")
Back to Journals » Patient Preference and Adherence » Volume 15
A Pilot Australian Pharmacist Health Coaching Trial of Participants with Poorly Controlled Hypertension: A Qualitative Study of Participants’ and Coaches’ Experiences
Authors Singh HK , Kennedy G , Stupans I
Received 5 November 2020
Accepted for publication 22 December 2020
Published 28 January 2021 Volume 2021:15 Pages 127—140
DOI https://doi.org/10.2147/PPA.S290403
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Harjit Kaur Singh,1 Gerard Kennedy,1– 3 Ieva Stupans1
1The School of Health and Biomedical Sciences, RMIT University, Bundoora, VIC, Australia; 2School of Science, Psychology and Sport, Federation University, Melbourne, Australia; 3Institute for Breathing and Sleep, Austin Health, Melbourne, Australia
Correspondence: Harjit Kaur Singh
School of Health and Biomedical Sciences, RMIT University, Bundoora, VIC 3083, Australia
Email [email protected]
Objective: An exploratory qualitative study was conducted to explore how stakeholders – participants and coaches experienced, and made sense of, being involved in coaching for people with poorly controlled hypertension.
Methods: Two pharmacists provided monthly health coaching sessions to twenty participants for three-months. Qualitative semi-structured interviews of participants were carried out by pharmacist coaches at baseline, one month, and at three months post-study completion. The pharmacist health coaches were also interviewed. Participant and pharmacist audio-recorded interviews were transcribed verbatim and analyzed thematically.
Results: Twenty participants with poorly controlled hypertension received health coaching. Analysis of the transcripts from participant interviews indicated the emergence of three main themes “beliefs about and management of hypertension”, “reflection on health goals” and “understanding of and experiences from health coaching”. Only one theme emerged from the pharmacist interviews: “logistics of health coaching in pharmacy”.
Conclusion: Analysis of interviews showed that participants experienced a variety of positive health changes. Changes included a better understanding of health coaching, more realistic beliefs about hypertension, and improved management of hypertension and health goals. Participants were also positive about their experiences of coaching. Interviews with the pharmacists revealed factors such as planning, teamwork, and time management which are related to the implementation and provision of health coaching in community pharmacy practice which could be overcome through consideration and planning.
Keywords: attitudes, opinions, behavior change, hypertension
Introduction
Hypertension is a chronic health condition leading to significant morbidity and mortality in Australia.1–3 Lifestyle behaviors, poor medication adherence, lack of disease knowledge, and insufficient monitoring are contributors to chronic illnesses such as hypertension.4 Increased knowledge about these factors can give individuals the confidence to change health behaviors and improve health-related quality of life (HRQoL).5 The management of hypertension is also influenced by adherence to anti-hypertensive medication; improvements can reduce the risk of complications and support the long-term positive prognosis of the condition.5
Community pharmacists are well situated to perform health promotion roles to improve patient’s management of chronic health conditions such as hypertension.6 These roles require an awareness of relevant problems, underlying symptoms, and a readiness to raise these with participants. It also requires active communication and counseling skills where the pharmacist is prepared to listen to, and respond constructively to, client’s questions and wishes.7 These attributes are collectively encapsulated within pharmacist health coaching services.8,9
Pharmacist health coaching is a promising professional pharmacy service, helping participants improve the management of chronic health conditions.8 Health coaching is a client-centered health promotion service provided to the participant by health care professionals for disease management.10 During health coaching, the stages of change (SOC) approach can be applied using a collaborative interaction between the participant and coach.10 Accountability for outcomes is shared equally by the participant and health professional, but it is the role of the coach to recognize the participant’s SOC and to subsequently, provide expert information to motivate the participant and facilitate progress towards goal attainment, positive knowledge, attitudinal, and behavioral change.8
Several, United States (US) based pharmacist health coaching studies have been reported in the literature. Some have specifically investigated the outcomes of pharmacist health coaching interventions in participants with hypertension and reported positive outcomes.8,11–14 The outcomes of the pharmacist health coaching studies11,13,14 reflect the usefulness of the service in assisting participants manage hypertension via health behavior and medication adherence education, and regular monitoring and follow-up.
However, most of these studies quantitatively assessed the effectiveness of pharmacist health coaching through clinical and non-clinical outcome measures, including validated medication adherence questionnaires, clinical targets, and cost-effectiveness. These studies did not include qualitative assessments, which are necessary to better understand and contextualize patients’ journeys and experiences of change because of health coaching.
The provision of health coaching services by pharmacists requires, consumer satisfaction and support to be assessed because they are integral to the initiation and utilization of primary care services. This also provides an opportunity for service improvement and consumer education about the benefits of the service.15 Furthermore, pivotal to service expansion within the community pharmacy are the attitudes and opinions of the pharmacists delivering the service because they can be both drivers and barriers to successful implementation. Previous pharmacist health coaching studies have not investigated the stakeholder’s experiences of community pharmacist health coaching interventions. Thus, this study aimed to explore how participants and pharmacist coaches experienced a coaching intervention for poorly controlled hypertension.
Materials and Methods
Study Design
We designed an exploratory qualitative semi-structured interviews study that examined how pharmacist health coaching changes behavior, knowledge, opinions, attitudes, and experiences of participants with poorly controlled essential hypertension.
The study also investigated the pharmacist health coaches’ perceptions of, and barriers/enablers to, pharmacist health coaching.
Ethics
The study conducted in Melbourne, Australia, was registered for inclusion in the Australia New Zealand Clinical Trials Registry (ANZCTR) on November 12, 2018, and received approval by the RMIT Human Research Ethics Committee (HREC project number: 21778) on December 21, 2018. All procedures performed in this study were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. There was no potential harm caused to participants, and confidentiality and anonymity was assured. Written informed consent was obtained from all participants.
Participants and Recruitment
Pharmacists from five community pharmacies in metropolitan Melbourne were approached to participate in the study. As the study involved regular visits to the pharmacy, pharmacies easily accessible to the researchers were approached.
From January 2019-June 2019, the pharmacists were asked to recruit participants they recognized as having poorly controlled hypertension for the pilot trial. Participants were included in the pilot trial if they met the following criteria: (1) aged over 18 years; (2) diagnosed with essential hypertension (≥ 140/90 mmHg) by a physician; (3) taking at least one antihypertensive; (4) recognized as having poorly controlled essential hypertension by the pharmacist (determined using dispensing history records to assess compliance and participant/pharmacy BP records); and (5) understands the English language. Participants were excluded from the trial if they were a current smoker or had stopped smoking within the last six months.
