")
Back to Journals » Journal of Inflammation Research » Volume 15
A Potential Role of Ethosuximide and Pentoxifylline in Relieving Abdominal Pain in Irritable Bowel Syndrome Patients Treated with Mebeverine: A Randomized, Double-Blind, Placebo-Controlled Trial
Authors El-Haggar SM, Hegazy SK, Abd-Elsalam SM, Elkaeed EB , Al-Karmalawy AA , Bahaa MM
Received 4 November 2021
Accepted for publication 4 February 2022
Published 19 February 2022 Volume 2022:15 Pages 1159—1172
DOI https://doi.org/10.2147/JIR.S346608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
This paper has been retracted.
Sahar M El-Haggar,1 Sahar K Hegazy,1 Sherief M Abd-Elsalam,2 Eslam B Elkaeed,3 Ahmed A Al-Karmalawy,4 Mostafa M Bahaa5
1Clinical Pharmacy Department, Faculty of Pharmacy, Tanta University, El-Gharbia Government, Tanta, 31527, Egypt; 2Tropical Medicine and Infectious Diseases Department, Faculty of Medicine, Tanta University, Tanta, 315274, Egypt; 3Department of Pharmaceutical Sciences, College of Pharmacy, AlMaarefa University, Riyadh, 13713, Saudi Arabia; 4Department of Pharmaceutical Medicinal Chemistry, Faculty of Pharmacy, Horus University-Egypt, New Damietta, 34518, Egypt; 5Pharmacy Practice Department, Faculty of Pharmacy, Horus University, New Damietta, Egypt
Correspondence: Mostafa M Bahaa, Pharmacy Practice Department, Faculty of Pharmacy, Horus University, New Damietta, Egypt, Tel +201025538337, Email [email protected]; [email protected]
Background and Purpose: Irritable bowel syndrome (IBS) is defined as an association of chronic abdominal pain with bowel habit abnormalities, without clear organic dysfunction. T-type calcium channels and low-grade mucosal inflammation are linked to abdominal pain; however, medical treatments for IBS abdominal pain are largely ineffective. In this study, we investigated if pentoxifylline (PTX) and ethosuximide could potentially alleviate abdominal pain in patients with IBS treated with mebeverine.
Methods: We recruited 150 patients from Tanta University Hospital to this randomized, prospective, and double blinded study. Patients were randomly allocated to three groups (n = 50). Group 1 (mebeverine) received 135 mg mebeverine three times/day (t.i.d). Group 2 (ethosuximide group) received 135 mg mebeverine t.i.d plus 250 mg ethosuximide twice daily (b.i.d) and group 3 (PTX group) received 135 mg mebeverine t.i.d plus 400 mg PTX b.i.d. Patients were assessed by a gastroenterologist at baseline and 6 months after therapy. Serum interleukin-8 (IL-8), IL-6, tumor necrosis-α (TNF-α), fecal myeloperoxidase, and fecal neutrophil gelatinase associated lipocalin (NGAL) levels were measured before and after therapy. The numeric pain rating scale (NRS) was also assessed before and after therapy.
Primary Outcomes: Reduced NRS scores and abdominal pain relief.
Secondary Outcomes: Decreased inflammatory biomarkers.
Results: After 6 months, groups 2 and 3 showed a significantly greater reduction in serum IL-8, IL-6, TNF-α, fecal myeloperoxidase, and fecal NGAL levels when compared to group 1 after therapy. Both groups 2 and 3 showed significant reductions in NRS scores when compared to the group 1.
Conclusion: Ethosuximide and PTX may be promising, novel adjunct drugs to antispasmodics for relieving abdominal pain in patients with IBS.
Trial Registration: Identifier: NCT04217733.
Keywords: IBS, inflammation, pentoxifylline, Ca++ channels, ethosuximide
Introduction
Irritable bowel syndrome (IBS) is characterized by abdominal discomfort, bloating, and changes in bowel movements in the absence of clear pathological features.1 A primary pathophysiological occurrence in IBS involves an altered intestinal epithelial barrier, which facilitates persistent low-grade mucosal inflammation resulting in visceral hypersensitivity (VH) and pain.2 In several chronic pain animal models, hypersensitivity refers to increased excitability associated with ion channel expression remodeling.3–5 In a case-controlled study, the Cav3.2 channel was found to be overexpressed in the colonic mucosa of individuals with IBS when compared with asymptomatic controls. Furthermore, blocking this channels also inhibited colonic hypersensitivity in an IBS animal model.1
Inflammation appears to have a role in IBS pathogenesis. One IBS study reported that mucosal inflammation persisted at the microscopic and molecular level, with the increased recruitment of enteroendocrine cells and inflammatory cytokines.6 In individuals with IBS, colonic hypersensitivity, T-type calcium channel overexpression, and low-grade mucosal inflammation resulted in inflammatory cytokine release and abdominal pain.1,7 It was also reported that the gastrointestinal mucosa of patients with IBS had higher inflammatory cytokine levels, plus higher mast cell numbers in close proximity to enteric nerve fibers.8 Anxiety and abdominal pain are also linked to higher cytokine levels in the colonic mucosa and increased pro-inflammatory cytokine production in isolated peripheral blood mononuclear cells.9
Medications that increase cyclic adenosine monophosphate (cAMP) levels can also decrease pro-inflammatory mediator levels and prevent mucosal inflammation by activating protein kinase A and inhibiting interleukin (IL) and tumor necrosis-α (TNF-α) synthesis.10
Mebeverine is a β-phenyl ethylamine derivative of reserpine that acts on smooth muscle cells in a relatively precise manner, without the adverse effects of atropine.11 The derivative also relieves spasms while maintaining normal gut motility by acting directly on the smooth muscle of the gastrointestinal tract.
Ethosuximide is a T-type calcium channel blocker with anti-epileptic functions. The Cav3.2 channel has been extensively investigated and linked to nociceptive pain.12 In an animal model of butyrate-induced VH, Marger et al showed that Cav3.2 channels were involved in chronic visceral pain, and by blocking these channels with ethosuximide, abdominal pain was reduced.13
Pentoxifylline (PTX) is a methyl-xanthine derivative that increases erythrocyte flexibility, decreases plasma fibrinogen, inhibits neutrophil activation, and suppresses erythrocyte/platelet aggregation, while also possessing antioxidant and anti-inflammatory characteristics.14 PTX exerts anti-inflammatory effects by inhibiting phosphodiesterase and activating the adenosine 2 receptor.15
In this study, we investigated if PTX and ethosuximide alleviated abdominal pain in patients with IBS treated with mebeverine.
Patients and Methods
Patients
150 patients who met inclusion criteria were recruited between November 2019 and January 2021 at the Gastroenterology Department, Faculty of Medicine, Tanta University, Egypt. Patients and physicians were blinded to exposure type and randomization. Study medications were supplied to patients by an unblinded pharmacist to ensure correct treatment assignment, however, the pharmacist was not included in outcome assessments.
Inclusion Criteria
Patients older than 18 years old, IBS symptoms diagnosed using ROME VI criteria, a negative pregnancy test, effective contraception use, and an average Numeric Pain Rating Scale (NRS) > 4 were included.
