")
Back to Journals » Infection and Drug Resistance » Volume 15
A Prognostic Model for In-Hospital Mortality in Critically Ill Patients with Pneumonia
Authors Hu L, Zhang Y, Wang J, Xuan J, Yang J, Wang J, Wei B
Received 23 June 2022
Accepted for publication 26 October 2022
Published 2 November 2022 Volume 2022:15 Pages 6441—6450
DOI https://doi.org/10.2147/IDR.S377411
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Le Hu,1,2 Ying Zhang,1,2 Jia Wang,1,2 Jingchao Xuan,1,2 Jun Yang,1,2 Junyu Wang,1,2 Bing Wei1,2
1Emergency Medicine Clinical Research Center, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Beijing Key Laboratory of Cardiopulmonary Cerebral Resuscitation, Clinical Center for Medicine in Acute Infection, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Junyu Wang; Bing Wei, Department of Emergency Medicine, Beijing Chao-Yang Hospital Jingxi Branch, Capital Medical University, No. 5 Jingyuan Road, Shijingshan, Beijing, 100043, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To determine the utility of a novel serum biomarker for the outcome prediction of critically ill patients with pneumonia.
Patients and Methods: A retrospective analysis of critically ill patients was performed at an emergency department. The expression and prediction value of parameters were assessed. Binary logistic regression analysis was utilized to determine the indicators associated with in-hospital mortality of pneumonia patients. The Last Absolute Shrinkage and Selection Operator was used to further determine the independent predictors, which were validated by multiple logistic regression. The receiver operator characteristic curve was performed to assess their prediction values. A prognostic nomogram model was finally established for the outcome prediction for critically ill patients with pneumonia.
Results: Retinol-binding protein (RBP) was significantly reduced in non-survived and pneumonia patients. CURB-65 score, levels of RBP, and blood urea nitrogen (BUN) were associated with in-hospital mortality of critically ill patients with pneumonia. Their combination was determined to be an ideal prognostic predictor (area under the curve of 0.762) and further developed into a nomogram prediction model (c-index 0.764).
Conclusion: RBP is a novel in-hospital mortality predictor, which well supplements the CURB-65 score for critical pneumonia patients.
Keywords: critical illness, retinol-binding proteins, mortality prediction
Introduction
Pneumonia, community-acquired pneumonia (CAP) and nosocomial pneumonia, is the most prevalent observed and remains a major cause of mortality among critically ill patients.1,2 Moderate or severe pneumonia has the most potential to cause various complications due to excessive inflammation, hypoxia, and diffuse intravascular coagulation (DIC).3,4 These patients presented higher mortality, more intensive care unit (ICU) admission, and longer hospital stay because of the increasing complexity of the disease.5 Although various kinds of critical care and management have been developed for lifesaving over the past several decades,6 the mortality of critically ill patients with pneumonia remains high in the emergency department.7,8
So far, a broad range of severity scoring systems have been studied among critically ill patients such as Acute Physiology and Chronic Health Evaluation II (APACHE II) scores,9 Glasgow Coma Scale (GCS),10 Sequential Organ Failure Assessment (SOFA)11 and CURB-65 scores.12,13 However, distinct factors are expected to be responsible for patients with different etiologies or comorbidities. Therefore, it is necessary to discover novel biomarkers utilized to assess and triage pneumonia patients with high risk, which would be critically beneficial for clinicians to perform precision therapy, and plan the emphases for future monitoring. It is also of outstanding importance for resource allocation and ICU management.
Retinol-binding protein (RBP) is a class of proteins binding to and transporting retinol and its active metabolites in vivo, mainly including plasma retinol-binding protein (RBP4), cellular retinol-binding protein (CRBP), cellular retinoid-binding protein (CRABP), cellular retinaldehyde-binding protein (CRALBP) and interphotoreceptor retinol binding protein (IRBP). RBP is usually considered a reliable indicator of nutritional status. Recent research has demonstrated that RBP works as an important mediator in various physiological and pathological processes and is associated with numerous cardiovascular diseases.14,15 RBP4 was found to have pro-inflammatory effects partially mediated by Toll-like receptor 4 (TLR4). Elevated RBP4 is correlated positively with hypertension, diabetes, and cardiovascular disease.16–19 There is growing evidence that circulating RBP levels decrease specifically in critical illness patients with liver disease or sepsis.20,21 However, whether RBP is diagnostically relevant to a poor prognosis in critically ill patients with pneumonia remains unclear.
Here in this study, we determined the association of serum RBP with in-hospital mortality of critical pneumonia patients, and validated the potential of serum RBP for the prediction of the mortality of critically ill patients with pneumonia, especially supplementing the classic CURB-65 score.
Materials and Methods
Study Design
This was a retrospective, monocentric observational study in critically ill patients admitted to the Department of Emergency Medicine at Beijing Chao-Yang hospital, Jingxi Branch from October 2019 to March 2021. Totally 242 patients (139 with pneumonia, 103 with non-pneumonia) enrolled in this investigation. As potential predictors, demographic data including age, sex, vital signs, and comorbidities were recorded. Biochemical tests were carried out in the clinical pathology laboratory of the hospital following the manufacturer’s instructions, including serum RBP, blood urea nitrogen (BUN), PCT, homocysteine, platelet (PLT), aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TBIL) and C-reactive protein (CRP) concentrations. Scales of disease severity including GCS, APACHE II, SOFA, and CURB-65 scores were employed in this study. These clinical data and scales were collected on the day of treatment beginning and less than 24 hours after admission. This study was approved by the Ethics Committee of Beijing Chao-Yang Hospital. Written informed consent was not deemed necessary due to the retrospective design.
