")
Back to Journals » International Medical Case Reports Journal » Volume 14
A Recurrent Synovial Osteochondromatosis of the Knee: A Case Report
Authors Manandhar S , Li J, Lu XC, Zhang Y, Zhang Y, Liu Y, Zhang C
Received 23 November 2020
Accepted for publication 12 January 2021
Published 10 February 2021 Volume 2021:14 Pages 67—72
DOI https://doi.org/10.2147/IMCRJ.S292283
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Sripur Manandhar, Jiazhen Li, Xin-Chang Lu, Yan Zhang, Yi Zhang, Yongkui Liu, Chao Zhang
Department of Orthopedics, First Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China
Correspondence: Jiazhen Li
Department of Orthopedics, First Affiliated Hospital of Zhengzhou University, No. 1 Jianshe East Road, Zhengzhou, 450052, People’s Republic of China
Tel +8613803853758
Email [email protected]
Abstract: We report a case of a farmer who presented with synovial osteochondromatosis of his right knee that mimicked a huge hardball. A synovial proliferative disease associated with metaplasia of cartilage resulting in sporadic multiple intra-articular and extra-articular loose bodies. Our focus is to report a rare case successfully operated which has an educational significance in clinical practice.
Keywords: synovial osteochondromatosis, osteocartilaginous nodules, chondrosarcoma, synovial sarcoma, synovectomy
Introduction
Synovial osteochondromatosis is an unusual benign (non-cancerous) pathological condition characterized by the formation of cartilage with synovial metaplasia, the synovium, which is the thin layer of tissue that lines the joints.1,2 Synovium is the specialized connective tissue that envelops diarthrodial joints and maintains a fluid-filled cavity to provide a lubricating environment for the articulating surfaces and has phagocytosis and immune function.3 Synovial osteochondromatosis can arise in any joint in your body, but the knee is most common.
Due to its rarity of the disease adequate radiological investigations, as well as pathological examination, are required for supporting the final decisive diagnosis.4 Surgical lavage and complete excision is preferred treatment because radiotherapy and chemotherapy have no effect on it and if it is uncontrollable then its progression might lead to chondrosarcoma, during which preferable final treatment applied for it is amputation.4–6 Secondary chondrosarcoma are malignant ones that arise from benign solitary and multiple osteochondromas which affects more in young patients and involves soft tissues more quickly than the primary central.7
Case Report
A 47-year-old white man who was a farmer and hailing from Liang Yuan Park, Shang Qiu City, Henan, China, sought the services of the First affiliated hospital of Zhengzhou University in the Department of Orthopedics, with a complaint of 5-month-old history of pain and swelling in his right knee.
The patient reported that he had undergone surgery in 2015 in a local hospital with the same diagnosis on his same right knee. The mass which was excised from the popliteal region of the knee at that year was 17 X 10 X 3 cm. Post-operatively, only for a month or so, he had to use crutches for walking, and then he continued his normal daily activities without pain and discomfort. He had no problem whatsoever until his recent development of complaints. His old radiological images were not available.
Around 5 months earlier, he suddenly felt pain with swelling in the same knee but the swelling was not on his popliteal region rather more pronounced anteriorly, laterally, and medially. His pain progressed from sporadic to become continuous with its intensity to be much higher than his previous state. His ROM gradually decreased with time as was the size of the lesion. For the last few months, the patient has had great difficulty in extending and flexing his right knee. He then had to again start using crutches for movement.
On physical examination, the patient presented, on inspection, increased volume in the anterior, laterally, and medial region of the knee, edema (++/5+), non-tender, hard texture, and mildly high temperature on palpation in comparison to the left knee. There were not any varicose veins or any other neurological deficits. The mass mimicked a huge hardball mass measuring around 35.0 x 25.0 x 20.0 cm which adhered to the surrounding tissues. [Figure 1] Due to the huge mass ROM as well as muscle strength was restricted, the active knee flexion was possible till 35°, knee extension 10°, knee internal rotation 5° and external rotation 20° whereas passive knee flexion up to 45°, knee extension 10°.8
 |
Figure 1 Pre-operative photograph of the swelling over the right knee. |
Radiographs of the knee were requested, and these showed an image of a sporadic osteoblastic mass spread in an area measuring 30.0 x 20.0 cm2. [Figure 2] For a greater understanding of the diagnosis, magnetic resonance imaging, and Computed Tomography scans of the right knee were requested. This showed that there was a well-delimited mass in the suprapatellar including the infrapatellar region that did not have a malignant appearance.