Exclusion Criteria
Diabetic, breastfeeding patients, and patients with liver abnormalities were excluded to avoid drug accumulation due to defective metabolic pathways, and also hepatic patients with elevated inflammatory cytokine levels, such as IL-6, IL-1, and TNF-α.16 Patients taking PTX for fatty liver disease were excluded to avoid anti-fibrotic reactions;17 these patients may have generated false positive results related to PTX therapeutic efficacy.
Patients with renal disease were excluded due to higher inflammatory cytokine levels potentially leading to false positive results. PTX is used for kidney disease as it has anti-inflammatory effects.18,19
Patients with chronic depression on tricyclic antidepressants and selective serotonin reuptake inhibitors were excluded. These drugs are widely used to treat patients with IBS as they relieve abdominal pain via analgesic effects. False positive results could be generated with mebeverine and PTX.20
Patients taking anti-epileptic drugs and psychotic patients were excluded; antipsychotic drugs are widely used to manage abdominal pain in IBS, thus, positive results would not only be attributed to study medications, but possibly to antipsychotic drugs, thereby generating false positive results.21
Patients with known allergies to mebeverine, succinimide, and PTX were excluded.
Study Design
This double blinded, randomized, prospective clinical trial compared the safety and effectiveness of ethosuximide and PTX in combination with mebeverine in relieving abdominal pain in patients with IBS.
The National Research Ethics Committee granted approval for this investigation (Tanta University Ethical Committee) with the approval code, 33422/10/19. In addition, the study was performed in accordance with the ethical standards of the Helsinki Declaration and associated changes in 1964. Patients were advised they could leave the trial at any time.
This study was registered in 2020 (at www.ClinicalTrials.gov, reference number NCT04217733) and called; A comparative study to assess the safety and effectiveness of ethosuximide and pentoxifylline in the treatment of abdominal pain related to irritable bowel syndrome.
As indicated in the consolidated standards of reporting trials (CONSORT) flow diagram (Figure 1), patients fulfilling inclusion criteria and providing written informed consent were randomly divided into three groups (n = 50).
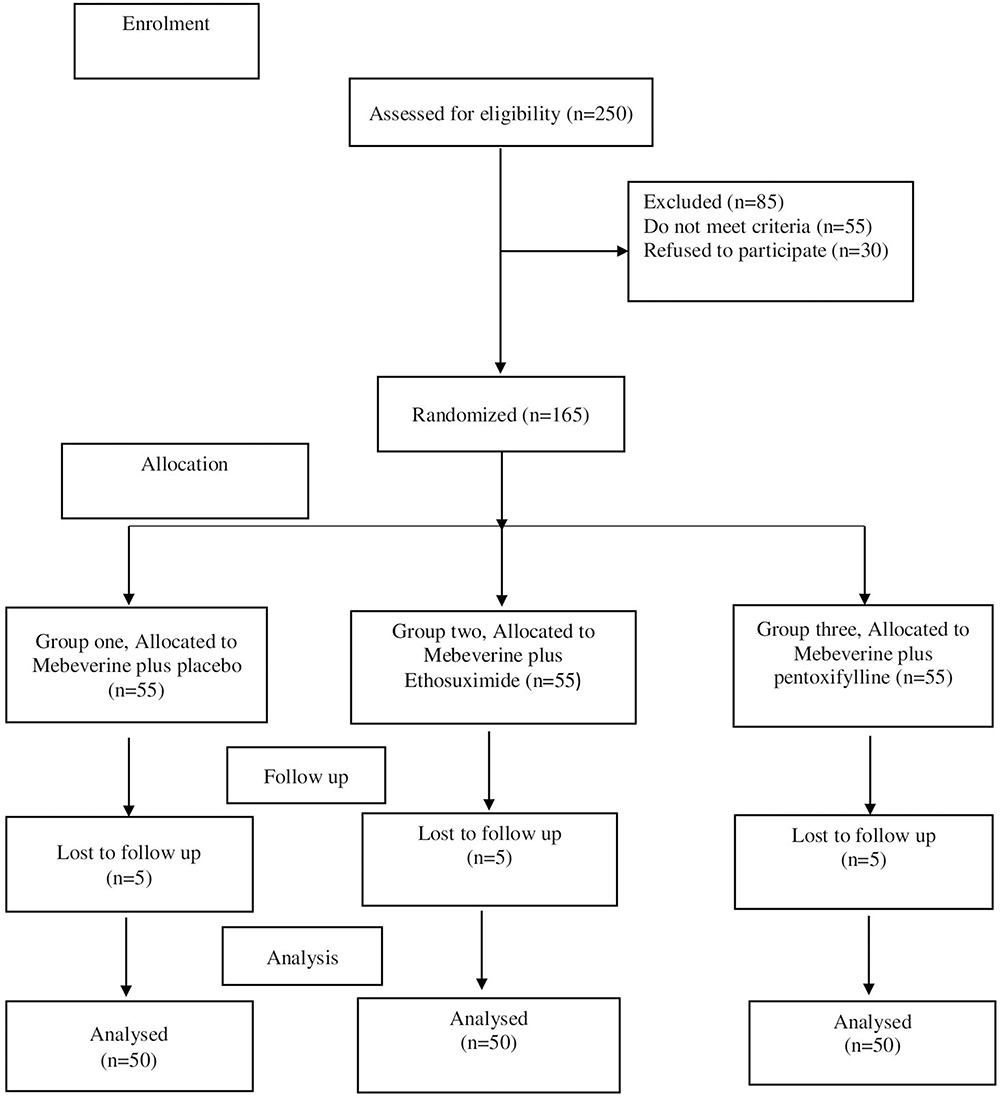 |
Figure 1 CONSORT diagram showing the disposition of all patients screened for the study. |
Group 1 was the control group; patients received 135 mg mebeverine hydrochloride capsules t.i.d plus placebo for 6 months (Coloverine 135 mg, Chemi Pharm, Egypt). This group included 22 patients with IBS predominant diarrhea and 28 patients with IBS predominant constipation.
Group two received 135 mg mebeverine capsules t.i.d plus 250 mg ethosuximide capsules b.i.d for 6 months (250 mg Ethoxa, Delta Pharm, Egypt). This group included 25 patients with IBS predominant diarrhea and 25 patients with IBS predominant constipation.
Group three received 135 mg mebeverine capsules t.i.d plus 400 mg PTX tablets b.i.d for 6 months. (400 mg Trental, Sanofi Aventis, Egypt). This group included 30 patients with IBS predominant diarrhea and 20 patients with IBS predominant constipation.
Sample Size Calculations
Sample size was calculated using data from a previous study,22,23 therefore, we calculated a sample size of 50 patients. We also take into consideration dropout rates.
Study Protocol
IBS patients were assessed for eligibility and underwent detailed physical, mental, and psychological assessments. Patients were randomized in a 1:1 ratio using a computer generated code according to CONSORT guidelines to receive either 135 mg mebeverine tablets three times daily (group 1), or 135 mg mebeverine three times daily plus 250 mg ethosuximide two times daily (group 2) or 135 mg mebeverine three times daily plus 400 mg PTX two times daily (group 3). Selected doses for mebeverine (135 mg three daily), PTX (400 mg twice daily), and ethosuximide (250 mg twice daily) were based on previous studies.24–26 All drugs were orally administered and subjects were advised on lifestyle and dietary changes.
