")
Back to Journals » Cancer Management and Research » Volume 11
A real-world evidence of efficacy of palliative gastrectomy plus chemotherapy in metastatic gastric cancer patients
Authors Yang LP , Wang ZX, He MM, Wu HX, Yuan SQ , Wang W, Jin Y , Ren C, Wang ZQ, Wang FH, Li YH, Wang F, Xu RH
Received 4 December 2018
Accepted for publication 25 March 2019
Published 2 May 2019 Volume 2019:11 Pages 3993—4003
DOI https://doi.org/10.2147/CMAR.S197052
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Antonella D'Anneo
Lu-Ping Yang,1 Zi-Xian Wang,1 Ming-Ming He,1 Hao-Xiang Wu,1 Shu-Qiang Yuan,2 Wei Wang,2 Ying Jin,1 Chao Ren,1 Zhi-Qiang Wang,1 Feng-Hua Wang,1 Yu-Hong Li,1 Feng Wang,1 Rui-Hua Xu1
1Department of Medical Oncology, Sun Yat-Sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou 510060, People’s Republic of China; 2Department of Gastric and Pancreatic Surgery, Sun Yat-Sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou 510060, People’s Republic of China
Background: The benefit of palliative gastrectomy for patients with metastatic gastric cancer (mGC) is controversial, and suitable candidates for surgery and treatment strategies remain unclear. The present study aimed to investigate the efficacy of palliative gastrectomy plus chemotherapy among patients with mGC and to identify the potential patients for such treatment using real-world data.
Methods: A dataset of 236 patients with mGC diagnosed at the Sun Yat-Sen University Cancer Center from January 1, 2006 to December 31, 2012 were analyzed retrospectively. The cohort comprised 80 patients who had palliative gastrectomy plus chemotherapy (SC) and 156 patients who had chemotherapy only (CO). Propensity score matching (PSM) was employed to minimize the influence of confounders.
Results: The median overall survival of the SC group was significantly better than that of the CO group (Before PSM: 17.0 months vs 12.0 months, P=0.038; after PSM: 17.0 months vs 13.0 months, P=0.017). In the multivariate analysis, SC (Before PSM: hazard ratio (HR) =0.68, P=0.023; after PSM: HR =0.64, P=0.021) was favored for better survival after adjustment for sex, age, year of diagnosis, primary tumor location, and tumor grade. Total gastrectomy (P=0.026) was associated with worse survival for the SC group. The significant survival advantage of SC over CO was retained in patients with single organ metastasis (P=0.016), peritoneal seedings (P=0.039), and those receiving taxane-based chemotherapy (P=0.011).
Conclusion: SC could improve the overall survival of patients with mGC as compared with CO. The chemotherapy regimen and type of resection were proven to influence efficacy. Patients who received taxane-based regimens might be suitable for palliative gastrectomy.
Keywords: first-line chemotherapy, metastatic gastric cancer, palliative gastrectomy, propensity score matching, survival
Introduction
Gastric cancer (GC) is the fifth most common malignancy and the third leading cause of cancer-related death worldwide.1 In China, GC ranks second in tumor incidence and mortality.2–5 In contrast to other East-Asian countries, early detection of GC is infrequent in the Chinese population,6,7 thus over 80% of patients with GC are diagnosed at an advanced stage with poor overall survival (OS).8 Consequently, it is crucial to provide an improved and optimized treatment strategy that can increase the survival of patients with metastatic gastric cancer (mGC).
Current guidelines generally recommend chemotherapy for patients with mGC, and chemotherapy combined with trastuzumab for those whose cancer is human epidermal growth factor receptor 2 (HER-2) positive. Gastrectomy is recommended to alleviate or control tumor-related complications, such as obstruction and bleeding. However, palliative gastrectomy to reduce the tumor burden or potentially prolong survival remains controversial. The phase 3 randomized controlled trial, REGATTA, has failed to demonstrate a survival benefit of gastrectomy followed by chemotherapy using S-1/cisplatin (SP) compared with chemotherapy alone for advanced GC with a single non-curable factor.9 Although this result seems to settle the discussion on palliative gastrectomy, several questions remain. Notably, patients who underwent palliative gastrectomy demonstrated poorer compliance with chemotherapy than those who had chemotherapy alone, and patients with lower third gastric cancer benefitted more from surgery than those with upper third tumors, implying that the timing of surgery and the type of resection provided might considerably influence survival benefit. Moreover, the chemotherapy used in the REGATTA trial was restricted to the combination of oral S-1 80 mg/m2 per day on days 1–21 and cisplatin 60 mg/m2 on day 8 of every 5-week cycle, and whether other regimens combined with surgery could be beneficial remains unclear. By contrast, many retrospective studies have challenged the conclusion of the REGATTA trial and have demonstrated improved survival following non-curative gastrectomy, among which one study even observed an increase in the median OS (mOS) of 9.8 months in patients who only had peritoneal seeding and received preoperative palliative chemotherapy.10–18 As such, it remains undetermined as to whether the survival improvement by palliative gastrectomy is dependent on factors related to the surgical performance or the chemotherapy regimen provided.
