")
Back to Journals » Journal of Healthcare Leadership » Volume 15
A Needs Assessment Survey of Division Chiefs at an Academic Children’s Hospital
Authors Johnston DL, Samson L , Jabbour M
Received 18 October 2022
Accepted for publication 9 January 2023
Published 17 January 2023 Volume 2023:15 Pages 11—18
DOI https://doi.org/10.2147/JHL.S393177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Donna L Johnston,1 Lindy Samson,2 Mona Jabbour2
1Division of Hematology/Oncology, CHEO, University of Ottawa, Ottawa, ON, Canada; 2CHEO, University of Ottawa, Ottawa, ON, Canada
Correspondence: Donna L Johnston, Division of Hematology/Oncology, Children’s Hospital of Eastern Ontario, 401 Smyth Road, Ottawa, ON, K1H 8L1, Canada, Tel +1-613-737-7600 ext 2210, Fax +1-613-738-4828, Email [email protected]
Purpose: The Division Chief at an academic health sciences centre has many leadership roles and responsibilities. There are no data on leadership training needs for Division Chiefs, and so we sought to design and implement a needs assessment for pediatric Division Chiefs at CHEO, a pediatric academic health sciences centre in Eastern Ontario, Canada.
Methods: A needs assessment survey was developed with the aim to document demographics, preparedness for the role of Division Chief and desired leadership training for the role. This survey was piloted, revised and then distributed to all the Division Chiefs at our institution. The results of each question were collated, and simple descriptive statistics were calculated.
Results: The survey was completed by 22 of 31 Division Chiefs. The majority of respondents were from the Department of Pediatrics (63.6%), followed by Surgery (20%), Psychiatry (3.3%) and Laboratory Medicine (3.3%). Their mean length of time as Division Chief was 5.5 years. Seventy-seven percent had concurrent leadership roles in addition to the role of Division Chief. None felt they were very well prepared for the role, five felt they were somewhat well prepared, nine were neutral, five were somewhat unprepared and three were very unprepared for the role. Half of the respondents received mentoring, either formal or informal, for their role and all but one felt that formal mentoring would have been useful. In terms of desired training, the Division Chiefs felt they had the most knowledge and skills in patient safety. All wanted training in developing divisional budgets, and many desired training in supporting the academic mission of the Division.
Conclusion: Overall, this needs assessment identified an unmet need for leadership training and development among Division Chiefs. The findings are being used to optimize onboarding of Division Chiefs and an ongoing leadership development program targeted at this group.
Keywords: needs assessment, Division Chiefs, leadership training
Introduction
An academic health sciences centre is an educational and healthcare institute formed when a health professional school is combined with an affiliated teaching hospital. Within a pediatric academic health sciences centre, there are many medical departments and within departments often several divisions. Each division is led by a Division Chief, who is usually appointed by the organizations’ Board of Directors. Job descriptions for Division Chiefs can be broad, including both hospital and university related mandates. Moreover, as with many health system leadership roles, the expectations, responsibilities and accountabilities of Division Chiefs have steadily evolved, along with the complexities of health system and health professional governance. This often includes oversight of quality and safety of patient care, academic career development and shared responsibilities for operational oversight and resource allocation within their service area. Despite this, there is insufficient training provided to individuals taking over this role within many institutions, and the individuals rely on other leadership experience and training in order to be successful in the role.
Effective leadership at the Division Chief level is important for several reasons. The overarching leadership role is to oversee the safety and quality of the care provided in the division, as well as overseeing career development and human resources issues of the medical staff within the division. This role also includes oversight of the educational and research activities of the division overall. The leadership provided in this role has a direct impact on the clinical and academic success of the members of the division and the quality of care provided within the organization. In order for physicians to be academically successful, they need to have the vision, support, time and resources to dedicate to their goals, and the Division Chief is instrumental in setting the stage for success in this regard. Optimizing the management and leadership skills for this role will have an impact on all members of the division and the division as a whole.
A needs assessment, with a focus on perceived needs, is an excellent educational tool to determine the training individuals feel would be helpful to them. In terms of leadership skills, previous needs assessments have been done in the areas of surgical education leadership,1 obstetrics and gynecology fellowship Program Directors,2 and gastroenterology Program Directors.3 These were used to identify training requirements for leadership roles for new Program Directors and provided valuable insight for individuals in those areas. However, there is no data on leadership training needs for Division Chiefs and so we sought to design and implement a needs assessment for pediatric Division Chiefs at our pediatric tertiary care academic health sciences centre in Eastern Ontario, CHEO. The purpose of this paper is to report on the identified training needs of Division Chiefs at our institution.
