")
Back to Journals » Journal of Healthcare Leadership » Volume 14
A Feeling of Ambiguity: A Qualitative Content Analysis of Managers’ Experiences of Evidence-Based Practice in Swedish Primary Care
Authors Abelsson T , Karlsson AK , Morténius H
Received 6 May 2022
Accepted for publication 3 September 2022
Published 19 September 2022 Volume 2022:14 Pages 143—153
DOI https://doi.org/10.2147/JHL.S371643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Russell Taichman
Tobias Abelsson,1,2 Ann-Kristin Karlsson,1 Helena Morténius1,3
1Department of Public Health and Community Medicine, University of Gothenburg, Gothenburg, Sweden; 2Department of Research and Development, Region Halland, Halmstad, Sweden; 3Department of Child and Adolescent Mental Health, Region Halland, Halmstad, Sweden
Correspondence: Tobias Abelsson, Email [email protected]
Background: The Primary care manager plays a vital role in promoting a research culture in the healthcare center. The position involves both the implementation of organizational directives and patient care. The research culture and use of evidence influence each individual healthcare professional and ultimately the quality of patient care.
Purpose: To describe primary healthcare managers’ understanding of evidence-based practice in the Swedish primary healthcare context and their ability to influence its implementation.
Methodology: Qualitative content analysis of data collected in individual interviews.
Results: In general, managers expressed a positive view toward the use of evidence in daily practice. However, they were sometimes hesitant about fully implementing evidence-based results. This was mostly attributed to the struggle of balancing finances and allocating sufficient time for staff to keep up with and engage in evidence-based practice.
Conclusion: The organizational culture impacts the mind-set of all co-workers including managers. Those managers influenced by traditions and norms may fall into the trap of devaluing the benefit of research and evidence. The inherent feeling of being alone and without guidance in some matters related to evidence-based practice inevitably leads to inconsistency and ambiguity. The use of clinical pathways that constitute one form of evidence has become a substitute for proper, careful, individual investigation, implementation, and evaluation of each patient case. This means that managers experience moral and physical stress when trying to meet organizational, staff, and patient demands.
Practice Implication: Awareness of managers’ influence and experience of working according to evidence-based practice is valuable to gain an insight into how Swedish primary healthcare functions at local level. Illuminating and discussing evidence-based practice is an assurance of quality that contributes to many aspects of the overall safety of care.
Keywords: information dissemination, management, primary healthcare, EBP, evidence-based practice
Introduction
Since its origin in Florence Nightingale’s 19th century nursing philosophy, modern medicine has been dominated by the paradigm of evidence-based practice (EBP).1 The common denominator over time has been the focus upon adopting clinical evidence in practice.1 EBP strives to integrate three spheres of interest: patient, research, and health professionals’ (HPs’) experience in order to provide the best care available for the patient.2–7 This has placed demands on each HP to possess the abilities required to make decisions based upon high-quality information,8,9 and sometimes to even revise old dogmas of teaching and practicing EBP.6 While the required information skillset must be acquired by each individual HP, the facilitation of EBP, in the form of ensuring the availability of support, resources, and a research culture, is the responsibility of the local management.10–15 Managers are often recruited from the HP-staff within primary care with their own individual preunderstanding of EBP.
This in turn places primary healthcare managers (in the following called managers) in a unique position as mediators of interests and facilitators of resources, requiring them to navigate between the interests of different commonalities and personnel groups.15,16 The above-mentioned roles involve interaction, where leadership depends upon the individual managers ability to communicate, prioritize, and exercise social skills.17 Communication has been strongly emphasized as a sign of good leadership.16,17 The leadership style, individual social skillset, and position in the healthcare organization gives managers great influence in terms of supporting EBP.17
In their study of Swedish managers experiences of and attitudes toward working with EBP, Abelsson et al reported that knowledge of evidence and its impact in the local PHC is generally good.12 However, the time devoted to gathering evidence and keeping up-to-date in their field varied.12 Lack of time and knowledge about information resources has been identified as potential barriers to the implementation of EBP.5,15 One of the prerequisites for EBP is HPs’ knowledge and ability to collect and implement evidence. In the context of Library and information science, the ability to recognize, investigate, and meet a perceived information need is termed information literacy.18 With regard to information retrieval, a further development is the concept of evidence readiness, where factors such as; professional training as well as training in EBP, equipment, and leadership constitute four pillars of importance for the ability to implement EBP.5 This model, which is supported by earlier research, integrates and explains much of the complexity that characterizes cooperation between management and HPs and their access to good quality information resources.8,19,20
The present body of knowledge concerning the concept of EBP and its implementation in primary healthcare research is mostly made up of studies focused upon either specific professional categories or their views on management/management strategies.11,19,21,22 We found few previous studies focusing on the evaluation, use, and implementation of evidence in a primary care context, although there has recently been an increase in the number of studies investigating managers and the determinants of their success in implementing EBP.23 For instance, Gifford et al published a systematic review in 2018 aimed at identifying the leadership behaviors that promoted good research use.11 The main finding was that managerial support for and a positive attitude toward committing to change were essential for good research implementation.11,15 Furthermore, in their systematic review Spehar et al explored general practitioners’ (GPs’) views of the managerial role.24,25 They revealed that GPs generally describe a conflict between the clinical and the management role, in addition to a sense of being unprepared for such a role.24
Thus, there is an evident lack of knowledge of managers experience of working in accordance with EBP in a primary care setting. Hence the aim of the present study was: To describe primary healthcare managers’ understanding of evidence-based practice in the Swedish primary healthcare context and their ability to influence its implementation.