Thus, the present study aimed to evaluate the survival benefit of palliative gastrectomy plus chemotherapy compared with chemotherapy alone in patients with mild- or asymptomatic mGC, to investigate the prognostic factors related to clinicopathology and treatment, and to optimize the treatment strategy based on real-world data.
Methods
Ethics statement
All patients provided written informed consent prior to the retrospective data retrieval from medical records. The study was conducted according to the principles expressed in the Declaration of Helsinki.
Patient and data collection
Patients diagnosed with gastric adenocarcinoma with synchronously distant metastasis from January 1st, 2006 to December 31st, 2012 in Sun Yat-Sen University Cancer Center (SYSUCC) were included in the study, and their clinicopathological data and radiographic images were reviewed for selection. Primary gastric tumors were diagnosed by endoscopy or surgical histopathology, and distant metastases were diagnosed by computed tomography or ultrasound imaging (or both), or biopsy histopathology. The palliative gastrectomy should be performed in the first-line treatment; however, the diagnosis-to-surgery interval was not limited for inclusion. The exclusion criteria were as follows: (1) Patients younger than 18 or with an Eastern Cooperative Oncology Group performance status (ECOG PS) ≥2; (2) patients with non-adenocarcinoma histology; (3) patients for whom it was unknown whether gastrectomy had been performed; (4) patients who have had metastasectomy, local ablation, or hyperthermic intraperitoneal chemoperfusion (HIPEC); (5) patients who did not receive palliative chemotherapy; (6) patients who had emergency gastrectomy to treat tumor-related complications; and (7) patients who received radical gastrectomy after successful conversion therapy. The following clinicopathological data were collected: Age; sex; year of diagnosis; primary tumor location; metastatic sites; tumor pathological type and grade; baseline serum carcinoembryonic antigen (CEA); and treatment information, including gastrectomy and its timing, types of resection and results of lymph node examining, first-line chemotherapy regimens, and cycles of usage. Figure 1 shows the process of patient selection. Patients recruited according to the inclusion and exclusion criteria were then sub-grouped as the SC group (patients receiving palliative gastrectomy plus chemotherapy) and the CO group (patients receiving chemotherapy only), based on the treatment received.
 | Figure 1 Flowchart illustrating the case selection process.Abbreviations: GC, gastric cancer; SYSUCC, Sun Yat- Sen University Cancer Center; ECOG PS, Eastern Cooperative Oncology Group performance status; HIPEC, hyperthermic intraperitoneal chemoperfusion. |
Follow-up data were collected from the follow-up records constructed and renewed by the Department of Follow-up of SYSUCC. Patients who were uncontactable or refused to answer inquiries were regarded as censored.
Data processing
CEA was categorized as normal or elevated based on its normal range (0–5.00 ng/mL), as used at our institution. To categorize metastatic lesions, bilateral organ metastases were regarded as one organ involving metastasis; for example, both ovaries with metastases were counted as one organ. Distant (ie, non-regional) metastatic lymph nodes located in multiple regions were also defined as one organ. Chemotherapy regimens were classified into: (1) Fluoropyrimidine (5- fluorouracil, capecitabine, or S-1) plus platinum (cisplatin or oxaliplatin); (2) taxane-based drugs (ie, regimens including paclitaxel and docetaxel); (3) fluoropyrimidine plus irinotecan; (4) fluoropyrimidine monotherapy; and (5) adriamycin-based drugs (ie, regimens including adriamycin and epirubicin). Types of resection were classified as total gastrectomy and partial gastrectomy, and those lacking clear surgical records for the classification, mainly because the surgery was performed in other hospitals, were referred to as “unknown”.
