")
Back to Journals » Clinical Ophthalmology » Volume 13
A rapid technique for en masse soft cataract phacoemulsification
Authors Om Parkash R, Mahajan S, Om Parkash T, Vajpayee RB , Om Parkash T
Received 7 December 2018
Accepted for publication 5 March 2019
Published 26 April 2019 Volume 2019:13 Pages 755—762
DOI https://doi.org/10.2147/OPTH.S197359
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video S1: This video demonstrates the RAPID technique in a stepwise manner. The nucleus is rotated (R) freely in the capsular bag from the side port incision by a second instrument. The phaco probe tip is partly aligned (A) sideways towards
Views: 17481
Rohit Om Parkash,1 Shruti Mahajan,1 Tushya Om Parkash,1 Rasik B Vajpayee,2 Tushar Om Parkash3
1Ophthalmology, Department of Cataract and Refractive Surgery, Dr Om Parkash Eye Institute, Amritsar, Punjab, India; 2Ophthalmology, FRCS, FRANZCO, Vision Eye Institute, Royal Victorian Eye and Ear Hospital, University of Melbourne, Melbourne, VIC, Australia; 3Department of Ophthalmology, Vydehi Institute of Medical Sciences and Research, Bangalore, Karnataka, India
Purpose: To describe a new, en masse, stepwise technique for purely soft cataracts.
Methods: RAPID, a soft cataract phacoemulsification technique, is an acronym-based procedure where R is rotation of nucleus, A is alignment of phacoemulsification tip sideways, P is placement of tip adjacent to the nuclear rim, I is impaling of tip into nuclear rim and D is devouring wherein nucleus is aspirated/emulsified. RAPID technique was performed in 54 eyes of 54 patients (31 males and 23 females; mean age 46.35±3.95 years). The soft nucleus was emulsified, after performing hydrodissection, in a stepwise manner in the safe zone away from posterior capsule and corneal endothelium. Centurion/Infiniti Phacoemulsification system (Alcon Laboratories, Inc.) was used with vacuum parameters at 475 mm Hg and an aspiration flow rate of 0–45 mL/min in linear mode. The primary outcome measures were cumulative dissipated energy (CDE), ultrasound time (UST), amount of fluid used, surgical complications and mean endothelial cell loss.
Results: Phacoemulsification with IOL implantation was performed successfully in all patients without any intraoperative complications. CDE was 1.03±0.61. Total UST for nuclear emulsification was 3.84±3.27 seconds and fluid used was 10±2.35 milliliters. Postoperative follow-up examinations were done on 1, 4, 14, 30 and 90 days. Mean percentage of endothelial cell loss was 7.05±2.65% (mean endothelial cell counts were 2383.75±105.21 cells/mm2 preoperatively and 2215.78±114.9 cells/mm2 3 months postoperatively).
Conclusion: RAPID is an en masse non-fragmentation technique for purely soft cataracts. This technique requires neither any specialized instrumentations nor the use of high vacuum with complimenting surge preventing software. Simple stepwise multi-planer approach of RAPID technique allows easy and fast emulsification of soft cataracts with simultaneous safeguarding of posterior capsule and corneal endothelium.
Keywords: soft cataract phacoemulsification, RAPID en masse phacoemulsification technique, soft cataract
Introduction
Purely soft cataracts are characterized by spongy consistency.1 They are seen in patients with posterior subcapsular cataracts, developmental cataracts and in individuals opting for refractive lens exchange.2–4 Such soft cataracts are found in young and middle-aged patients.5 However, these soft-looking cataracts become relatively hard and large as the age increases.6
The number of patients undergoing soft cataract phacoemulsification at an early stage has increased.5 This increasing trend is attributed to growing visual demands, increased cosmetic needs, onset of cataract in younger age group and availability of ambulatory surgical technique.3–7 Furthermore, the surgeons’ confidence has grown manifold in recommending surgery in early cataracts because of improvement in techniques and instrumentations, advancements in phacoemulsification technologies and availability of premium intraocular lenses (IOLs).7
Commonly used fragmentation techniques of phacoemulsification for soft cataracts are challenging.8–10 The fragmentation techniques due to their limitations cannot be used in very soft cataracts.11
Non-fragmentation techniques are preferred for soft cataracts due to the challenges in fragmentation techniques.12 The plethora of non-fragmentation techniques described to emulsify soft cataracts require special maneuvers, customized instrumentation, high fluidics and surge preventing software.9,13–19 These factors limit the use of the existing non-fragmentation techniques for exclusively soft cataracts.