Inclusion and Exclusion Criteria
Critically ill patients hospitalized from October 2019 to March 2021 were above 18 year-old, diagnosed with pneumonia with radiographic infiltration and at least 2 compatible clinical symptoms (body temperature >38°C, productive cough, chest pain, shortness of breath, or crackles on auscultation) according to the definitions in current guidelines were included in this study.22 Critically ill patients without pneumonia were consecutively included during the study period. Patients with incomplete information or biochemical data defined in the “Study design” section were excluded from this study.
Outcome
Critical care outcome was set as the primary outcome, which is defined as either hospital discharge or in-hospital death.
Statistical Analyses
Information was presented as number (percentage) or median (interquartile range) for categorical characteristics. A univariate and multiple logistic regression model was employed using SPSS version 22.0 (SPSS, Inc., IL, USA). 2-tailed Chi-square (χ2) statistics test and Mann–Whitney U-test were performed to evaluate the categorical data and numerical data between survived and non-survived populations, respectively. Logistic least absolute shrinkage and selection operator (LASSO) regression was used to identify the most relevant variables associated with in-hospital mortality. A nomogram for predicting death risk in patients with pneumonia was established by R software, and the discrimination and calibration of the nomogram were evaluated using the concordance index (C-index). The receiver operator characteristic curve (ROC) was taken to evaluate the predictive ability of biomarkers for in-hospital death in critically ill patients with pneumonia.
Results
Demographic and Clinical Characteristics of Included Patients
A total of 139 critically ill patients with pneumonia were enrolled in this investigation, among which 36 patients (25.9%) were non-survived in the hospital. The baseline characteristics of the study population are summarized in Table 1. Eighty-one were male and fifty-eight were female, most of which were elderly patients above 65-year-old (86.3%). The most common comorbidity in the whole study population was cerebrovascular disease (n = 36, 25.9%), followed by diabetes (n = 29, 20.9%), and cardiovascular disease (n = 25, 18.0%). The prevalence of chronic obstructive pulmonary disease, chronic kidney disease, and hepatopathy as comorbidities at baseline was presented as 10.1%, 7.9% and 3.6%, respectively. The results of various biochemical parameters and scoring systems indicating the severity of illness, APACHE II score, GCS score, SOFA score, CURB-65 score are presented in Table 1. Furthermore, the grouped statistics of these characteristics are presented and compared between survived and non-survived patients in Table 1.