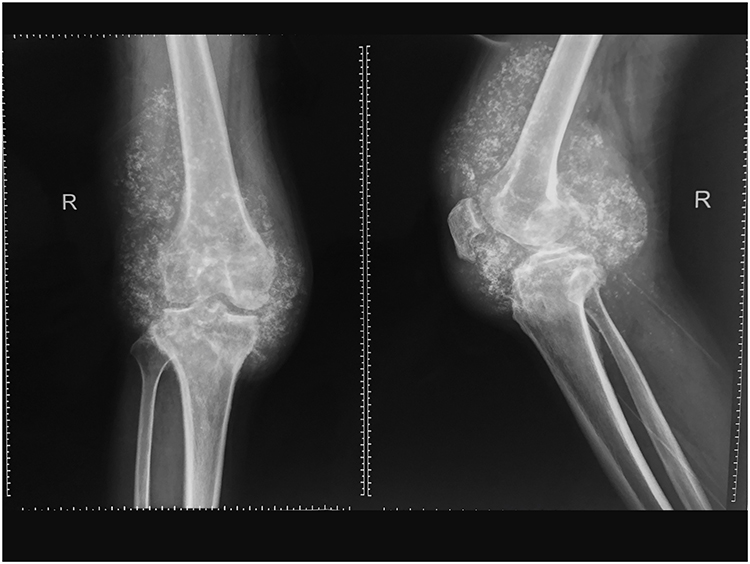 |
Figure 2 X-rays (AP/Lateral) depicting the multiple soft tissue calcification within and outside the joint capsule of the right knee. |
The patient was treated surgically, with excision of the mass. The incision was about 15 cm in length and was exposed layer to layer showing the ankylosis and obvious swelling of the knee region. After exposure bony lesions were found to be adhered to the soft tissues in cluster form with unclear boundaries and local infiltration internally. [Figure 3] The multi osteocartilaginous nodules anterior to the femur were excised in blocks while the patella which was engulfed and eroded by the lesion was scrapped, repaired, and was protected. In the posterior region, few lesions were entangled with blood vessels and nerves so it was not excised completely. As complete excision of the tumor lesions was not possible there is a high chance of recurrence and it was informed to the family members. The knee replacement is not feasible in his case therefore patient was counseled for it might eventually lead to amputation. The resected mass was sent for histopathological examination. [Figure 4] Microscopic examination in Hematoxylin Eosin staining was done and was observed in 40x, 100x, 200x, 400x magnifications. [Figure 5A–D] The result of the histopathological examination was that this was a case of synovial osteochondromatosis.