We describe RAPID technique for a simplified en masse nuclear emulsification of purely soft cataracts.
Material and methods
This was a single centered observational study conducted in a private setting hospital from March 2018 to September 2018. The protocol adhered to the tenets of the Declaration of Helsinki and received approval from the ethics committee of Dr Om Parkash Eye Hospital. All the patients provided a written informed consent for the surgery and for inclusion in this study.
RAPID technique was performed in 54 patients having soft cataract. There were 31 males and 23 females with a mean age of 46.35±3.95 years. The patients presenting with posterior sub capsular cataracts, developmental cataracts and those opting for refractive lens exchange were included in the study. Based on Lens Opacity Classification (LOCS) III grading of cataract, the patients included in the study presented with nuclear colour grade 1 (NC1), nuclear opalescence grade 1 (NO1), cortical cataract grade 1 (C1) and posterior subcapsular cataract grade 1 (P1 to P4). Patients with nuclear nuclear colour >NC1 and nuclear opalescence grade more than NO1 were excluded from the study. It was further observed that the overly soft looking nuclei in the higher age group were relatively hard and large and could not be maneuvered like purely soft cataracts.6 Hence, patients above 50 years of age were also excluded from the study.
Technique
All surgeries were performed under topical anesthesia with 0.5% proparacaine (Sunways India) eyedrops. The surgery was performed using Centurion/Infiniti Phacoemulsification system (Alcon Laboratories, Inc., Fort Worth, TX, USA). The parameters used were 475 mm Hg vacuum and 0–45 mL/min aspiration flow rate in linear mode with torsional phacoemulsification. There were 14 surgeries in our study that were performed by 2 trainee surgeons to determine the ease of learning. Rest of the surgeries were performed by the training surgeon. A temporal, clear corneal 2.2 mm or 2.8 mm incision was made. After completing a routine capsulorhexis of 5 mm, hydrodissection was performed. Hydrodelineation was not done. The steps of RAPID technique were as follows (Figures 1–5, Video 1).
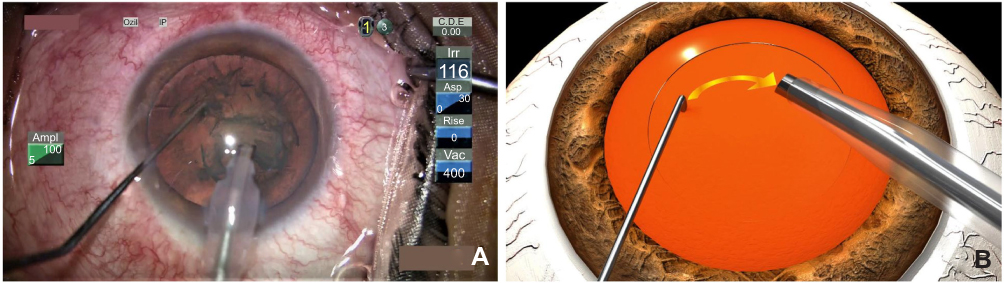 | Figure 1 (A) Surgical video still showing R: rotation of the nucleus with the second instrument. (B) Animation showing R: rotation of the nucleus with the second instrument. |
 | Figure 5 (A) Surgical video still showing D: devouring of the nucleus. (B) Animation showing D: devouring of the nucleus. |
R – Rotation of the nucleus. (Figure 1A and B): This was a crucial step of the RAPID technique. The rotation in soft cataracts is usually difficult due to strong cortico-nuclear adhesions. Multiple point hydrodissection was attempted to completely separate the epinuclear-nuclear mass from the cortex. The nucleus was rotated freely in the capsular bag with the second-hand instrument from the side port incision. The preferred second-hand instrument was a blunt tip chopper/sinskey hook. Free rotation of the nucleus allowed complete cortico-nuclear separation. While rotating, care was taken to avoid cheese wiring through the viscoid nucleus. The second instrument was placed superficially just inside the capsulorhexis margin to provide torque for nuclear rotation. In cases where the rotation was difficult, rotation was attempted in clockwise and anti-clockwise directions.
