")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
A Post Hoc Holter ECG Analysis of Olodaterol and Formoterol in Moderate-to-Very-Severe COPD
Authors Andreas S , Bothner U, de la Hoz A, Kloer I, Trampisch M, Alter P
Received 17 January 2020
Accepted for publication 15 July 2020
Published 10 August 2020 Volume 2020:15 Pages 1955—1965
DOI https://doi.org/10.2147/COPD.S246353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Stefan Andreas,1,2 Ulrich Bothner,3 Alberto de la Hoz,3 Isabel Kloer,3 Matthias Trampisch,3 Peter Alter4
1Department of Cardiology and Pneumology, University Medical Center Göttingen, Göttingen, Germany; 2LungClinic Immenhausen, Immenhausen, Germany, Member of the German Center for Lung Research (DZL); 3Boehringer Ingelheim International GmbH, Ingelheim am Rhein, Germany; 4Department of Medicine, Pulmonary and Critical Care Medicine, Philipps University of Marburg (UMR), Member of the German Center for Lung Research (DZL), Marburg, Germany
Correspondence: Stefan Andreas Department of Cardiology and Pneumology
University Medical Center Göttingen, Robert-Koch-Str. 40, Göttingen, Germany
Tel +49 05673 501 1112
Fax +49 05673-501-1101
Email [email protected]
Background: Patients with chronic obstructive pulmonary disease (COPD) are at risk of developing cardiac arrhythmias and elevated heart rate. A theoretical mechanistic association based on the interaction of long-acting β2-agonists (LABAs) with adrenoreceptors in the heart and vasculature is assumed as a potential class-related risk. Therefore, we performed a pooled analysis of Holter electrocardiogram (ECG) data from four 48-week, randomized, double-blind, placebo-controlled, parallel-group, Phase III clinical trials evaluating olodaterol (5 μg or 10 μg) or formoterol (12 μg) versus placebo.
Methods: We analyzed Holter ECG data from a representative subset of 775 patients with Global Initiative for Chronic Obstructive Lung Disease stage 2– 4 COPD from four studies (1222.11– 14) assessing olodaterol (5 μg and 10 μg) and formoterol (12 μg) versus placebo.
Results: No statistically significant (P> 0.3) or clinically relevant differences in the shift from baseline of premature supraventricular or ventricular beats were observed among the active treatment and the placebo groups. Minor and transient differences were observed in the adjusted mean heart rate from baseline during treatment in all groups. There was a numerically small but statistically significant increase for formoterol at Week 24, olodaterol 5 μg at Weeks 12 and 40, and olodaterol 10 μg at Week 40 (all less than 3.0 beats per minute). Mean heart rates returned to a statistically non-significant change at Week 48 for all treatment groups. No increase in major adverse cardiovascular events was observed.
Conclusion: Treatment with olodaterol or formoterol is not associated with arrhythmias or a persistent increase in heart rate as assessed by Holter ECG in patients with COPD.
Trial Registration: ClinicalTrials.gov identifiers: NCT00782210 (1222.11); NCT00782509 (1222.12); NCT00793624 (1222.13); NCT00796653 (1222.14).
Keywords: olodaterol, formoterol, arrhythmia, Holter ECG, heart rate
Plain Language Summary
The present study aimed to explore whether two drugs (olodaterol and formoterol) commonly used for the treatment of chronic obstructive pulmonary disease (COPD) are associated with irregular heartbeats (arrhythmias) or changes in heart rate. This consideration is based on the fact that these drugs belong to a class called long-acting β2-agonists (LABAs). These drugs have the potential to affect heart rhythm in individuals with COPD, which could be detrimental to their health. To better understand this, the heart rhythm of a group of patients taking olodaterol and formoterol in four clinical trials was monitored at pre-specified time points during the study using a 24-hour wearable Holter electrocardiogram recorder. Combined data from these studies show that treatment with olodaterol and formoterol did not cause adverse changes in heart rhythm. Small, temporary increases in heart rate were seen with both drugs, but these were not persistent at the end of the 48-week observation period. Therefore, we conclude that treatment with olodaterol or formoterol is not associated with arrhythmias or persistent increases in heart rate.
Background
Chronic obstructive pulmonary disease (COPD) is associated with cardiovascular (CV) comorbidities, hospitalization and death.1,2 These comorbidities include thromboembolic disorders, myocardial ischemia and infarction, or stroke with a substantially higher prevalence in patients with COPD compared with healthy individuals.1,3-5 Other concerns for COPD patients include increased resting heart rate and cardiac arrhythmias (supraventricular and ventricular arrhythmias, and atrial fibrillation), which are risk markers for heart disease and impaired prognosis.6–9 Given this background, the safety of long-acting β2-agonists (LABAs) in this setting should be evaluated. As a drug class, LABAs have the potential to affect cardiac characteristics such as heart rate and rhythm disturbances.10,11 These effects are potentially mediated by stimulation of β2-adrenoreceptors (ARs) in the atria, ventricles and peripheral vasculature and are opposite to those of β-blockers used to treat cardiac arrhythmias.10,12-14 Indeed, in the human heart, β1 and β2-ARs coexist in both atria and in both ventricles with a β1/β2 ratio of approximately 65/35% in the atria and 75/25% in the ventricles.9
Olodaterol is a more recently developed, once-daily LABA designed with the aim of improving β2-AR selectivity and intrinsic activity.15 It is structurally distinct from formoterol and salmeterol. All β-agonist compounds are racemates, with the (R)-enantiomer being the active component and the (S)-enantiomer being inactive at therapeutic concentrations.15–17 In vitro studies suggest that the (S)-enantiomer may induce tachyphylaxis or receptor desensitization.15 Thus, pure (R,R)-β-agonists like olodaterol provide bronchodilation at lower doses than the racemate, potentially allowing for fewer β2-AR-mediated side effects.15
Although a previous analysis showed that long-term administration of olodaterol or formoterol does not adversely influence heart rate or blood pressure in patients with moderate-to-severe COPD,13 there is a lack of data on long-term effects of LABAs on heart rhythm. To address this and test the hypothesis that a greater selectivity of olodaterol may translate into lower cardiac side effects, we conducted an extensive analysis of Holter electrocardiogram (ECG) data collected from subsets of patients taking part in four 48-week, randomized, double-blind, placebo-controlled, parallel-group, Phase III trials assessing olodaterol 5 µg or 10 µg, or formoterol 12 µg, versus placebo in patients with Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage 2–4 (ie moderate-to-very-severe) COPD. Here, we report the findings from a pooled analysis of studies 1222.11–14.
