JS, Ko SH. Risk factors and adverse outcomes of severe hypoglycemia in type 2 diabetes mellitus. Diabetes Metab J. 2016;40(6):423–432. doi:10.4093/dmj.2016.40.6.423
10. Thorpe CT, Gellad WF, Good CB, et al. Tight glycemic control and use of hypoglycemic medications in older veterans with type 2 diabetes and comorbid dementia. Diabetes Care. 2015;38(4):588–595. doi:10.2337/dc14-0599
11. Lipska KJ, Ross JS, Miao Y, Shah ND, Lee SJ, Steinman MA. Potential overtreatment of diabetes mellitus in older adults with tight glycemic control. JAMA Intern Med. 2015;175(3):356–362. doi:10.1001/jamainternmed.2014.7345
12. Muller N, Khunti K, Kuss O, et al. Is there evidence of potential overtreatment of glycaemia in elderly people with type 2 diabetes? Data from the GUIDANCE study. Acta Diabetol. 2017;54(2):209–214.
13. Wojszel ZB, Kasiukiewicz A. A retrospective cross-sectional study of type 2 diabetes overtreatment in patients admitted to the geriatric ward. BMC Geriatr. 2019;19(1):242. doi:10.1186/s12877-019-1256-2
14. Polish Diabetes Association. Clinical recommendations for the management of patients with diabetes 2011. Diabetol Prakt. 2011;12:(Suppl A):A1-A46.
15. Kasiukiewicz A, Wojszel ZB, Klimiuk K, Kuprjanowicz B, Bień B. The prevalence of the frailty syndrome among patients admitted to a geriatric ward – a retrospective study.
16. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. doi:10.1159/000180580
17. Mahoney FI, Barthel DW. Functional evaluation: the barthel index. Md State Med J. 1965;14:61–65.
18. Fillenbaum GG, Smyer MA. The development, validity, and reliability of the OARS multidimensional functional assessment questionnaire. J Gerontol. 1981;36(4):428–434. doi:10.1093/geronj/36.4.428
19. Norton D, McLaren R, Exton-Smith AN. An Investigation of Geriatric Nursing Problems in Hospital. Edinburgh; New York: Churchill Livingstone; 1975.
20. Boussageon R, Bejan-Angoulvant T, Saadatian-Elahi M, et al. Effect of intensive glucose lowering treatment on all cause mortality, cardiovascular death, and microvascular events in type 2 diabetes: meta-analysis of randomised controlled trials. BMJ. 2011;343:d4169. doi:10.1136/bmj.d4169
21. Hubbard RE, Andrew MK, Fallah N, Rockwood K. Comparison of the prognostic importance of diagnosed diabetes, co-morbidity and frailty in older people. Diabet Med. 2010;27(5):603–606. doi:10.1111/j.1464-5491.2010.02977.x
22. Wojszel ZB, Kasiukiewicz A, Klimiuk K, Wojskowicz A. Control of carbohydrate metabolism in patients with diabetes admitted to the geriatrics department - retrospective analysis [Polish]. Diabetol Klin. 2013;2(2):68.
23. Hay LC, Wilmshurst EG, Fulcher G. Unrecognized hypo- and hyperglycemia in well-controlled patients with type 2 diabetes mellitus: the results of continuous glucose monitoring. Diabetes Technol Ther. 2003;5(1):19–26. doi:10.1089/152091503763816427
24. Diabetes Control Complications Trial Research Group, Nathan DM, Genuth S, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977–986. doi:10.1056/NEJM199309303291401
25. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–853.