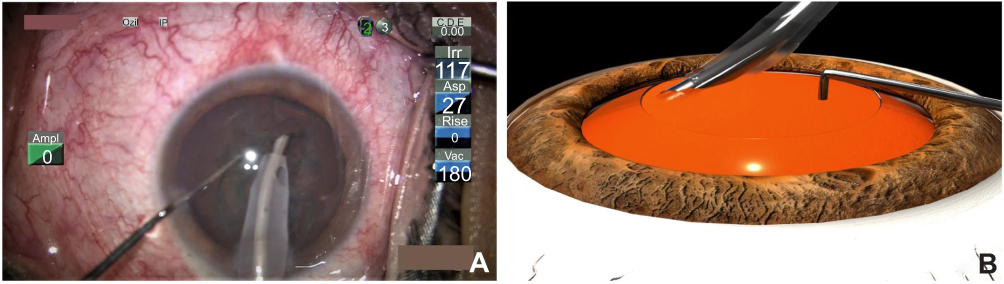
A – Alignment of the phacoemulsification tip (Figure 2A and B): The phacoemulsification probe with 45 degrees Kelman tip was introduced into the anterior chamber. The tip was aligned sideways towards the direction of the side port to allow coordinated rotation and feeding of the nucleus by the second instrument into the phacoemulsification tip.
 | Figure 2 (A) Surgical video still showing A: Alignment of the phaco-tip sideways. (B) Animation showing A: Alignment of the phaco-tip sideways. |
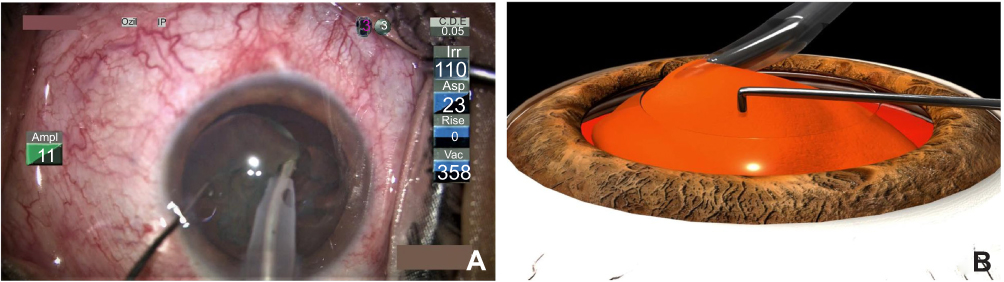
P – Placement of the tip at the nuclear rim (Figure 3A and B).
 | Figure 3 (A) Surgical video still showing P: placement of the phaco-tip at the nuclear rim. (B) Animation showing P: placement of the phaco-tip at the nuclear rim. |
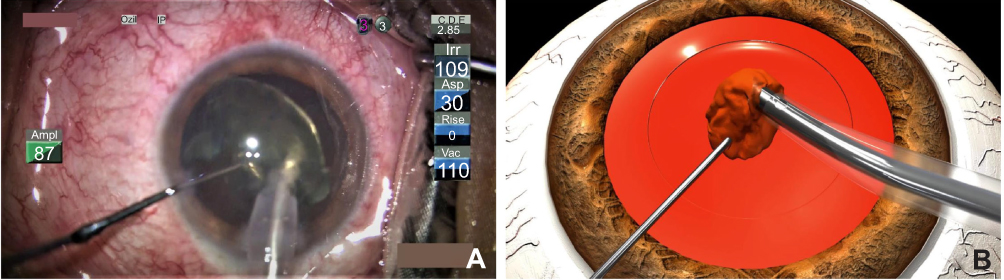
I – Impaling of the phacoemulsification probe into the nuclear rim (Figure 4A and B): The phacoemulsification probe was impaled into the substance of the nucleus adjacent to the rim. A sustained occlusion was achieved by impaling the nucleus with the phacoemulsification tip sideways. Impaling was done exclusively in aspiration mode by vacuum. At times, phacoemulsification power was needed for milliseconds to embed into the nucleus. In the event of occlusion break, the nuclear rim was re-impaled at the site next to the aspirated nucleus.
 | Figure 4 (A) Surgical video still showing I: impaling of the nuclear rim. (B) Animation showing I: impaling of the nuclear rim. |
D – Devouring or aspiration/emulsification of the nucleus (Figure 5A and B): The soft nucleus was initially impaled onto the phacoemulsification tip which caused simultaneous aspiration and rotation of the nucleus. At the same time, the phacoemulsification probe tip was moved centrally into the safe zone. The controlled aspiration/emulsification of the impaled nuclear mass was continued and the nucleus was moved, in a circular manner, out of the bag away from the posterior capsule into the plane of anterior capsule or iris. At that stage, the actively coordinated manipulation of the chopper fed the residual nucleus to the probe in a clockwise manner with or without flipping it. Phacoemulsification or aspiration in very soft cataracts was performed maintaining the safe zone criteria. Routine phacoemulsification parameters were employed. No special instruments or surge prevention softwares were used in our technique.