Materials and Methods
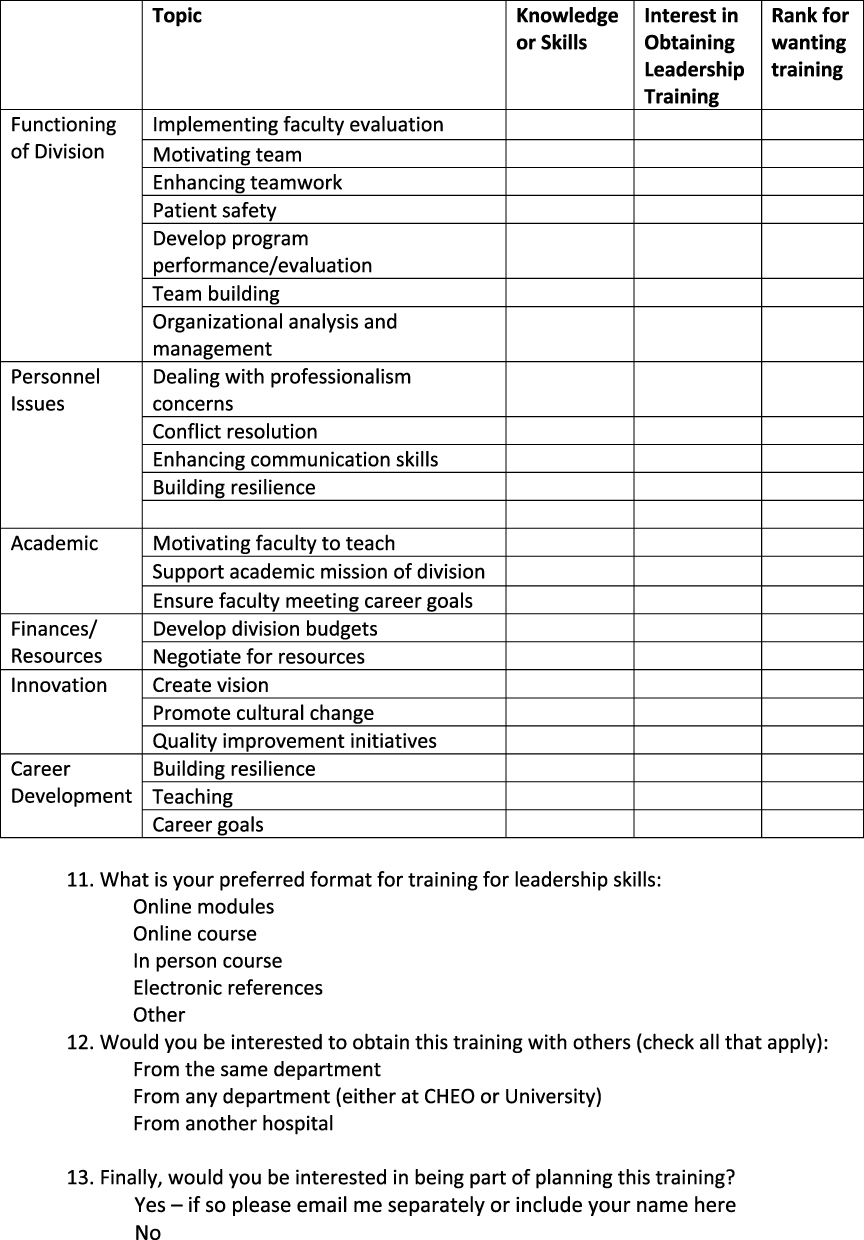
A needs assessment survey was developed de novo by one author (DJ). Literature review of other needs assessments for educational leadership formed the basis for initial item generation1–4 incorporating relevant questions based on our objectives and chosen survey domains. The aim was to document demographics, preparedness for the role of Division Chief and desired leadership training for the role. Items were revised by the other authors (MJ, LS) and resulted in a 13-item final questionnaire covering the domains of functioning of the division, personnel issues, academic, financial/resources, innovation and career development (Figure 1). These were deemed most relevant by the authors based on informal feedback from Division Chiefs on survey objectives and specific domains. The final survey was piloted using read-through methodology by like individuals to potential respondents. This was then created on Survey Monkey (San Mateo, California, USA).