Methods
Study Design
Studies 1222.11 and 1222.12 were 48-week, randomized, double-blind, placebo-controlled, parallel-group, Phase III replicate trials. Detailed study methods have been published previously.18 Overall, 1,266 patients with moderate-to-very-severe COPD (GOLD stage 2–4) were treated with olodaterol 5 μg, olodaterol 10 μg or placebo delivered once daily via Respimat® Soft Mist™ inhaler (SMI).18 The co-primary efficacy endpoints were forced expiratory volume in 1 second (FEV1) area under the curve 3 hours post-dose (AUC0–3) response (change from baseline) and trough FEV1 response (measured as pre-dose FEV1) at 12 weeks.18
Studies 1222.13 and 1222.14 were 48-week, randomized, double-blind, placebo-controlled, parallel-group, Phase III trials. Detailed study methods have been published previously.19 Overall, 1,838 patients with moderate-to-very-severe COPD (GOLD stage 2–4) were treated with olodaterol (5 or 10 μg) once daily (via SMI), 12 μg formoterol twice daily (via Aerolizer® dry powder inhaler [DPI]) or placebo (SMI/DPI, double-dummy).19 The co-primary efficacy endpoints were FEV1 AUC0–3 response, trough FEV1 response and Mahler transition dyspnea index after 24 weeks of treatment.19
All of the four studies, except for the additional comparison with formoterol in studies 1222.13 and 1222.14, had an identical design, thereby enabling complete pooling of the safety data.
Inclusion and exclusion criteria were also the same for the four studies. Patients with COPD aged ≥40 with a smoking history of >10 pack-years and a post-bronchodilator FEV1 of <80% predicted were included. Patients were excluded if they had a significant disease other than COPD, a history of asthma, of myocardial infarction within 1 year of screening, unstable or life-threatening cardiac arrhythmia, life-threatening pulmonary obstruction, if they regularly used daytime oxygen therapy or were currently in, or had recently completed, a pulmonary rehabilitation program.
Sub-Analyses on Holter ECGs
In each study, 24-hour Holter monitoring was performed in a subset of patients at selected sites who were capable of and trained to handle centralized Holter ECG monitoring. All patients at selected sites were invited to participate in this sub-study. Holter monitoring was performed in patients giving informed consent to participate in the sub-study and capable of carrying and returning the equipment after 24 hours. Two hundred patients (50 patients per treatment group) participated in studies 1222.11/12/13 and 175 patients in study 1222.14. Sites were provided with standard equipment by the sponsor (12-Lead Mortara H12+ Digital Holter Recorder, eResearchTechnology, Inc, Philadelphia, USA). Holter ECG recordings were transferred to the central vendor (eResearchTechnology, Inc) for review by a cardiologist before data upload to the study database. Holter monitoring was to be performed in a subset of up to 800 patients prior to randomization at Visit 2 (baseline), and during randomized treatment at Visit 5 (Day 85, Week 12), Visit 7 (Day 169, Week 24), Visit 9 (Day 281, Week 40) and Visit 10 (Day 337, Week 48).
Statistical Analysis
The 24-hour Holter ECG records were evaluated for mean heart rate, as well as the number of supraventricular premature beats (SVPBs) and ventricular premature beats (VPBs) in a pre-specified analysis. Increase or decrease in SVPBs and VPBs from baseline on treatment was established using two-way shift tables. Shifts were defined based on predefined cut-offs with the following categories: <10, ≥10 to <30, ≥30 to <50, ≥50 to <100, ≥100 to <500, ≥500 to <1000, ≥1000 to <2000 and ≥2000 premature beats in 24 hours. The number of individuals who moved from one category to another (increase, decrease or no change) was then calculated. Categories assigned at baseline and at Weeks 12, 24, 40 and 48 were compared to give shifts in SVPBs and VPBs. The shift proportions were tested for significant differences between treatments and differences in the frequency of shifts (increase, decrease or unchanged from baseline) were evaluated between treatments using Chi-squared testing. Additional data were collected across all studies on the heart rates measured by the Holter ECGs. Adjusted mean changes from baseline and treatment differences for the 24-hour Holter ECG mean heart rates were analyzed using a mixed-effect model repeat measurement with fixed effects for treatment, visit, treatment-by-visit interaction, baseline and baseline-by-visit interaction. Patient is considered a random variable and an unstructured covariance structure was used. P<0.05 was considered a significant difference for all post hoc statistical analyses at an alpha level of 0.05.
Results
Baseline Demographics
In total, 775 patients were included in Holter ECG monitoring subsets. The patient characteristics of all studies have been described previously.18,19 Baseline demographics for the subset of patients included in the Holter ECG examinations are displayed in Table 1 and were generally representative of the whole study populations.20 The subset consisted of 68.4% males, with a mean age of 63.1 years. When classified by GOLD, the majority of patients were GOLD stage 2 (52.3%) or GOLD stage 3 (39.5%), with 7.9% classified as GOLD stage 4. At baseline, 13.6% of patients had documented pre-existing conditions of cardiac arrhythmia and 14.5% of patients had ischemic heart disease. With regard to CV risk, the Holter subset was representative of the full study population20 in relation to their CV medication presented at baseline. However, the Holter subset had a slightly higher incidence of cardiac arrhythmia compared with the full study population (Supplementary Table 1). Overall, the treatment groups were well balanced; however, a lower percentage of patients (48.8%) in the formoterol 12 μg group were affected by CV disease at baseline compared with the other treatment groups (62.8% for the olodaterol 10 μg group, 62.6% for the olodaterol 5 μg group and 57.1% for the placebo group; Table 1).