Results
In all cases, the overly soft cataract was emulsified safely. The cumulative dissipated energy (CDE) was 1.03±0.61. The total ultrasound time (UST) for nucleus emulsification was 3.84±3.27 seconds (sec). The estimated fluid used was 10±2.35 milliliters (mL) (Table 1). No intra-operative complications were encountered in our surgeries. Phacoemulsification surgery with IOL implantation was performed successfully in all patients.
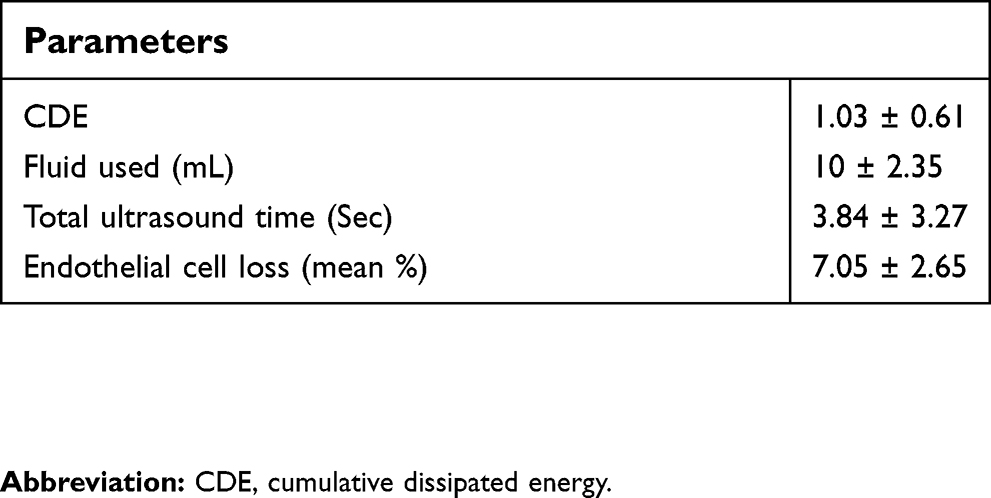 | Table 1 RAPID technique – surgical parameters used |
In the 14 surgeries performed by trainee surgeons, an occlusion break was observed in 3 cases at the time of impaling the nuclear rim. However, the procedure was completed successfully by impaling at the adjacent part of the rim. Thus, the technique has a short learning curve for novice surgeons. The trainee surgeons did not encounter any difficulty or complication while carrying out the procedures.
Our technique did not entail the use of high fluidics. The use of moderate 400 mm Hg vacuum in linear setting minimized the chances of iatrogenic trauma to the posterior capsule. There was no posterior capsule rupture observed in any case. The mean percentage of endothelial cell loss was 7.05±2.65% (Table 1) (mean endothelial cell counts were 2383.75±105.21 cells/mm2 preoperatively and 2215.78±114.9 cells/mm2 after 3 months postoperatively). The immediate postoperative evaluation was unremarkable.
Discussion
Overly soft cataracts cannot be split.20 The routine fragmentation techniques such as divide and conquer, stop and chop and direct chop have their limitations in soft cataract phacoemulsification. It is difficult to hold and divide the overly soft nucleus. The optimal vacuum needed to hold the nucleus is very often associated with breaking of occlusion and aspiration of the nucleus. The multiple efforts to fragment the nucleus by chopping or dividing cause cheese wiring through the nucleus. This often leads to an undivided bowl of nucleus which makes safe emulsification challenging.8–11
Hydro-chop, visco-fracture and V-slice techniques are the fragmentation techniques exclusively used for overly soft cataracts. These techniques have limited use because of the failure to achieve complete division of the nucleus.21–23
The inherent inability to divide the viscous material makes non-fragmentation techniques the preferred techniques in very soft cataracts. The non-fragmentation techniques work on the principle that the soft nuclei that cannot be split should be bent, flexed or maneuvered to achieve phacoemulsification.20 Zeng et al., in their study on comparison of non-chopping rotation technique with axial rotation quick chop phacoemulsification technique, concluded that non-chopping techniques were more successful for soft to medium hard cataracts.12
We propose RAPID, the non-fragmentation emulsification technique of soft cataracts. The easy to perform technique has a short learning curve, a fair degree of reproducibility, a high safety profile, and can be performed by surgeons of all levels of expertise. In our technique, a routine 5 mm capsulorhexis is adequate. The standard sized capsulorhexis allows capsulotomy edges to cover IOL optic all around (Table 2).