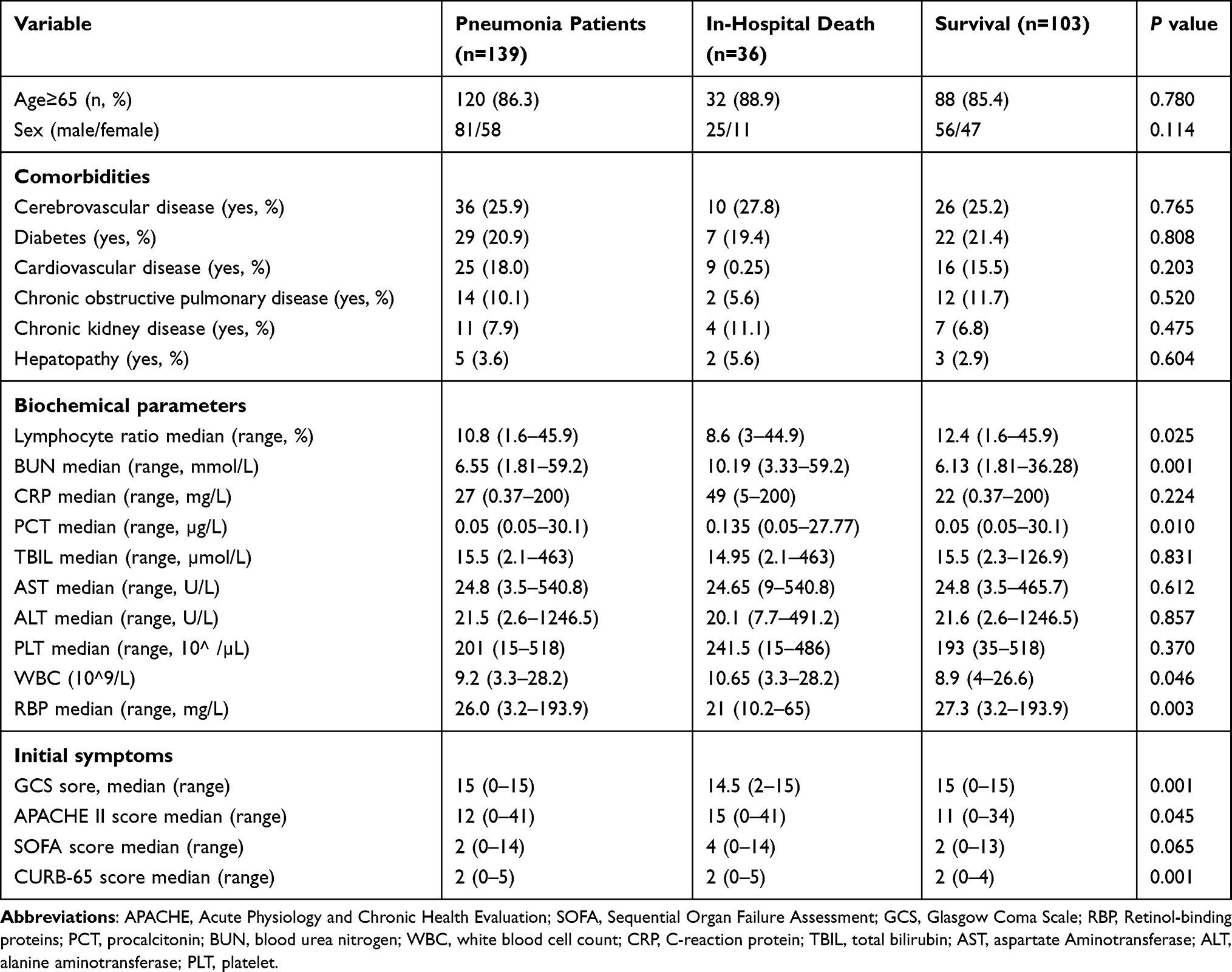 |
Table 1 Demographics, Laboratory and Clinical Information of the Patients |
RBP Levels are Particularly Reduced in Critically Ill Patients with Pneumonia and Non-Survived Patients
Among all the patients enrolled, the median serum concentration of RBP in pneumonia patients was 26.0 mg/L (range, 3.2–193.9 mg/L) compared with non-pneumonia patients (median 34.5 mg/L, range 3.9–123.5 mg/L, shown in Figure 1A). The RBP level of non-survived patients was particularly lower within the total critically ill patients (Figure 1B) or the pneumonia patients (Figure 1C). To identify the factors impacting on mortality of pneumonia critical patients, all the enrolled biochemical parameters and scaling systems were compared among the patients. The results showed that survived patients exhibited higher GCS scores (P=0.001), RBP level (P=0.003), and lymphocyte ratios (P=0.025), but lower CURB-65 scores (P=0.001), APACHE II scores (P=0.045), PCT levels (P=0.010), WBC (P=0.046) and BUN levels (P=0.001) than those of the non-survived patients (Table 1 and Figure 1).
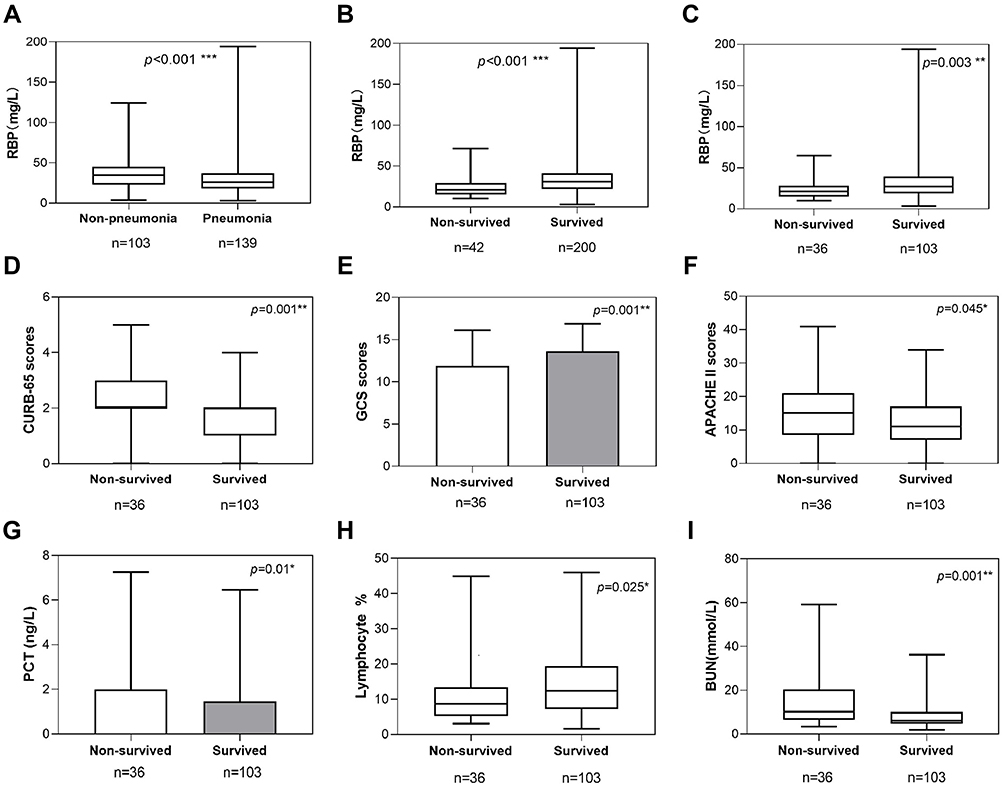 |
Figure 1 Factors associated with mortality for critically ill patients. (A), RBP levels in serum sample from the patients with or without pneumonia. (B). RBP levels in serum sample from survived or non-survived cases. (C), RBP levels in serum sample from survived or non-survived cases in the patients with pneumonia. CURB-65 (D), GCS Scores (E), APACHE II (F), PCT level (G), lymphocyte ratio (H) and BUN level (I), which showed significant difference (P<0.05) between survived or non-survived cases with pneumonia. (*P<0.05, **P<0.01). |
Identification of Potential Predictors for the Outcome of Critically Ill Patients with Pneumonia
After the identification of these related factors, we further analyzed their potential as prognostic indicators. First, a univariate logistic regression analysis was performed to identify the specific independent indicators for the mortality of the enrolled patients with pneumonia. As listed in Table 2, scores of SOFA, CURB-65, APACHE II, and GCS, levels of RBP, BUN, and WBC were identified as the independent prognostic risk factors, among which CURB-65 score (OR = 2.023, P = 0.001), SOFA score (OR = 1.146, P = 0.018), APACHE II score (OR = 1.055, P = 0.041), BUN (OR = 1.059, P = 0.003), WBC (OR = 1.088, P = 0.026) are positively correlated with mortality, while RBP level (OR = 0.958, P = 0.013) and GCS score (OR = 0.885, P = 0.014) are negatively correlated with mortality.