26. Lipska KJ, Warton EM, Huang ES, et al. HbA1c and risk of severe hypoglycemia in type 2 diabetes: the Diabetes and Aging Study. Diabetes Care. 2013;36(11):3535–3542. doi:10.2337/dc13-0610
27. Ishikawa T, Koshizaka M, Maezawa Y, et al. Continuous glucose monitoring reveals hypoglycemia risk in elderly patients with type 2 diabetes mellitus. J Diabetes Investig. 2018;9(1):69–74. doi:10.1111/jdi.12676
28. Roth J, Muller N, Lehmann T, Heinemann L, Wolf G, Muller UA. HbA1c and age in non-diabetic subjects: an ignored association? Exp Clin Endocrinol Diabetes. 2016;124(10):637–642. doi:10.1055/s-0042-105440
29. Prinz N, Stingl J, Dapp A, et al. High rate of hypoglycemia in 6770 type 2 diabetes patients with comorbid dementia: a multicenter cohort study on 215,932 patients from the German/Austrian diabetes registry. Diabetes Res Clin Pract. 2016;112:73–81. doi:10.1016/j.diabres.2015.10.026
30. Alsahli M, Gerich JE. Hypoglycemia in patients with diabetes and renal disease. J Clin Med. 2015;4(5):948–964. doi:10.3390/jcm4050948
31. Nicolucci A, Prosperini G, Buzzetti R, et al. A multistep approach for the stratification of the risk of severe hypoglycemia in patients with type 2 diabetes. Minerva Endocrinol. 2018;43(4):501–510. doi:10.23736/S0391-1977.18.02850-X
32. Borzi V, Frasson S, Gussoni G, et al. Risk factors for hypoglycemia in patients with type 2 diabetes, hospitalized in internal medicine wards: findings from the FADOI-DIAMOND study. Diabetes Res Clin Pract. 2016;115:24–30. doi:10.1016/j.diabres.2016.01.020
33. Yu S, Fu AZ, Engel SS, Shankar RR, Radican L. Association between hypoglycemia risk and hemoglobin A1C in patients with type 2 diabetes mellitus. Curr Med Res Opin. 2016;32(8):1409–1416. doi:10.1080/03007995.2016.1176017
34. Karter AJ, Warton EM, Lipska KJ, et al. Development and validation of a tool to identify patients with type 2 diabetes at high risk of hypoglycemia-related emergency department or hospital use. JAMA Intern Med. 2017;177(10):1461–1470. doi:10.1001/jamainternmed.2017.3844
35. American Diabetes A. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S90–S102. doi:10.2337/dc19-S009
36. Yu O, Azoulay L, Yin H, Filion KB, Suissa S. Sulfonylureas as initial treatment for type 2 diabetes and the risk of severe hypoglycemia. Am J Med. 2018;131(3):317e31–317e322. doi:10.1016/j.amjmed.2017.09.044
37. Muller N, Lehmann T, Gerste B, et al. Increase in the incidence of severe hypoglycaemia in people with type 2 diabetes in spite of new drugs: analysis based on health insurance data from Germany. Diabet Med. 2017;34(9):1212–1218. doi:10.1111/dme.13397
38. Kokoszka A, Kot W. Relationship of the patient age and intensity of type 2 diabetes treatment. Pol Arch Med Wewn. 2007;117(9):396–401.
39. Bonaventura A, Carbone S, Dixon DL, Abbate A, Montecucco F. Pharmacologic strategies to reduce cardiovascular disease in type 2 diabetes mellitus: focus on SGLT-2 inhibitors and GLP-1 receptor agonists. J Intern Med. 2019. doi:10.1111/joim.12890
40. Dekkers CCJ, Gansevoort RT, Heerspink HJL. New diabetes therapies and diabetic kidney disease progression: the role of SGLT-2 inhibitors. Curr Diab Rep. 2018;18(5):27. doi:10.1007/s11892-018-1107-0
41. Sajja AP, Dey AK, Guha A, Elnabawi Y, Joshi AA, Kalra A. SGLT-2 inhibitors and GLP-1 agonists: first-line therapy for diabetes with established cardiovascular disease. J Cardiovasc Pharmacol Ther. 2019;1074248419838511.
42. Walker RJ, Strom Williams J, Egede LE. Influence of race, ethnicity and social determinants of health on diabetes outcomes. Am J Med Sci. 2016;351(4):366–373. doi:10.1016/j.amjms.2016.01.008
43. Andermann A. Screening for social determinants of health in clinical care: moving from the margins to the mainstream. Public Health Rev. 2018;39:19. doi:10.1186/s40985-018-0094-7
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.