Follow-Up
Patients were followed-up with weekly telephone calls and monthly meetings. At the first visit, patients underwent a full medical history, liver function tests, kidney function tests, thyroid function tests, and complete blood counts to exclude any organic dysfunction. Serum inflammatory biomarkers (IL-6, IL-8, and TNF-α) and fecal inflammatory biomarkers (neutrophil gelatinase associated lipocalin (NGAL) and myeloperoxidase) were also measured. NRS was also assessed. All patients underwent the same assessments as on the first visit. Also, patients were continuously assessed for the development of new symptoms or treatment-related adverse events.
Therapeutic Assessments
Therapeutic effectiveness was evaluated through assessment of NRS scores, measurement of serum IL-6, IL-8, TNF-alpha, fecal NGAL, and fecal myeloperoxidase.
Sample Collection
Before study commencement and at 6 months after the intervention, between 8 am and 10 am in the morning, 10 mL venous blood was withdrawn from the antecubital vein. For complete blood count analysis, 2 mL blood was slowly transferred into EDTA tubes. The remaining 8 mL was slowly transferred into plain test tubes and allowed clot before centrifugation for 10 min at 4500 g (Hettich Zentrifugen EBA 20). Serum was split into two aliquots: the first was used for routine thyroid, liver, and kidney function tests, and the second was frozen at −80°C for cytokine determination. Stool samples were weighed, dissolved in normal saline, and vortexed. Cleared supernatants were used for fecal NGAL and myeloperoxidase analysis.
Biochemical Analysis
Liver enzymes (aspartate transaminase (AST) and alanine aminotransferase (ALT)) were measured using a spectrophotometric kinetic method. The Jaffé reaction was used to determine serum creatinine levels which reflected kidney function.27 For complete blood count analysis, an automated hematology analyzer was used to analyze 2 mL blood in EDTA tubes.
Using manufacturer’s instructions, commercially available enzyme-linked immunosorbent assay (ELISA) kits were used to quantify serum levels (expressed as pg/ml). IL-8 (catalog no: 201-12-0090), TNF-α (catalog no: 201-12-0083), and IL-6 (catalog no: 201-12-0091) kits were supplied by Sunredio, Shanghai, China.
Stool samples were processed as described, with clear supernatants collected for myeloperoxidase and NGAL analysis using ELISA kits according to manufacturer’s instructions. Fecal NGAL (catalog no: 201-12-1720) and myeloperoxidase (catalog no: 201-12-0081) were supplied by Sunredio. Fecal NGAL was expressed as pg/g stool and fecal myeloperoxidase as ng/g stool.
Statistical Analysis
Statistical analyses were performed in Prism version 6 (GraphPadsoftware, Inc, San Diego, CA, USA). Paired Student’s t-tests were used to determine significant differences between each group before and after therapy. A one-way ANOVA test followed by a post hoc test was used to determine significant differences between groups before and after therapy. Data were presented as the mean and standard deviation. Parameters were correlated using Pearson’s correlation coefficient. The Chi-square test was used on categorical data. All p values were two-tailed, with p < 0.05 considered statistically significant.
Study Outcomes
Primary Outcomes
Decreased NRS scores and abdominal pain relief. The Numeric Rating Scale (NRS-11) is an 11-point scale for patient self-reporting of pain. It is based solely on the ability to perform activities of daily living (ADLs) and can be used for adults and children 10 years old or older.28
Secondary Outcomes
Decreased serum levels and fecal inflammatory biomarkers.
Results
Clinical and Demographic Characteristics
We observed no statistically significant variations between control and intervention groups in terms of baseline demographic data (Table 1).
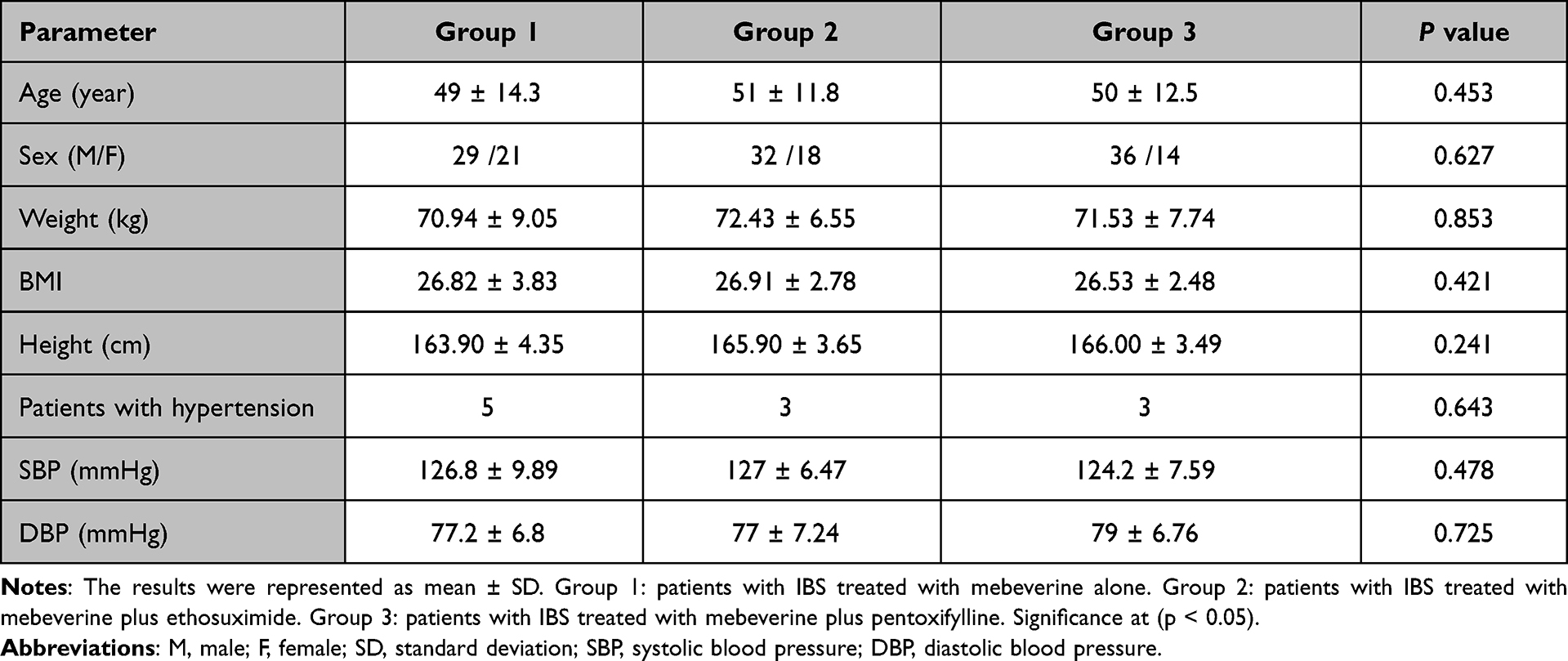 |
Table 1 Clinical and Demographic Data of the Patients |
Baseline Laboratory Data
Using ANOVA, we observed no significant differences between groups for all laboratory data: Hb (p = 0.255), WBCs (p = 0.547), RBCs (p = 0.847), ALT (p = 0.884), AST (p = 0.367), Sr Cr (p = 0.745), T3 (p = 0.583), T4 (p = 0.741), and TSH (p = 0.689) (Table 2).