Figure 1 Continued. Figure 1 Questionnaire.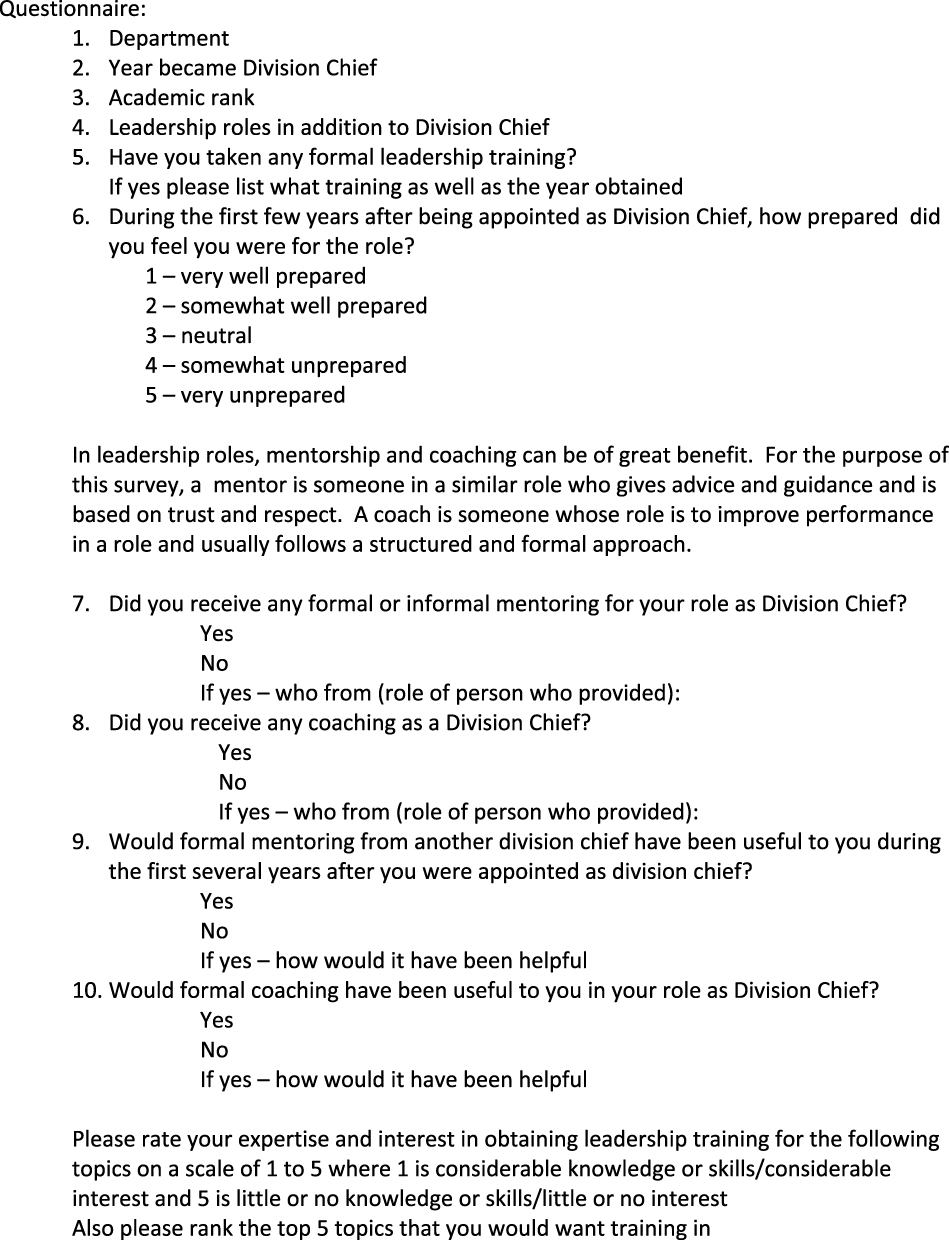
CHEO is a tertiary care academic pediatric hospital and children’s treatment centre with programs that span the continuum in each of acute medical and surgical care, mental health and development and rehabilitation. It serves a patient population from Eastern Ontario, Western Quebec and Nunavut and is a provincial reference centre for newborn screening and genetic testing. It has an independent research institute and is affiliated with the University of Ottawa. Within CHEO there are eight Departments (Pediatrics, Anesthesia and Pain Medicine, Genetics, Surgery, Medical Imaging, Lab Medicine, Ophthalmology, and Psychiatry). Within these Departments, there are three divisions in Lab Medicine, 18 in Pediatrics, 8 in Surgery and 2 in Psychiatry. As per the hospital bylaws, each Division Chief is appointed by the Board of Directors, for a 5-year term that is renewable once. Within CHEO, all departments with divisions, are part of a hospital-wide comprehensive alternate funding plan.