 |
Figure 3 Intra-operative (anterior approach) photograph showing the nature of the synovial osteochondromatosis. |
 |
Figure 4 Multiple cartilaginous loose bodies found in the joint cavity excised and sent for biopsy. |
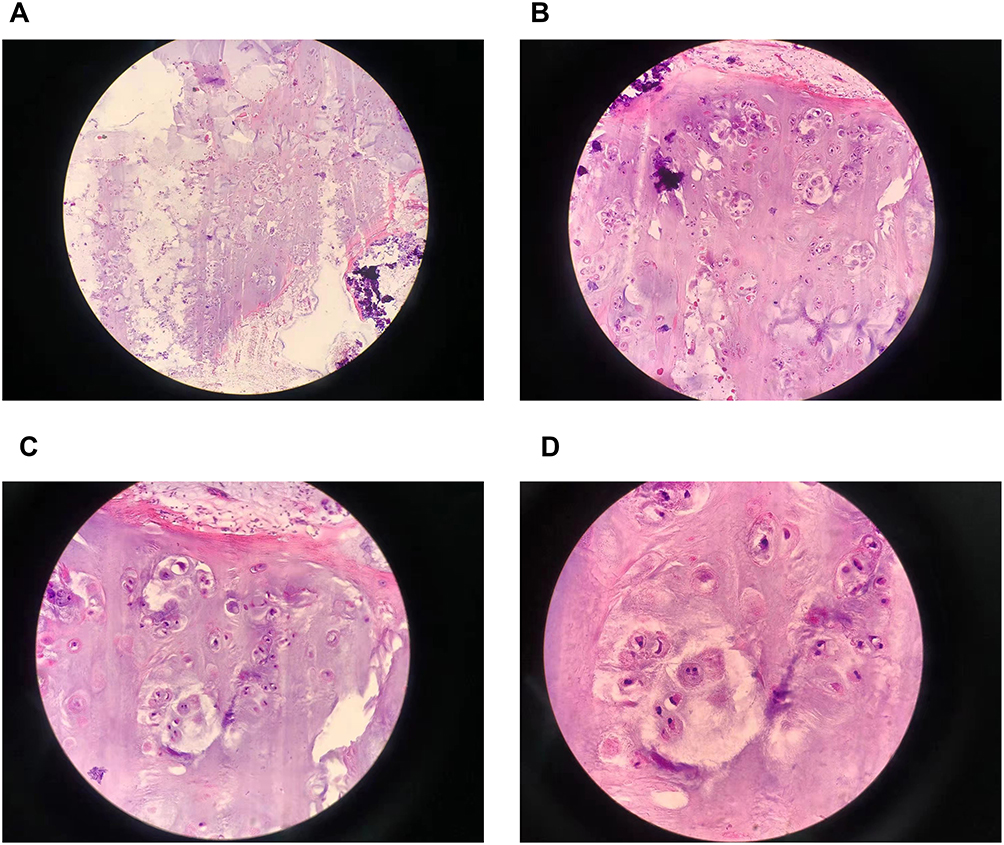 |
Figure 5 Photomicrograph histopathology of the biopsy showing, synovial hyperplasia, synovial loose bodies, sub synovial cartilaginous nodules (Hematoxylin Eosin staining Original magnification 40× in A, 100× in B, 200× in C, and 400× in D). |
Besides some changes in skin color and slight numbness felt in the operated region which eventually regressed. The postoperative was uneventful and the patient was released for physiotherapy after the stitches had been removed and have been advised to use crutches for 3 weeks and with advice for physiotherapy for muscle strengthening exercises. Due to the recurrence and lesions being entangled to nerves and vessels, he has been counseled and called for a follow-up and explained the possibility of amputation if his knee troubled him again.
Outcomes
On follow-up the patient’s symptoms have improved significantly. His ROM has improved, his knee flexion is around 80°, knee extension almost 0°, internal knee rotation is around 10° external knee rotation 30°, therefore no more uses crutches for walking. He does not have other deficits. The patient is doing fine right now.
Discussion
Synovial osteochondromatosis is an unusual condition of unknown cause. It may be idiopathic or secondary to diseases such as osteoarthrosis neuropathic arthropathy, osteoarthritis among others. It generally monoarticular but rarely bilateral, affecting predominantly the knee, hip, or elbow, and it’s mostly intra-articular.5 It affects 2times more in males than in females, with maximum occurrence in the age group 20–40 years.9 Patients generally complain of pain, edema, and ROM restriction of the affected joint and aggravated by infection or trauma.
It’s a progressive pathological disease with rare cases of spontaneous regression.10 There is a chance of malignant transformation so any patients with rapid late deterioration of symptoms should be evaluated for chondrosarcoma or synovial sarcoma.11,12 The treatment is surgical, it includes complete excision of any intra-articular body and resection of the synovial membranes involved, although complete removal is tough at times causing early recurrences.2 Numerous surgeons agree on the complete evacuation of every single body with subtotal synovectomy. Whereas due to the chances of recurrence, it is better to do a total synovectomy including extraction of all those involved bursae.13
The histological findings hyperplasia of the synovial membrane with foci of cartilaginous metaplasia. In this report, we described a case of synovial osteochondromatosis of the knee in a farmer that mimicked a huge hardball. The case was diagnosed and managed in accordance with the literature.
