")
Back to Journals » Patient Preference and Adherence » Volume 12
A pilot study of observed physician–parent–child communication and child satisfaction in a gastroenterology clinic
Authors Becker TD , Lin HC, Miller VA
Received 19 April 2018
Accepted for publication 22 May 2018
Published 26 July 2018 Volume 2018:12 Pages 1327—1335
DOI https://doi.org/10.2147/PPA.S171620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Timothy D Becker,1 Henry C Lin,2 Victoria A Miller3
1Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 2Division of Gastroenterology, Hepatology, and Nutrition, Children’s Hospital of Philadelphia, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 3Division of Adolescent Medicine, Children’s Hospital of Philadelphia, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
Background: Child participation in pediatric medical visits is low. In this pilot study, we sought to better understand relationships between observed communication and child-reported perceptions of communication in a clinical setting.
Materials and methods: For this cross-sectional observational study, pediatric gastroenterology appointments (n=39) were videotaped and coded to quantify various adult affective (eg, chit-chat, empathy) and facilitative (eg, asking questions, encouraging responses) behaviors toward the child, interference with child participation (eg, interrupting or ignoring child), and child verbal participation. Post-visit surveys assessed child perceptions of having voice in the clinical encounter, ease of understanding, and satisfaction with communication.
Results: Parent and provider chit-chat was associated with child-reported ease of understanding. Provider facilitation was positively associated with child participation, but affective communication strategies were not. Physician interference was negatively associated with ease of understanding but positively associated with perception of voice.
Conclusion: Facilitative communication may improve outcomes by enhancing child participation and thus exchange of medical information, whereas chit-chat appears to positively impact children’s perceptions of communication.
Keywords: physician–patient communication, partnership, child participation, pediatric patient experience, child satisfaction
Introduction
Communication between physicians, patients, and patients’ families underlies nearly all aspects of medical practice. Over recent decades, efforts have been made throughout medicine to enhance patient autonomy by encouraging patient-centered communication styles and involving patients as shared decision makers. Despite these advances, communication in the pediatric setting has remained largely adult dominated. Although evidence suggests that child participation has increased somewhat over the decades,1 numerous studies have shown that overall child participation in medical encounters remains low.2–6 Studies have found that physicians infrequently facilitate youth input7 and parents interfere with physician–child communication.4,6,8
National pediatric leaders have recognized the importance of increasing child and adolescent participation in healthcare encounters.9,10 Adolescents have reported preferring direct communication with them rather than with their parents11 and valuing direct communication and responsiveness to their concerns.12–14 In studies of youth, patient-centered communication style has been associated with increased medication adherence15 and perceptions of control and competence in managing a chronic disease.16 Participation and decision-making involvement are distinct from shared decision making, a concept initially developed in the setting of adult patient and provider relationships (extended to adult caregivers in pediatrics) that requires mutual information sharing and agreement about decisions.17,18 Since children are still in the process of developing their decision making and communication capabilities, they are not necessarily equal partners in decision making. However, children learn about, practice, and develop communication and decision-making skills through participation in clinical encounters,19 and the experience of participation sets the stage for increased participation over time.20 Increased child participation in medical encounters may also enhance clinically relevant information exchange, since youth may have information that parents do not have,21 reduce complications, improve youth decision making and self-advocacy skills,22 and improve child satisfaction with healthcare; however, these relationships are still unclear.
Communication in medical appointments serves two broad purposes – to build a therapeutic alliance between the patient and physician and promote an efficient exchange of information in order to ensure accurate diagnosis and treatment. Communication has thus traditionally been classified into affective and instrumental subtypes.23 Affective communication builds the doctor-patient relationship through empathic statements, friendly talk, and displays of concern. Instrumental communication facilitates information exchange by asking questions, soliciting opinions, and checking for self and other understanding. Early observational studies of physician–patient–parent communication indicated that physician behavior toward children was predominantly affective, while that with parents was predominantly instrumental.24,25 However, subsequent research has underscored that physician communication with children is not exclusively affective, and significant important information exchange occurs as well.26
Since child participation in pediatric encounters is a developmental process, it is important that children’s satisfaction with the experience of participating is understood. Despite the suspicion that physician communication style and quality are related to pediatric patient satisfaction with communication, the relationship between observed communication and child satisfaction has been studied infrequently. To our knowledge, only one observational study has investigated the relationship between observed communication and child satisfaction.3 Wassmer et al measured the amount of time participants spent engaging in generally instrumental, affective, or social speech, but did not scrutinize the effects of specific communication strategies directed at the child.
