")
Back to Journals » International Medical Case Reports Journal » Volume 13
A Rare Case of Simultaneous Intrahepatic and Porcelain Gallbladder: Case Report
Authors Aliniagerdroudbari E, Ershadinia N, Bagherpor G, Babaniamansour S
Received 3 May 2020
Accepted for publication 2 July 2020
Published 15 July 2020 Volume 2020:13 Pages 271—274
DOI https://doi.org/10.2147/IMCRJ.S261103
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Ehsan Aliniagerdroudbari,1 Nazanin Ershadinia,2 Ghasem Bagherpor,3 Sepideh Babaniamansour4
1Department of Surgery, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 2Department of Surgery, Islamic Azad University of Medical Sciences, Sari, Mazandaran, Iran; 3Department of Surgery, Valiasr Hospital of Qaemshahr, Islamic Azad University of Medical Sciences, Sari, Mazandaran, Iran; 4Department of Surgery, Islamic Azad University of Medical Sciences, Tehran, Iran
Correspondence: Sepideh Babaniamansour
School of Medicine, Islamic Azad University of Medical Sciences, Shariati Street, Qolhak, Tehran, Iran
Tel +98 911 216 0329
Email [email protected]
Abstract: Intrahepatic gallbladder is a rare anomaly that is due to the failure of gallbladder migration from liver to its proper position. This condition increases the risk of cholelithiasis, hepatic abscess and cholangiocarcinoma. Calcification in the wall of the gallbladder, which is known as porcelain gallbladder, also increases the risk of malignancy. In this report a 47-year-old man presented at the emergency department with continuous right upper quadrant abdominal pain who was misdiagnosed with acute cholecystitis. During abdominal surgery, gallbladder was not detectable in its proper location. Therefore, the patient underwent enhanced abdominal computed tomography scan and magnetic resonance cholangiopancreatography and the results showed an intrahepatic porcelain gallbladder. In order to avoid future complications, intrahepatic gallbladder should always be considered in patients whose physical examination and radiologic findings do not match.
Keywords: gallbladder, porcelain, intrahepatic, cholecystitis, case report
Introduction
Gallbladder anomalies are very rare with a prevalence of 0.1 to 0.7% worldwide. Intrahepatic gallbladder is a type of anomaly that is due to failure of migration of gallbladder from liver to its proper position during the second month of gestation. In this anomaly, the gallbladder is embedded within the liver parenchyma. The ectopic location disrupts emptying of gallbladder and therefore causes bile stasis which may lead to gallstone formation. It will also put the patient at risk of hepatic abscess and cholangiocarcinoma.1,2
In a study, the prevalence of cholelithiasis among patients with intrahepatic gallbladder was about 60%. Cholelithiasis can increase the incidence of recurrent cholecystitis, partial and complete calcification, and porcelain gallbladder.2,3
The prevalence of porcelain gallbladder in patients with intrahepatic gallbladder is higher than in patients without any anomaly and it increases complications such as malignancy.1 Complications assessment and therapeutic intervention of intrahepatic gallbladder is required due to its high morbidity. Early diagnosis and intervention are critical in gastrointestinal anomalies to prevent serious complications. Choosing the appropriate therapeutic method is a subject of controversy among surgeons. Some studies supported the superiority of surgical procedure in reducing the morbidity and mortality compared with observation. However, some surgeons did not find any significant differences between the two procedures.4–6
In this study we reported a case with a porcelain intrahepatic gallbladder.
Case Presentation
A 47-year-old man reported to the emergency department (ED) with the complaint of continuous abdominal pain in right upper quadrant (RUQ) radiated to right shoulder. The onset of pain was 24 hours prior to arrival at the ED. He had a history of 10 pack/year smoking but had no history of alcohol consumption. He also reported two episodes of similar abdominal pain in RUQ with a continuous pattern in the past year. He underwent supportive treatment with a sonography report of chronic cholecystitis. His past medical and drug history were unremarkable. In review of systems, there was no further complaint except abdominal pain. On initial evaluation he was afebrile (axillary temperature of 37.1°C) with blood pressure of 120/85 mmHg, pulse rate of 85 per minute, and respiratory rate of 10 per minute. There was no evidence of icterus. In abdominal examination, on light palpation there was moderate tenderness in RUQ and epigastric region. Murphy’s sign was negative. There was no evidence of organomegaly and no palpable mass was detected. Laboratory results showed white blood cell count of 5600/µL with 60% polymorphonuclear, amylase level of 63 U/L (normal range of below 100 U/L) and normal liver and renal function tests. The patient underwent ultrasonography with primary diagnosis of biliary colic. Sonographic findings included gallbladder with thick edematous wall, free fluid around and a number of stones inside and also bile ducts with normal diameter. According to these findings the patient was transferred to the operating room for laparoscopic cholecystectomy after hydration and initiation of intravenous antibiotic. Due to the inability to detect the gallbladder during laparoscopy, laparotomy with Kocher incision was done. The gallbladder was not detectable even after laparotomy and a mass was seen and palpated in right lobe of liver. The laparotomy was ended after lavage of abdominal cavity and placing a surgical drain without any further action. Afterward a gastroenterology consult was requested and the patient underwent enhanced abdominal computed tomography (CT) scan and magnetic resonance cholangiopancreatography (MRCP). The CT scan showed a hypodense structure in right lobe of liver with calcified wall which was filled with air, fluid and multiple stones. The report suggested diagnosis of intrahepatic porcelain gallbladder [Figure 1].