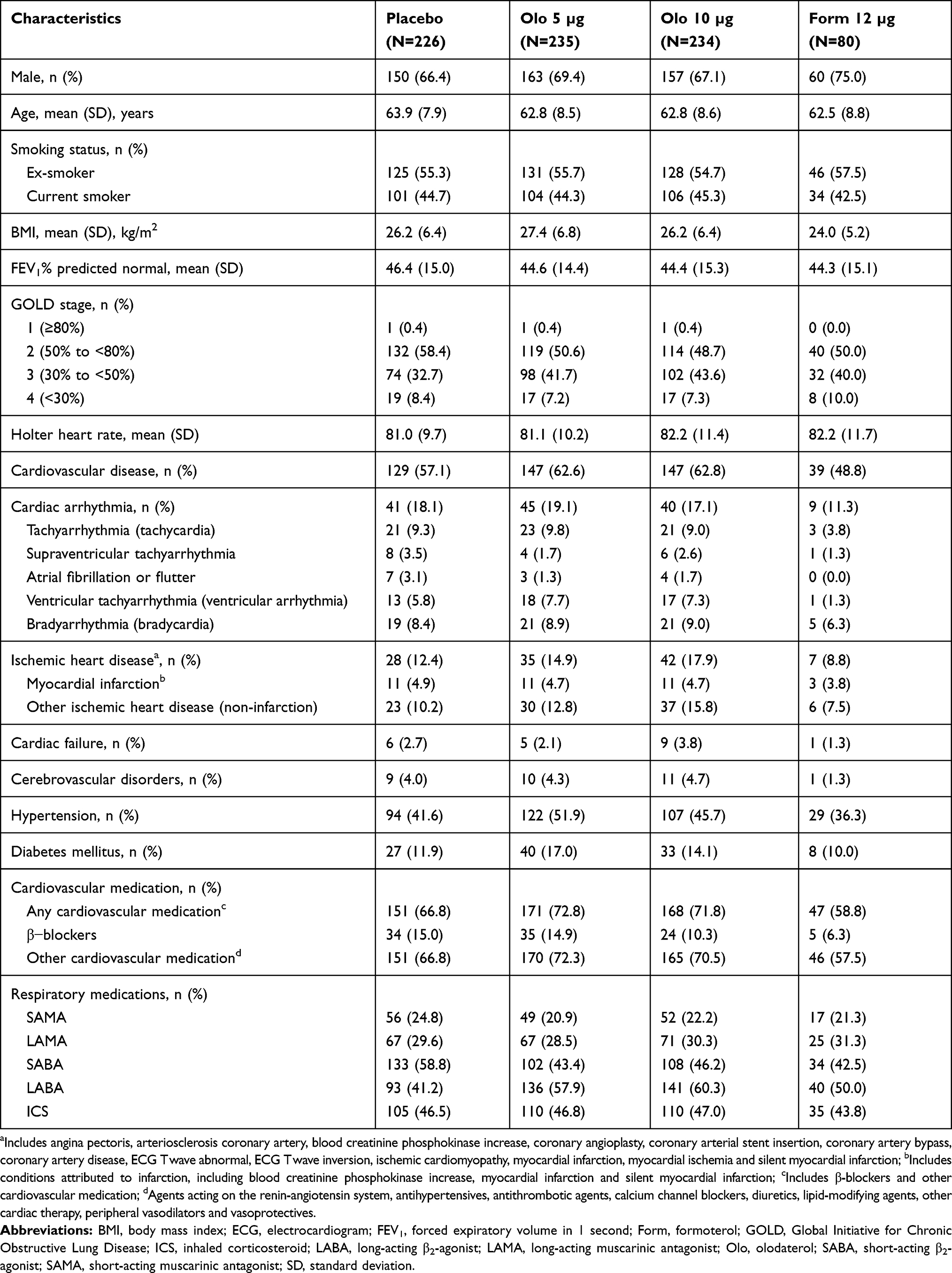 |
Table 1 Baseline Demographics of Holter ECG Subgroups (1222.11, 1222.12, 1222.13 and 1222.14) |
Holter ECG Data
Shift in SVPB
Neither medically relevant nor statistically significant differences were observed in the SVPB shifts (ie, proportion of patients whose SVPB increased or decreased from baseline) with the active treatments—olodaterol 5 µg, olodaterol 10 μg and formoterol 12 µg—compared with placebo (p-values = 0.3087, 0.9024, 0.4355 and 0.4857 for Week 12, Week 24, Week 40 and Week 48, respectively, Chi-squared test; Figure 1). At Week 48, 38 (23.3%), 43 (25.3%), 32 (18.5%) and 16 (26.7%) patients had an increase in SVPBs from baseline, and 47 (28.8%), 51 (30.0%), 65 (37.6%) and 19 (31.7%) patients had a decrease from baseline with placebo, olodaterol 5 µg, olodaterol 10 µg and formoterol 12 µg, respectively.
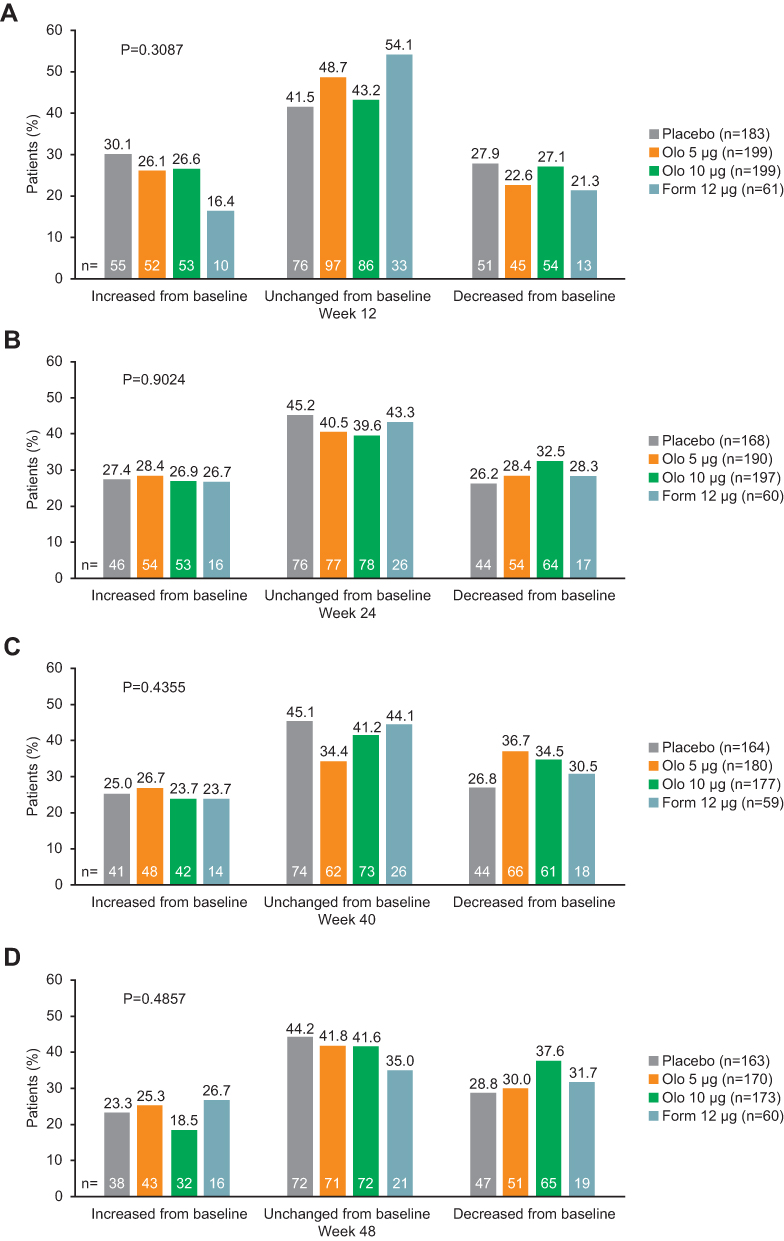 |
Figure 1 Shifts in SVPB: olodaterol and formoterol vs placebo at (A) Week 12, (B) Week 24, (C) Week 40 and (D) Week 48. P-values for overall differences between category of change and category of treatment calculated by Chi-squared frequency tests; Numbers above the bars are % of patients whereas numbers within the bars are number of patients.Abbreviations: Form, formoterol; Olo, olodaterol; SVPB, supraventricular premature beats. |
Shift in VPB
Neither medically relevant nor statistically significant differences were observed in the VPB shifts with the active treatments—olodaterol 5 µg, olodaterol 10 μg and formoterol 12 µg—compared with placebo (p-values = 0.6021, 0.3592, 0.6850 and 