The present pilot study sought to investigate relationships between communication and child satisfaction with communication in a subspecialty pediatric clinic setting. It was hypothesized that child satisfaction would be positively associated with patient-centered communication, including both facilitative communication directed at the child (ie, physician asking questions and physician partnership) and affective communication (ie, rapport, chit-chat, and jokes).11,27 By contrast, it was expected that physician interference with child participation would be negatively associated with child satisfaction. Consistent with previous research, it was hypothesized that physician and parent affective communication and facilitative communication directed at the child would be positively associated with child verbal participation8,28–30 and that parent and physician interference would be negatively associated with child participation.4,8 Finally, it was hypothesized that physician facilitative communication, child verbal participation, and child satisfaction would correlate positively with child’s age2,5,6,8,26,31 and that child verbal participation would be positively associated with parent education levels.5,6,32
Materials and methods
Recruitment and participants
This descriptive cross-sectional study was part of a larger study assessing patient-preferred communication strategies, observed communication, knowledge retention, and patient satisfaction. Ten physicians in the outpatient Gastroenterology Clinic at the Children’s Hospital of Philadelphia were consented and enrolled for participation, based on availability on specific study days and a high-volume clinic schedule. Patients of the enrolled physicians and their parents who attended the clinic were recruited and enrolled from January 2016 to October 2016.
Patients were eligible for study inclusion if the child was between ages 8 and 17 years, the primary caregiver (parent or legal guardian) accompanied the patient to the clinic visit, the patient provided informed assent, and the caregiver provided written informed consent and permission. Patients were excluded if the clinicians had previously identified social or legal concerns, the caregiver was absent, or the patient or caregiver was non-English speaking.
Procedures
The study was approved by the Children’s Hospital of Philadelphia Institutional Review Board. Eligible physicians were verbally consented once for multiple clinic visits. Eligible patients and caregivers were approached by a member of the research team in-person on the visit day to ask about participation in the study, which consisted of video recording of the clinic session and administration of questionnaires to the patient and caregiver. Patients and caregivers were informed that they could ask that the video recorder be turned off for any reason, including discussion of sensitive topics or undressing for physical examination. They were also informed that they could ask that the entire recording be erased after the visit. Written informed consent and permission were obtained from parents/caregivers, and assent to participate was obtained from children.
Immediately after the visit, a research assistant verbally administered questionnaires separately to patients and caregivers. Each caregiver and child participant who completed the questionnaires received a US$10 gift card. Raw data were input and managed in Research Electronic Data Capture.33