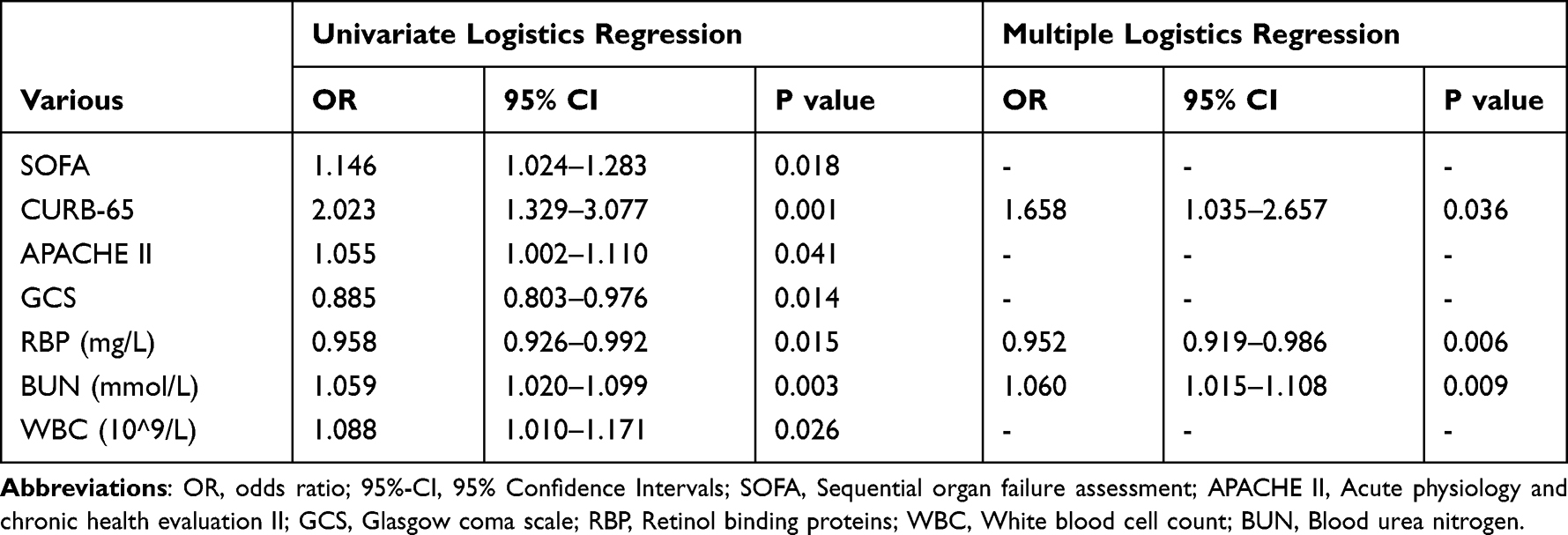 |
Table 2 Univariate and Multiple Logistic Regression Analyses to Identify the Individual Risk Factors for Critically Ill Patients with Pneumonia |
Then, to determine a combination consisting of the most influencing factors, additional least absolute shrinkage and selection operator (LASSO) regression was incorporated to select parameters associated mostly with the mortality of patients with pneumonia. The result of LASSO regression is shown in Figure 2, which reveals that the CURB-65 score, BUN level, and RBP level were highly associated with the outcome of critical illness. Finally, multiple logistic regression was utilized based on the results of LASSO regression to evaluate the significance of the risk factors, listed in the multiple logistic regression analysis in Table 2. Results show that CURB-65 (OR = 1.658, P = 0.036) and BUN (OR = 1.059, P = 0.009) are positively correlated with, and RBP (OR = 0.952, P = 0.006) is negatively correlated with the outcome as indicators.