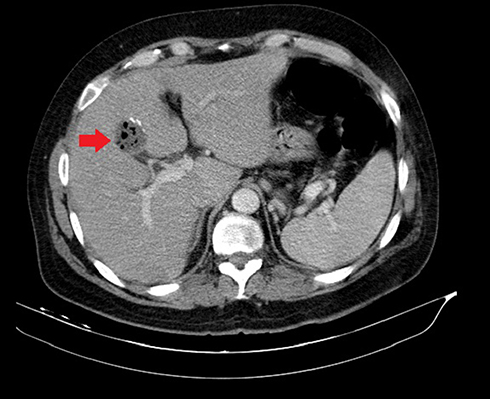 |
Figure 1 Enhanced abdominal CT scan showing intrahepatic gallbladder with calcifications and filled with several stones. (1.4x magnification). |
MRCP also reported a mild dilated common bile duct and central intrahepatic bile ducts [Figure 2]. After necessary investigations, due to presence of simultaneous intrahepatic and porcelain gallbladder, the surgeon decided to perform both cholecystectomy and hepatotomy to ensure the absence of malignancy. The patient was referred to a better-equipped center to undergo the surgery.
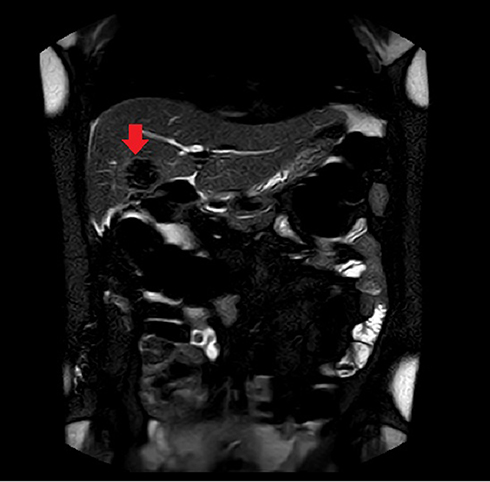 |
Figure 2 MRCP showing intrahepatic gallbladder with calcification and mild dilated intrahepatic bile ducts. (1x magnification). |
Discussion
One of the most important problems associated with intrahepatic gallbladder is the misdiagnosis with other diseases with similar radiographic manifestations.7 The type of surgical procedure in this congenital variant has always been controversial due to misplacement of intrahepatic gallbladder from its normal anatomical location. Type of treatment in intrahepatic gallbladder varies from transhepatic drainage to hepatectomy and is influenced by two important factors including location and type of clinical symptoms. High incidence of cholelithiasis in intrahepatic gallbladder can increase the probability of symptomatic cases and can lead to diagnostic errors in the imaging process. In this regard, Popli et al suggested prophylactic cholecystectomy in both symptomatic and asymptomatic patients with intrahepatic gallbladder.4
But in other studies, therapeutic approach was used only in patients with symptoms or clinical complications. In a study conducted by Schmahmann et al, simple gallbladder drainage with choledocholithotomy proved effective in a patient with intrahepatic gallbladder and acute cholecystitis.8
Furthermore, in a case of intrahepatic gallbladder in ectopic liver in pelvic, hepatotomy and cholecystectomy was done for the patient with acute cholecystitis diagnosis.2
Open cholecystectomy accompanied by hepatectomy is either due to occurrence of cholecystectomy’s side effects such as gallbladder perforation or due to inability of differentiating intrahepatic gallbladder with other hepatic lesions such as malignancies or Caroli disease.9,10
Porcelain gallbladder which is defined as calcification in gallbladder can increase the probability of cancer through cell changes caused by chronic cholecystitis. Therefore, surgical intervention is mostly recommended.11
Previously all patients with porcelain gallbladder underwent cholecystectomy. However, many surgeons do not agree with prophylactic cholecystectomy of porcelain gallbladder in asymptomatic patients. The decision to perform prophylactic surgery of porcelain gallbladder differs in each patient and depends on factors such as patient’s age, underlying diseases, pattern of calcification.12–14
Surgical approach to porcelain gallbladder has significantly changed in recent years. Previously, porcelain gallbladder was assumed unremovable by laparoscopy due to its brittle wall. But nowadays, reports suggest that laparoscopic cholecystectomy is possible, especially in the presence of noncalcified and unobstructed cystic duct. Cystic duct can be assessed by cholangiography during operation or by ultrasonography before operation.13,15
Porcelain intrahepatic gallbladder presented in this report is a rare case of gallbladder anomaly and should always be considered in patients whose physical examination and radiologic findings do not match in order to avoid future complications.