Measures
Demographics
Caregivers completed a demographics questionnaire that included questions about their relationship to the child, race, and the caregiver’s highest level of education. Patient age, visit diagnosis, and number of previous visits to the gastroenterology clinic were documented from the electronic medical record.
Coding system to measure communication
The video observations were coded according to an adaptation of the Roter Interaction Analysis System (RIAS), a system used widely in pediatric communication research. In the original system, each utterance by a parent, child, or clinician is categorized into one of 38 mutually exclusive categories.34 RIAS codes were modified to meet the needs of a non-transcribed, video-coded study directed toward understanding the impact of verbal interactions relevant to child satisfaction and health-related engagement. As such, parent–physician interactions were not coded. Each adult utterance directed at affective communication toward the child (Rapport, Chit-Chat, Joke), facilitation of child involvement (Ask Child Question, Partnership), or interference with child involvement was coded for the speaker (parent or physician) and the specific category of communication (Table 1). Rapport, Partnership, and Interference were summary scores made up of sub-categories of these types of communication (Table 1). Information giving by adults was not coded, due to challenge in determining to whom such speech was directed and the focus of the study on efforts to facilitate child involvement. All child utterances were coded and summed into a total score for Child Verbal Participation (Table 1). Thirty-five cases were double coded so that inter-rater reliability could be assessed. Intraclass correlation coefficients (ICCs), using a two-way random effects model, were computed. For the physician communication variables, ICCs were considered excellent and ranged from 0.86 to 0.98, with the exception of Interference, which had an ICC of 0.47 (fair). For the parent communication variables, ICCs were considered excellent and ranged from 0.81 to 0.98, with the exception of chit-chat, which had an ICC of 0.58 (fair). The ICC for child verbal participation was 0.99 (excellent).35
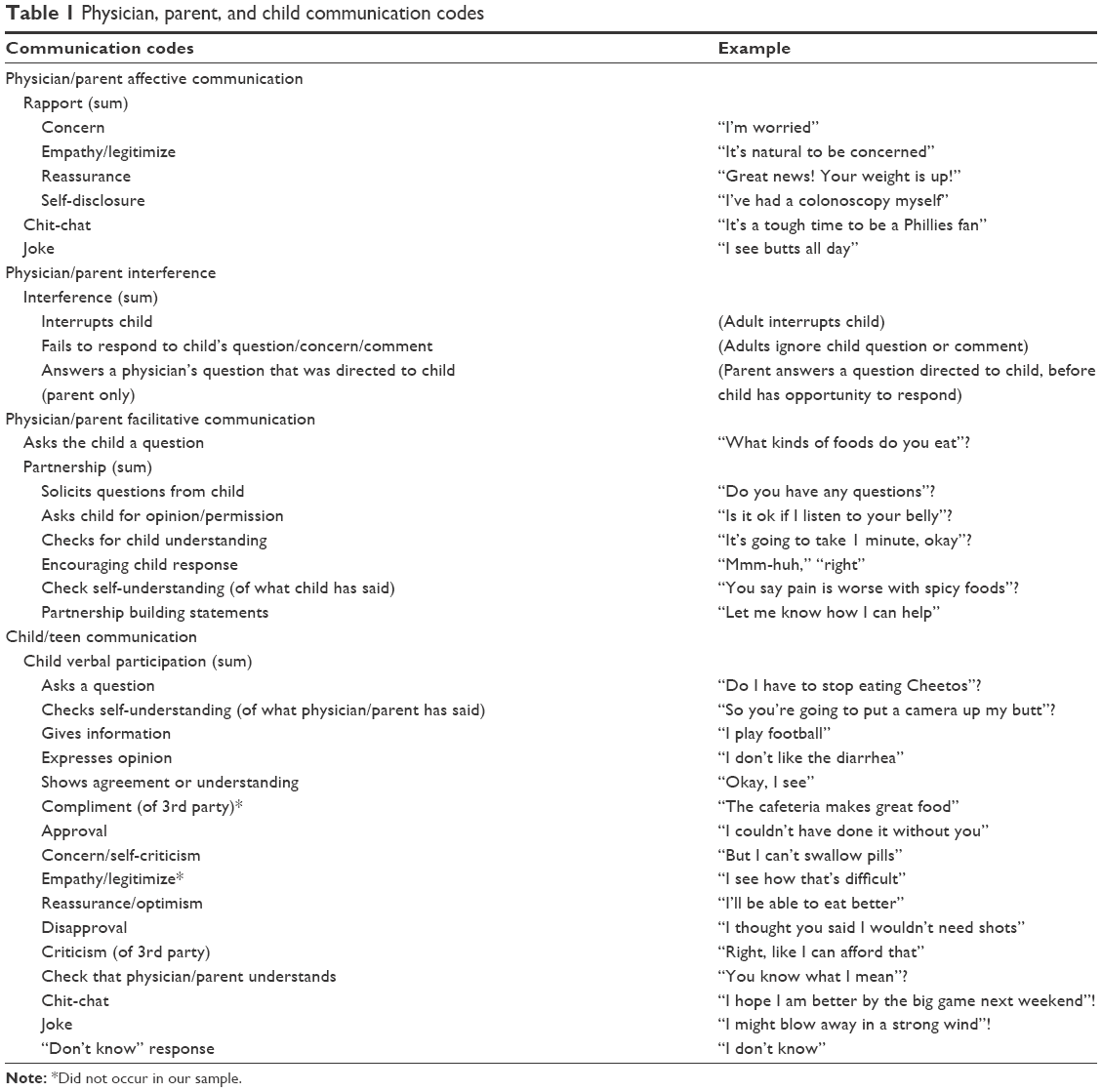 | Table 1 Physician, parent, and child communication codes |
Patient satisfaction
Child perceptions of clinic visit
The perceptions survey included three questions that have been previously described.36 Questions included “How easy was it to understand the information that was discussed during your clinic visit today?”, “How much of a voice did you have in the clinic visit today?”, and “How satisfied are you with communication between you and your doctor today?”. Each item had a four-point Likert-type response scale: not much/not very, a little bit, quite, and very/a lot.
Metro assessment of child satisfaction (MACS)
The MACS consists of eight items and has been validated as a measure of child satisfaction in outpatient pediatric visits.37 Examples of questions include “did the doctor talk to you before he/she did something?”, “did the doctor listen to what you said?”, and “did you understand what the doctor said to you?”. Internal consistency analysis yielded low Cronbach’s alpha in this sample (α=0.07), and so the MACS was discarded in hypothesis testing.