0.3256 for Week 12, Week 24, Week 40 and Week 48, respectively, Chi-squared test; Figure 2). At Week 48, 35 (21.5%), 45 (26.5%), 44 (25.4%) and 10 (16.7%) patients had an increase in VPBs from baseline, and 54 (33.1%), 46 (27.1%), 45 (26.0%) and 13 (21.7%) had a decrease from baseline with placebo, olodaterol 5 µg, olodaterol 10 µg and formoterol 12 µg, respectively.
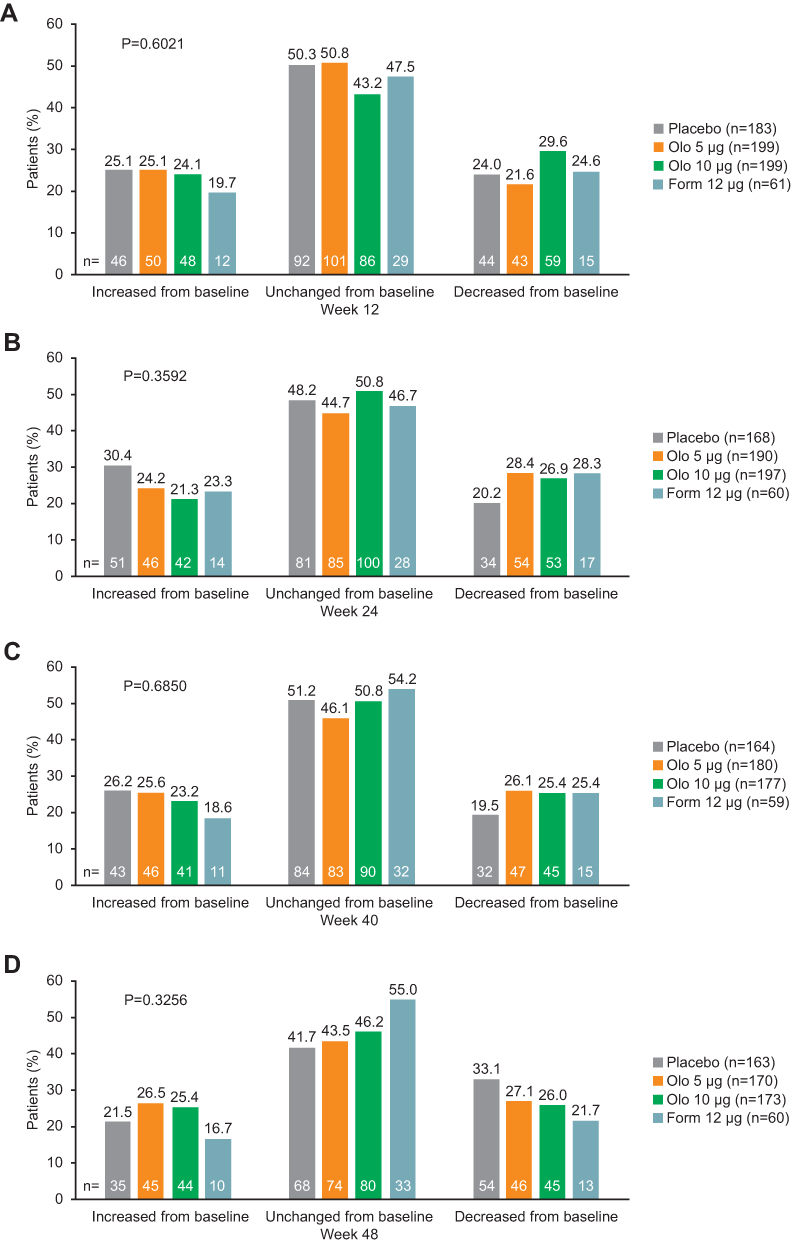 |
Figure 2 Shifts in VPB: olodaterol and formoterol vs placebo at (A) Week 12, (B) Week 24, (C) Week 40 and (D) Week 48. P-values for overall differences between category of change and category of treatment calculated by Chi-squared frequency tests; Numbers above the bars are % of patients whereas numbers within the bars are number of patients.Abbreviations: Form, formoterol; Olo, olodaterol; VPB, ventricular premature beats. |
Holter ECG Heart Rate Data
Overall, numerically small and not clinically relevant differences in the mean heart rate from baseline were observed during treatment. The mean heart rate at baseline was similar between the treatment groups (81.0 beats per minute [bpm] for placebo, 81.1 bpm for olodaterol 5 μg, 82.2 bpm for olodaterol 10 μg and 82.2 bpm for formoterol 12 μg; Figure 3A). During the long-term treatment, there was a numerically small but statistically significant increase with formoterol at Week 24 (+2.9 bpm; p=0.0022), olodaterol 5 μg at Week 12 (+1.1 bpm; p=0.0186) and Week 40 (+1.6 bpm; p=0.0146), and olodaterol 10 μg at Week 40 (+1.7 bpm, p=0.0068) (Figure 3B). At Week 48, no significant changes from baseline were observed for any treatment.