Statistical analysis
Comparisons of patient characteristics between the SC and CO groups were performed using the chi-squared and Fisher’s exact tests for categorical variables. OS was the primary endpoint of this study, which was defined as the time from the date of histological diagnosis of primary cancer to the date of death or last follow-up. The Kaplan–Meier method, with the log-rank test, were used for survival analysis. Multivariate Cox analysis, involving factors with a P-value <0.100 in the univariate Cox regression analysis, was used to identify independent prognostic factors. Additionally, prognostic factors of the patients in the SC group were investigated. To minimize the effects of confounding factors, the propensity score matching (PSM) method was used to match SC and CO patients in a 1:1 ratio based on the patients’ age, sex, year of diagnosis, primary tumor location, numbers of organs involving metastasis, tumor grade, and baseline CEA. The matching process was conducted using the “MatchIt” R package.19 The subsequent survival analyses were based on the matched population. Subgroup analyses to evaluate the survival benefit of palliative gastrectomy were performed in patients with particular metastatic lesions and in those receiving different chemotherapy treatments. We carried out the sensitivity analysis based on patients whose OS exceeded 3 months to eliminate possible bias from a relatively poor prognosis (OS <3 months) caused by vicious tumor biological behavior, not the treatment itself. All data analyses were performed using SPSS Statistics 22.0 (IBM Corp., Version 22.0, Armonk, NY, USA) and the “MatchIt” R packages (The R Foundation, version 3.4.2). A two-sided P-value <0.05 was considered statistically significant.
Results
Patient characteristics
A total of 236 patients were included in the present study. Table 1 summarizes the patient characteristics of the study population. There were 80 patients and 156 patients in the SC and CO groups, respectively. The commonly used first-line chemotherapy regimens were fluoropyrimidine plus platinum and taxane-based regimen for both cohorts; however, only 53.0% (n=125) of the patients received more than four cycles of first-line chemotherapy. Patients in the SC group tended to be diagnosed in the earlier years, to have well or moderately differentiated tumors, to have cancer in the lower two thirds of the stomach, and to have