Over the past 5 years, the Chief of Staff has instituted regular meetings of both the Division and Department Chiefs to create a community of practice. The intended goals are to share information, discuss best practices, provide targeted venues for leadership development and serve to support those in this role. The questionnaire was introduced to the Division Chiefs at one of these hospital Division Chiefs’ meetings, as well as at a Department of Pediatrics Division Chiefs’ meeting. These presentations were followed by an electronic survey sent via email to the email distribution list of all Division Chiefs at CHEO. A follow-up email was sent to the same email distribution list 10 days later.
Respondents consented to participation upon submission of the survey, which was articulated in the survey introduction. The study was not required to be approved by the Research Ethics Board (REB) at our institution as it was a quality improvement study, which is exempt from REB review.
The results of each question were collated, and simple descriptive statistics were calculated.
Results
The survey was sent to a total of 31 Division Chiefs at CHEO and was completed by 22 of them resulting in a 71% completion rate. All submitted surveys had at least 80% of the questions answered.
Demographics
Of the 22 Division Chiefs who completed the survey, 14 were from Pediatrics (63.6%), 6 from Surgery (20%), 1 from Psychiatry (3.3%) and 1 from Lab Medicine (3.3%). Based on number of Division Chiefs within each department, completion was 77.8% (14 of 18) for Pediatrics, 75% (6 of 8) for Surgery, 50% (1 of 2) for Psychiatry and 33.3% (1 of 3) for Lab Medicine. The academic rank of those who completed the survey was full professor in 4 (13.3%), associate professor in 16 (53.3%) and assistant professor in 2 (6.7%). The length of time they had been a Division Chief was a mean of 5.5 years, median of 5 years, and with a range of just became a Division Chief this year to had been one for 20 years. Seventeen of the 22 respondents had leadership roles in addition to the role of being a Division Chief. These roles ranged from other hospital roles and university roles to national and international leadership roles. Nineteen of the respondents (86.4%) had taken some type of formal leadership training, which was provided through the hospital, the university and/or an external source of training.
Preparedness for Role
Self-perception of preparedness for their roles among Division Chiefs was as follows: none (0%) felt they were very well prepared, 5 (22.7%) felt they were somewhat well prepared, 9 (40.9%) were neutral, 5 (22.7%) were somewhat unprepared and 3 (13.6%) were very unprepared for the role. Only 5 (22.7%) received any coaching for their role as Division Chief but 81.8% felt that formal coaching would have been useful to them in their role as Division Chief. Half of the respondents received mentoring, either formal or informal, for their role as Division Chief and all but one (95.4%) felt that formal mentoring from another Division Chief would have been useful to them during their first few years of their appointment. Respondents’ main themes of interest regarding mentoring were in better understanding the role and having an experienced sounding board for their ideas.
Leadership Skills/Training
The Division Chiefs were asked to rate their expertise and interest in obtaining leadership training for various topics and to rank the top five topics for which they would want training. As shown in Table 1, the topic that Division Chiefs felt they had the most knowledge and skills in was patient safety. Of the 22 items in which the Division Chiefs wanted training, the area with the highest ranking were topics of finances and resources. Among these areas of interest for leadership training, 100% of Division Chief respondents wanted training in developing divisional budgets. The next most desired training was in supporting the academic mission of the Division followed by developing program performance and evaluation. The overwhelming preferred format for this training was an in-person course (68%), followed by online course (22%) and online module (9%). The majority preferred to obtain this training with others from any department (71%), followed by equal numbers preferring from those from the same department or from another hospital (15% each). Half of the respondents expressed interest in being part of planning for this training.