Pharmacist Training
Pharmacists were trained how to recognize and recruit eligible participants, how-to health coach participants using the SOC approach, and how to conduct the qualitative semi-structured interviews. The health coach training was conducted face-to-face at a time and place convenient for the pharmacist. Pharmacists were provided with a proforma, which provided further guidance for each health coaching session.
The Intervention
Participants received health coaching sessions from a community pharmacist once a month for three months. During these sessions, pharmacist health coaches provided the participants with education about hypertension, associated complications, treatment options, and clinical targets, to improve their knowledge and attitude about hypertension. During this time participants set goals specific to modifiable health behaviors diet, exercise, and medication management with the intent to improve management of hypertension. These goals were reviewed at subsequent health coaching sessions.
The pharmacist health coaches conducted qualitative semi-structured interviews with participants at baseline, at one month, and three- months -post-study completion. These interviews facilitated in-depth exploration of participants’ experiences about health coaching.
Except for the three-month post-study completion telephone interview, all pharmacist health coaching sessions, and interviews involved face-to-face contact. Pharmacist health coaches were also interviewed after the first health coaching session and after the completion of the study by one of the researchers. All interviews of participants and pharmacists in the study were audio-recorded for subsequent qualitative analysis.
The flexible interview schedule was developed to support the aims of the study which included a brief structured list of questions to prompt the pharmacist health coaches and the researchers to discuss key issues (Appendix). This identified broad areas to be covered together with examples of suggested probes, although the interviewer was also free to follow up on other issues that might arise and to probe and clarify responses. This approach led to discussions in which participants and pharmacists were able to identify and explain issues of importance to them rather than being limited by the narrower requirements of a structured questionnaire. Participants and pharmacists were given a full explanation about the study before the interviews and further written information was provided.
Data Analysis