metastatic lesions in only one organ, compared with the patients in the CO group. The chemotherapy regimens and the number of agents applied, the route of administration, and the number of treatment cycles were comparable between groups. After being matched using PSM, no significant differences were detected in all the characteristics analyzed, except the proportions of hepatic metastasis and peritoneal metastasis. This implied that patients with hepatic metastasis tended not to receive palliative gastrectomy while those with peritoneal metastasis did. However, given that metastatic lesions could involve more than one organ, there was no clinical significance in obtaining a balanced distribution of metastatic organs.
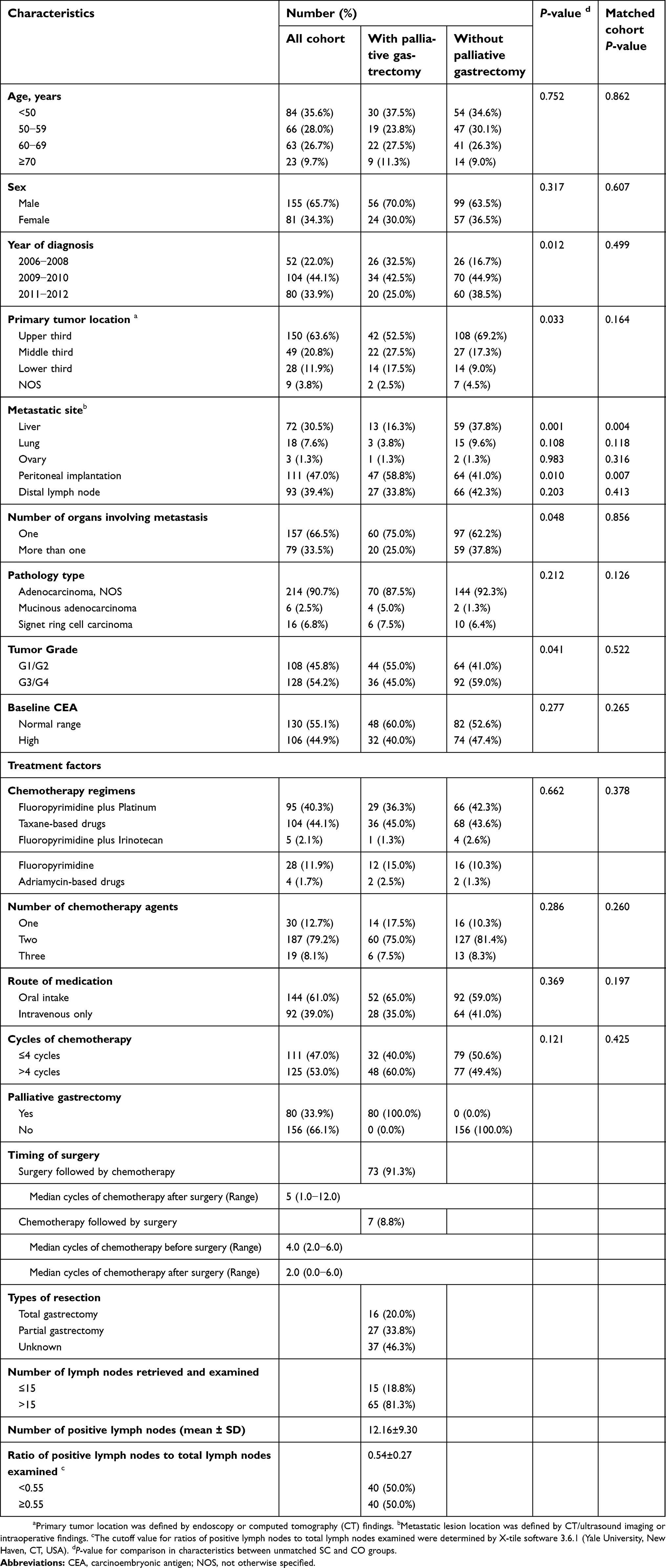 | Table 1 Demographic and clinicopathological characteristics of the unmatched and matched population by propensity score matching (PSM) |
Survival analysis
The mOS of the SC group was significantly longer than that of the CO group (17.0 months vs 12.0 months, P=0.038) (Figure 2A). Palliative gastrectomy also demonstrated significantly prolonged mOS in the matched population (17.0 months vs 13.0 months, P=0.017) (Figure 2B). In the multivariate analysis, after adjustment for sex, age at diagnosis, year of diagnosis, primary tumor location, and tumor grade, palliative gastrectomy (hazard ratio (HR) =0.68 [95% confidence interval (CI): 0.49−0.95], P=0.023; matched HR =0.64 [95% CI: 0.44−0.94], P=0.021) was proved to be associated with better survival.
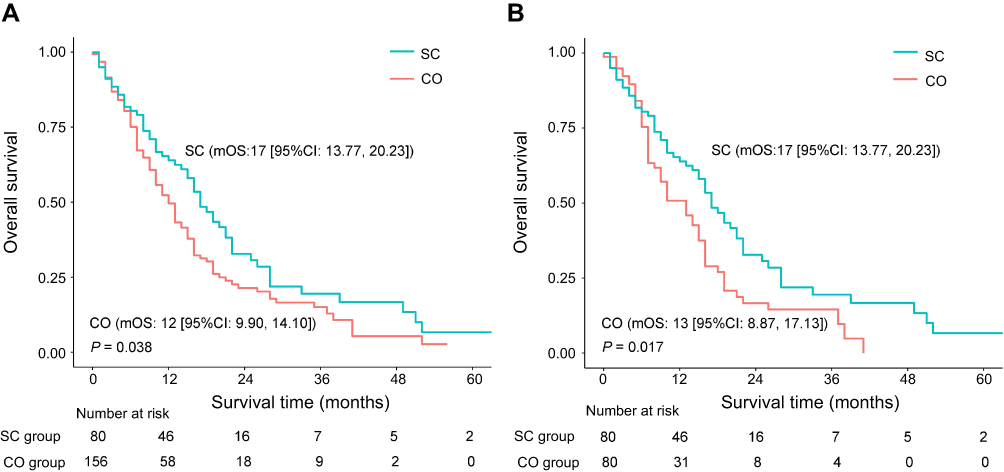 | Figure 2 Kaplan–Meier survival curves of the patients who received palliative gastrectomy plus chemotherapy (SC group) and those who received chemotherapy only (CO group) before (A) and after (B) the propensity score matching. |
Subgroup analysis of patients with different metastatic sites and chemotherapy regimens
Figure 3 demonstrates the survival benefit of SC as compared to CO in particular subgroups of patients. Among the patients whose metastatic lesions were limited to a single organ, palliative gastrectomy was observed to robustly improve their mOS (HR =0.62 [95% CI, 0.42−0.92], P=0.016). In terms of chemotherapy, a prolonged survival advantage was obtained from gastrectomy in patients who received taxane-based chemotherapy (HR =0.52 [95% CI, 0.31−0.86], P=0.011) rather than fluoropyrimidine plus platinum (HR =0.76 [95% CI, 0.43−1.33], P=0.330).