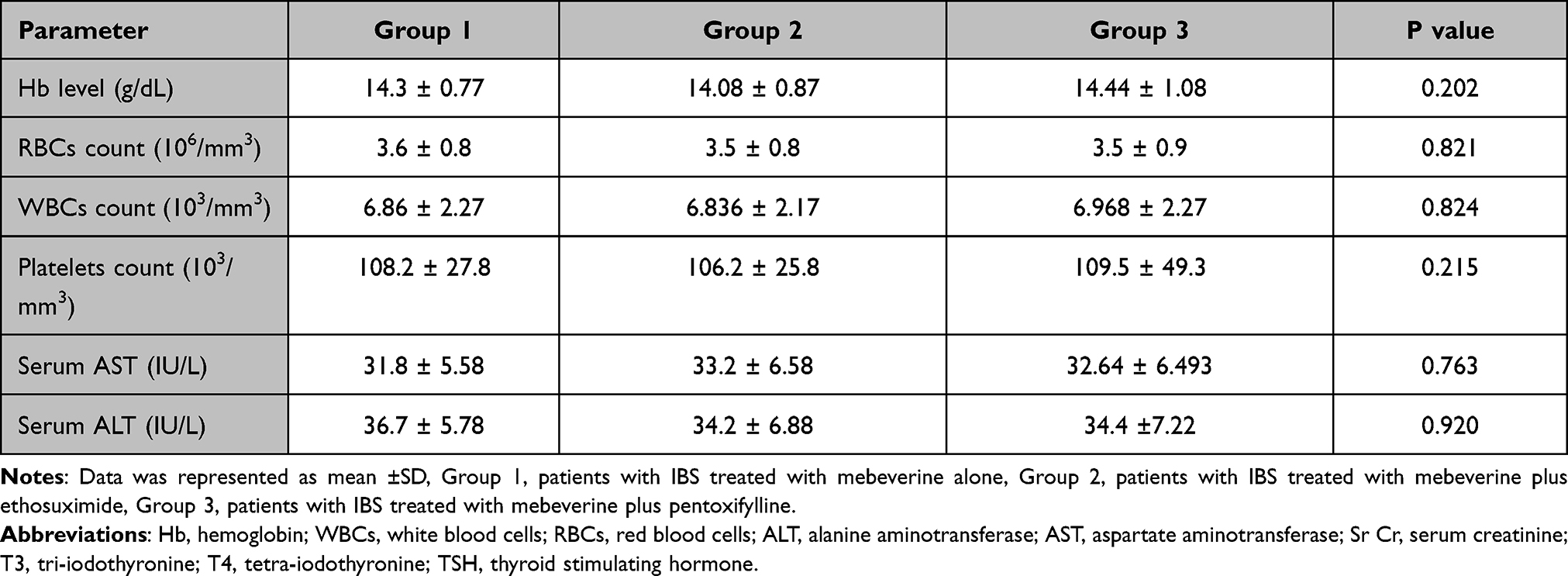 |
Table 2 Baseline Laboratory Data |
The Effect of Ethosuximide and PTX on Serum and Fecal Biomarkers
We observed no significant differences in all biomarkers at therapy commencement (Table 3). After 6 months of treatment, using paired t-tests for all analyses, group 1 showed significantly decreased biomarkers: serum IL-6 (90.9 ± 4.64 vs 37.28 ± 1.02, p = 0.0001), serum IL-8 (280.8 ± 10.02 vs 108.9 ± 3.57, p = 0.0001), serum TNF-α (366.4 ± 13.60 vs 93.33 ± 3.92, p = 0.0001), fecal NGAL (1642 ± 75.06 vs 561 ± 22.13, p = 0.0001), and fecal myeloperoxidase (26.15 ± 0.97 vs 17.47 ± 0.72, p = 0.0001).
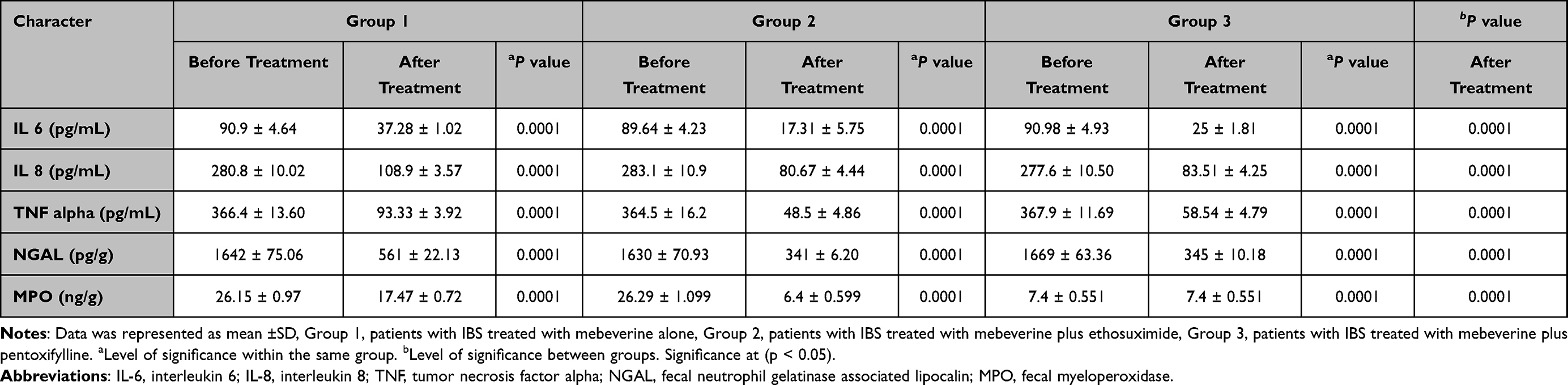 |
Table 3 Effect of Ethosuximide and Pentoxifylline on Serum and Fecal Biomarkers |
After 6 months of treatment, group 2 showed significantly decreased biomarkers: serum IL-6 (89.64 ± 4.23 vs 17.31 ± 5.75, p = 0.0001), serum IL-8 (283.1 ± 10.9 vs 80.67 ± 4.44, p = 0.0001), serum TNF-α (364.5 ± 16.2 vs 48.5 ± 4.86, p = 0.0001), fecal NGAL (1630 ± 70.93 vs 341 ± 6.20, p = 0.0001), and fecal myeloperoxidase (26.29 ± 1.099 vs 6.4 ± 0.599, p = 0.0001).
Group 3 showed statistically significant decreases in all biomarkers after 6 months of therapy: serum IL-6 (90.98 ± 4.93 vs 25 ± 1.81, p = 0.0001), serum IL-8 (277.6 ± 10.50 vs 83.51 ± 4.25, p = 0.0001), serum TNF-α (367.9 ± 11.69 vs 58.54 ± 4.79, p = 0.0001), fecal NGAL (1669 ± 63.36 vs 345 ± 10.18, p = 0.0001), and fecal myeloperoxidase (26.49 ± 0.899 vs 7.4 ± 0.551, p = 0.0001).