The digitally recorded interviews with participants and pharmacists were transcribed verbatim and de-identified by one team member. The data was thematically analyzed by one researcher16 Two other researchers then participated in cross-checking and came to a consensus on areas of disagreement. Transcripts were read repeatedly, and salient terms and quotes were extracted. These were organized and consolidated to form categories. The categories were derived inductively; that is, from the data. The categories were then organized into main themes containing subcategories. After initial categorization, some subcategories were reorganized, renamed, and combined. The results are illustrated by quotes from the interview.
Each of the twenty participants was assigned a number to maintain their anonymity (given after each quotation). Saturation of themes occurred in participant interviews and no new themes emerged from the data. Given that only two pharmacists carried out the coaching theme saturation was not clearly defined in the transcripts from the pharmacist interviews. The analysis revealed that the pharmacists responded to the probe questions in a similar way.
Results
Two pharmacists consented to participate in the study and to the publication of anonymized responses. These pharmacists were female and had three and five years of pharmacy experience respectively. Due to the following barriers: too busy, lacked sufficient time, and because there was no remuneration, only two pharmacists from a single pharmacy agreed to participate in the trial.
Thirty participants were approached for the trial and screened, but only twenty-one participants met the inclusion criteria and consented to participate. Only one participant was lost to follow-up and did not complete the study. Overall, 60% of the participants were females and the average age was 64±13.7 years. Participants were taking one or more (1.4±0.7) antihypertensive medications at enrolment. The demographic characteristics of all the study participants are described in Table 1.
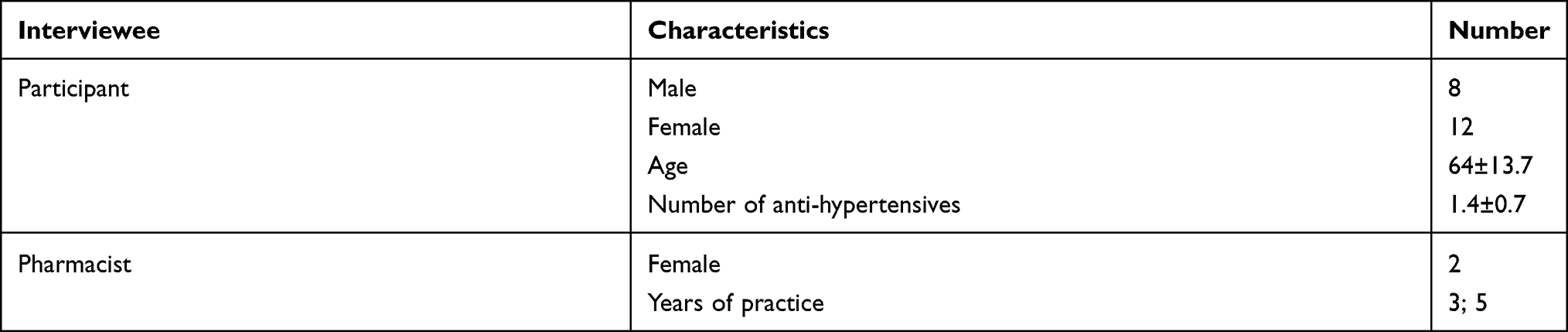 |
Table 1 The Demographic Characteristics of the Patients and Pharmacists |
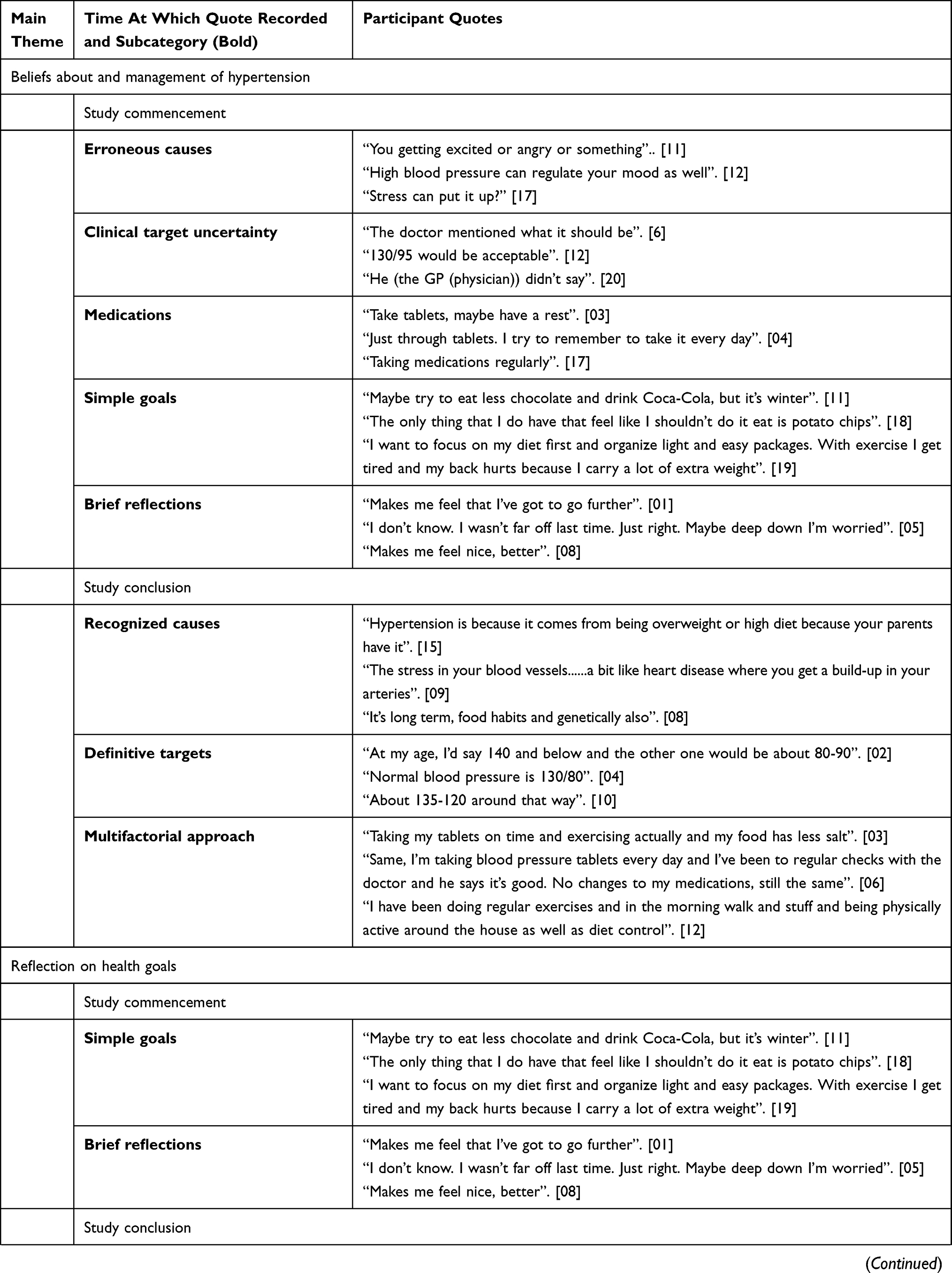
The duration of the interviews with participants and pharmacists averaged 8.5 minutes (range 2–34 min). After analysis of the participant interview transcripts from the beginning and the end of the study, the main themes that emerged were the “beliefs about and management of hypertension”, “reflection on health goals” and “understanding of and experiences from health coaching”. While the analysis of the transcripts from pharmacist interviews showed the emergence of one theme “logistics of health coaching in pharmacy”. Themes are presented in Table 2. Subcategories are described in the following text.
 |
 |
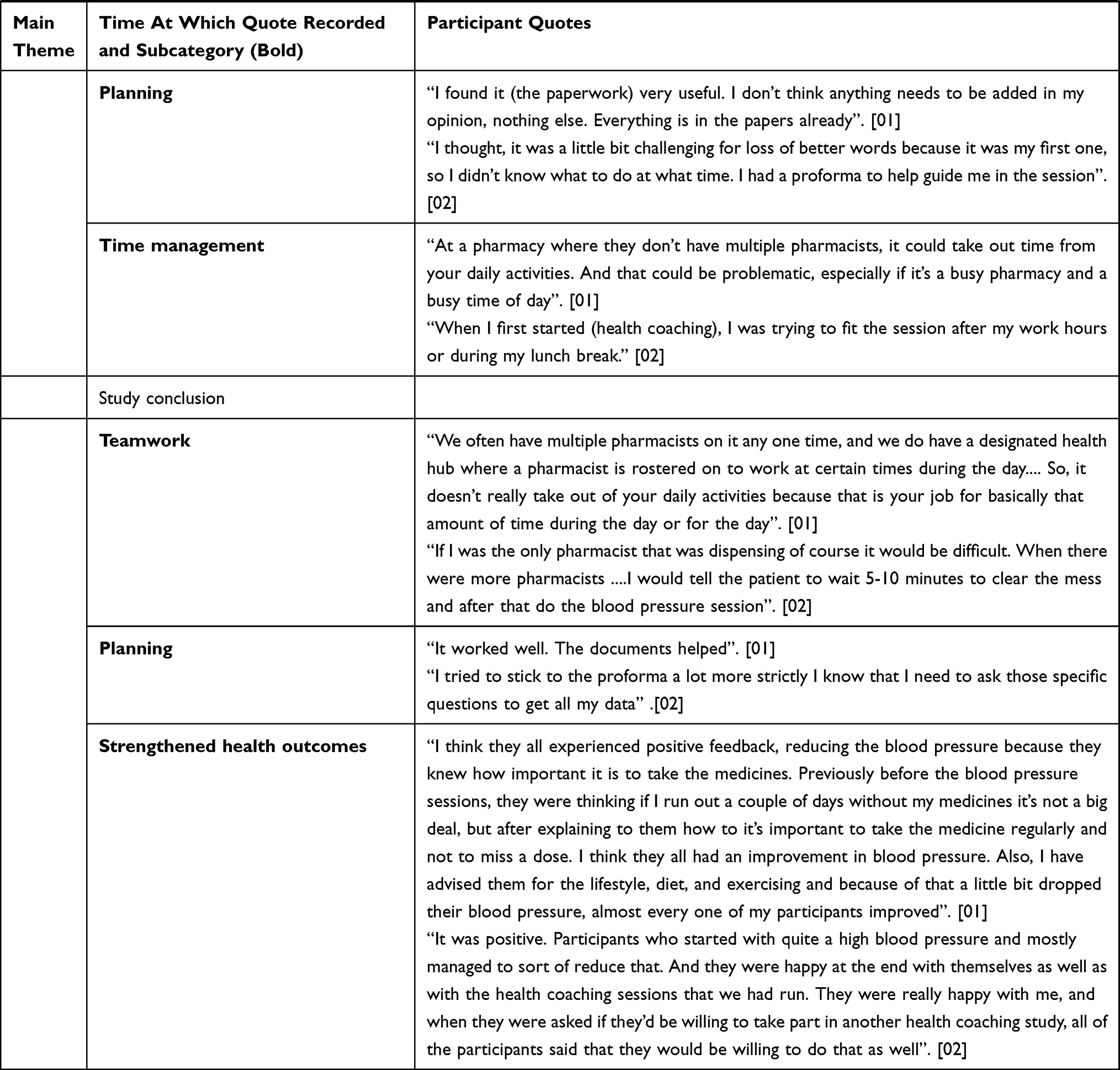 |
Table 2 Themes and Categories from Interviews |
Beliefs About and Management of Hypertension
Study Commencement
Some participants listed erroneous causes for hypertension at the beginning of the study, which showed uncertainty in knowledge and understanding about this chronic health condition. The causes listed were related to stress, mood, and wellbeing.