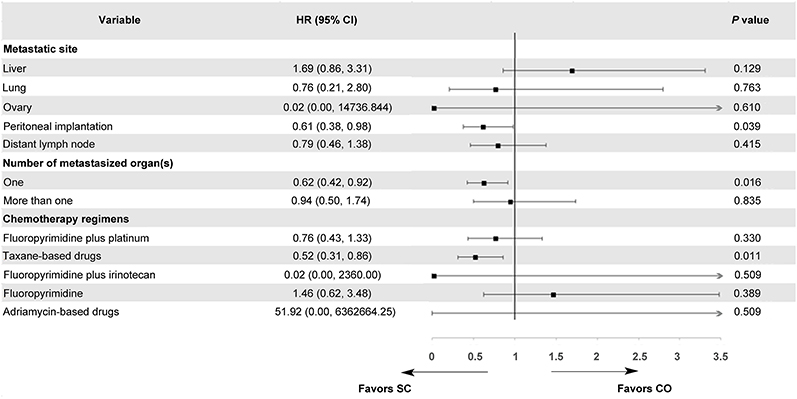 | Figure 3 A forest plot evaluating the survival benefit of palliative gastrectomy plus chemotherapy (SC) versus chemotherapy only (CO) in the subsets of patients with specific metastatic lesions and chemotherapy regimens. |
Surgical factors that favored a prolonged survival among SC patients
The analyses took into consideration variables associated with surgery, including the timing of surgery, the type of resection, the number of lymph nodes examined, and the ratio of positive lymph nodes to total lymph nodes examined, in addition to patient characteristics (Table 2). The type of resection was found to be independently associated with survival (P=0.026). Poorer survival was observed in patients who underwent total gastrectomy compared with patients who underwent other types of gastrectomy. Nevertheless, the timing of surgery (before or after chemotherapy started) and the number of retrieved lymph nodes were found to have no significant influence on survival. Moreover, in the univariate Cox analysis, a high ratio (≥0.55) of positive lymph nodes to total lymph nodes examined was significantly associated with poorer survival (P=0.024), but was not an independent prognostic factor in the multivariate analysis (P=0.076).
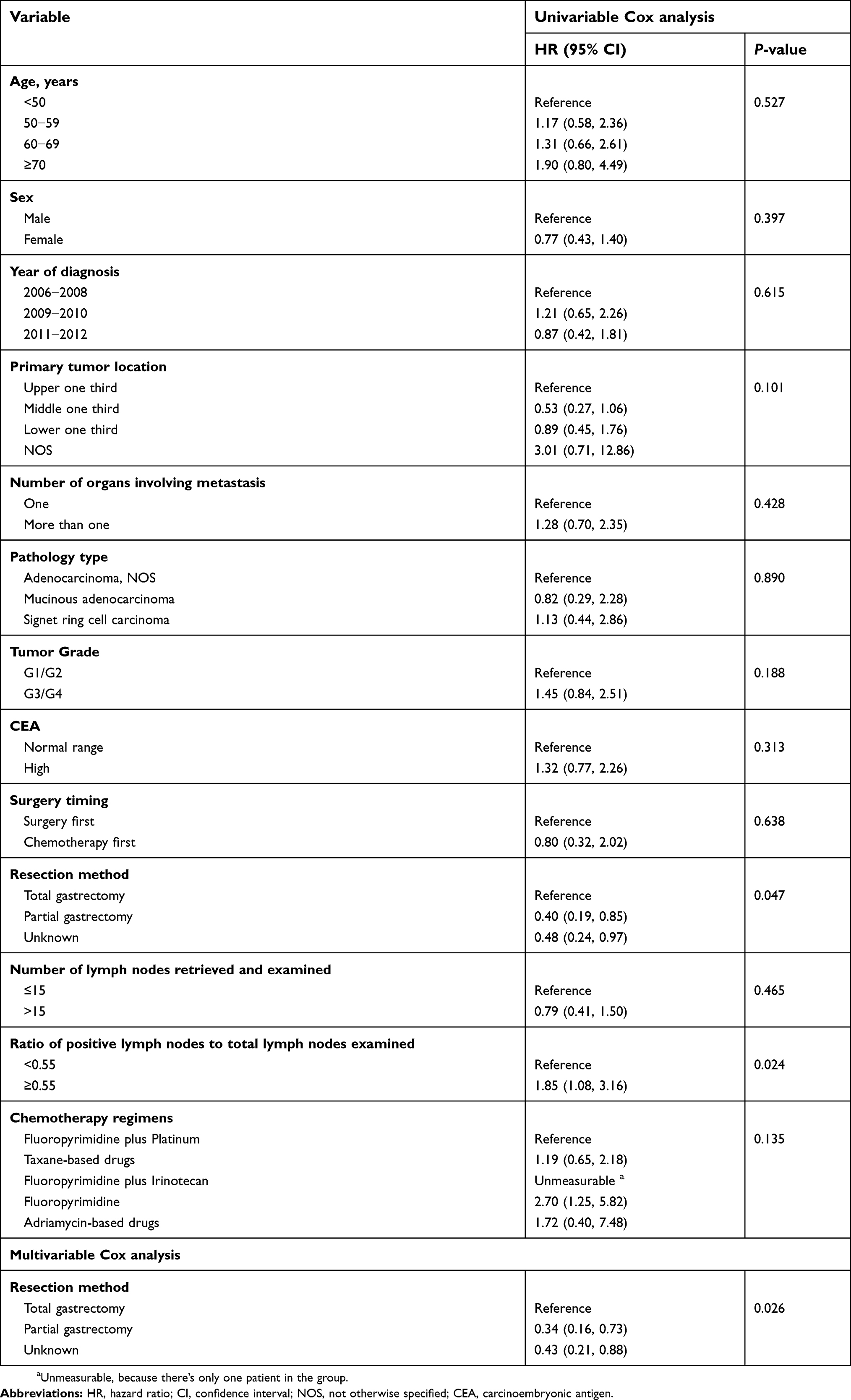 | Table 2 Results of the univariate and multivariate survival analysis by Cox regression of the patients who received gastrectomy plus chemotherapy (SC) |
Sensitivity analysis
After excluding 45 patients with OS ≤3 months, the efficacy of SC was re-evaluated and similar results were obtained. The mOS of the SC group remained significantly longer than that in the CO group (19 months [95% CI, 15.28−22.72] vs 13 months [95% CI, 10.88−15.12], P=0.033). In the multivariate analysis, SC (HR =0.68 [95% CI, 0.47−0.97], P=0.034) remained the superior regimen, demonstrating more favorable survival.