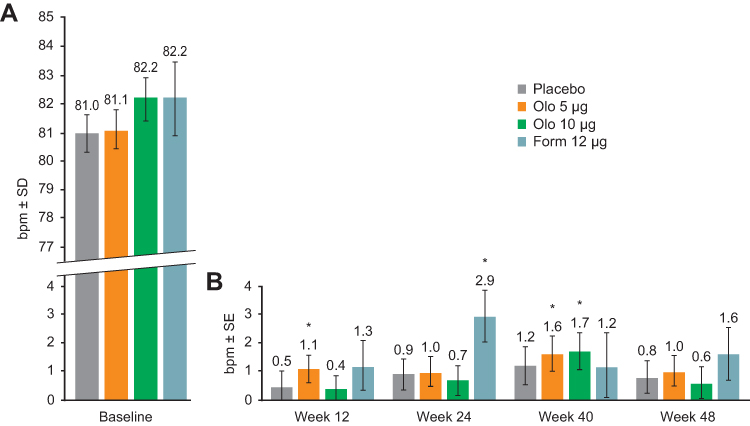 |
Figure 3 Unadjusted baseline heart rate (A) and adjusted mean change in heart rate from baseline (B): olodaterol and formoterol vs placebo during treatment. *P<0.05. P-values are for adjusted mean change from baseline. Abbreviations: bpm, beats per minute; Form, formoterol; Olo, olodaterol; SD, standard deviation; SE, standard error. |
Safety (Adverse Events)
During the 48 weeks of treatment, there was no increase in the number of patients with major adverse CV events (MACE; including cardiac disorder, vascular disorder, myocardial infarction, stroke, sudden death, cardiac death and sudden cardiac death) or fatal MACE with olodaterol (5 µg or 10 µg) or formoterol compared with placebo (MACE: 5 [2.1%], 8 [3.4%], 2 [2.5%] and 9 [4.0%], respectively; fatal MACE [including death unknown]: 2 [0.9%], 1 [0.4%], 1 [1.3%] and 2 [0.9%], respectively) (Table 2). Incidence of cardiac arrhythmia was similar across treatments. The number of patients with cardiac arrhythmia in the olodaterol (5 µg or 10 µg) or formoterol groups was similar compared with the placebo group (supraventricular tachyarrhythmia: 4 [1.7%], 5 [2.1%], 4 [5.0%] and 9 [4.0%], respectively; atrial fibrillation or flutter: 2 [0.9%], 3 [1.3%], 1 [1.3%] and 6 [2.7%], respectively; ventricular tachyarrhythmia: 15 [6.4%], 12 [5.1%], 7 [8.8%] and 8 [3.5%]) (Table 2).
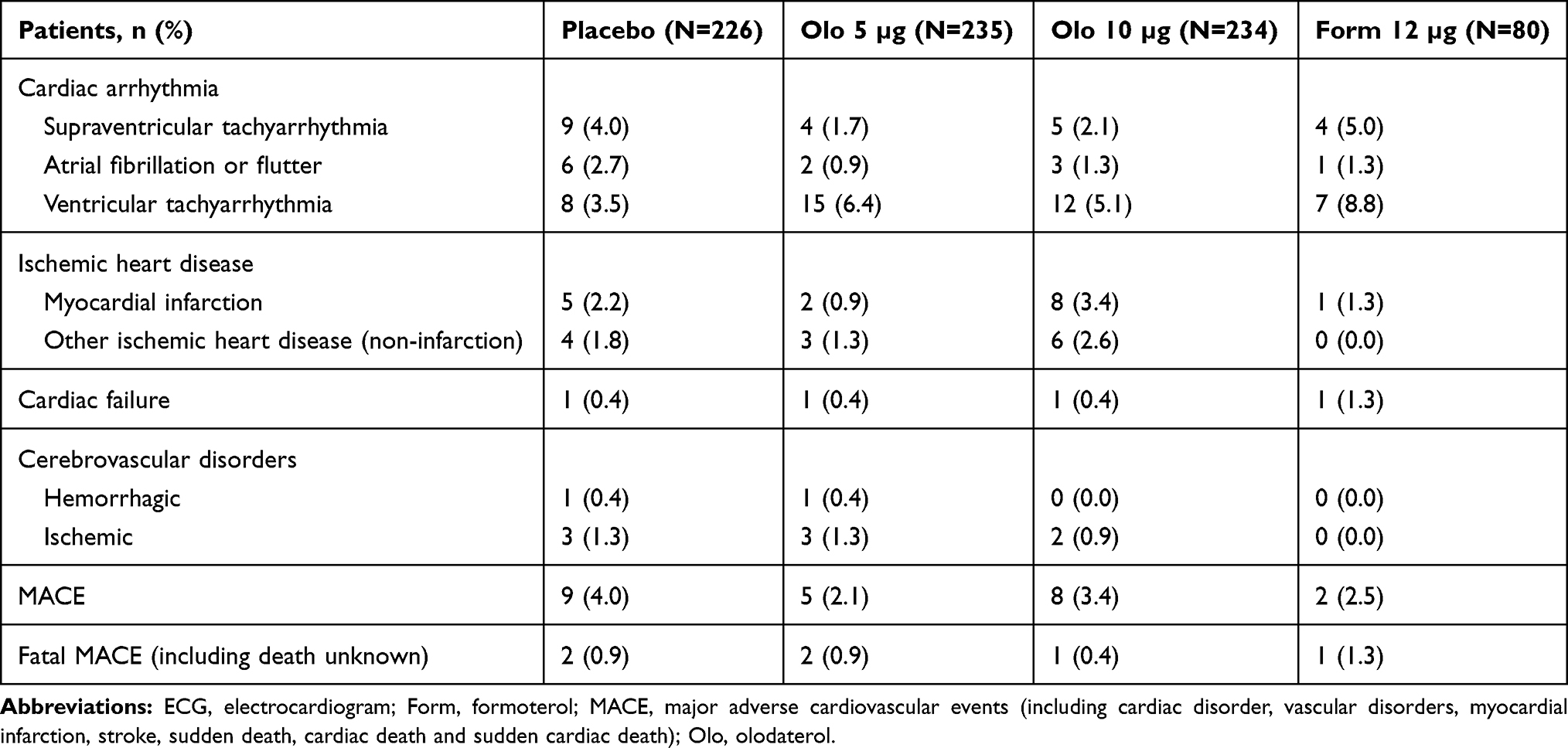 |
Table 2 Adverse Events of Holter ECG Subgroups |
Discussion
Airway obstruction and lung hyperinflation are characteristics of COPD.21 Previous echocardiography data show that lung hyperinflation leads to impaired left ventricular diastolic filling and global right heart dysfunction in patients with COPD.21–23 These mechanisms, alongside hypoxia, chemoreflexes and reduced baroreflexes, may cause neurohumoral activation and increased heart rate.24 Bronchodilators exhibit beneficial effects on daily physical activity, endurance time, hyperinflation and ventricular filling.23,25 Consequently, they have the potential to improve cardiac function26 and reduce neurohumoral activation and heart rate.24
However, there is an ongoing debate about the long-term cardiac safety of cardioactive inhaled pulmonary drugs, such as LABAs, in patients with COPD and concomitant CV morbidities.27 Indeed, LABAs have the potential to induce increased heart rate through stimulation of β2-ARs in the heart.9 For example, salmeterol has been associated with an acute heart rate increase but its cardiac safety has been demonstrated with a longer treatment duration.9 Given this background and that increased heart rate is associated with a higher mortality in patients with COPD, it was of interest to investigate the effect of the LABAs olodaterol and formoterol on cardiac parameters using Holter ECG monitoring. Continuous Holter ECGs are commonly used to diagnose and monitor cardiac arrhythmias,28 and the European Society of Cardiology guidelines recommend 24–48 hours’ continuous Holter recording when arrhythmia is known or suspected to occur.29
Olodaterol is a once-daily LABA designed to improve β2-AR selectivity and intrinsic activity compared with formoterol and salmeterol.15,30 Phase III trials show that olodaterol 5 μg administered using an SMI induces the fast onset of bronchodilation with significant lung function improvements up to 48 weeks in patients with moderate-to-very-severe COPD.15
This paper reports the results of an analysis of Holter ECG data from a subset of patients receiving either olodaterol 5 μg or 10 μg, formoterol 12 μg or placebo in four Phase III trials (1222.11–14). The purpose of the analysis was to examine the cardiac safety of two LABAs and determine whether the structural difference between olodaterol and formoterol results in an observable difference in the safety profiles of the drugs.