Ethical Approval
All procedures of the studies were in accordance with the ethical standards of the institutional Committee of Islamic Azad University of Sari Medical Branch, Iran. Regarding the policies of the University, institutional approval was not required to publish case report and also case series involving fewer than three patients.
Consent of Patient
Informed consent was obtained from the patient for publication of this case report and accompanying images.
Disclosure
The authors declare that they have no financial or nonfinancial competing interests.
References
1. Thakrar R, Monib S, Pakdemirli E, Thomson S. Calcified gallbladder cancer: is it preventable? J Surg Case Rep. 2019;2019(3):rjz069. doi:10.1093/jscr/rjz069
2. Mathis R, Stodghill J, Shaver T, Younan G. Cholecystectomy of an intrahepatic gallbladder in an ectopic pelvic liver: a case report and review of the literature. Case Rep Surg. 2017;2017:3568768. doi:10.1155/2017/3568768
3. Iqbal S, Ahmad S, Saeed U, Al-Dabbagh M. Porcelain gallbladder: often an overlooked entity. Surg J. 2017;3(4):e145–e147.
4. Popli MB, Popli V, Solanki Y. Ectopic gall bladder: a rare case. Saudi J Gastroenterol. 2010;16(1):50. doi:10.4103/1319-3767.58771
5. DesJardins H, Duy L, Scheirey C, Schnelldorfer T. Porcelain gallbladder: is observation a safe option in select populations? J Am Coll Surg. 2018;226(6):1064–1069. doi:10.1016/j.jamcollsurg.2017.11.026
6. Babaniamansour S, Aliniagerdroudbari E, Bagherpour G, Kheiry F. Simultaneous volvulus of transverse colon and cecum in a patient with down syndrome: a case report. Case Rep Clin Pract. 2019;4(2):52–56.
7. Rafailidis V, Varelas S, Kotsidis N, Rafailidis D. Two congenital anomalies in one: an ectopic gallbladder with phrygian cap deformity. Case Rep Radiol. 2014;2014:246476. doi:10.1155/2014/246476
8. Schmahmann JD, Dent DM, Mervis B, Kottler RE. Cholecystitis in an intrahepatic gallbladder. A case report. S Afr Med J. 1982;62(27):1042–1043.
9. Guiteau JJ, Fisher M, Cotton RT, Goss JA. Intrahepatic gallbladder. J Am Coll Surg. 2009;209(5):672. doi:10.1016/j.jamcollsurg.2009.03.027
10. Donati M, Biondi A, Basile F, Gruttadauria S. An atypical presentation of intrahepatic perforated cholecystitis: a modern indication to open cholecystectomy. Report of a case. BMC Surg. 2014;14(1):6. doi:10.1186/1471-2482-14-6
11. Sheth S, Bedford A, Chopra S. Primary gallbladder cancer: recognition of risk factors and the role of prophylactic cholecystectomy. Am J Gastroenterol. 2000;95(6):1402–1410. doi:10.1111/j.1572-0241.2000.02070.x
12. Stephen AE, Berger DL. Carcinoma in the porcelain gallbladder: a relationship revisited. Surgery. 2001;129(6):699–703. doi:10.1067/msy.2001.113888
13. Khan ZS, Livingston EH, Huerta S. Reassessing the need for prophylactic surgery in patients with porcelain gallbladder: case series and systematic review of the literature. Arch Surg. 2011;146(10):1143–1147. doi:10.1001/archsurg.2011.257
14. Smith PW, Farrar RA, Evangelista RS. Intrahepatic porcelain gallbladder: coexistence of pathologies. Am Surg. 2012;78(9):E414–E415. doi:10.1177/000313481207800913
15. Kwon AH, Inui H, Matsui Y, Uchida Y, Hukui J, Kamiyama Y. Laparoscopic cholecystectomy in patients with porcelain gallbladder based on the preoperative ultrasound findings. Hepato Gastroenterol. 2004;51(58):950–953.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.