Discussion
In patients with mGC, survival prolongation by palliative gastrectomy is still controversial. In the present study, based on real-world data, we aimed to evaluate the survival benefit of palliative gastrectomy plus chemotherapy compared with chemotherapy alone, to investigate treatment factors that favored better survival, and to develop optimal multi-disciplinary treatment.
The results of the present study were consistent with previous retrospective studies,11,13–17,20,21 in that we demonstrated that patients who received palliative gastrectomy plus chemotherapy had a longer OS as compared with those who received chemotherapy only. A meta-analysis involving 19 non-randomized studies and comprising 2,911 patients observed a possible survival benefit of gastrectomy compared with non-surgical strategies for stage IV GC .17 Other studies analyzed factors that favored the beneficial effects of gastrectomy to narrow down the potential surgical candidates, and to optimize clinical treatment. Hsu et al found that younger age, better preoperative nutritional status, less nodal involvement, and postoperative chemotherapy could independently prolong the survival of patients who received palliative gastrectomy.20 A previous study from our group showed that patients with GC with peritoneal seeding could benefit from palliative chemotherapy followed by gastrectomy. That study also showed that margin-free gastrectomy and more than four cycles of palliative chemotherapy were independent favorable prognostic factors.11 In the present study, SC was found to be associated with better survival, and subgroup analyses for patients with single organ metastasis and patients with peritoneal seedings confirmed the survival improvement resulting from palliative gastrectomy.
To the best of our knowledge, this is the first study to investigate the survival benefit of palliative gastrectomy taking treatment factors (including surgical performance and chemotherapy medication) into consideration. The REGATTA trial strictly limited the chemotherapy medication and dosage, thus its external validation for patients receiving various regimens with different self-suitable dosages should be doubted. For this reason, we used real-world data and further carried out subgroup survival analyses stratified by the chemotherapy regimens. The most commonly accepted first-line chemotherapy regimen as the primary recommendation in China is fluoropyrimidine (5-FU or capecitabine or S-1) plus platinum (cisplatin or oxaliplatin).22–24 Taxane-based regimens are also adopted as first-line chemotherapy; however, a high incidence of intolerance of taxane-based duplexes or triplexes has retarded their clinical application.25–27 In the subgroup analysis, a survival advantage was derived from gastrectomy in patients receiving taxane-based chemotherapy, whereas patients treated with fluoropyrimidine plus platinum might not gain a survival benefit from gastrectomy. The chemotherapy-regimen-dependent feature may be attributed to the negative conclusion of the REGATTA trial which used SP for postoperative chemotherapy. The present study preliminarily indicated that specific chemotherapy regimens, such as taxane-based chemotherapy, were suitable for combination with palliative gastrectomy; however, further corroborative evidence is required.
For the patients in the SC group, how to maximize benefit from surgery was explored and questions from the REGATTA trial about the timing and types of surgery were also investigated. In the present study, patients who underwent partial gastrectomy had better survival compared with those who underwent total gastrectomy, probably because of better organ function-preservation.28 The timing of palliative surgery in relation to chemotherapy was not associated with survival according to our analysis. However, several possible advantages of preoperative chemotherapy were reported in previous studies, including the chance of achieving conversing purpose for curative resection and better treatment compliance compared with postoperative chemotherapy.29 For the extent of lymphadenectomy, the number of lymph nodes retrieved was not a prognostic factor, which suggested that D2 lymphadenectomy might not be meaningful and necessary in the palliative gastrectomy. Moreover, since patients with better survival had an opportunity to receive additional chemotherapy, cycles of chemotherapy were not included in the survival analysis.