Analytic plan
We analyzed data with STATA MP, version 13.0, copyright 1985–2013 by StataCorp (College Station, TX, USA). We utilized frequencies, means, and SD to describe patient characteristics and communication observed in the visits. Variables were tested for normality by examining the skewness, with a value of less than 2 considered sufficiently normal.38 Dichotomous variables were created for parent education (college education or not) and race (white/non-white), given limited variation within those variables in the sample. Statistical methods to test the hypotheses included independent sample t-tests to test difference in means between dichotomous variables, Pearson correlations, to test relationships between two interval variables with normal distributions, and Spearman correlations, and to test relationships including variables with non-normal distributions or ordinal variables (eg, child perceptions).
Results
Participants
Ten of 11 approached physicians participated in the study (91%; 8 females, 2 males) and each conducted a mean of 3.9 appointments (SD=2.81; range 1–9).
For the larger study, 172 patients and caregivers were approached, 121 (70%) agreed to participate in the surveys, and 85 of the 121 survey participants (70%) also agreed to video observation. Among the 85 patients in the larger study who agreed to video observation, 41 were aged 8–17 years and therefore eligible to complete self-report questionnaires. Two children did not complete the outcomes surveys, resulting in a final sample of 39 patients for the present analysis. The most common visit diagnoses were abdominal pain (n=17, 44%), constipation (n=12, 31%), nausea and/or vomiting (n=7, 18%), and various combinations of malnutrition, weight loss, or poor weight gain (n=6, 15%). Patients could have more than one diagnosis. Patient and family demographic and visit characteristics are summarized in Table 2.
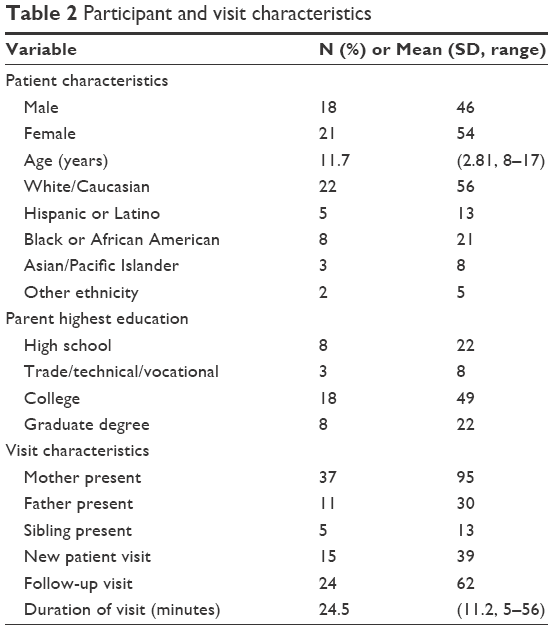 | Table 2 Participant and visit characteristics |
Descriptive findings
Most children perceived high levels of understanding information discussed during the visit, with 54% (n=21) reporting the visit was “very easy” to understand and 28% (n=11) reporting it was “quite easy” to understand. Patients varied in their perception of having voice in the visit, with 28% (n=11) reporting “a lot of voice”, 36% (n=14) reporting “quite a bit” of voice, and 36% (n=14) reporting “a little bit”. Overall, patients reported high levels of satisfaction with communication with their physician, with 74% (n=29) endorsing that they were “very satisfied” with the physician’s communication during the visit. Descriptive statistics for parent, physician, and child communication can be found in Table 3.
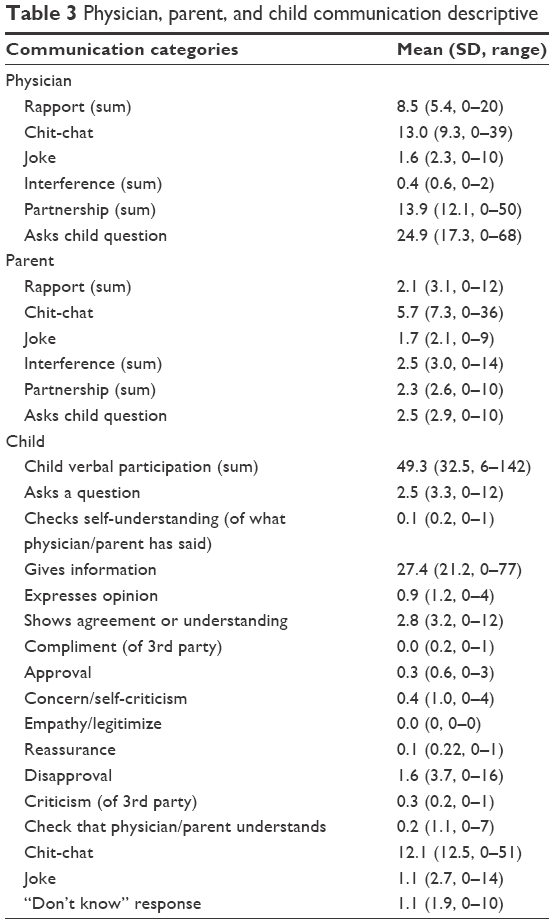 | Table 3 Physician, parent, and child communication descriptive |
Hypothesis testing of outcomes
Association of child satisfaction with parent and physician communication
Contrary to our hypothesis regarding facilitative communication, no relationships were found between physician or parent asking questions or physician or parent partnership and any of the three child satisfaction outcomes.