Our analysis included a large cohort of 775 patients. Treatment groups were well balanced but there was a lower percentage of patients (48.8%) in the formoterol 12 μg group affected by CV disease at baseline compared with the other treatment groups (62.8% for the olodaterol 10 μg group, 62.6% for the olodaterol 5 μg group and 57.1% for the placebo group; Table 1). This may mean that any effect of formoterol on Holter ECG parameters was less likely to occur in this group compared with the potentially higher risk inherent in the olodaterol groups. However, the analysis shows that there was no evidence of a pro-arrhythmic SVPB and VPB effect for olodaterol 5 µg or 10 µg, or formoterol 12 µg, compared with placebo. With respect to heart rate, only small and transient changes were observed over the 48 weeks of treatment for all treatment groups. It remains uncertain whether these small increases in the mean heart rate, which were statistically significant with formoterol at Week 24, olodaterol 5 μg at Week 12 and Week 40, and olodaterol 10 μg at Week 40, should be attributed to the direct pharmacologic effects of bronchodilators or to increased physical activity following bronchodilation therapy or both.31 A similar trend was observed for placebo over the 48 weeks of treatment and this might indicate a progression of the disease; however, the observation of longer treatment periods may allow the drawing of stronger conclusions. We also found no increase in the number of patients with fatal or major adverse CV events or changes in heart rhythm with any active drug compared with placebo. These results are in line with previous studies demonstrating the cardiac safety of olodaterol and formoterol in patients with COPD.13,32
Neither the structural differences between olodaterol and formoterol nor the difference in baseline CV disease seems to have influenced the analysis outcome. This may not be surprising given the likely low systemic bioavailability of the inhaled drugs.33 Moreover, the high selectivity, high intrinsic activity and enantiopurity of olodaterol allow lower microgram dose amounts compared with other LABAs.18,34 As a consequence of lower doses, less active drug is available for a systemic distribution. Indeed, pharmacokinetic evaluation shows that inhaled olodaterol plasma concentrations decline quickly (37–56% of maximum measured concentration at 6 hours on regular treatment following inhalation of 10 and 20 μg olodaterol); furthermore, trough plasma concentrations were mostly below the limit of quantification (2.0 pg/mL) following inhalation of olodaterol 5 μg once daily and were quantifiable in only one-third of patients after olodaterol 5 μg twice daily and 10 μg once daily.15,35
To our knowledge, this study represents one of the largest and most detailed databases of Holter ECG data in COPD—involving 775 patients—and benefits from the availability of baseline and follow-up data for multiple defined time points and treatment groups. Furthermore, the Holter monitoring enables accurate collection of 24-hour heart rate data during both rest and daily activity. Nevertheless, this analysis also has some limitations. Study sites that were not able to perform Holter ECGs and patients who were not capable of carrying the device were not included in the analysis. Therefore, the subset of patients included in this analysis were not selected at random. At baseline, the Holter subset was representative of the full study population in terms of CV medication but had a slightly higher incidence of arrhythmia. The small difference in cardiac arrhythmia may be explained by the fact that patients in the Holter subset were being treated at specialist hospitals more likely to detect arrhythmia or that they volunteered to be screened as they were familiar with the equipment from previous screening. Additionally, around half of the patients included in the Holter analysis who were treated with a LABA during the trial were receiving LABA therapy at baseline. Previous studies have suggested that an increased risk of CV disease is limited to the initiation of inhaled LABA therapy;36 however, due to the nature of this post hoc analysis, we are unable to investigate whether prior medication had any effect on outcomes. The current post hoc analysis provides useful data in addition to the current literature; however, to detect statistically significant differences of this small magnitude would require a larger study population. Furthermore, although this is a large database, the sample size did not allow reliable detection of differences in rare events such as ventricular tachycardia or sudden cardiac death. Patients with more unstable CV diseases may have been excluded from the trials and subsequent Holter ECG subset. Therefore, further work is needed to study patients with more unstable CV diseases. In this post hoc analysis, the larger treatment groups were broadly well balanced; however, by chance, the smaller formoterol group had fewer cardiovascular risk factors. Despite this, we do not feel that this imbalance has impacted the results of this study.