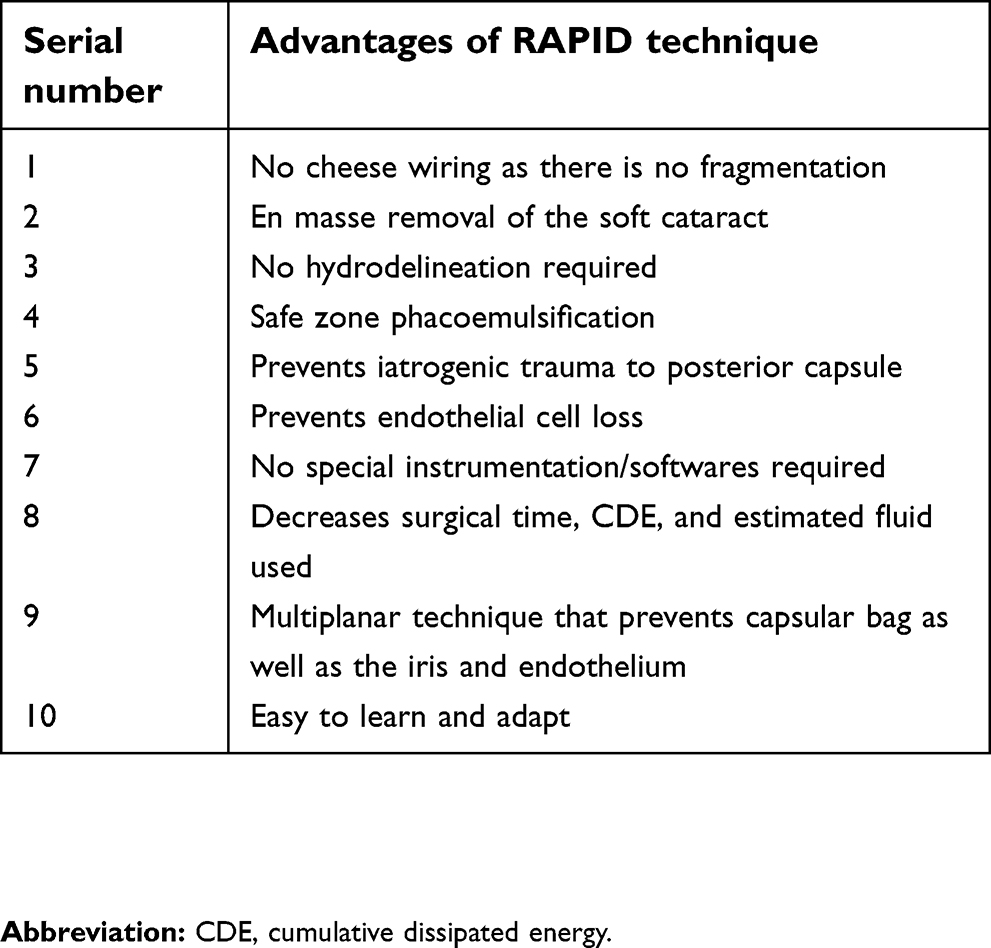 | Table 2 Advantages of RAPID technique |
Our RAPID technique involves en masse emulsification of the nucleus. Hydrodelineation is not required since the epinuclear-nuclear mass is emulsified as a whole. The emulsification begins in the capsular bag itself. In our technique, as the soft nucleus gets aspirated/emulsified and debulked, it is gradually moved in a circular manner away from the posterior capsule and out of the bag into the plane of the anterior capsule and iris. The coordinated maneuvering of the nucleus makes our technique a multi-planer technique (Table 2).
The use of normal fluidics and the coordinated movement between the second instrument and the phacoemulsification tip to move the nucleus away from the posterior capsule eliminate the possibility of posterior capsule rupture. Besides, there is neither sculpting of the overly soft nucleus nor anterior tumbling of the nucleus which further reduces the risk of posterior capsular rent (Table 2).