Consistent with our hypothesis regarding affective communication, physician chit-chat correlated positively with ease of understanding (rs=0.36, p<0.05). However, no relationships were found between physician chit-chat and perceptions of voice in the clinic visit or satisfaction with communication, or between physician rapport or joke and any of the three outcomes. Parent chit-chat also correlated positively with ease of understanding (rs=0.42, p<0.01). No relationships were found between parent chit-chat and perception of voice in the clinic visit or satisfaction with communication, or between parent rapport or joke and any of the three outcomes.
Consistent with our hypothesis, physician interference correlated negatively with ease of understanding (rs=−0.42, p<0.01); however, contrary to expected, physician interference correlated positively with child’s perception of voice in the visit (rs=0.40, p<0.05), and was not related to satisfaction with communication. Parent interference was not related to any of the three outcomes.
Association of child participation with parent and physician communication
As hypothesized, child verbal participation correlated positively with facilitative physician behaviors, including partnership (r=0.52, p<0.001) and asking questions (r=0.56, p<0.001). However, we found that only one affective communication strategy, chit-chat, was associated with any satisfaction outcome, child ease of understanding. Contrary to hypothesis, child verbal participation correlated positively with physician interference (r=0.37, p<0.05). Child verbal participation was also not related to parent questions or partnership, parent interference, parent chit-chat, jokes, or rapport-building.
Association of child participation and satisfaction with demographics
No relationship was found between child verbal participation and child age, sex, or parent education level. Physician asking questions and partnership were not related to patient age. Child age correlated positively with ease of understanding (rs=0.40, p<0.05) and voice in clinic visit (rs=0.46, p<0.01), but was not related to satisfaction with communication.
Discussion
Although children’s preferences about communication have been assessed in a variety of qualitative studies,13,39,40 little is known about how children’s perceptions correlate with adult communication behaviors in actual observed encounters.41 To our knowledge, only one previous observational study has attempted to measure the child’s perspective but defined styles of communication broadly and found no relationship between communication styles and child satisfaction.3 The present pilot study sought to better understand how adult communication impacts child perceptions by assessing associations between various child-directed adult communication strategies and child perceptions of understanding, voice, and satisfaction with communication.
We expected that affective communication strategies, such as chit-chat, jokes, and rapport would be associated with child satisfaction by fostering a friendly atmosphere. In this study, only one affective communication strategy, chit-chat, which includes non-medical small talk, was associated with any satisfaction outcome, child ease of understanding. Social conversation may set the tone of the encounter as one that is friendly and accessible to the child, thus enhancing child understanding.24 Child-directed chit-chat is presumably tailored to be developmentally appropriate, and thus may be more interesting and easier to understand than medical topics, which may not always be as developmentally tailored. Alternatively, high levels of chit-chat may reflect other, unmeasured visit characteristics. For example, it is possible that chit-chat is more likely when the visit is less acute or complex, and satisfaction relates to this characteristic of the visit rather than chit-chat itself.
As expected, physician interference with child participation was negatively associated with child-reported ease of understanding. However, interference was positively associated with child perception of having voice. This suggests that although physicians might have interfered more frequently because the child was speaking a lot, perhaps due to child misunderstandings, the child still felt heard, despite the interference.
Contrary to expectations, child satisfaction outcomes were not related to other affective strategies, such as rapport building, or to communication aiming to facilitate child involvement. Furthermore, observed levels of child communication were not related to child satisfaction outcomes. Although healthcare communication style has been shown to be important to adult satisfaction,42 children may value different aspects of the clinical experience. For example, a previous study of adolescent perceptions of healthcare found characteristics related to clinic cleanliness and clinician competency to be more important to youth than most characteristics of the patient-provider relationship.12 Sleath et al previously found that children were most satisfied with doctors who knew them as a person, rather than those who used a participatory style.27
As expected, child verbal participation was positively related to physician facilitative behaviors, such as asking questions and partnership, but participation was not associated with affective behaviors. This suggests physician efforts to engage children by asking questions, encouraging responses, and checking understanding are fruitful, despite challenges to youth participation, including perceived lack of interest, time restrictions, and parent interference.6 Contrary to previous studies, observed child participation did not correlate with age; however, child perceptions of ease of understanding and having voice increased with age. A possible explanation for these findings is that although the quantity of child verbal participation did not increase with age, the quality of participation (eg, input into decision making) might have increased in ways not measured in this study, leading to increased satisfaction.