“You getting excited or angry or something”. [11]
“High blood pressure can regulate your mood as well”. [12]
“Stress can put it up?” [17]
When asked about what their blood pressure should be most participants expressed clinical target uncertainty. Participants referred to their general practitioners (GPs) during this time and mentioned having/not having been informed about this.
“The doctor mentioned what it should be”. [6]
“130/95 would be acceptable”. [12]
“He (the GP (physician)) didn’t say”. [20]
When questioned about how they managed their hypertension most participants showed a basic understanding as they referred predominately to using medications at the beginning of the study. Participants also discussed the commitment to taking antihypertensive medications regularly.
“Take tablets, maybe have a rest”. [03]
“Just through tablets. I try to remember to take it every day”. [04]
“Taking medications regularly”. [17]
Study Conclusion
The post-study interviews revealed that participants’ beliefs about the causes of hypertension had changed because of pharmacist health coaching. Participants were able to discuss the recognized causes of hypertension, which included being overweight, diet, lifestyle, and family history. Some were technical in their responses and described the clinical effects of hypertension within the body.
“Hypertension comes from being overweight or high diet because your parents have it”. [15]
“The stress in your blood vessels ... a bit like heart disease where you get a build-up in your arteries”. [09]
“It’s long term, food habits and genetically also”. [08]
At the completion of the study, pharmacist health coaching had also changed the participants’ awareness of clinical goals as they described definitive targets for hypertension.
“At my age, I’d say 140 and below and the other one would be about 80–90”. [02]
“Normal blood pressure is 130/80”. [04]
“About 135–120 around that way”. [10]
Through continued education and guidance during the health coaching session’s participants showed broader knowledge about hypertension and its management. Follow-up interviews indicated this as participants reported that the management of hypertension required a multifactorial approach. This included exercise, diet, regular blood pressure monitoring, and visits to the GP.
“Taking my tablets on time and exercising actually and my food has less salt”. [03]
“Same, I’m taking blood pressure tablets every day and I’ve been to regular checks with the doctor and he says it’s good. No changes to my medications, still the same”. [06]
“I have been doing regular exercises and in the morning walk and stuff and being physically active around the house as well as diet control”. [12]
Reflection on Health Goals
Study Commencement
When encouraged to nominate personal health goals specific to the modifiable health behaviors diet, exercise, and medication management to improve the management of their hypertension at the beginning of the health coaching study, participants articulated simple goals. These goals included making changes to predominantly one modifiable health behavior. For many participants, this was related to their diet.
“Maybe try to eat less chocolate and drink Coca-Cola, but it’s winter”. [11]
“The only thing that I do have that feel like I shouldn’t do it eat is potato chips”. [18]
“I want to focus on my diet first and organize light and easy packages. With exercise I get tired and my back hurts because I carry a lot of extra weight”. [19]
Upon follow-up at one month, the participant’s described brief reflections of their initial health goals, predominantly referring to their feelings and experiences.
“Makes me feel that I”ve got to go further”. [01]
“I don’t know. I wasn’t far off last time. Just right. Maybe deep down I’m worried”. [05]
Makes me feel nice, better”. [08]
Study Conclusion
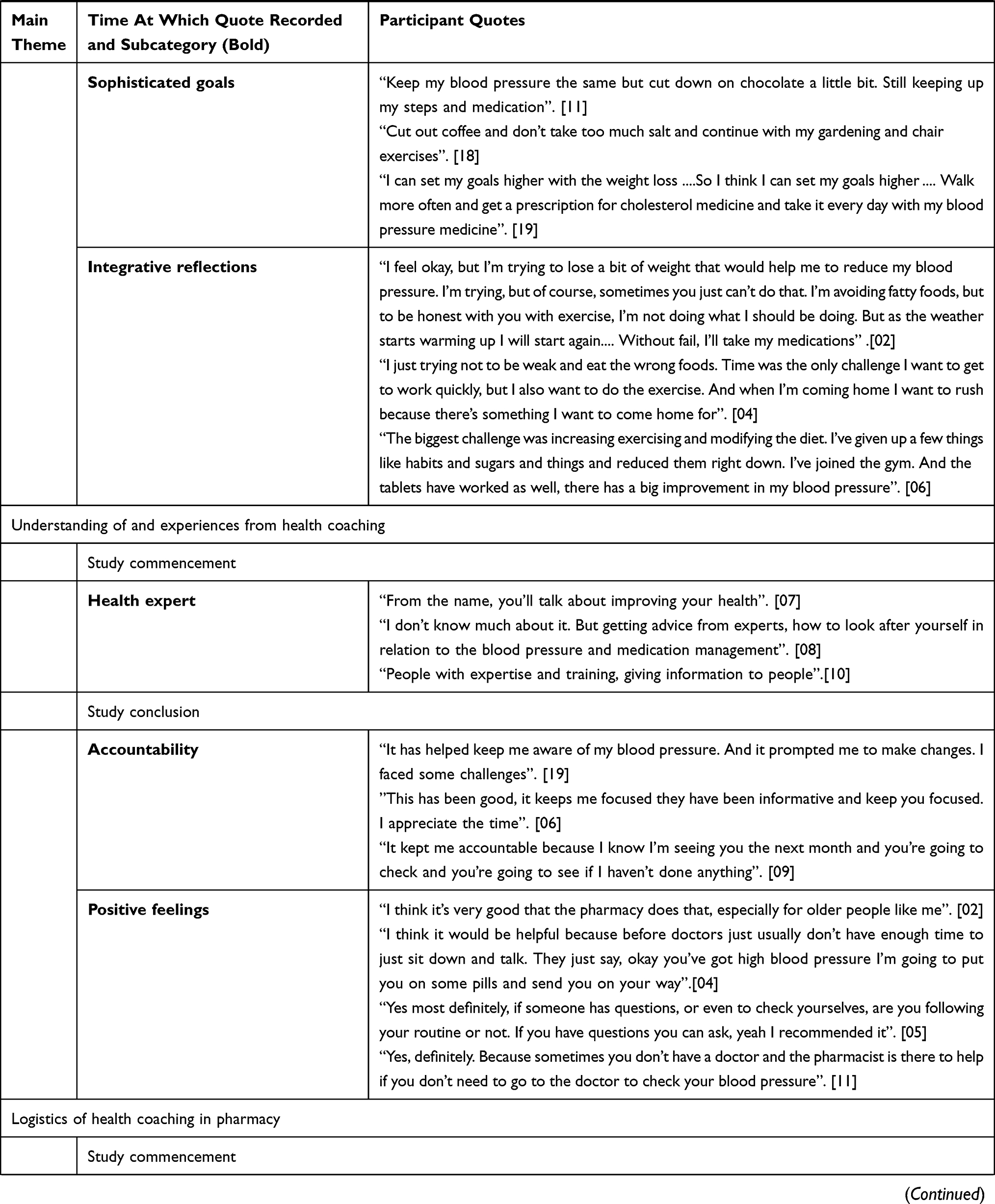
As the study progressed participant’s health goals became more sophisticated goals. They referred to making changes concurrently to the modifiable health behaviors including diet, exercise, and medication management.