Conclusions
These data provide reassurance for clinicians that long-term treatment with olodaterol or formoterol, as assessed by Holter ECG, is associated with neither an increased risk of cardiac arrhythmias nor a major impact on heart rate in patients with GOLD 2–4 COPD.
Abbreviations
AR, adrenoreceptor; AUC0–3, area under the curve 3 hours post-dose; bpm, beats per minute; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; DPI, dry powder inhaler; ECG, electrocardiogram; FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Pulmonary Disease; LABA, long-acting β2-agonist; MACE, major adverse cardiovascular event; SMI, Soft Mist™ inhaler; SVPB, supraventricular premature beat; VPB, ventricular premature beat.
Data Sharing Statement
Boehringer Ingelheim is committed to responsible sharing of clinical study reports, related clinical documents, and patient-level clinical study data. Researchers are invited to submit enquiries via the Clinical Study Data Request website (https://www.clinicalstudydatarequest.com).
Ethics Approval and Consent to Participate
All studies included in this analysis were performed in accordance with the provisions of the Declaration of Helsinki (1996 version), the International Conference on Harmonisation Tripartite Guideline for Good Clinical Practice, and local regulations. The protocol was approved by the ethics research boards of the respective institutions, applicable regulatory requirements and Boehringer Ingelheim Standard Operating Procedures. A full list of participating sites in the studies included in this analysis is included in the supplementary file (Supplementary Table 2), and can be found at https://clinicaltrials.gov/ct2/show/NCT00782210, https://clinicaltrials.gov/ct2/show/NCT00782509, https://clinicaltrials.gov/ct2/show/NCT00793624 and https://clinicaltrials.gov/ct2/show/NCT00796653. All patients provided written informed consent. This article does not report individual patient data; all data presented here are anonymized. The clinical trial protocols and the informed consent and patient information forms were reviewed and received approval/favorable opinion from a constituted local Institutional Review Board or an Independent Ethics Committee at each center prior to the start of the study.
Acknowledgments
All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Author Contributions
All the authors have made substantial contributions to study design, data acquisition, analysis or interpretation, drafting the article, or critically revising the content, provided final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
SA reports personal fees from Boehringer Ingelheim and GlaxoSmithKline, and payments for presenting from Boehringer Ingelheim, AstraZeneca, Berlin Chemie, Chiesi and Novartis, outside the submitted work. UB, AdlH, IK and MT are employees of Boehringer Ingelheim. PA reports grants from the German Federal Ministry of Education and Research (BMBF) Competence Network Asthma and COPD (ASCONET), AstraZeneca, GlaxoSmithKline, Grifols Deutschland, MSD Sharp & Dohme, Pfizer, Takeda, Boehringer Ingelheim and Novartis Deutschland, grants and non-financial support from Bayer Schering Pharma AG and Chiesi, grants, personal fees and non-financial support from Novartis Deutschland, and grants and personal fees from Novartis Deutschland, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Alter P, Mayerhofer B, Kahnert K, et al. Prevalence of cardiac comorbidities, and their underdetection and contribution to exertional symptoms in COPD: results from the COSYCONET cohort. Int J Chron Obstruct Pulmon Dis. 2019;14:2163–2172. doi:10.2147/COPD.S209343
2. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2020 report). Published 2019. Available from: https://goldcopd.org/wp-content/uploads/2019/11/GOLD-2020-REPORT-ver1.0wms.pdf.
3. Feary JR, Rodrigues LC, Smith CJ, Hubbard RB, Gibson JE. Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary care. Thorax. 2010;65(11):956–962. doi:10.1136/thx.2009.128082
4. Cazzola M, Calzetta L, Bettoncelli G, et al. Cardiovascular disease in asthma and COPD: a population-based retrospective cross-sectional study. Respir Med. 2012;106(2):249–256. doi:10.1016/j.rmed.2011.07.021
5. Cazzola M, Rogliani P, Matera MG. Cardiovascular disease in patients with COPD. Lancet Respir Med. 2015;3(8):593–595. doi:10.1016/S2213-2600(15)00279-9
6. Janssen O, Schaumann F, Holz O, et al. Low-dose endotoxin inhalation in healthy volunteers-a challenge model for early clinical drug development. BMC Pulm Med. 2013;13(1):19. doi:10.1186/1471-2466-13-19
7. Hawkins NM, Huang Z, Pieper KS, et al. Chronic obstructive pulmonary disease is an independent predictor of death but not atherosclerotic events in patients with myocardial infarction: analysis of the Valsartan in Acute Myocardial Infarction Trial (VALIANT). Eur J Heart Fail. 2009;11(3):292–298. doi:10.1093/eurjhf/hfp001
8. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28(6):1245–1257. doi:10.1183/09031936.00133805
9. Cazzola M, Imperatore F, Salzillo A, et al. Cardiac effects of formoterol and salmeterol in patients suffering from COPD with preexisting cardiac arrhythmias and hypoxemia. Chest. 1998;114(2):411–415. doi:10.1378/chest.114.2.411
10. Boehringer Ingelheim International GmbH. Striverdi Respimat 2.5 microgram, solution for inhalation – summary of product characteristics, Europe. Published 2019. Available from: https://www.medicines.org.uk/emc/product/3255/smpc.