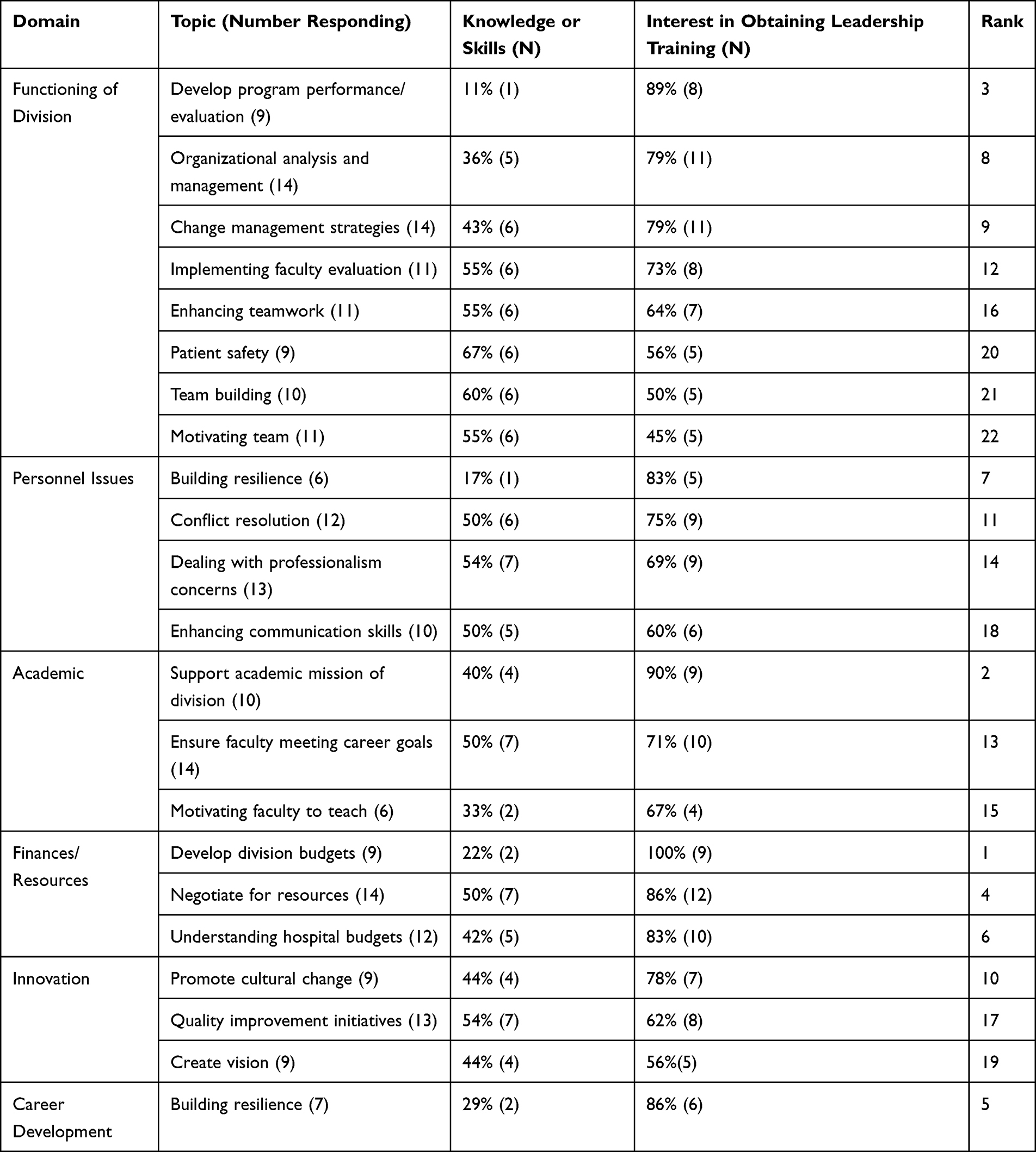 |
Table 1 Leadership Training Knowledge and Interest in Obtaining Training (N=20 Respondents) |
Discussion
Division Chiefs play an important and challenging role within the evolving complexity of the health system. Being a Division Chief provides an excellent leadership opportunity and requires specific skills to be effective in this role. Obtaining these skills can be a challenge for some, and to date this has depended locally on individual Division Chiefs seeking their own training to address their perceived gaps (personal communication). We successfully designed and carried out a needs assessment to identify current expertise and specific leadership development needs among pediatric Division Chiefs across several departments in our institution. Our survey had much stronger completion rates than previously published ones (71% vs 22.5–58.5%), allowing for more meaningful results.
Previous needs assessments of both gastroenterology3 and obstetrics and gynecology2 Program Directors found that a mentorship program would be very beneficial to those in this role, and our needs assessment also found that mentorship would have been very useful when taking on this role. Fortunately, about half of our respondents received some mentoring in the role. These results highlight the ongoing need to ensure that mentorship is in place for those taking on the role of Division Chief. One excellent source of mentorship is a previous Division Chief, and this role could be formally established and supported to optimize transfer of skill and experience.