“Keep my blood pressure the same but cut down on chocolate a little bit. Still keeping up my steps and medication”. [11]
“Cut out coffee and don’t take too much salt and continue with my gardening and chair exercises”. [18]
“I can set my goals higher with the weight loss ... So I think I can set my goals higher ... Walk more often and get a prescription for cholesterol medicine and take it every day with my blood pressure medicine”. [19]
Upon reflection about of their goals after the study, participant described integrative reflections. These acknowledgments included details about their feeling towards their goals, their accomplishments, and downfalls, as well as actions for the future.
“I feel okay, but I’m trying to lose a bit of weight that would help me to reduce my blood pressure. I’m trying, but of course, sometimes you just can’t do that. I’m avoiding fatty foods, but to be honest with you with exercise, I’m not doing what I should be doing. But as the weather starts warming up I will start again ... Without fail, I’ll take my medications”. [02]
“I just trying not to be weak and eat the wrong foods. Time was the only challenge I want to get to work quickly, but I also want to do the exercise. And when I’m coming home I want to rush because there’s something I want to come home for”. [04]
“The biggest challenge was increasing exercising and modifying the diet. I’ve given up a few things like habits and sugars and things and reduced them right down. I’ve joined the gym. And the tablets have worked as well, there has been a big improvement in my blood pressure”. [06]
Understanding of and Experiences from Health Coaching
Study Commencement
Most participants showed a basic understanding of health coaching at the beginning of the study. They acknowledged that health coaches were extensively trained and were health experts. Participants recognized the value of pharmacist health coaching and that it was the coach’s obligation to provide expert advice to them on how to improve their blood pressure and medication management, with the intent to improve their health.
“From the name, you’ll talk about improving your health”. [07]
“I don’t know much about it. But getting advice from experts, how to look after yourself in relation to the blood pressure and medication management”. [08]
“People with expertise and training, giving information to people”. [10]
Study Conclusion
Participants understanding of health coaching and the process involved was seen to have progressed at the completion of the study. Patient awareness of and the importance of monitoring hypertension was enhanced, as they described the process of health coaching as collaborative and having stimulated accountability to make changes for their health.
“It has helped keep me aware of my blood pressure. And it prompted me to make changes. I faced some challenges”. [19]
“This has been good; it keeps me focused they have been informative and it keeps you focused. I appreciate the time”. [06]
“It kept me accountable because I know I’m seeing you the next month and you’re going to check and you’re going to see if I haven’t done anything”. [09]
At three months post-study completion, participants were asked about their experiences of the health coaching sessions, if they had learned anything new, and about the provision of the service by other pharmacists in the future. All the participants shared and described positive feelings about the service.
“I think it’s very good that the pharmacy does that, especially for older people like me”. [02]
“I think it would be helpful because before doctors usually don’t have enough time to just sit down and talk. They just say, okay you’ve got high blood pressure I’m going to put you on some pills and send you on your way”. [04]
“Yes most definitely, if someone has questions, or even to check yourselves, are you following your routine or not. If you have questions you can ask. I recommend it”. [05]
“Yes, definitely. Because sometimes you don’t have a doctor and the pharmacist is there to help if you don’t need to go to the doctor to check your blood pressure”. [11]
Logistics of Health Coaching in Pharmacy
Study Commencement
When asked about their initial health coaching session, pharmacists stated that considerable planning was required to ensure that they conducted the sessions properly and discussed all the relevant information. They referred to the proformas that were provided, which gave some guidance during the health coaching process.
“I found it (the paperwork) very useful. I don’t think anything needs to be added in my opinion. Everything is in the papers already”. [01]
“I thought, it was a little bit challenging for loss of better words because it was my first one, so I didn’t know what to do at what time. I had a proforma to help guide me in the session”. [02]
During this time, the pharmacists also stated that time management played a key role in scheduling health coaching appointments whilst also allowing them to keep up with their conventional duties in the pharmacy. They also acknowledged that for a pharmacy with limited staffing the provision of services such as health coaching might not be feasible.
“At a pharmacy where they don’t have multiple pharmacists, it could take out time from your daily activities. And that could be problematic, especially if it’s a busy pharmacy and a busy time of day”. [01]
“When I first started (health coaching), I was trying to fit the session after my work hours or during my lunch break”. [02]
Study Conclusion
Interviews with pharmacists at the completion of the study showed that the pharmacists acknowledged and appreciated the teamwork at their pharmacy, which at times allowed them to work health coaching sessions around their conventional duties. The pharmacists also indicated that adequate staff rostering also made one-on-one health coaching sessions with participants possible.
“We often have multiple pharmacists on it any one time, and we do have a designated health hub where a pharmacist is rostered on to work at certain times during the day ... So, it doesn’t really take out of your daily activities because that is your job for basically that amount of time during the day or for the day”. [01]
“If I was the only pharmacist that was dispensing of course it would be difficult. When there were more pharmacists ... I would tell the participant to wait 5-10 minutes to clear the mess and after that do the blood pressure session”. [02]
Similarly, to interviews at the beginning of the study, during post-study interviews pharmacists reported that planning the health coaching sessions adequately made it convenient for them to administer. This also involved adhering to the proforma, which allowed them to collect all the appropriate information for that session.
“It worked well. The documents helped”. [01]
“I tried to stick to the proforma a lot more strictly I know that I need to ask those specific questions to get all my data”. [02]
At the completion of the study, interviews with the pharmacists revealed that they had positive views on the impact that health coaching had on the participants. They reported that participants had experienced strengthened health outcomes. These outcomes included reaching lifestyle goals, clinical targets as well as satisfaction towards the health coaching service.