ANOVA analyses followed by post hoc tests indicated that groups 2 and 3 showed significant decreases in all biomarkers when compared to group 1 (p < 0.0001).
The Effect of Ethosuximide and PTX on NRS Scores
We observed statistically significant differences between patients before and after treatments (p < 0.0001) (Table 4). After 12 weeks, significant decreases in NRS scores were observed in ethosuximide and PTX groups when compared to the mebeverine group (p < 0.0001).
 |
Table 4 Effect of Ethosuximide and Pentoxifylline on Numeric Pain Rating Scale |
Side Effect Analyses
In terms of side effects, no significant differences were observed between groups (p > 0.05), except for the PTX group which showed significant changes in sexual performance (p < 0.0003) (Table 5).
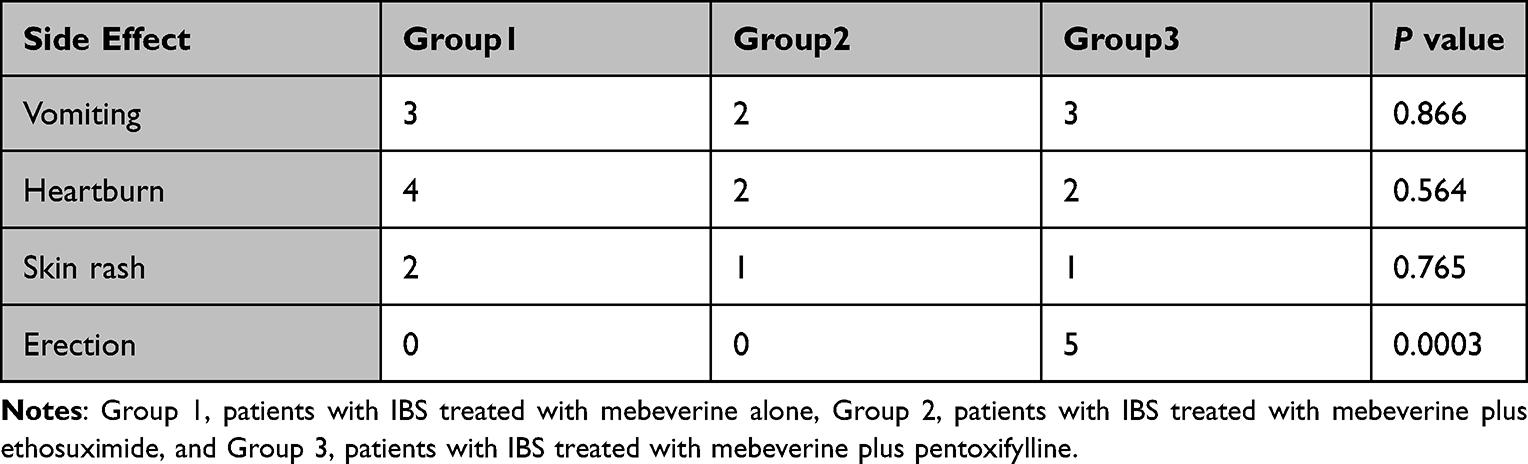 |
Table 5 Analysis of Drug Related Side Effects |
Correlation Analyses Between Parameters
We observed a significant positive correlation between NRS and myeloperoxidase in group 3 (p = 0.04, r = 0.442) and a significant positive correlation between NGAL and NRS in group 2 (p = 0.009, r = 0.554) (Table 6).
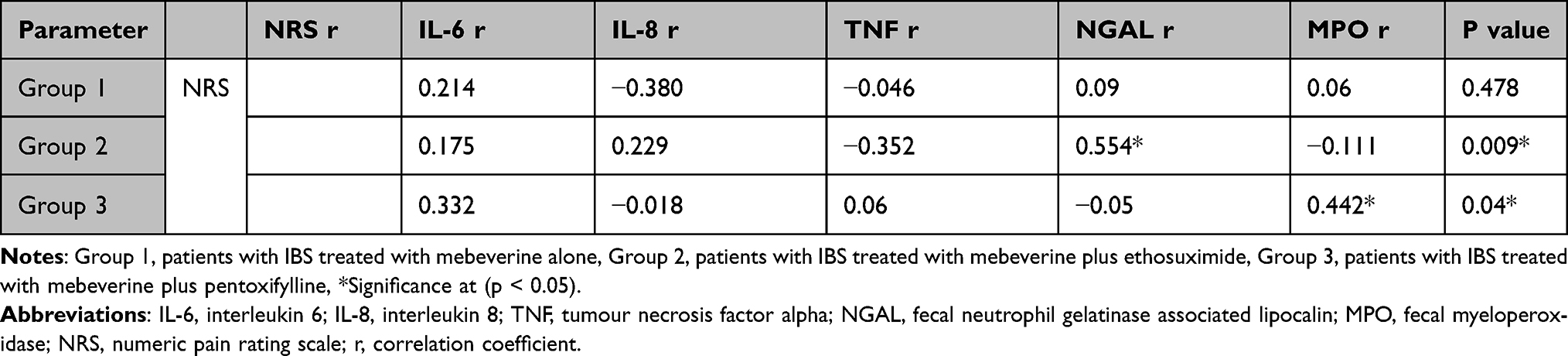 |
Table 6 Correlation Analysis Between the Studied Parameters After Three Months of Therapy |
Discussion
IBS is marked by chronic abdominal discomfort and abnormal bowel patterns, as defined by the Rome IV classification system.29
Most abdominal pain therapies for patients with IBS are largely ineffective, suggesting a fundamental public health concern. To our knowledge, this is the first comparative study to investigate the therapeutic effects of two different drug classes as adjuvant therapy with traditional antispasmodics in the treatment of IBS-related abdominal pain. It is accepted that ethosuximide was used in the treatment of absence attacks,26 but its use in IBS is based on its action as a T-type calcium blocker. In addition, PTX was used here based on its phosphodiesterase inhibitory activity and adenosine 2 receptor activation abilities, leading to elevated cAMP levels.15 The cAMP-mediated stimulation of protein kinase A suppresses NF-κB nuclear translocation which further suppresses inflammatory cytokine transcription.30 PTX also prevents p38 MAPK and ERK activation which helps assemble NADPH oxidases which are implicated in neutrophil oxidative bursts. This transcriptional regulation is largely responsible for the anti-inflammatory and anti-oxidative properties of PTX.30 In neutrophils, the PTX metabolites M1, M4, and M5 suppress superoxide generation by C5 Des Arg and formyl-methionylleucylphenylalanine.31
No significant variations in demographic or clinical characteristics were identified between groups at study commencement, thus, the therapeutic benefits were mainly attributed to the study drugs.