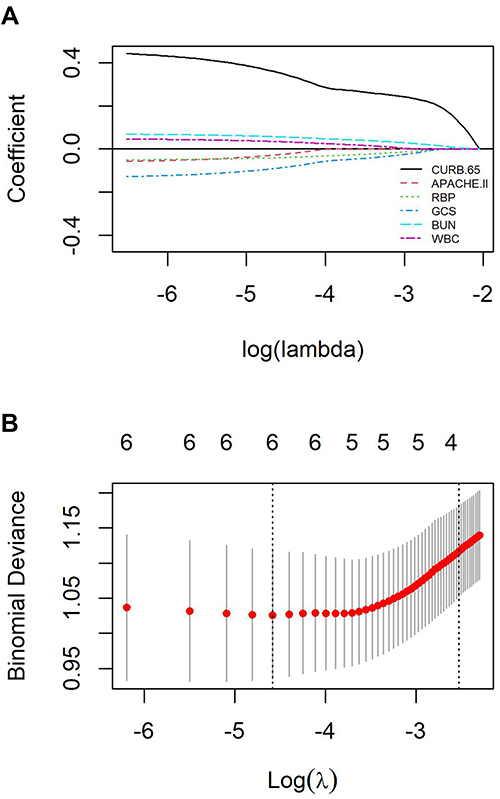 |
Figure 2 Logistic LASSO regression for the prediction of in-hospital mortality. (A), LASSO coefficient profiles of the potential risk factors for pneumonia patients. 10-fold cross-validation was taken as the threshold value for parameter lambda selection. X axis represents the log of penalty coefficient lambda while Y axis represents the. (B), Confidence interval in every lambda of LASSO regression. X axis represents the log (λ) while Y axis represents the partial likelihood deviance (binomial deviance). Ten-fold cross-validation in the log (λ) sequence was used to plot the vertical dotted line at the value selected. The three risk factors were selected by the lambda at which the minimal deviance was achieved (minimum criteria and the 1-SE of the minimum criteria). |
Assessment of Performance of the Predictors
Predictive performance of the three identified individual predictors and their combinations, as well as three other classic independent scales, SOFA, APACHE II, and GCS, were assessed by ROC curve analysis in the critically ill patients with pneumonia, the results of which are presented in Table 3. All the three identified indicators and their combinations performed better than SOFA, APACHE II, or GCS score, whereas the RBP level achieved an area under the ROC curve (AUC) of 0.666 (95% CI = 0.566–0.766), following the CURB-65 scores of 0.682 (95% CI = 0.582–0.782), and the BUN of 0.679 (95% CI = 0.577–0.782). The AUC for assessment of RBP and BUN combined with CURB-65 score was 0.762 (95% CI = 0.667–0.857), with the Youden index of 42.0%, which is the best among all the predictors. Interestingly, the specificity of the classic CURB-65 system evaluated by ROC analysis is high at 83.5% while the sensitivity is only 41.7%. RBP has a sensitivity of 63.9% and the sensitivity of the combination of CURB-65, RBP, and BUN increases as high as 75.0% with a specificity of 67.0%.
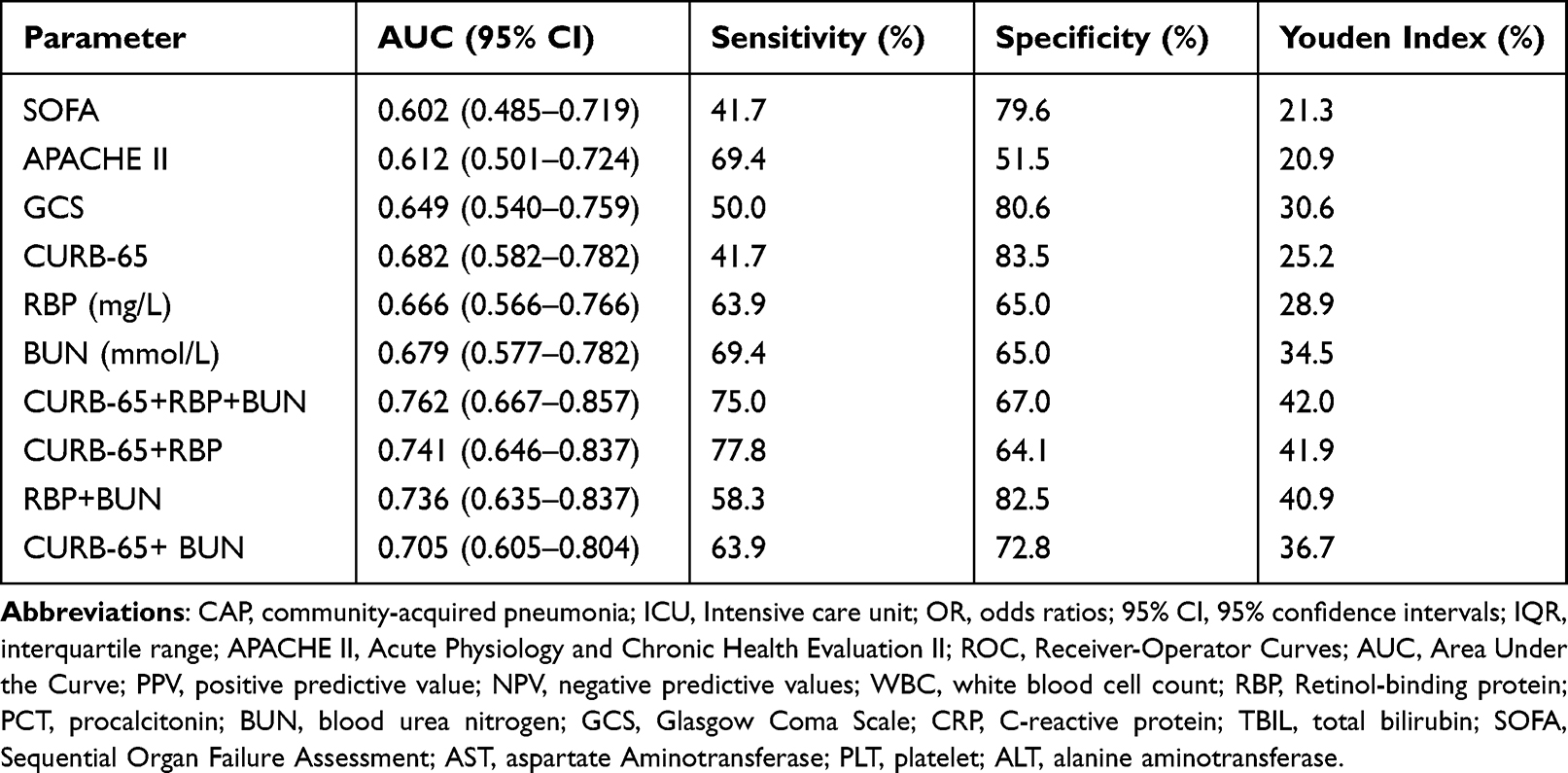 |
Table 3 Receiver Operating Characteristic (ROC) Curve Analyses Comparing the Diagnostic Power of New Parameters in Predicting In-Hospital Mortality for Critically Ill Patients with Pneumonia |
Effects of the Survival Prediction Model Established Based on the Predictors
We introduced nomogram regression with the significantly correlated factors consisting of CURB-65 scores, RBP level, and BUN level integrated, for predicting the mortality of an individual critically ill patient with pneumonia (Figure 3A). The calibration curve (c-index 0.764) indicates that the novel prediction approximates the actual outcomes more closely (Figure 3B) and is quite more accessible in common situations.