Lessons, Take Home Message
Synovial osteochondromatosis in the knee region is a rare pathology, nevertheless, it should not be left out in the differential diagnosis with patients with swelling, pain, and other symptoms.11 As the excision was not completely evacuated previously, it led to recurrence with more severity. We recommend surgical management with total synovectomy and complete excision of the occupying lesions including every single free body when the lesion causes symptoms and neurological deficits.
Consent to Publish
This is a case report for which the patient had no objections and therefore provided written informed consent, for publication of his case detail, and the accompanying images. The images did not contain any patient records and personal information. Institutional approval was not required for this case report.
Acknowledgment
The authors would like to thank Dr. Qian Du, MD Department of Pathology of First Affiliated Hospital of Zhengzhou University, Zhengzhou, China for her valuable contributions in pathological data analysis and her help in revision of the paper.
Disclosure
The article represents original work and has not been published elsewhere. The authors report no conflicts of interest in this work.
References
1. Singh S, Neelakandan K, Sood C, Krishnan J. Disseminated synovial chondromatosis of the knee treated by open radical synovectomy using combined anterior and posterior approaches. J Clin Orthop Trauma. 2014;5(3):157–160. doi:10.1016/j.jcot.2014.07.005
2. Vadi SK, Chouhan DK, Gorla AKR, Shukla J, Sood A, Mittal BR. Potential adjunctive role of radiosynovectomy in primary synovial osteochondromatosis of the knee: a case report. Nucl Med Mol Imaging. 2017;51(3):252–255. doi:10.1007/s13139-016-0466-1
3. Castrogiovanni P, Di Rosa M, Ravalli S, et al. Moderate physical activity as a prevention method for knee osteoarthritis and the role of synoviocytes as biological key. Int J Mol Sci. 2019;20(3):511. doi:10.3390/ijms20030511
4. Temple HT, Gibbons CL. Oxford Textbook of Orthopaedics and Trauma. In: Bulstrode C, Buckwalter J, Carr A, et al, editors. Tumors and tumor-related conditions about the knee. Oxford: Oxford University Press. 2002;2:1153–1154.
5. Maurice H, Crone M, Watt I. Synovial chondromatosis. J Bone Joint Surg Br. 1988;70(5):807–811. doi:10.1302/0301-620X.70B5.3192585
6. Aeffner F, Weeren R, Morrison S, Grundmann I, Weisbrode S. Synovial osteochondromatosis with malignant transformation to chondrosarcoma in a dog. Vet Pathol. 2012;49(6):1036–1039. doi:10.1177/0300985811432347
7. Björnsson J, McLeod RA, Unni KK, Ilstrup DM, Pritchard DJ. Primary chondrosarcoma of long bones and limb girdles. Cancer. 1998;83(10):2105–2119. doi:10.1002/(SICI)1097-0142(19981115)83:10<2105::AID-CNCR9>3.0.CO;2-U
8. Pereira LC, Rwakabayiza S, Lécureux E, Jolles BM. Reliability of the knee smartphone-application goniometer in the acute orthopedic setting. J Knee Surg. 2017;30(03):223–230. doi:10.1055/s-0036-1584184
9. Vijay Shankar MD. Synovial & Tenosynovial Chondromatosis. PathologyOutlines.com; November 13, 2020.
10. Prager RJ, Mall J. Arthrographic diagnosis of synovial chondromatosis. Am J Roentgenol. 1976;127(2):344–346. doi:10.2214/ajr.127.2.344
11. Liu S, Zhou X, Song A, Huo Z, Wang Y, Liu Y. A rare case of giant synovial osteochondromatosis of the thigh: a case report. Medicine. 2019;98(49):e18269. doi:10.1097/MD.0000000000018269
12. Hallam P, Ashwood N, Cobb J, Fazal A, Heatley W. Malignant transformation in synovial chondromatosis of the knee? Knee. 2001;8(3):239–242. doi:10.1016/S0968-0160(01)00084-9
13. Zakir M, Tauqir J, Munawar F, et al. Synovial osteochondromatosis. Prof Med J. 2018;25(09):1442–1446. doi:10.29309/TPMJ/18.5058
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.