We observed a statistically significant decrease in IL-6, IL-8, TNF-α, NGAL, and myeloperoxidase levels in the mebeverine group when compared with baseline values. Undoubtedly, these effects were due to mebeverine, as this drug has been used for several years to treat spasms and abdominal pain in patients with IBS.24
Our data showed that group 2 (ethosuximide) and group 3 (PTX) produced a statistically significant reduction in serum IL-6 levels when compared to group 1 (mebeverine) at base line. Treatment with PTX and its metabolite, M1 significantly reduced colon damage and inflammation in colitis, a low-grade mucosal inflammation model, and resulted in decreased serum cytokines.32 In IBS animal models, ethosuximide significantly decreased both serum and colonic IL-6 levels.1 Thus, our data agreed with several studies.33,34
NGAL is highly induced in intestinal epithelia, with most NGAL secreted apically (ie luminally). Therefore, fecal NGAL serves as a noninvasive indicator of intestinal inflammation.35 Picard et al reported a significant increase in fecal NGAL during IBS, but levels were reduced upon ethosuximide supplementation in an IBS model.1 PTX administration to rats decreased NGAL levels and was highly effective in reducing nitrogen mustard-induced oxidative stress.36 Our findings were consistent with previous studies showing that PTX reduced oxidative stress and mucosal inflammation.37
We also observed a statistically significant decrease in IL-8 serum levels in ethosuximide and PTX groups when compared to the mebeverine group. Such increased IL-8 levels in IBS patients in our study agreed with several other studies.38–40 Also, several animal models also reported the effects of PTX on gut inflammation severity.41 PTX also reduced platelet aggregation and inhibited neutrophil activation, thereby improving microcirculatory blood flow in digestive system organs and increasing tissue oxygenation.42 These observations strongly suggested that the beneficial effects of PTX in IBS are, at least in part, related to improved microcirculatory blood flow in the gastrointestinal tract.
Decreased TNF-α serum levels in PTX and ethosuximide groups were supported by several studies.41–46 Combined PTX and TNF-α monoclonal antibody therapy in a dextran sulfate-induced mouse colitis model significantly reduced serum TNF-α levels when compared with TNF-α monoclonal antibody alone.47 Under stress conditions, the hypothalamic-pituitary-adrenal axis and the sympathetic nervous system become activated. This latter activation (sympathetic nervous system) was shown to redistribute cardiac output and significantly reduce blood flow through the digestive system, and also cause localized ischemia. However, earlier studies showed that reduced blood flow through the stomach and localized hypoxia increased susceptibility of the gastric mucosa to damaging factors, leading to mucosal lesion development.48 Moreover, gastric injury was associated with reduced mucosal blood flow, whereas gastric mucosa protection and healing were both associated with increased gastric blood flow.49
We observed a statistically significant decrease in fecal myeloperoxidase when groups 2 (ethosuximide) and 3 (PTX) were compared with group 1 (mebeverine), and at baseline. During degranulation, myeloperoxidase, which is a lysosomal protein, is released into neutrophil phagosomes. Here, hypochlorous acid is formed when myeloperoxidase interacts with hydrogen peroxide and a halide, or tyrosyl radicals when it combines with tyrosine. These substances are highly toxic and are secreted from cells to kill alien microbes. Similarly, these substances may also damage normal tissue leading to inflammation.50 Myeloperoxidase is often highly expressed under different inflammatory conditions, including irritable bowel disease (IBD) and IBS.51 Consequently, myeloperoxidase serves as a noninvasive fecal or colonic biomarker determining IBD and IBS status.52 Our study data were supported by and compatible with several mucosal inflammation studies.53,54 Picard et al showed that colonic myeloperoxidase was overexpressed in IBS animal models, caused mucosal inflammation, with levels reduced after ethosuximide treatment.1 PTX reduced myeloperoxidase accumulation and restored superoxide dismutase activity.41
We also identified a significant reduction in NRS scores in both ethosuximide and PTX groups when compared with the mebeverine group, in agreement with a previous clinical study.46 We also identified a significant positive correlation between NRS scores and myeloperoxidase levels in group 3, which reflected the PTX mechanism of action as an anti-inflammatory agent and cytokine release inhibitor,41,55 however, a correlation does not mean causality. A significant positive correlation was also identified between NGAL and NRS scores in group 2, and possibly reflected the role of ethosuximide in decreasing inflammatory cytokine levels in agreement with previous research.2
Furthermore, the PTX group showed increased erection rates and enhanced sexual performance. Kumar et al reported that PTX administration in combination with tadalafil increased erection rates in patients with erectile dysfunction.56 Thus, our data agreed and correlated with previous studies.57,58
Conclusions
Previous data suggests that VH leads to the overexpression of T-type calcium channels and low-grade mucosal inflammation, therefore, IL-8, TNF-α, IL-6, fecal myeloperoxidase, and fecal NGAL could be effective clinical biomarkers for understanding the effects of PTX and ethosuximide in relieving abdominal pain in patients with IBS treated with mebeverine.
Both ethosuximide and PTX should be considered promising adjuvant therapies in relieving abdominal pain related to IBS as they decreased mucosal inflammation and VH by reducing IL-6, IL-8, TNF-α, fecal myeloperoxidase, and fecal NGAL levels.
Despite study limitations (short follow-up period, small sample size, and a lack of varied doses), we recommend conducting larger scale randomized clinical studies, with larger sample sizes, and longer periods to confirm our findings.
VH or the balloon distention test, like other forms of endoscopy, require intravenous sedation in a hospital or outpatient surgical facility. This test should be performed in future studies. We cannot perform this test due to poor patient compliance; it is invasive and many Egyptian patients refuse it.
Data Sharing Statement
All materials and data are transparent and available upon reasonable request from authors, as are the assertions that they support, and they are matched to field standards for transparency. All individual demographic, clinical, serum and fecal data are available at any time from the corresponding author.
Ethical Approval
The study was approved by the National Research Ethics Committee (Tanta University Ethical Committee, approval code 33422/10/19). The study complied with the ethical criteria of the Helsinki Declaration and later amendments in 1964.
Ethical Consent
All study participants provided written informed consent. Because no private data were used, consent for publication was not required.