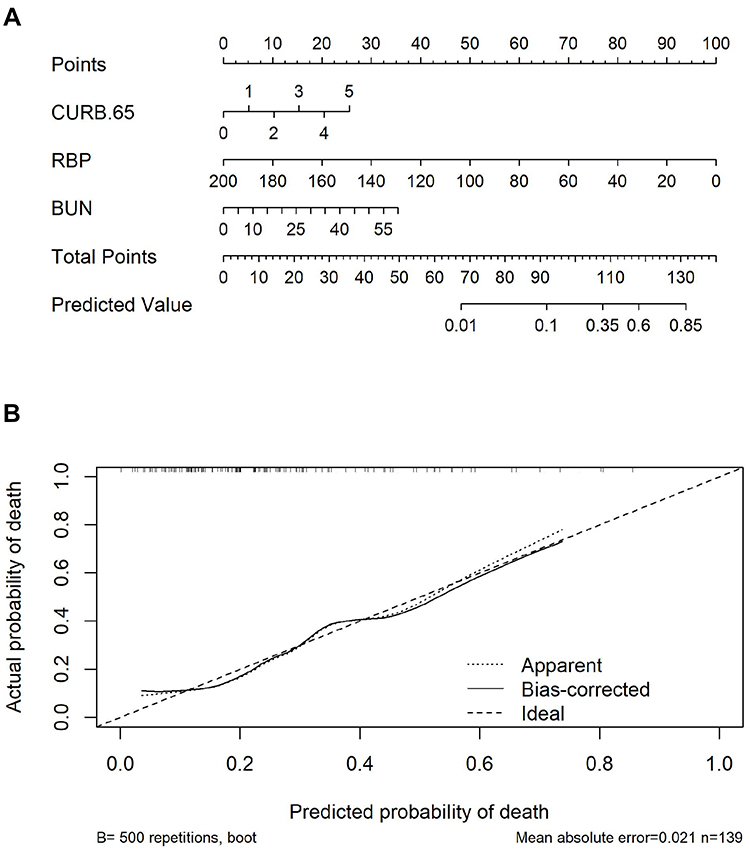 |
Figure 3 Nomogram Analysis for the prediction of the unfavorable outcome. (A) A nomogram chart for the prediction of in-hospital mortality within pneumonia patients. (B) The corresponding calibration curves of the nomogram above. A dashed line is a reference line where an ideal nomogram should lie. |
Discussion
In this study, we explored a novel serum predictor model for in-hospital mortality of critical illness patients with pneumonia. The following are the most compelling results of this study: (1) A low level of RBP showed a close correlation with the mortality in the population with pneumonia. (2) RBP was a novel prognostic indicator more reliable than some classic scaling systems such as SOFA, APACHE II, and GCS in predicting the in-hospital mortality of critically ill pneumonia patients. (3) High sensitivity of RBP concentration compensated for the disadvantage of CURB-65 in differentiating non-survivors. (4) A more reliable and accessible nomogram was established to predict the probability of death in critically ill patients with pneumonia.
Despite many widely used severity scoring systems designed to stratify patients according to the severity of illness and to predict in-hospital mortality and ICU readmission in critically ill patients, for instance, a high APACHE II score is generally linked to severe critical illness,23,24 there are still a lot of unmet needs for more timely and accurate outcome prediction. One important reason for such dissatisfaction is the complex complications of the critical illness patient in the emergency department. Different comorbidities make it more complicated when administrate proper treatments and make predictions. Some scoring systems are designed specifically for a particular complication in critical illness, such as SOFA, GCS, CURB-65, etc. Each of these may be effective for part of the critically ill patients but does not work well for others. As we confirmed with our cases (data not shown), SOFA score, APACHE II score, GCS score, and CURB-65 score were individual risk factors for critically ill patients generally, but only CURB-65 is correlated with the pneumonia population as presented in this study. CURB-65 is previously reported quite suitable for mortality risk prediction for critically ill patients specifically with pneumonia,25 which is in line with our result. In this study, a novel serum biomarker, RBP level, is identified not only as an individual prognostic predictor (in-hospital death) but also as improving the CURB-65 system when combined with it, indicating promising clinical applicability.