“I think they all experienced positive feedback, reducing their blood pressure because they knew how important it is to take the medicines. Previously before the blood pressure sessions, they were thinking a couple of days without my medicines is not a big deal, but after explaining to them the importance of taking the medicine regularly and not to miss a dose, I think they all had an improvement in blood pressure. Also, I have advised them about lifestyle, diet, and exercising, and because of that their blood pressure dropped, almost every one of my participants improved”. [01]
“It was positive. Participants who started with quite a high blood pressure mostly managed to reduce that. And they were happy at the end with themselves as well as with the health coaching sessions that we had run. They were really happy with me, and when they were asked if they’d be willing to take part in another health coaching study, all of the participants said that they would be willing to do that as well”. [02]
Discussion
This study provides an extensive and consistent perspective of the stakeholders involved in pharmacist health coaching interventions, which has not previously been reported in the literature. It presents the participant’s, and pharmacist’s sentiments, attitudes, and experiences about health coaching before, during and after a pilot health coaching study. It also introduces the logistical pros and cons that may need to be addressed if health coaching is to be established as a professional pharmacy service in Australia. Many of the views collected during this study align with the findings from a study that previously evaluated the integration and feasibility of health coaching in the Australian community pharmacy.17
Beliefs About and Management of Hypertension
The results also iterate the strong connection between participant engagement and desirable participant outcomes.21 Pharmacist health coaching strengthened participant interest and health confidence; this was reflected by changes to beliefs about hypertension. Participants were initially uncertain about the causes of and the clinical targets for hypertension. This lack of understanding and health confidence can inevitably lead to potentially avoidable complications and hospital admissions.21 This correlated with participant’s minimalistic explanations about their management of hypertension, involving mainly the use of medications. Medication non-adherence is one of the most common preventable causes of cardiovascular events in individuals with hypertension.26 However, interventions involving both pharmacological and non-pharmacological approaches are imperative to achieving maximum therapeutic benefits to disease management.27 The concluding outcomes of pharmacist health coaching support these findings, whereby, participant’s health goals changed after regular health coaching sessions. Participants subsequently described the management of their hypertension to involve a multifactorial approach, which included making changes to their exercise, diet, regular blood pressure monitoring, and having regular visits with their GP. This is an encouraging result given that the management of chronic health conditions is complex and requires comprehensive management plans to foster a greater focus on self-management of hypertension.28 It also indicates that pharmacist health coaching improved participant’s health knowledge and progress through the SOC. These results are consistent with a physical activity hospital-based health promotion service study provided to participants with type 2 diabetes. In this study, exercise specialists individualized physical activity counseling based on the SOC model, and follow-up occurred at baseline and three-months. The results showed that a statistically significant difference was found in the participants’ stage of change, 59% (p< 0.001) of participants made a positive change to their physical activity status.29 Although similar outcomes were apparent from both studies, the present study indicates that pharmacists are equally qualified to provide health promotion services and from an easily accessible location. This was reflected by confident responses at the completion of the study describing recognized causes and definitive targets for hypertension. These results are also likely to coincide with improvements in clinical outcomes, given that participant knowledge and awareness of hypertension are important factors in monitoring and achieving blood pressure control.22,23 The outcomes of previous research investigating participant health confidence also support these findings. In one study, participant health confidence was associated with participant satisfaction and positively reported self-related health status.24 In another study, it was found that engaging participants in the self-management of their blood pressure enhanced their confidence in health management and improved their HRQoL.25
In recognizing the relationship between health confidence, self-rated health status, and participant satisfaction, health professionals can better meet their participant’s needs.24 Furthermore, given that participant satisfaction is used as an indicator of the quality of health services,24 it is reasonable to suggest that participants were satisfied with the health coaching services provided to them and that their expectations for the service were met. This is a promising finding as it provides the groundwork for the expansion of pharmacist health coaching services in Australia.
Reflection on Health Goals
The process of health coaching requires participants to establish personal goals at commencement, thereby motivating health improvement.8 Despite being prompted to consider goals specific to each modifiable health behavior: diet, exercise, and medication management during the health coaching sessions participants initially composed simple goals referring to modifying a single health behavior. However, through education, advice, collaborative discussion, and goal setting during regular health coaching sessions, periodic follow-up of the participants indicated that their reflections changed from being brief reflections at the beginning of the study to integrative reflections at the completion of the study. This suggests that pharmacist health coaching raised participant’s awareness about their health enabling them to recognize the challenges they faced towards health improvement. It also facilitated them to build on former health goals, empowering them to subsequently set sophisticated goals as the study progressed. This showed that participants improved their health literacy allowing them to reflect on their situation and associate their actions (or inaction) with their health.30 This mirrors findings from similar programs involving integrated models of patient care engaging a health coach in conjunction and complementary to a health professional.30,31 However, the present study indicates that pharmacists can merge professional roles being a health professional and health coach simultaneously while also producing favorable patient outcomes.
Understanding of and Experiences from Health Coaching
Interviews with the participants at the beginning of the study revealed that although they had a basic understanding of health coaching, they had misconceptions about the process involved. Participants initially described health coaching as a pharmacist-led process during which they failed to describe their own participation. However, at the completion of the pilot trial patient’s thoughts had changed and they described themselves as being more accountable for their health and considered the process of health coaching as collaborative. Studies have shown that participant accountability and involvement in health care decision making empowers them to improve health outcomes through the services that they receive.18 The changes in participant thoughts reflect favorable remodeling of attitudes and behaviors towards health management and services as an outcome of pharmacist health coaching within the community pharmacy. These outcomes are also backed by studies within health psychology that show that as affective associations; feelings associated with specific health behaviors, became more positive, as behaviors associated with physical activity increased.19,20 This suggests that incorporating models to encourage participants to modify health behaviors into clinical interventions would be favorable for participants.19
At the completion of the study, participants exhibited positive feelings about the service and acknowledged several favorable outcomes because of the service. For example, some participants reported that before health coaching with the pharmacist, they had been unclear why they were taking their medicines (or what the medicines were meant to treat) and now felt more knowledgeable about their medicines. It was also apparent from the interviews that participants appreciated the role of the pharmacist in facilitating improvements to their hypertension and would go back to the pharmacist to obtain advice from them in the future. Participants also acknowledged that the service would benefit others; by increasing health knowledge and reducing the burden on doctors if it were offered by additional pharmacies. The findings highlight that the coaching relationship was an important aspect of the health coaching experience. The role played by the pharmacist coach in the interpersonal relationship, the connection, and interactions with the coach, and how participants felt in that interaction, were important factors of this relationship. At a more practical level, these results support previous studies that discuss the value of pharmacy services individualized to patients,32,33 and the acceptance of and satisfactory experiences of patients who receive these unique services.33 Conversely, in health coaching studies lacking face-to-face communication, relationship development was at times hampered.31
Logistics of Health Coaching in Pharmacy
The changes in participant behavior, health beliefs, opinions, attitudes, and experiences were consistent with the findings from the post-study interviews with the pharmacists. Pharmacists observed that participant’s outcomes had changed alongside health coaching. These improvements are related to both clinical targets; blood pressure, and non-clinical targets; beliefs, knowledge, and attitudes. Considering the promising results they facilitated in participants, pharmacists also expressed positive views on the provision of health coaching within the community pharmacy.