The area of greatest need among all Division Chiefs identified by our assessment was in financial literacy and specifically development of divisional budgets. Interestingly, this was also identified by obstetrics and gynecology Program Directors needs assessments as something for which they wanted more training.2 This likely highlights the lack of training provided to physicians in this area in general and represents an area for education for different types of medical leaders at various stages of training. While residency programs usually provide training regarding the financial aspects of independent practice office management, they rarely address hospital and health system financing structures and processes, which are needed as a Division Chief. As well, CHEO physicians are in an alternate funding plan, which adds complexity with regard to resources available to create and recruit into new positions. This model of funding may influence the financial literacy of Division Chiefs.
The survey noted that the majority of Division Chiefs had previously taken some type of formal leadership training, which was provided through the hospital, the university, and/or an external source of training. However, the results show that although they had participated in leadership development training, they clearly did not feel prepared for the role of Division Chief. Many of the competencies prioritized by the survey respondents for further training are more management skills (budget development, time and resource allocation, etc.) which are often not integral parts of medical leadership training programs or workshops, which tend to focus on other aspects of leadership. Helping potential and new Division Chiefs find leadership programs that incorporate skill development for all aspects of the role may lead to more comfort and preparedness in these areas. Previous literature on the effectiveness of leadership training in healthcare has shown that the perceived learning of participants in terms of leadership skills improves with training, but interestingly there are limited data on the impact of such training on the organization.5
Good leadership at the divisional level has been shown to be important, especially related to productivity, quality of care and faculty wellbeing. In a recent survey of pediatric surgeons, poor leadership was found to be a driver of distress and well-being among respondents.6 An interesting study examined the influence of leaders on quality improvement of physicians.7 They found that medical leaders influenced their colleagues toward quality improvement when they chose to exert this influence. The literature supports the importance of good leadership in physician performance.
The strengths of our study are the high response rate and novel nature of this needs assessment. The results indicate specific areas where new Division Chiefs would like further training. Limitations include that several of the Division Chiefs had been in the role for a long time and so may have recall bias due to their retrospective nature. Similarly, several respondents were brand-new to the role and so may not yet have the knowledge of what is needed to be effective in the role. Finally, this was performed within one pediatric institution. The results thus may be more specific to this population of Division Chiefs, however we believe that the themes are generalizable to other Division Chiefs at other academic institutions.
Conclusion
Overall, this needs assessment identified an unmet need for leadership training and development among Division Chiefs at an academic pediatric institution and delineated many topics that Division Chiefs felt would help them in their role. Within our institution, there is leadership training offered to leaders of all types, but these results suggest that they need targeted offerings tailored for the unique needs of academic physicians. Informed by the results of this survey, a targeted Division Chief Leadership Development Program was designed and is currently being implemented at our institution. A formal evaluation will analyze its impact and outcomes. We have also used the findings of our survey to guide our Division Chief community of practice meeting topics. This information can be used at other institutions to support the leadership of Division Chiefs. At the current time of a challenged healthcare system following 2 years of the COVID-19 pandemic, it is more important than ever to prepare our medical leaders for their roles as leaders.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sanfey H, Schenarts K, Rogers DA, et al. Needs assessment for an American College of Surgeons certificate in applied surgical education leadership (CASEL). J Surg Educ. 2018;75:e112–e119. doi:10.1016/j.jsurg.2018.05.007
2. Botros SM, Learman LA, Bell C, et al. Needs assessment survey of obstetrics and gynecology subspecialty fellowship program directors. Am J Obstet Gynecol. 2018;219:207–208. doi:10.1016/j.ajog.2018.04.038
3. Thackeray EW, Pardi DS, Norby SM, et al. Mentorship programs for gastroenterology program directors. Is there an unmet need? J Clin Gastroenterol. 2011;45:e97–e100. doi:10.1097/MCG.0b013e3182203183
4. Stefan A, Hall JN, Sherbino J, et al. Faculty development in the age of competency-based medical education: a needs assessment of Canadian emergency medicine faculty and senior trainees. Can J Emerg Med. 2019;21:527–534. doi:10.1017/cem.2019.343
5. Stoller JK. Developing physician leaders: does it work? BMJ Leader. 2020;4:1–5. doi:10.1136/leader-2018-000116
6. Rialon KL, Mueller C, Ottosen M, et al. Drivers of distress and well-being amongst pediatric surgeons. J Pediatr Surg. 2021;56:841–848. doi:10.1016/j.jpedsurg.2021.01.001
7. Palmer RH, Hargraves JL, Orav EJ, et al. Leadership for quality improvement in group practices. Med Care. 1996;34:SS40–SS51. doi:10.1097/00005650-199609002-00005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.