11. Chen Y-F, Cheng Y-C, Chou C-H, Chen C-Y, Yu C-J. Major comorbidities lead to the risk of adverse cardiovascular events in chronic obstructive pulmonary disease patients using inhaled long-acting bronchodilators: a case-control study. BMC Pulm Med. 2019;19(1):233. doi:10.1186/s12890-019-0999-z
12. Salpeter SR, Ormiston TM, Salpeter EE. Cardiovascular effects of β-agonists in patients with asthma and COPD. Chest. 2004;125(6):2309–2321. doi:10.1378/chest.125.6.2309
13. Andreas S, Bothner U, Trampisch M, Haensel M, Buhl R, Alter P. Effect of long-acting β2-agonists olodaterol and formoterol on heart rate and blood pressure in chronic obstructive pulmonary disease patients. Pulm Pharmacol Ther. 2018;52:1–6. doi:10.1016/j.pupt.2018.08.002
14. Rabe KF, Hurst JR, Suissa S. Cardiovascular disease and COPD: dangerous liaisons? Eur Respir Rev. 2018;27(149):
15. Matera MG, Ora J, Cazzola M. Differential pharmacology and clinical utility of long-acting bronchodilators in COPD - focus on olodaterol. Ther Clin Risk Manag. 2015;11:1805–1811. doi:10.2147/TCRM.S73581
16. Handley DA, Morley J. The pursuit of precision pharmaceuticals: divergent effects of β2 agonist isomers. Expert Opin Investig Drugs. 1998;7(10):1601–1616. doi:10.1517/13543784.7.10.1601
17. Ramsay CM, Cowan J, Flannery E, McLachlan C, Taylor DR. Bronchoprotective and bronchodilator effects of single doses of (S)-salbutamol, (R)-salbutamol and racemic salbutamol in patients with bronchial asthma. Eur J Clin Pharmacol. 1999;55(5):353–359. doi:10.1007/s002280050640
18. Ferguson GT, Feldman GJ, Hofbauer P, et al. Efficacy and safety of olodaterol once daily delivered via Respimat® in patients with GOLD 2–4 COPD: results from two replicate 48-week studies. Int J Chron Obstruct Pulmon Dis. 2014;9:629–645. doi:10.2147/COPD.S61717
19. Koch A, Pizzichini E, Hamilton A, et al. Lung function efficacy and symptomatic benefit of olodaterol once daily delivered via Respimat® versus placebo and formoterol twice daily in patients with GOLD 2–4 COPD: results from two replicate 48-week studies. Int J Chron Obstruct Pulmon Dis. 2014;9:697–714. doi:10.2147/COPD.S62502
20. McGarvey L, Niewoehner D, Magder S, et al. One-year safety of olodaterol once daily via Respimat® in patients with GOLD 2–4 chronic obstructive pulmonary disease: results of a pre-specified pooled analysis. COPD. 2015;12(5):484–493. doi:10.3109/15412555.2014.991864
21. Alter P, Watz H, Kahnert K, et al. Airway obstruction and lung hyperinflation in COPD are linked to an impaired left ventricular diastolic filling. Respir Med. 2018;137:14–22. doi:10.1016/j.rmed.2018.02.011
22. Watz H, Waschki B, Meyer T, et al. Decreasing cardiac chamber sizes and associated heart dysfunction in COPD: role of hyperinflation. Chest. 2010;138(1):32–38. doi:10.1378/chest.09-2810
23. Hohlfeld JM, Vogel-Claussen J, Biller H, et al. Effect of lung deflation with indacaterol plus glycopyrronium on ventricular filling in patients with hyperinflation and COPD (CLAIM): a double-blind, randomised, crossover, placebo-controlled, single-centre trial. Lancet Respir Med. 2018;6(5):368–378. doi:10.1016/S2213-2600(18)30054-7
24. Raupach T, Bahr F, Herrmann P, et al. Slow breathing reduces sympathoexcitation in COPD. Eur Respir J. 2008;32(2):387–392. doi:10.1183/09031936.00109607
25. Maltais F, O’Donnell D, Galdiz Iturri JB, et al. Effect of 12 weeks of once-daily tiotropium/olodaterol on exercise endurance during constant work-rate cycling and endurance shuttle walking in chronic obstructive pulmonary disease. Ther Adv Respir Dis. 2018;12:1–13. doi:10.1177/1753465818755091
26. Berton DC, Barbosa PB, Takara LS, et al. Bronchodilators accelerate the dynamics of muscle O2 delivery and utilisation during exercise in COPD. Thorax. 2010;65(7):588–593. doi:10.1136/thx.2009.120857
27. Lahousse L, Verhamme KM, Stricker BH, Brusselle GG. Cardiac effects of current treatments of chronic obstructive pulmonary disease. Lancet Respir Med. 2016;4(2):149–164. doi:10.1016/S2213-2600(15)00518-4
28. Galli A, Ambrosini F, Lombardi F. Holter monitoring and loop recorders: from research to clinical practice. Arrhythm Electrophysiol Rev. 2016;5(2):136–143. doi:10.15420/AER.2016.17.2
29. Priori SG, Blomström-Lundqvist C, Mazzanti A, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). EP Europace. 2015;17(11):1601–1687. doi:10.1093/europace/euv319
30. Incorvaia C, Montagni M, Makri E, Riario-Sforza GG, Ridolo E. Striving for optimal bronchodilation: focus on olodaterol. Int J Chron Obstruct Pulmon Dis. 2016;11:439–444. doi:10.2147/COPD.S96070
31. Watz H, Troosters T, Beeh KM, et al. ACTIVATE: the effect of aclidinium/formoterol on hyperinflation, exercise capacity, and physical activity in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2545–2558. doi:10.2147/COPD.S143488
32. Nelson HS, Gross NJ, Levine B, et al. Cardiac safety profile of nebulized formoterol in adults with COPD: a 12-week, multicenter, randomized, double- blind, double-dummy, placebo- and active-controlled trial. Clin Ther. 2007;29(10):2167–2178. doi:10.1016/j.clinthera.2007.10.007
33. Borghardt JM, Kloft C, Sharma A. Inhaled therapy in respiratory disease: the complex interplay of pulmonary kinetic processes. Can Respir J. 2018;2018:2732017. doi:10.1155/2018/2732017
34. Bouyssou T, Hoenke C, Rudolf K, et al. Discovery of olodaterol, a novel inhaled β2-adrenoceptor agonist with a 24h bronchodilatory efficacy. Bioorg Med Chem Lett. 2010;20(4):1410–1414. doi:10.1016/j.bmcl.2009.12.087
35. Maleki-Yazdi MR, Beck E, Hamilton AL, Korducki L, Koker P, Fogarty C. A randomised, placebo-controlled, phase II, dose-ranging trial of once-daily treatment with olodaterol, a novel long-acting β2-agonist, for 4 weeks in patients with chronic obstructive pulmonary disease. Respir Med. 2015;109(5):596–605. doi:10.1016/j.rmed.2015.02.012
36. Wang M-T, Liou J-T, Lin CW, et al. Association of cardiovascular risk with inhaled long-acting bronchodilators in patients with chronic obstructive pulmonary disease: a nested case-control study. JAMA Intern Med. 2018;178(2):229–238. doi:10.1001/jamainternmed.2017.7720
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.