Acknowledgments
The authors thank the research center at AlMaarefa University for funding this work. The authors also thank the physicians at the Tanta University Hospital, Gastrointestinal Department for enabling patients to participate in this research and the Faculty of Pharmacy for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Picard E, Carvalho FA, Agosti F, et al. Inhibition of Cav3. 2 calcium channels: a new target for colonic hypersensitivity associated with low‐grade inflammation. Br J Pharmacol. 2019;176(7):950–963. doi:10.1111/bph.14608
2. Kerckhove N, Scanzi J, Pereira B, et al. Assessment of the effectiveness and safety of ethosuximide in the treatment of abdominal pain related to irritable bowel syndrome–IBSET: protocol of a randomised, parallel, controlled, double-blind and multicentre trial. BMJ Open. 2017;7(7):e015380. doi:10.1136/bmjopen-2016-015380
3. Cervero F, Laird JM. Role of ion channels in mechanisms controlling gastrointestinal pain pathways. Curr Opin Pharmacol. 2003;3(6):608–612. doi:10.1016/j.coph.2003.06.007
4. Wood JD. Neuropathy in the brain-in-the-gut. Eur J Gastroenterol Hepatol. 2000;12(6):597–600. doi:10.1097/00042737-200012060-00002
5. Scanzi J, Accarie A, Muller E, et al. Colonic overexpression of the T‐type calcium channel Cav3. 2 in a mouse model of visceral hypersensitivity and in irritable bowel syndrome patients. Neurogastroenterol Motil. 2016;28(11):1632–1640. doi:10.1111/nmo.12860
6. Ng QX, Soh AY, Loke W, et al. The role of inflammation in irritable bowel syndrome (IBS). J Inflamm Res. 2018;11:345. doi:10.2147/JIR.S174982
7. Seyedmirzaee S, Hayatbakhsh MM, Ahmadi B, et al. Serum immune biomarkers in irritable bowel syndrome. Clin Res Hepatol Gastroenterol. 2016;40(5):631–637. doi:10.1016/j.clinre.2015.12.013
8. Lee JY, Kim N, Park JH, et al. Expression of neurotrophic factors, tight junction proteins, and cytokines according to the irritable bowel syndrome subtype and sex. J Neurogastroenterol Motil. 2020;26(1):106. doi:10.5056/jnm19099
9. Zhen Y, Chu C, Zhou S, Qi M, Shu R. Imbalance of tumor necrosis factor-α, interleukin-8 and interleukin-10 production evokes barrier dysfunction, severe abdominal symptoms and psychological disorders in patients with irritable bowel syndrome-associated diarrhea. Mol Med Report. 2015;12(4):5239–5245. doi:10.3892/mmr.2015.4079
10. Farajollahi-Moghadam M, Sanjari-Moghaddam H, Hasemi MG, Sanatian Z, Talaei A, Akhondzadeh S. Efficacy and safety of pentoxifylline combination therapy in major depressive disorder: a randomized, double-blind, placebo-controlled clinical trial. Int Clin Psychopharmacol. 2021;36(3):140–146. doi:10.1097/YIC.0000000000000353
11. Rai RR, Nijhawan S. Comparative evaluation of efficacy and safety of drotaverine versus mebeverine in irritable bowel syndrome: a randomized double-blind controlled study. Saudi J Gastroenterol. 2021;27(3):136. doi:10.4103/sjg.SJG_266_20
12. Sekiguchi F, Kawabata A. T-type calcium channels: functional regulation and implication in pain signaling. J Pharmacol Sci. 2013;122(4):244–250. doi:10.1254/jphs.13R05CP
13. Marger F, Gelot A, Alloui A, et al. T-type calcium channels contribute to colonic hypersensitivity in a rat model of irritable bowel syndrome. Proc Natl Acad Sci. 2011;108(27):11268–11273. doi:10.1073/pnas.1100869108
14. Hamburg NM, Creager MA. Pathophysiology of intermittent claudication in peripheral artery disease. Circ J. 2017;81:281–289.
15. McCarty MF, O’Keefe JH, Dinicolantonio JJ. Pentoxifylline for vascular health: a brief review of the literature. Open Heart. 2016;3(1):e000365. doi:10.1136/openhrt-2015-000365
16. Kumar R, Prakash S, Chhabra S, et al. Association of pro-inflammatory cytokines, adipokines & oxidative stress with insulin resistance & non-alcoholic fatty liver disease. Indian J Med Res. 2012;136(2):229.
17. Okunieff P, Augustine E, Hicks JE, et al. Pentoxifylline in the treatment of radiation-induced fibrosis. J Clin Oncol. 2004;22(11):2207–2213. doi:10.1200/JCO.2004.09.101
18. Agharazii M, St-Louis R, Gautier-Bastien A, et al. Inflammatory cytokines and reactive oxygen species as mediators of chronic kidney disease-related vascular calcification. Am J Hypertens. 2015;28(6):746–755. doi:10.1093/ajh/hpu225
19. Leporini C, Pisano A, Russo E, de Sarro G, Coppolino G, Bolignano D. Effect of pentoxifylline on renal outcomes in chronic kidney disease patients: a systematic review and meta-analysis. Pharmacol Res. 2016;107:315–332. doi:10.1016/j.phrs.2016.03.001
20. Talley NJ, Kellow JE, Boyce P, Tennant C, Huskic S, Jones M. Antidepressant therapy (imipramine and citalopram) for irritable bowel syndrome: a double-blind, randomized, placebo-controlled trial. Dig Dis Sci. 2008;53(1):108–115.
21. Peled A, Wald O, Burger J. Burger, development of novel CXCR4-based therapeutics. Expert Opin Investig Drugs. 2012;21(3):341–353. doi:10.1517/13543784.2012.656197
22. Reme SE, Stahl D, Kennedy T, Jones R, Darnley S, Chalder T. Mediators of change in cognitive behaviour therapy and mebeverine for irritable bowel syndrome. Psychol Med. 2011;41(12):2669–2679. doi:10.1017/S0033291711000328
23. El‑Haggar SM, Hegazy SK, Abd-Elsalam SM, Bahaa MM. “Pentoxifylline, a nonselective phosphodiesterase inhibitor, in adjunctive therapy in patients with irritable bowel syndrome treated with mebeverine.”. Biomed Pharmacother. 2022;145:112399. doi:10.1016/j.biopha.2021.112399
24. Talley NJ. Drug therapy options for patients with irritable bowel syndrome. Am J Manag Care. 2001;7(8 Suppl):S261–S267.