Ultimately, affective and facilitative communication strategies are both suspected to be important to patient engagement in healthcare, perhaps by different pathways, as the present results imply. Affective strategies, such as chit-chat, may enhance patients’ positive feelings about medical encounters and may improve outcomes via increased adherence, whereas facilitative strategies increase the exchange of information between physician and patient, likely enabling more accurate diagnosis and appropriate treatment planning. However, these hypotheses require further investigation.43
Limitations
The results of this study should be interpreted with several limitations in mind. This study examined a small sample with limited racial and socioeconomic diversity, thus limiting generalizability, as communication patterns have been shown to vary by these characteristics.29,32 Also, the ages of patients varied from 8 to 17 years, encompassing a range of developmental stages, during which child participation has been shown to evolve.44 Selection bias might have limited inclusion of less social physicians or families or those with more strained physician-family relationships. Participants were aware that they were being videotaped, thus leading to the possibility of a Hawthorne effect – that participants did not display their typical behavior due to awareness of observation. However, prior research in pediatric sub-specialty clinics suggests negligible effects of observational reactivity with respect to communication.45 In addition, the sample was cross-sectional and included both new patient visits and follow-up visits, and results may be confounded by the stage and quality of the ongoing physician–family relationship.2,46
Child satisfaction outcomes should be understood in light of measurement limitations. Although the Metro Assessment of Child Satisfaction, a previously validated multi-item scale for pediatric medical encounter satisfaction, was utilized, it was found to have low internal consistency in the present sample and was discarded. As a result, the study reports single-item measures, which are more susceptible to random error and lower construct validity, because they are less likely to account for all facets of a construct.47 However, the single-item measures used have been previously reported to describe children’s perceptions in medical settings,36 and child satisfaction related to observed participation has rarely been previously measured in any form.
Although RIAS, from which this study’s coding scheme was derived, has been validated and widely applied in medical communication research, the method has notable limitations in capturing important aspects of physician–patient communication. Although verbal interactions were coded in detail, the scheme did not explicitly capture non-verbal communication, such as head nods, smiling, and gaze, which may influence patient communication, especially in younger children.2 Since the coding scheme resulted in sums of interaction types, it ignored sequence of turn taking, such as the physician giving the patient space to talk,41 thus limiting understanding of communication dynamics. For example, previous studies have suggested that certain parent behaviors can shift physician attention from child to parent, thus decreasing subsequent child participation.8 The scheme also does not analyze speech content; so although the child participation measure serves as an indicator of quantity of participation, it says little about quality, such as input into decision making.
Questions for future research
This analysis suggests that child perceptions of medical communication are associated with age and chit-chat directed at the child. However, further research is needed to elucidate how adult communication strategies and child participation are related to child satisfaction with healthcare. Future research that utilizes multiple items to capture various dimensions of child satisfaction (eg, trust in clinician and healthcare system, feeling respected, feeling heard, feeling supported, shared understanding with physician, and satisfaction with decisions) will enhance reliability and validity of findings. Furthermore, since physician–patient relationships evolve over time, longitudinal studies of satisfaction and participation should clarify if satisfaction with one encounter influences no-show rates and participation levels in future encounters.
Ultimately, clinical research aims to improve patient outcomes, but relationships between child participation and outcomes remain enigmatic. We sought to better delineate the relationship of participation with satisfaction and perceived understanding, but future studies are also needed to investigate relationships with actual patient understanding, patient recall of information exchanged in the clinical encounter, patient sense of control over their health, adherence to clinical regimens, and health outcomes, such as chronic disease exacerbations and biomarkers of disease progression.
Implications for practice
The present pilot study builds on existing pediatric communication literature to suggest how provider and parent communication behaviors impact child communication and perceptions of voice, ease of understanding, and satisfaction with communication. Providers can use facilitative strategies such as asking questions, soliciting questions from the child, and checking for understanding to increase child participation and by doing so may facilitate children’s development of social skills in clinical contexts. The finding that chit-chat was associated with improved perceptions of understanding suggests that providers can strategically use developmentally appropriate non-medical small talk to engage patients.