RBP is an acute responsive protein, reflecting inflammation and nutritional determinants.26,27 Recently, the serum RBP concentration was shown to be a crucial signal for the organ function, metabolism, and inflammation status of critically ill patients, especially the RBP4.28 A low concentration of RBP at baseline was found associated with a bad outcome in liver ICU patients, which could predict short-term mortality of the patients, but not long-term mortality.29 Consistent with these findings, we also present here that RBP level is specifically reduced in the non-survived pneumonia population of the study, indicating that low RBP was the main risk factor for in-hospital mortality in critical pneumonia patients. The predictive performance of the baseline RBP was much better than the severity scoring systems other than CURB-65, which demonstrates it as a better predictor in severe comorbidities. ROC analysis revealed CURB-65 is a highly specific (83.5%) predictor but relatively low sensitive (41.7%). Then, the combination of CURB-65, RBP, and BUN showed an improved sensitivity (75.0%) analyzed with ROC yet a compromised specificity (67.0%). This result implies that RBP probably supplements CURB-65 system in sensitivity to achieve improvement.
High BUN concentration at admission was reported as an independent risk parameter for predicting mortality in critically ill patients.30,31 Moreover, serum BUN concentration was significantly higher in non-survived patients, and also shows the potential as an outcome prediction indicator combined with RBP. BUN level was implied correlated with RBP level in some cases indicating that they may share some mechanisms.32,33 BUN level is considered in the CURB-65 system (score 1 point when above 7 mmol/L), which strongly implies the role of BUN in predicting the outcome of critical pneumonia patients. Here, the inclusion of BUN into the prediction model containing CURB-65 increases its weight, which better balances the specificity and sensitivity.
Our study has several limitations. First, the sample size of this single-center investigation is relatively small. Selection bias may exist so a multiple-center study with larger sample size is needed to verify the mortality-associated risk factors identified in this study. Second, these findings proved that baseline RBP levels predicted short-term mortality well in critically ill patients but more work should be done to assess the efficacy of RBP in predicting long-term mortality. Third, total RBP serum level was employed in this study in which subtypes of RBP were not discriminated. A distinct subtype of RBP probably has differentiated biological functions. Therefore, detection and analysis of specific RBP subtypes in the prediction are needed in future investigations to optimize the model. Last, RBP showed its shortcoming of specificity as a predictor when it supplements CURB-65 with sensitivity, which suggests that this combinational predicting model may be optimized further by incorporating another critical illness or pneumonia highly specific biomarker in the future. On the other hand, we only confirmed the predictive role of RBP in the pneumonia population of this study. The validity of RBP in outcome prediction of critically ill patients with other complications needs to be further investigated in the future, to reveal whether RBP is pneumonia specific or general for comorbidity situations.
Conclusion
In summary, our findings revealed that two serum biomarkers, RBP and BUN, were identified closely correlated with the outcome of critically ill patients with pneumonia. The combination of RBP level, BUN level, and the classic CURB-65 scoring system showed the best performance and then was developed as a prediction model.
Data Sharing Statement
All original data used in the study have been de-identified and are available from the corresponding author Bing Wei on request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Beijing Chao-Yang Hospital, and written informed consent was not deemed necessary due to the retrospective design. The patients’ data were anonymized or maintained with confidentiality. This study was conducted in compliance with the Declaration of Helsinki.
Acknowledgments
We would like to thank for the helpful contributions of all staff of Emergency Medicine Clinical Research Center.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fernando SM, Tran A, Cheng W, et al. Diagnosis of ventilator-associated pneumonia in critically ill adult patients-a systematic review and meta-analysis. Intensive Care Med. 2020;46:1170–1179. doi:10.1007/s00134-020-06036-z
2. Zaragoza R, Vidal-Cortés P, Aguilar G, et al. Update of the treatment of nosocomial pneumonia in the ICU. Crit Care. 2020;24:383. doi:10.1186/s13054-020-03091-2
3. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323:1061–1069. doi:10.1001/jama.2020.1585
4. Klok FA, Kruip MJ, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020;191:145–147. doi:10.1016/j.thromres.2020.04.013
5. Lee JS, Giesler DL, Gellad WF, et al. Antibiotic therapy for adults hospitalized with community-acquired pneumonia: a systematic review. JAMA. 2016;315:593–602. doi:10.1001/jama.2016.0115
6. Song Y, Yao C, Yao Y, et al. XueBiJing injection versus placebo for critically Ill patients with severe community-acquired pneumonia: a randomized controlled trial. Crit Care Med. 2019;47:e735–e743. doi:10.1097/CCM.0000000000003842
7. Larcher R, Pineton de Chambrun M, Garnier F, et al. One-year outcome of critically ill patients with systemic rheumatic disease: a multicenter cohort study. Chest. 2020;158:1017–1026. doi:10.1016/j.chest.2020.03.050
8. Micek ST, Chew B, Hampton N, et al. Case-control study assessing the impact of nonventilated hospital-acquired pneumonia on patient outcomes. Chest. 2016;150:1008–1014. doi:10.1016/j.chest.2016.04.009
9. Huang J, Xuan D, Li X, et al. The value of APACHE II in predicting mortality after paraquat poisoning in Chinese and Korean population: a systematic review and meta-analysis. Medicine. 2017;96:e6838. doi:10.1097/MD.0000000000006838
10. de Munter L, Polinder S, Lansink KW, et al. Mortality prediction models in the general trauma population: a systematic review. Injury. 2017;48:221–229. doi:10.1016/j.injury.2016.12.009
11. Wang H, Kang X, Shi Y, et al. SOFA score is superior to APACHE-II score in predicting the prognosis of critically ill patients with acute kidney injury undergoing continuous renal replacement therapy. Ren Fail. 2020;42:638–645. doi:10.1080/0886022X.2020.1788581
12. Sanz F, Restrepo MI, Fernández E, et al. Hypoxemia adds to the CURB-65 pneumonia severity score in hospitalized patients with mild pneumonia. Respir Care. 2011;56:612–618. doi:10.4187/respcare.00853
13. Li M, Liu J, Tan R, et al. Risk factors for slowly resolving pneumonia in the intensive care unit. J Microbiol Immunol Infect. 2016;49:654–662. doi:10.1016/j.jmii.2014.11.005
14. Olsen T, Blomhoff R. Blomhoff, retinol, retinoic acid, and retinol-binding protein 4 are differentially associated with cardiovascular disease, type 2 diabetes and obesity: an overview of human studies. Adv Nutr. 2020;11:644–666.