25. Ward A, Clissold SP. Pentoxifylline. Drugs. 1987;34(1):50–97. doi:10.2165/00003495-198734010-00003
26. Buchanan RA, Kinkel AW, Turner JL, et al. Ethosuximide dosage regimens. Clin Pharmacol Ther. 1976;19(2):143–147. doi:10.1002/cpt1976192143
27. Husdan H, Rapoport A. Estimation of creatinine by the Jaffe reaction: a comparison of three methods. Clin Chem. 1968;14(3):222–238. doi:10.1093/clinchem/14.3.222
28. Kahl C, Cleland JA. Visual analogue scale, numeric pain rating scale and the McGill pain questionnaire: an overview of psychometric properties. Phys Ther Rev. 2005;10(2):123–128. doi:10.1179/108331905X55776
29. Mearin F, Ciriza C, Mínguez M, et al. Clinical Practice guideline: irritable bowel syndrome with constipation and functional constipation in the adult. Rev Esp Enferm Dig. 2016;108(6):332–363. doi:10.17235/reed.2016.4389/2016
30. Donate-Correa J, Tagua VG, Ferri C, et al. Pentoxifylline for renal protection in diabetic kidney disease. A model of old drugs for new horizons. J Clin Med. 2019;8(3):287. doi:10.3390/jcm8030287
31. Chen YM, Chiang W-C, Lin S-L, et al. Therapeutic efficacy of pentoxifylline on proteinuria and renal progression: an update. J Biomed Sci. 2017;24(1):1–15. doi:10.1186/s12929-017-0390-4
32. Wen WX, Lee SY, Siang R, Koh RY. Repurposing pentoxifylline for the treatment of fibrosis: an overview. Adv Ther. 2017;34(6):1245–1269. doi:10.1007/s12325-017-0547-2
33. Peterson TC, Peterson MR, Raoul JM. The effect of pentoxifylline and its metabolite-1 on inflammation and fibrosis in the TNBS model of colitis. Eur J Pharmacol. 2011;662(1–3):47–54. doi:10.1016/j.ejphar.2011.04.030
34. Bashashati M, Moradi M, Sarosiek I. Interleukin-6 in irritable bowel syndrome: a systematic review and meta-analysis of IL-6 (-G174C) and circulating IL-6 levels. Cytokine. 2017;99:132–138. doi:10.1016/j.cyto.2017.08.017
35. Jonefjäll B, Öhman L, Simrén M, Strid H. IBS-like symptoms in patients with ulcerative colitis in deep remission are associated with increased levels of serum cytokines and poor psychological well-being. Inflamm Bowel Dis. 2016;22(11):2630–2640. doi:10.1097/MIB.0000000000000921
36. Chassaing B, Srinivasan G, Delgado MA, Young AN, Gewirtz AT, Vijay-Kumar M. Fecal lipocalin 2, a sensitive and broadly dynamic non-invasive biomarker for intestinal inflammation. PLoS One. 2012;7(9):e44328. doi:10.1371/journal.pone.0044328
37. Sunil VR, Vayas KN, Cervelli JA, et al. Pentoxifylline attenuates nitrogen mustard-induced acute lung injury, oxidative stress and inflammation. Exp Mol Pathol. 2014;97(1):89–98. doi:10.1016/j.yexmp.2014.05.009
38. Al-Gholam MA, Mansour FK, Abdel-Fattah NA, Nooh HZ. Effect of pentoxifylline on experimental-dextran sulphate sodium-induced colitis in rats. J Adv Med Med Res. 2014;4(10):2037–2057. doi:10.9734/BJMMR/2014/5108
39. Vara EJ, Brokstad KA, Hausken T, Lied GA. Altered levels of cytokines in patients with irritable bowel syndrome are not correlated with fatigue. Int J Gen Med. 2018;11:285. doi:10.2147/IJGM.S166600
40. Caviglia GP, Tucci A, Pellicano R, et al. “Clinical response and changes of cytokines and zonulin levels in patients with diarrhoea-predominant irritable bowel syndrome treated with bifidobacterium longum ES1 for 8 or 12 weeks: a preliminary report.”. J Clin Med. 2020;9(8):2353. doi:10.3390/jcm9082353
41. Hustoft TN, Hausken T, Ystad SO, et al. Effects of varying dietary content of fermentable short‐chain carbohydrates on symptoms, fecal microenvironment, and cytokine profiles in patients with irritable bowel syndrome. Neurogastroenterol Motil. 2017;29(4):e12969. doi:10.1111/nmo.12969
42. Karatay E, Utku Ö, Erdal H, et al. Pentoxifylline attenuates mucosal damage in an experimental model of rat colitis by modulating tissue biomarkers of inflammation, oxidative stress, and fibrosis. Turk J Med Sci. 2017;47(1):348–356. doi:10.3906/sag-1508-98
43. González-Pacheco H, Amezcua-Guerra LM, Sandoval J, Arias-Mendoza A. Potential usefulness of pentoxifylline, a non-specific phosphodiesterase inhibitor with anti-inflammatory, anti-thrombotic, antioxidant, and anti-fibrogenic properties, in the treatment of SARS-CoV-2. Eur Rev Med Pharmacol Sci. 2020;24(14):7612–7614. doi:10.26355/eurrev_202007_22259
44. Berg LK, Goll R, Fagerli E, et al. Intestinal inflammatory profile shows increase in a diversity of biomarkers in irritable bowel syndrome. Scand J Gastroenterol. 2020;55(5):537–542. doi:10.1080/00365521.2020.1754455
45. Norlin AK, Walter S, Icenhour A, et al. Fatigue in irritable bowel syndrome is associated with plasma levels of TNF-α and mesocorticolimbic connectivity. Brain Behav Immun. 2021;92:211–222. doi:10.1016/j.bbi.2020.11.035
46. El‑Haggar SM, Hegazy SKM, Abd‐Elsalam S, Bahaa MM. “Open‐label pilot study of ethosuximide as adjunctive therapy for relieving abdominal pain related to irritable bowel syndrome”. J Clin Pharm Ther. 2021. doi:10.1111/jcpt.13556
47. Li B, Rui J, Ding X, Yang X. Exploring the multicomponent synergy mechanism of Banxia Xiexin decoction on irritable bowel syndrome by a systems pharmacology strategy. J Ethnopharmacol. 2019;233:158–168. doi:10.1016/j.jep.2018.12.033
48. Murthy S, Cooper HS, Yoshitake H, Meyer C, Meyer CJ, Murthy NS. Combination therapy of pentoxifylline and TNFalpha monoclonal antibody in dextran sulphate-induced mouse colitis. Aliment Pharmacol Ther. 1999;13(2):251–260.
49. Sørbye H, Svanes K. The role of blood flow in gastric mucosal defence, damage and healing. Dig Dis. 1994;12(5):305–317. doi:10.1159/000171465
50. Warzecha Z, Dembiński A, Brzozowski T, et al. Histamine in stress ulcer prophylaxis in rats. J Physiol Pharmacol. 2001;52(3):407–421.
51. Klebanoff SJ. Myeloperoxidase: friend and foe. J Leukoc Biol. 2005;77(5):598–625. doi:10.1189/jlb.1204697
52. Lau D, Baldus S. Myeloperoxidase and its contributory role in inflammatory vascular disease. Pharmacol Ther. 2006;111(1):16–26. doi:10.1016/j.pharmthera.2005.06.023
53. Pattison DI, Davies MJ. Reactions of myeloperoxidase-derived oxidants with biological substrates: gaining chemical insight into human inflammatory diseases. Curr Med Chem. 2006;13(27):3271–3290. doi:10.2174/092986706778773095
54. Hansberry DR, Shah K, Agarwal P, Agarwal N. Fecal myeloperoxidase as a biomarker for inflammatory bowel disease. Cureus. 2017;9(1):e1004. doi:10.7759/cureus.1004
55. Majeed M, Nagabhushanam K, Arumugam S, Majeed S, Ali F. Bacillus coagulans MTCC 5856 for the management of major depression with irritable bowel syndrome: a randomised, double-blind, placebo controlled, multi-centre, pilot clinical study. Food Nutr Res. 2018;62. doi:10.29219/fnr.v62.1218
56. Li H, Tan G, Tong L, et al. Pentoxifylline inhibits pulmonary inflammation induced by infrarenal aorticcross-clamping dependent of adenosine receptor A2A. Am J Transl Res. 2016;8(5):2210.
57. Kumar S, Roat R, Agrawal S, Jayant K, Mavuduru RS, Kumar S. Combination therapy of tadalafil and pentoxifylline in severe erectile dysfunction; A prospective randomized trial. Pol J Surg. 2015;87(8):377–383. doi:10.1515/pjs-2015-0075
58. Law YX, Tai BC, Tan YQ, Lata RN, Lee KC. A small group randomized double-blind placebo-controlled study to evaluate the efficacy of daily pentoxifylline in the management of patients with erectile dysfunction with suboptimal treatment response to sildenafil. Sex Med. 2020;8(1):14–20. doi:10.1016/j.esxm.2019.08.012
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.