There is minimal damage to the corneal endothelium in our technique because of lower use of CDE, lesser utilization of UST and lack of proximity of the partially emulsified soft nucleus with the corneal endothelium. The en masse emulsification of the nucleus does not require any special phacoemulsification tip, settings or instruments thus making our technique simple and safe (Table 2).
Our technique, contrary to the traditional carouselling or the supra capsular techniques, does not entail hydro prolapsing or maneuvering of nucleus out of the capsular bag.13,24 Phacoemulsification in the anterior chamber can cause collateral damage to the corneal endothelium or to the iris.25
Our technique is simple. There is no requirement of specialized 20 degrees phacoemulsification tip (right bent D-shaped with a semicircular opening) and a third irrigation port as in the endocapsular carouselling technique described by Jardine et al.13 (Table 3). The RAPID technique involves usage of normal fluidics in overly soft cataracts as against the high fluidics in the endo-capsular technique. Lower fluidics are preferred in soft cataracts to prevent post-occlusion surge and potential damage to the posterior capsule.26
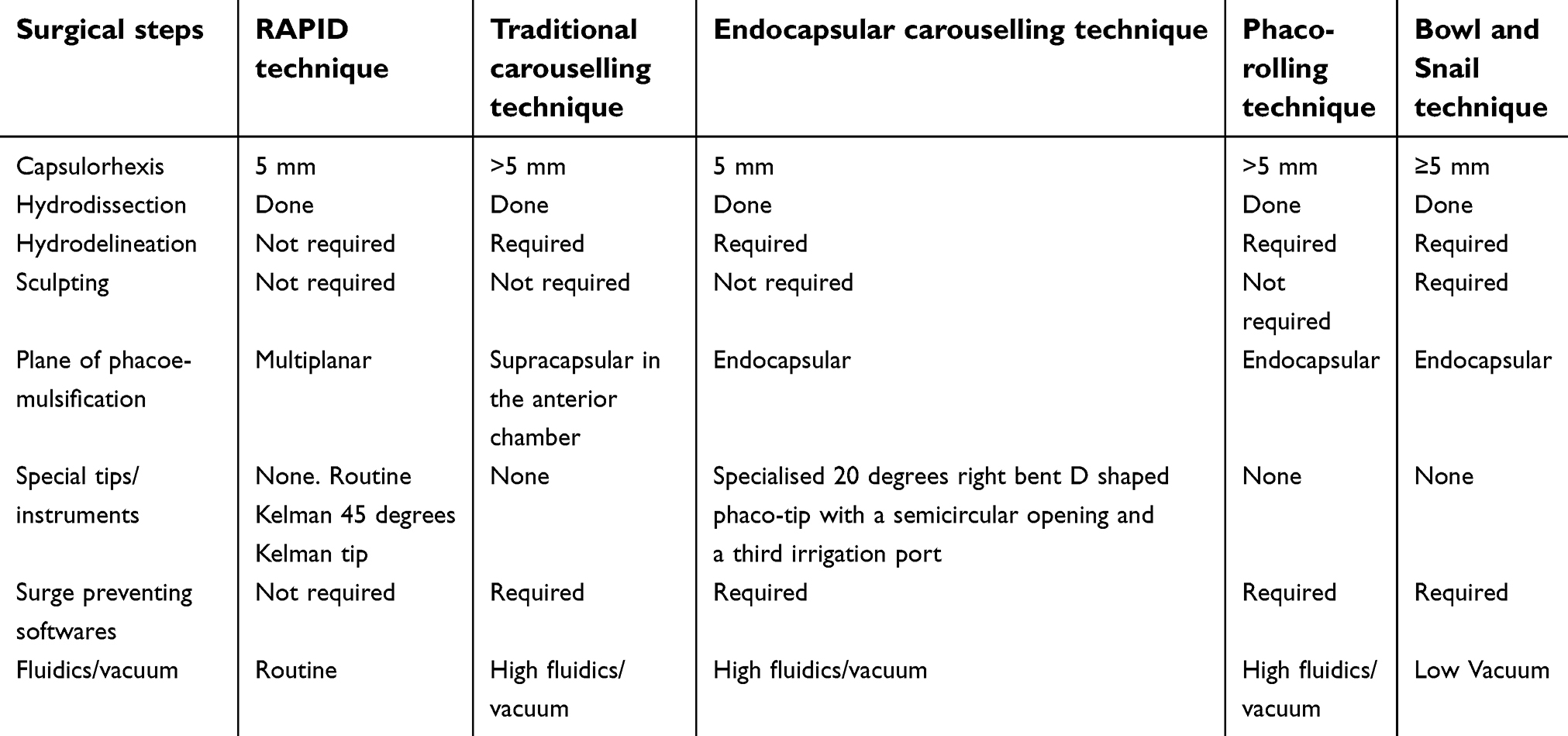 | Table 3 Comparaison of non-fragmentation techniques and RAPID technique |
Güell et al. described a variant of carouselling technique in phaco-rolling technique for soft to medium-hard cataracts14 (Table 3). The high vacuum used during soft nuclear emulsification in the bag increases the tendency to posterior capsular rent during the phase of occlusion break. The large capsulorhexis used in Guell’s technique negates the long-term advantages of optimal sized capsulorhexis.27
Gomaa et al. introduced the bowl and snail technique11 (Table 3). In Gomaa’s technique, sculpting a deep central bowl in a discoid soft nucleus can be dangerous. The emulsification of C-shaped nuclear rim with rotation can jeopardize the integrity of posterior capsule.24
Our RAPID technique provides a perfect blend of above-described maneuvers which increases the safety profile and circumvents the predisposition to complications. However, a prospective comparative study with other phacoemulsification techniques for soft cataracts is necessary.