Despite the benefits, pharmacists also described several logistical aspects that would need to be considered for health coaching to become an established professional pharmacy service available through community pharmacies in Australia. They described the need for careful planning relating to the scheduling and the content of the health coaching sessions. It has been previously noted that the use of motivational strategies and behavior change techniques that are tailored to meet individual preferences to facilitate patients to reach goals can be challenging in a time-limited consultation especially in the absence of specific training in these techniques.31 However, pharmacists acknowledged the study proformas were beneficial, during busy periods as they overcame the need to plan discussion points for sessions and reiterated the concepts learned during training. Proformas are structured documents that may serve a role in guiding health professionals to reinforce particular educational points to patients34 and may also improve documentation of key information.35 The utilization of proformas to guide health coaching sessions may account for the improvements to participants understanding of health coaching, beliefs about hypertension, and management of hypertension at the completion of the study as it prompted pharmacists to reiterate key points about hypertension to participants and also facilitated the monitoring of clinical and non-clinical information. Although the need to plan health coaching sessions were managed using proformas, the scheduling aspect required time management, teamwork, and cooperation within the pharmacy team. The pharmacists alluded to the need to ensure the conventional pharmacy operations continue without interruption from the administration of professional pharmacy services such as health coaching. Similar points were described by the pharmacy owner suggesting that consideration of these aspects is imperative if pharmacy health coaching is to be established as a professional pharmacy service in Australia. Similarly, these issues have also been raised within previous literature investigating the implementation of professional services in Australian community pharmacies.36
Clinical Implications
Consumer evaluations offer useful insight into the performance of health care providers and their services,24 as well as patient willingness to accept services.37 It also provides direction for service improvement pre and -post-initiation.38 The findings from the study indicated that pharmacist health coaching was associated positively with changed participant’s opinions, attitudes, and experiences towards the service as well as their knowledge about and their management of hypertension. Research has previously shown that interventions based on changing participants’ attitudes, knowledge, and experience can positively change their self-care behaviors towards the management of chronic health conditions.39 The present study supports this finding, whereby the provision of pharmacist health coaching over three months changed beliefs and experiences in participants with hypertension. This may be the underlying reason for the improvements to participants’ clinical health outcomes in previous studies,11,13,14 enabling them to be sustained long-term.10 As such pharmacist health coaching could be used for the management of other chronic health conditions; a facilitator to the implementation of pharmacist health coaching within Australian community pharmacies.17 In addition, the study identifies areas in which community pharmacists can focus on, such as the causes, and holistic management of hypertension when providing conventional pharmacy services to participants. These views add a valuable overview for guiding the training of pharmacists to health coach, the process of health coaching as well as the integration of the service into community pharmacy practice. It also encourages the expansion of the pharmacist’s role towards patient-focused services, which could also be integrated into Australian GP practices to support GP workloads and to improve the quality of patient care.
Although these outcomes coincided with the opinions and attitudes of the pharmacist health coaches, some logistical factors to the implementation of the service were also identified, which could be overcome through careful consideration and planning and were not considered barriers to the provision of health coaching in Australian community pharmacies.
Limitations
A limitation to this study was its small sample size, though is appropriate given that research involved a pilot trial. Another limitation to the present study is that only a single pharmacy site agreed to and recruited participants for the study. Despite these limitations, however, the present findings are novel - this is the first study to examine the experiences of participants and pharmacists towards health coaching. The results provide a rationale for future larger-scale studies.
Conclusion
This paper presents the experiences of stakeholders involved with community pharmacy health coaching which have not previously been investigated. Analysis of interview transcripts at the beginning and at the completion of the pharmacist health coaching program presented the participant’s journey; they experienced a variety of changes, which otherwise may not have been revealed by quantitative outcome measures used in conventional health coaching studies. Participant’s understanding of health coaching, beliefs about hypertension, management of hypertension improved. Their reflections on and experiences from the service were also positive. In the interviews with the pharmacists, the positive outcomes the participants experienced were reiterated, but they also revealed several logistical issues that would need to be considered to facilitate the implementation of the service in Australia. Together, this suggests there may be merit in further developing pharmacy-based health coaching services for participants with hypertension and other chronic health conditions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arima H, Barzi F, Chalmers J. Mortality patterns in hypertension. J Hypertens. 2011;29:S3–S7. doi:10.1097/01.hjh.0000410246.59221.b1
2. Kjeldsen SE. Hypertension and cardiovascular risk: general aspects. Pharmacol Res. 2018;129:95–99. doi:10.1016/j.phrs.2017.11.003
3. Sharman JE, Stowasser M. Australian Association for Exercise and Sports Science Position Statement on Exercise and Hypertension. J Sci Med Sport. 2009;12(2):252–257. doi:10.1016/j.jsams.2008.10.009
4. Yi-Bing W, De-gui K, Long-Le M, Le-xin W. Patient related factors for optimal blood pressure control in patients with hypertension.. Afr Health Sci. 2013;13(3):579–583. doi:10.4314/ahs.v13i3.8
5. Khalesi S, Irwin C, Sun J. Dietary patterns, nutrition knowledge, lifestyle, and health-related quality of life: associations with anti-hypertension medication adherence in a sample of Australian adults. High Blood Pressure Cardiovasc Prevent. 2017;24(4):453–462. doi:10.1007/s40292-017-0229-9
6. George PP, Molina JAD, Cheah J, Chan SC, Lim BP. The evolving role of the community pharmacist in chronic disease management - a literature review.. Ann Acad Med Singapore. 2010;39(11):861–867.
7. Smith F. Community pharmacists and health promotion: a study of consultations between pharmacists and clients. Health Promot Int. 1992;7(4):249–255. doi:10.1093/heapro/7.4.249
8. Singh HK, Kennedy GA, Stupans I. A systematic review of pharmacy health coaching and an evaluation of patient outcomes. Res Soc Admin Pharm. 2019;15(3):244–251. doi:10.1016/j.sapharm.2018.04.012
9. Singh HK, Kennedy GA, Stupans I. Competencies and training of health professionals engaged in health coaching: A systematic review. Chronic Illn. 2020;1742395319899466. doi:10.1177/1742395319899466
10. Lonie JM, Austin Z, Nguyen R, Gill I, Tsingos-Lucas C. Pharmacist-based health coaching: a new model of pharmacist-patient care. Res Soc Admin Pharm. 2017;13(3):644–652. doi:10.1016/j.sapharm.2016.06.015
11. Luder H, Frede S, Kirby J, King K, Heaton P. Health Beliefs Describing Patients Enrolling in Community Pharmacy Disease Management Programs. J Pharm Pract. 2016;29(4):374–381. doi:10.1177/0897190014566311
12. Herborg H, Haugølle LS, Sørensen L, Rossing C, Dam P. Developing a generic, individualised adherence programme for chronic medication users. Pharm Pract (Granada). 2008;6(7):148–157. doi:10.4321/S1886-36552008000300006
13. DiDonato KL, May JR, Lindsey CC. Impact of wellness coaching and monitoring services provided in a community pharmacy. J Am Pharm Assoc. 2013;53(1):14–21. doi:10.1331/JAPhA.2013.11227
14. Wertz D, Hou L, DeVries A, et al. Clinical and economic outcomes of the Cincinnati Pharmacy Coaching Program for diabetes and hypertension. Managed Care. 2012;21(3):44–54.