Conclusion
This pilot study was one of the first to assess the relationship between observed physician–parent–child communication and child-reported satisfaction outcomes. We found that chit-chat, an affective strategy, and age were positively related to patient perceptions of communication. Physician interference was negatively associated with child-perceived ease of understanding. Although physician and parent use of facilitative communication strategies was related to observed child verbal participation, such strategies were not associated with any of the child-reported outcomes. Further research is needed to clarify pathways between child participation and health outcomes.
Acknowledgments
The Division of Gastroenterology, Hepatology, and Nutrition and Division of Adolescent Medicine, Department of Pediatrics, Children’s Hospital of Philadelphia funded the project. We are grateful to our research staff, patients, families, and colleagues at Children’s Hospital of Philadelphia for assistance in completion of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Meeuwesen L, Kaptein M. Changing interactions in doctor-parent-child communication. Psychol Health. 1996;11(6):787–795. | ||
van Dulmen AM. Children’s contributions to pediatric outpatient encounters. Pediatrics. 1998;102(3 Pt 1):563–568. | ||
Wassmer E, Minnaar G, Abdel Aal N, et al. How do paediatricians communicate with children and parents? Acta Paediatr. 2004;93(11):1501–1506. | ||
Savage E, Callery P. Clinic consultations with children and parents on the dietary management of cystic fibrosis. Soc Sci Med. 2007;64(2):363–374. | ||
Cox ED, Smith MA, Brown RL, Fitzpatrick MA. Learning to participate: effect of child age and parental education on participation in pediatric visits. Health Commun. 2009;24(3):249–258. | ||
van Staa AL; On Your Own Feet Research Group. Unraveling triadic communication in hospital consultations with adolescents with chronic conditions: the added value of mixed methods research. Patient Educ Couns. 2011;82(3):455–464. | ||
Sleath BL, Carpenter DM, Sayner R, et al. Child and caregiver involvement and shared decision-making during asthma pediatric visits. J Asthma. 2011;48(10):1022–1031. | ||
Tates K, Elbers E, Meeuwesen L, Bensing J. Doctor-parent-child relationships: a “pas de trois.” Patient Educ Couns. 2002;48(1):5–14. | ||
Fiks AG, Localio AR, Alessandrini EA, Asch DA, Guevara JP. Shared decision-making in pediatrics: a national perspective. Pediatrics. 2010;126(2):306–314. | ||
Sawyer SM, Ambresin AE, Bennett KE, Patton GC. A measurement framework for quality health care for adolescents in hospital. J Adolesc Health. 2014;55(4):484–490. | ||
Britto MT, DeVellis RF, Hornung RW, DeFriese GH, Atherton HD, Slap GB. Health care preferences and priorities of adolescents with chronic illnesses. Pediatrics. 2004;114(5):1272–1280. | ||
Ginsburg KR, Slap GB, Cnaan A, Forke CM, Balsley CM, Rouselle DM. Adolescents’ perceptions of factors affecting their decisions to seek health care. JAMA. 1995;273(24):1913–1918. | ||
Carpenter DM, Stover A, Slota C, et al. An evaluation of physicians’ engagement of children with asthma in treatment-related discussions. J Child Health Care. 2014;18(3):261–274. | ||
Coyne I, Amory A, Kiernan G, Gibson F. Children’s participation in shared decision-making: children, adolescents, parents and healthcare professionals’ perspectives and experiences. Eur J Oncol Nurs. 2014;18(3):273–280. | ||
Kyngäs H, Hentinen M, Barlow JH. Adolescents’ perceptions of physicians, nurses, parents and friends: help or hindrance in compliance with diabetes self-care? J Adv Nurs. 1998;27(4):760–769. | ||
Croom A, Wiebe DJ, Berg CA, et al. Adolescent and parent perceptions of patient-centered communication while managing type 1 diabetes. J Pediatr Psychol. 2011;36(2):206–215. | ||
Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes, at least two to tango). Soc Sci Med. 1997;44(5):681–692. | ||
Wyatt KD, List B, Brinkman WB, et al. Shared decision making in pediatrics: a systematic review and meta-analysis. Acad Pediatr. 2015;15(6):573–583. | ||
Ruhe KM, De Clercq E, Wangmo T, Elger BS. Relational capacity: broadening the notion of decision-making capacity in paediatric healthcare. J Bioeth Inq. 2016;13(4):515–524. | ||
Edwards A, Elwyn G. Inside the black box of shared decision making: distinguishing between the process of involvement and who makes the decision. Health Expect. 2006;9(4):307–320. | ||