This was a retrospective real-world study; therefore, factors influencing medical decisions on SC or CO as first-line treatment were various and hard to completely control. Thus, several measures were taken to reduce bias. Appropriate inclusion and exclusion criteria were set to maximize the comparability between the groups and to enhance the simulation of the real decision-making situation. For instance, patients’ general conditions are usually considered when deciding to perform surgery or not, and in the study, weaker patients with ECOG PS ≥2 were excluded. Moreover, the PSM and multivariate survival analyses were employed simultaneously to minimize the effects of confounding factors.
There are several limitations in the study. First, the second or end-line chemotherapy was not included for analysis, and progression-free survival was not evaluated as an endpoint for first-line treatment. However, the study objective was to investigate the OS benefit of first-line treatment strategy. Second, although other researches have demonstrated the safety of palliative gastrectomy, 15 evaluation of postoperative complications, adverse events caused by chemotherapy, and the quality of life among the patients in the SC group should be performed in our study; the evaluation were limited because of a lack of information. Third, the sample sizes of some subgroups were too small to analyze, and the conclusions drawn from the subgroup analysis need to be validated in future studies with higher evidence levels.
In conclusion, the present study provided real-world evidence that palliative gastrectomy plus chemotherapy could improve survival in patients with mild or asymptomatic mGC compared with chemotherapy alone. Treatment factors, such as chemotherapy regimens and type of resection, might influence the survival benefit of palliative gastrectomy. Patients who received taxane-based regimens might be suitable for palliative gastrectomy.
Availability of data and materials
The key raw data have been deposited into the Research Data Deposit (
Acknowledgments
We are grateful that this study was supported by National Key R&D Program of China (2018YFC1313300), Natural Science Foundation of Guangdong Province (2014A030312015), Science and Technology Program of Guangdong (2015B020232008), Science and Technology Program of Guangzhou (15570006, 201508020250, 201604020003).
Disclosure
Dr Rui-Hua Xu reports grants from National Key R&D Program of China, Natural Science Foundation of Guangdong Province, Science and Technology Program of Guangdong, and Science and Technology Program of Guangzhou, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I,Siegel RL, Torre LA, Jemal A,. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
3. Chen, W., Zheng R., Zeng H., Zhang S. The updated incidences and mortalities of major cancers in China, 2011. Chin J Cancer. 2015;34(11):502–507. doi:10.1186/s40880-015-0042-6
4. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. doi:10.3322/caac.21208
5. Zheng R, Zeng H, Zhang S, Chen W. Estimates of cancer incidence and mortality in China, 2013. Chin J Cancer. 2017;36(1):66. doi:10.1186/s40880-017-0234-3
6. Zong L, Abe M, Seto Y, Ji J. The challenge of screening for early gastric cancer in China. Lancet. 2016;388(10060):2606. doi:10.1016/S0140-6736(16)32226-7
7. Fang C, Wang W, Deng J-Y, et al. Proposal and validation of a modified staging system to improve the prognosis predictive performance of the 8th AJCC/UICC pTNM staging system for gastric adenocarcinoma: a multicenter study with external validation. Cancer Commun (Lond). 2018;38(1):67. doi:10.1186/s40880-018-0337-5
8. Wang W, Sun Z, Deng J-Y, et al. A novel nomogram individually predicting disease-specific survival after D2 gastrectomy for advanced gastric cancer. Cancer Commun (Lond). 2018;38(1):23. doi:10.1186/s40880-018-0293-0
9. Fujitani K, Yang H-K, Mizusawa J, et al. Gastrectomy plus chemotherapy versus chemotherapy alone for advanced gastric cancer with a single non-curable factor (REGATTA): a phase 3, randomised controlled trial. Lancet Oncol. 2016;17(3):309–318. doi:10.1016/S1470-2045(15)00553-7
10. He, M.M., Zhang D.S., Wang F., et al. The role of non-curative surgery in incurable, asymptomatic advanced gastric cancer. PLoS One. 2013;8(12):e83921. doi:10.1371/journal.pone.0059760
11. Yuan SQ, Nie R-C, Chen S, et al. Selective gastric cancer patients with peritoneal seeding benefit from gastrectomy after palliative chemotherapy: a propensity score matching analysis. J Cancer. 2017;8(12):2231–2237. doi:10.7150/jca.18932
12. Hsu JT, Liao J-A, Chuang H-C, et al. Palliative gastrectomy is beneficial in selected cases of metastatic gastric cancer. BMC Palliat Care. 2017;16(1):19. doi:10.1186/s12904-017-0192-1
13. Chang YR, Han DS, Kong S-H, et al. The value of palliative gastrectomy in gastric cancer with distant metastasis. Ann Surg Oncol. 2012;19(4):1231–1239. doi:10.1245/s10434-011-2056-x
14. Chiu CF, Yang H-R, Yang M-D, et al. Palliative gastrectomy prolongs survival of metastatic gastric cancer patients with normal preoperative CEA or CA19-9 values: a retrospective cohort study. Gastroenterol Res Pract. 2016;2016:1–9. doi:10.1155/2016/6846027
15. Dittmar Y, Rauchfuss F, Goetz M, et al. Non-curative gastric resection for patients with stage 4 gastric cancer-a single center experience and current review of literature. Langenbecks Arch Surg. 2012;397(5):745–753. doi:10.1007/s00423-012-0902-3
16. Ebinger SM, Warschkow R, Tarantino I, Schmied BM, Güller U, Schiesser M. Modest overall survival improvements from 1998 to 2009 in metastatic gastric cancer patients: a population-based SEER analysis. Gastric Cancer. 2016;19(3):723–734. doi:10.1007/s10120-015-0541-9
17. Lasithiotakis K, Antoniou SA, Antoniou GA, Kaklamanos I, Zoras O. Gastrectomy for stage IV gastric cancer. a systematic review and meta-analysis. Anticancer Res. 2014;34(5):2079–2085.