15. Blaner WS, Brun PJ, Calderon RM, et al. Retinol-binding protein 2 (RBP2): biology and pathobiology. Crit Rev Biochem Mol Biol. 2020;55:197–218. doi:10.1080/10409238.2020.1768207
16. Moraes-Vieira PM, Yore MM, Sontheimer-Phelps A, et al. Retinol binding protein 4 primes the NLRP3 inflammasome by signaling through Toll-like receptors 2 and 4. Proc Natl Acad Sci USA. 2020;117:31309–31318. doi:10.1073/pnas.2013877117
17. Abbasi F, Moosaie F, Khaloo P, et al. Gelatinase-associated lipocalin and retinol-binding protein-4 as biomarkers for diabetic kidney disease. Kidney Blood Press Res. 2020;45:222–232. doi:10.1159/000505155
18. Li XZ, Zhang KZ, Yan JJ, et al. Serum retinol-binding protein 4 as a predictor of cardiovascular events in elderly patients with chronic heart failure. ESC Heart Fail. 2020;7:542–550. doi:10.1002/ehf2.12591
19. Si Y, Liu J, Han C, et al. The correlation of retinol-binding protein-4 and lipoprotein combine index with the prevalence and diagnosis of acute coronary syndrome. Heart Vessels. 2020;35:1494–1501. doi:10.1007/s00380-020-01627-8
20. Lee MJ, Gong DW, Burkey BF, et al. Pathways regulated by glucocorticoids in omental and subcutaneous human adipose tissues: a microarray study. Am J Physiol Endocrinol Metab. 2011;300:e571–80. doi:10.1152/ajpendo.00231.2010
21. Langouche L, Vander Perre S, Frystyk J, et al. Adiponectin, retinol-binding protein 4, and leptin in protracted critical illness of pulmonary origin. Crit Care. 2009;13(4):R112. doi:10.1186/cc7956
22. Grief SN, Loza JK. Guidelines for the evaluation and treatment of pneumonia. Prim Care. 2018;45:485–503. doi:10.1016/j.pop.2018.04.001
23. Kuo WK, Hua CC, Yu CC, et al. The cancer control status and APACHE II score are prognostic factors for critically ill patients with cancer and sepsis. J Formos Med Assoc. 2020;119:276–281. doi:10.1016/j.jfma.2019.05.012
24. Lee H, Lim CW, Hong HP, et al. Efficacy of the APACHE II score at ICU discharge in predicting post-ICU mortality and ICU readmission in critically ill surgical patients. Anaesth Intensive Care. 2015;43:175–186. doi:10.1177/0310057X1504300206
25. Patel S. Calculated decisions: CURB-65 score for pneumonia severity. Emerg Med Pract. 2021;23:CD1–CD2.
26. Shin SJ, Chen CH, Kuo WC, et al. Disruption of retinoid homeostasis induces RBP4 overproduction in diabetes: O-GlcNAcylation involved. Metabolism. 2020;113:154403. doi:10.1016/j.metabol.2020.154403
27. Zabetian-Targhi F, Mahmoudi MJ, Rezaei N, et al. Retinol binding protein 4 in relation to diet, inflammation, immunity, and cardiovascular diseases. Adv Nutr. 2015;6:748–762. doi:10.3945/an.115.008292
28. Koch A, Weiskirchen R, Sanson E, et al. Circulating retinol binding protein 4 in critically ill patients before specific treatment: prognostic impact and correlation with organ function, metabolism and inflammation. Crit Care. 2010;14:R179. doi:10.1186/cc9285
29. Chen WT, Lee MS, Chang CL, et al. Retinol-binding protein-4 expression marks the short-term mortality of critically ill patients with underlying liver disease: lipid, but not glucose, matters. Sci Rep. 2017;7:2881. doi:10.1038/s41598-017-03096-y
30. Arihan O, Wernly B, Lichtenauer M, et al. Blood Urea Nitrogen (BUN) is independently associated with mortality in critically ill patients admitted to ICU. PLoS One. 2018;13:e0191697. doi:10.1371/journal.pone.0191697
31. Wernly B, Lichtenauer M, Vellinga NAR, et al. Blood urea nitrogen (BUN) independently predicts mortality in critically ill patients admitted to ICU: a multicenter study. Clin Hemorheol Microcirc. 2018;69:123–131. doi:10.3233/CH-189111
32. Liu SJ, Zhai YP, Yu YP, et al. Significance of low molecular weight urinary protein for assessment of early renal damage in patients with multiple myeloma. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2013;21:410–414. doi:10.7534/j.issn.1009-2137.2013.02.031
33. Zhang WX, Zhou W, Zhang ZM, Zhang ZQ, He JF, Shi BY. Decreased retinol-binding protein 4 in the sera of patients with end-stage renal disease after kidney transplantation. Genet Mol Res. 2014;13:8126–8134. doi:10.4238/2014.October.7.7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.