The RAPID technique has a few limitations (Table 4). Firstly, our technique requires an adequate 5 mm capsulorhexis. It is difficult to perform the RAPID technique in a small-sized rhexis because of difficult maneuvering of the large-sized nuclear epinuclear mass. Secondly, it is difficult to perform RAPID technique in older age group because the soft looking nucleus is relatively large and hard.6 Our RAPID technique requires a highly flexible soft nucleus for maneuvering which becomes difficult when the nucleus is not overly soft.
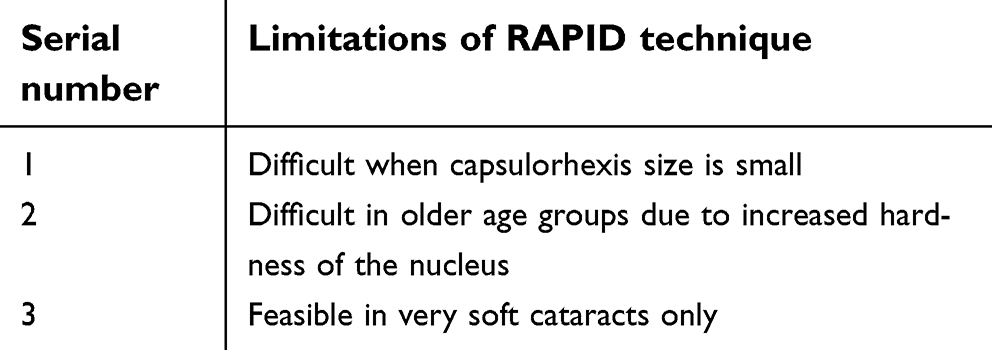 | Table 4 Limitations of RAPID technique |
Conclusion
It is known that overly soft cataracts are frequently associated with difficult nucleus emulsification. There are special fragmentation techniques which do not work well in the very soft cataracts because of the inability to achieve complete division. Non-fragmentation techniques are the preferred techniques for the overly soft cataracts. RAPID is the non-fragmentation technique for overly soft cataracts wherein complete nuclear division is not possible. The step-by-step en masse RAPID technique is an easy to learn and perform technique because it requires neither any specialized instrumentations nor the use of high vacuum with complimenting surge preventing software. This smart multi-planer technique systematically performed in the safe zone away from posterior capsule and corneal endothelium allows safe phacoemulsification of soft nucleus.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wallace RB
2. Scheie HG. Aspiration of congenital or soft cataracts: a new technique. Am J Ophthalmol. 1960;50:1048–1056.
3. Alio JL, Grzybowski A, El Aswad A, Romaniuk D. Refractive lens exchange. Surv Ophthalmol. 2014;59(6):579–598. doi:10.1016/j.survophthal.2014.04.004
4. Brown RH, Zhong L, Lynch MG. Clear lens extraction as treatment for uncontrolled primary angle-closure glaucoma. J Cataract Refract Surg. 2014;40:840–841. doi:10.1016/j.jcrs.2014.03.002
5. Gollogly HE, Hodge DO, St Sauver JL, Erie JC. Increasing incidence of cataract surgery: population-based study. J Cataract Refract Surg. 2013;39(9):1383–1389. doi:10.1016/j.jcrs.2013.03.027
6. Waikar S, Bhardwaj A. Morphological analysis of the lens nucleus. Med J Armed Forces India. 2000;56(3):195–197. doi:10.1016/S0377-1237(17)30164-8
7. Masket S, Lane SS, Lindstrom RL, Slade S. Cataract patients: younger every year. Rev Ophthalmol. 2013. Available from:
8. Vasavada A, Singh R. Surgical techniques for difficult cataracts. Curr Opin Ophthalmol. 1999;10:46–52. doi:10.1097/00055735-199902000-00009.