15. Wirth F, Tabone F, Azzopardi LM, Gauci M, Zarb-Adami M, Serracino-Inglott A. Consumer perception of the community pharmacist and community pharmacy services in Malta. J Pharm Health Serv Res. 2010;1(4):189–194. doi:10.1111/j.1759-8893.2010.00034.x
16. Maguire M, Delahunt B. Doing a thematic analysis: A practical, step-by-step guide for learning and teaching scholars. AISHE-J. 2017;9:3.
17. Singh HK, Kennedy GA, Stupans I. Pharmacist health coaching in Australian community pharmacies: what do pharmacy professionals think? Health Soc Care Community. 2020;28(4):1190–1198. doi:10.1111/hsc.12952
18. Vahdat S, Hamzehgardeshi L, Hessam S, Hamzehgardeshi Z. Patient involvement in health care decision making: a review. Iran Red Crescent Med J. 2014;16(1):1. doi:10.5812/ircmj.12454
19. Kiviniemi MT, Voss-Humke AM, Seifert AL. How do i feel about the behavior? The interplay of affective associations with behaviors and cognitive beliefs as influences on physical activity behavior.. Health Psychol. 2007;26(2):152. doi:10.1037/0278-6133.26.2.152
20. Van Cappellen P, Rice EL, Catalino LI, Fredrickson BL. Positive affective processes underlie positive health behaviour change. Psychol Health. 2018;33(1):77–97. doi:10.1080/08870446.2017.1320798
21. Wasson J, Coleman EA. Health confidence: an essential measure for patient engagement and better practice.. Fam Pract Manag. 2014;21(5):8–12.
22. Lam JY, Guirguis LM. Patients´ blood pressure knowledge, perceptions and monitoring practices in community pharmacies. Pharm Pract. 2010;8(3):187. doi:10.4321/S1886-36552010000300006
23. Alexander M, Gordon NP, Davis CC, Chen RS. Patient knowledge and awareness of hypertension is suboptimal: results from a large health maintenance organization. J Clin Hyper. 2003;5(4):254–260. doi:10.1111/j.1524-6175.2003.01963.x
24. Zhang Y, Rohrer J, Borders T, Farrell T. Patient satisfaction, self-rated health status, and health confidence: an assessment of the utility of single-item questions. Am J Med Quality. 2007;22(1):42–49. doi:10.1177/1062860606296329
25. Johnson ML, Zimmerman L, Welch JL, Hertzog M, Pozehl B, Plumb T. Patient activation with knowledge, self-management and confidence in chronic kidney disease. J Ren Care. 2016;42(1):15–22. doi:10.1111/jorc.12142
26. Pladevall M, Brotons C, Gabriel R, et al. Multicenter cluster-randomized trial of a multifactorial intervention to improve antihypertensive medication adherence and blood pressure control among patients at high cardiovascular risk (the COM99 study). Circulation. 2010;122(12):1183–1191. doi:10.1161/CIRCULATIONAHA.109.892778
27. DeSimone ME, Crowe A. Nonpharmacological approaches in the management of hypertension. J Am Acad Nurse Pract. 2009;21(4):189–196. doi:10.1111/j.1745-7599.2009.00395.x
28. Lawn S, Schoo A. Supporting self-management of chronic health conditions: common approaches. Patient Educ Couns. 2010;80(2):205–211. doi:10.1016/j.pec.2009.10.006
29. Taket A, Crichton N, Gauvin S. DOROTHEA: diabetes on referral option to healthy exercise for adults. Evaluating the effects of DOROTHEA: a pilot activity promotion scheme for adults with type 2 diabetes in Lambeth and Southwark. 2006.
30. Liddy C, Johnston S, Irving H, Nash K, Ward N. Improving awareness, accountability, and access through health coaching: qualitative study of patients‘ perspectives.. Canadian Family Phys Med De Famille Canadien. 2015;61(3):e158–e164.
31. Hinman RS, Delany CM, Campbell PK, Gale J, Bennell KL. Physical therapists, telephone coaches, and patients with knee osteoarthritis: qualitative study about working together to promote exercise adherence. Phys Ther. 2016;96(4):479–493. doi:10.2522/ptj.20150260
32. McMillan SS, Kelly F, Sav A, King MA, Whitty JA, Wheeler AJ. Australian community pharmacy services: a survey of what people with chronic conditions and their carers use versus what they consider important. BMJ Open. 2014;4(12):12. doi:10.1136/bmjopen-2014-006587
33. Wood K, Gibson F, Radley A, Williams B. Pharmaceutical care of older people: what do older people want from community pharmacy? Int J Pharm Pract. 2015;23(2):121–130. doi:10.1111/ijpp.12127
34. Pace-Bardon M, Bilocca D, Jackson K, Bradding P, Green RM. 11 the Use of Asthma Care Bundle Proformas Can Improve Quality of Care in Acute Asthma Admissions. BMJ Publishing Group Ltd; 2017.
35. Thompson A. Do post-take ward round proformas improve communication and influence quality of patient care? Postgrad Med J. 2004;80(949):675–676. doi:10.1136/pgmj.2003.016097
36. Moullin JC, Sabater-Hernández D, Benrimoj SI. Qualitative study on the implementation of professional pharmacy services in Australian community pharmacies using framework analysis. BMC Health Serv Res. 2016;16(1):439. doi:10.1186/s12913-016-1689-7
37. Suh D-C. Consumers’ willingness to pay for pharmacy services that reduce risk of medication-related problems. J Am Pharm Assoc. 2000;40(6):818–827. doi:10.1016/S1086-5802(16)31129-9
38. Panvelkar PN, Saini B, Armour C. Measurement of patient satisfaction with community pharmacy services: a review. Pharm World Sci. 2009;31(5):525–537. doi:10.1007/s11096-009-9311-2
39. Gohar F, Greenfield SM, Beevers DG, Lip GY, Jolly K. Self-care and adherence to medication: a survey in the hypertension outpatient clinic. BMC Complement Altern Med. 2008;8(1):4. doi:10.1186/1472-6882-8-4
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.