18. Schmidt T, Alldinger I, Blank S, et al. Surgery in oesophago-gastric cancer with metastatic disease: treatment, prognosis and preoperative patient selection. Eur J Surg Oncol. 2015;41(10):1340–1347. doi:10.1016/j.ejso.2015.05.005
19. Ho DE, Gary King KI, Stuart EA. MatchIt: nonparametric preprocessing for parametric causal inference. J Stat Softw. 2011;42(8). doi:10.18637/jss.v042.i08
20. Hsu JT, Liao J-A, Chuang H-C, et al. Palliative gastrectomy is beneficial in selected cases of metastatic gastric cancer. BMC Palliat Care. 2017;16:9. doi:10.1186/s12904-017-0192-1
21. Warschkow R, Baechtold M, Leung K, et al. Selective survival advantage associated with primary tumor resection for metastatic gastric cancer in a Western population. Gastric Cancer. 2018;21(2):324–337. doi:10.1007/s10120-017-0742-5
22. Kang YK, Kang W-K, Shin D-B, et al. Capecitabine/cisplatin versus 5-fluorouracil/cisplatin as first-line therapy in patients with advanced gastric cancer: a randomised phase III noninferiority trial. Ann Oncol. 2009;20(4):666–673. doi:10.1093/annonc/mdn717
23. Luo HY, Xu R-H, Wang F, et al. Phase II trial of XELOX as first-line treatment for patients with advanced gastric cancer. Chemotherapy. 2010;56(2):94–100. doi:10.1159/000305256
24. Koizumi W, Narahara H, Hara T, et al. S-1 plus cisplatin versus S-1 alone for first-line treatment of advanced gastric cancer (SPIRITS trial): a phase III trial. Lancet Oncol. 2008;9(3):215–221. doi:10.1016/S1470-2045(08)70035-4
25. Dai X, Zhang X, Wang C, Jiang J, Wu C. Paclitaxel/oxaliplatin/fluorouracil (TOF) regimen versus S-1/oxaliplatin (SOX) regimen for metastatic gastric cancer patients. Oncotarget. 2017;8(18):30495–30501. doi:10.18632/oncotarget.13721
26. Van Cutsem E, Moiseyenko VM, Tjulandin S, et al. Phase III study of docetaxel and cisplatin plus fluorouracil compared with cisplatin and fluorouracil as first-line therapy for advanced gastric cancer: a report of the V325 study group. J Clin Oncol. 2006;24(31):4991–4997. doi:10.1200/JCO.2006.06.8429
27. Wang J, Xu R, Li J, et al. Randomized multicenter phase III study of a modified docetaxel and cisplatin plus fluorouracil regimen compared with cisplatin and fluorouracil as first-line therapy for advanced or locally recurrent gastric cancer. Gastric Cancer. 2016;19(1):234–244. doi:10.1007/s10120-015-0457-4
28. Nomura E, Lee S-W, Tokuhara T, Nitta T, Kawai M, Uchiyama K. Functional outcomes according to the size of the gastric remnant and the type of reconstruction following distal gastrectomy for gastric cancer: an investigation including total gastrectomy. Jpn J Clin Oncol. 2013;43(12):1195–1202. doi:10.1093/jjco/hyt141
29. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11–20. doi:10.1056/NEJMoa055531
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.