9. Fishkind WJ. Management of the soft nucleus. In: Fishkind WJ, editor. Complications in Phacoemulsification; Avoidance, Recognition, and Management. New York, NY: Thieme; 2002:105–111.
10. Buratto L. Techniques of phacoemulsification. In: Buratto L, editor. Phacoemulsification: Principles and Techniques. Thorofare, NJ: Slack; 1998:71–170.
11. Gomaa A, Liu C. Bowl-and-snail technique for soft cataract. J Cataract Refract Surg. 2011;37:8–10. doi:10.1016/j.jcrs.2010.10.027.
12. Zeng M, Liu X, Zhang X, et al. A comparative study of non-chopping rotation and axial rotation versus quick chop phacoemulsification techniques. Ophthalmic Surg Lasers Imaging. 2009;40:222–231. doi:10.3928/15428877-20090430-01.
13. Jardine GJ, Wong GC, Elsnab JR, Gale BK, Ambati BK. Endocapsular carousel technique phacoemulsification. J Cataract Refract Surg. 2011;37:433–437. doi:10.1016/j.jcrs.2010.12.013.
14. Guell JL, Vazquez M, Lucena J, et al. Phaco rolling technique. J of Cataract Refract Surg. 2004;30:2043–2045. doi:10.1016/j.jcrs.2004.05.005.
15. Brown DC. The phaco flip technique. Cataract Refractive Surg Today [Internet]. 2002;2(9):58–59. Available form:
16. Uthoff D, Holland D, Herbst T, Foerster J, Rüfer F, Pölzl M. Rock ‘n’ roll phacoemulsification technique: noncracking and nonchopping approach. J Cataract Refract Surg. 2013;39:1636–1639. doi:10.1016/j.jcrs.2013.08.042.
17. Fabian E, Maier M, Parasta A. New phaco fluidics control: CASE to prevent surge. Available from:
18. Fabian E, Maier M. New WhiteStar signature system: carouselling technique for emulsification of different hardness of the nuclei. Available from:
19. Fabian E. Phaco-Carouselling plus WhiteStar ICE technology: a cool solution. Available from:
20. Koch PS. Four quadrant cracking. In: Koch PS, editor. Converting to Phacoemulsification. Thorofare, NJ: Slack; 1992:75–79.
21. Braga-Mele R, Khan BU. Hydro-chop technique for soft lenses. J Cataract Refract Surg. 2006;32(1):18–20. doi:10.1016/j.jcrs.2005.11.023.
22. Malavazzi GR, Nery RG. Visco-fracture technique for soft lens cataract removal. J Cataract Refract Surg. 2011;37:11–12. doi:10.1016/j.jcrs.2010.10.032.
23. Yee J, Bray K, Godara P, et al. The V-Slice technique. Cataract Refractive Surg Today [Internet]. 2016. Available from:
24. Jacob S. Soft cataract phacoemulsification. Eurotimes. 2017. Available from:
25. Agarwal A, Jacob S. Supracapsular phacoemulsification. In: Agarwal A, Agarwal A, Jacob S, editors. Phacoemulsification. Panama City, Panama: Jaypee Highlights medical publishers Inc.; 2012:189–191.
26. Fishkind WJ, Wallace RB, Henderson BA, et al. Phaco machine settings. Cataract Refractive Surg Today [Internet]. 2008: 30–37. Available from:
27. Raviv T. The perfectly sized capsulorhexis. Cataract Refractive Surg Today [Internet]. 2009: 37–41. Available from:
Supplementary material
Notes: RAPID, a soft cataract phacoemulsification technique, is an acronym-based procedure where R is rotation of nucleus, A is alignment of phacoemulsification tip sideways, P is placement of tip adjacent to the nuclear rim, I is impaling of tip into nuclear rim and D is devouring wherein nucleus is aspirated/emulsified.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.