Hafetz J, Miller VA. Child and parent perceptions of monitoring in chronic illness management: a qualitative study. Child Care Health Dev. 2010;36(5):655–662. | ||
Downing J, Gleeson H, Clayton PE, et al. Communication with young people in paediatric and adult endocrine consultations: an intervention development and feasibility study. BMC Endocr Disord. 2017;17(1):33. | ||
Bensing JM, Dronkers J. Instrumental and affective aspects of physician behavior. Med Care. 1992;30(4):283–298. | ||
Freemon B, Negrete VF, Davis M, Korsch BM. Gaps in doctor-patient communication: doctor-patient interaction analysis. Pediatr Res. 1971;5:298–311. | ||
Tannen D, Wallat C. Interactive frames and knowledge schemas in interaction: examples from a medical examination/interview. Soc Psychol Q. 1987;50(2):205–216. | ||
Tates K, Meeuwesen L, Bensing J, Elbers E. Joking or decision-making? Affective and instrumental behaviour in doctor-parent-child communication. Psychol Health. 2002;17(3):281–295. | ||
Sleath B, Ayala GX, Washington D, et al. Caregiver rating of provider participatory decision-making style and caregiver and child satisfaction with pediatric asthma visits. Patient Educ Couns. 2011;85(2):286–289. | ||
Miller VA, Werner-Lin A, Walser SA, Biswas S, Bernhardt BA. An observational study of children’s involvement in informed consent for exome sequencing research. J Empir Res Hum Res Ethics. 2017;12(1):6–13. | ||
Stivers T. Physician-child interaction: when children answer physicians’ questions in routine medical encounters. Patient Educ Couns. 2012;87(1):3–9. | ||
Wissow LS, Roter D, Bauman LJ, et al. Patient-provider communication during the emergency department care of children with asthma. The National Cooperative Inner-City Asthma Study, National Institute of Allergy and Infectious Diseases, NIH, Bethesda, MD. Med Care. 1998;36(10):1439–1450. | ||
Miller VA, Baker JN, Leek AC, Drotar D, Kodish E. Patient involvement in informed consent for pediatric phase I cancer research. J Pediatr Hematol Oncol. 2014;36(8):635–640. | ||
Stivers T, Majid A. Questioning children: interactional evidence of implicit bias in medical interviews. Soc Psychol Q. 2007;70(4):424–441. | ||
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. | ||
Roter D, Larson S. The Roter interaction analysis system (RIAS): utility and flexibility for analysis of medical interactions. Patient Educ Couns. 2002;46(4):243–251. | ||
Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol Assess. 1994;6(4):284–290. | ||
Miller VA, Feudtner C, Jawad AF. Children’s decision-making involvement about research participation: associations with perceived fairness and self-efficacy. J Empir Res Hum Res Ethics. 2017;12(2):87–96. | ||
Simonian SJ, Tarnowski KJ, Park A, Bekeny P. Child, parent, and physician perceived satisfaction with pediatric outpatient visits. J Dev Behav Pediatr. 1993;14(1):8–12. | ||
Curran PJ, West SG, Finch JF. The robustness of test statistics to nonnormality and specification error in confirmatory factor analysis. Psychol Methods. 1996;1(1):16–29. | ||
Coyne I, Gallagher P. Participation in communication and decision-making: Children and young people’s experiences in a hospital setting. J Clin Nurs. 2011;20(15–16):2334–2343. | ||
Hsiao JL, Evan EE, Zeltzer LK. Parent and child perspectives on physician communication in pediatric palliative care. Palliat Support Care. 2007;5(4):355–365. | ||
Tates K, Meeuwesen L. Doctor-parent-child communication. A (re) view of the literature. Soc Sci Med. 2001;52(6):839–851. | ||
Williams S, Weinman J, Dale J. Doctor-patient communication and patient satisfaction: a review. Fam Pract. 1998;15(5):480–492. | ||
Street RL Jr, Makoul G, Arora NK, Epstein RM. How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ Couns. 2009;74(3):295–301. | ||
Coburn SS, Eakin MN, Roter D, et al. Patient-provider communication in nephrology care for adolescents and young adults. Patient Educ Couns. 2017;100(9):1680–1687. | ||
Antal H, Hossain MJ, Hassink S, et al. Audio-video recording of health care encounters for pediatric chronic conditions: observational reactivity and its correlates. J Pediatr Psychol. 2015;40(1):144–153. | ||
Swedlund MP, Schumacher JB, Young HN, Cox ED. Effect of communication style and physician-family relationships on satisfaction with pediatric chronic disease care. Heal Commun. 2012;27(5):498–505. | ||
Sarstedt M, Wilczynski P. More for Less? A Comparison of single-item and multi-item measures. Die Betriebswirtschaft. 2009;69(2):211–227. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.