Conceptual Framework
The conceptual framework of the present study is the clinical development and implementation of EBP by means of concepts gathered from implementation and management research.
As previously mentioned, the concept of EBP has its roots in the care of wounded soldiers in the 19th century.1 Clinical decision-making methods were advanced during the Second World War by the work of Archibald Cochrane, who was captured and subsequently served as a medical officer in various German prisoner of war camps, where he attempted to improve the health of the prisoners.26 In the 1970s an obstetrician called Ian Chalmers was inspired by Cochrane’s work and created the first registry of randomized controlled trials. With the establishment of the Cochrane collaboration, aptly named after Archibald Cochrane, Chalmers and a number of epidemiologists continued the introduction of the EBP-methodology and built the basis of what would become its leading authority; the Cochrane foundation.26 Until then the concept of EBP was referred to by the synonym Evidence based medicine (EBM). In this process David Sackett, one of Chalmers’ collaborators, coined the best-known formal definition of EBM:
“Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.”4
The concept of readiness/willingness to change was adopted from management research and used in this article to describe the development process of an organization when facing new ways of working.5
Method
Design
The study was designed as a qualitative content analysis with an inductive approach.
Selection and Recruitment of Participants
The recruitment of participants took place in 2020. The inclusion criteria were employees with management duties and working in a publicly funded primary healthcare center (PHC). There are 23 PHCs in the county studied of which all were invited to participate in the study.
Study Setting
Due to the ongoing pandemic situation, the study had to be conducted as recorded telephone interviews instead of the planned face-to-face ones. Participants were called after arranging a time and date. As the interviews were performed via the telephone, complete privacy could only be ensured by the discretion of each participant. The interviews were recorded and transcribed verbatim. Mean time for interviews was 30 minutes.
First author, a male librarian trained to handle health professionals need for informatic support, acted as interviewer in all interviews. There was no previous relationship between interviewer and participants regarding personal and professional sphere of interest. All but one participants were female.
Data Collection
Data collection began in the first quarter of 2020. The first step was to compile a list of publicly funded PHCs and their managers. An introductory letter containing information about the study was sent to all potential participants on the list. The participants who agreed to participate were then contacted in order to arrange a date and time for the interview. The interviews were consecutively conducted by telephone during the data collection period. A reminder was sent seven and 14 days after the introductory letter, thus a total of three invitations to participate in the study. Written consent was achieved by confirmation of interview date and oral consent by approving to the information given in the introduction of each interview. The interviews were conducted with help of an interview guide constructed by the research group which consisted of open-ended questions followed up by additional clarifying questions when needed. The opening question was always about the participants engagements in their PHC.
Data Analysis
The data analysis was carried out according to the method described by Graneheim and Lundman.27,28 After transcription each of the authors read through the entire data and then identified meaning units in the form of statements from the interview text. The authors then met and discussed the selection until agreement was achieved. The meaning units were then reduced, condensed, and coded (Table 1). The first author sorted the codes into tentative subcategories. For this step in the process the authors met again and discussed the subcategories and their content. The subcategories were sorted into categories, which formed the manifest content illustrating the HPMs’ perspective on defining and working in accordance with the concept of EBP. The discussion ended when consensus was achieved. After identification of the subcategories a similar process was performed to determine the categories and their meanings. In the next step, the meaning of each subcategory was condensed, thus revealing the manifest meaning in a wider context (Table 2). From these a final abstraction was conducted and the last step was the identification of an overall theme that encompassed the latent meaning of the data.28 The results were illustrated by citations from the participants.
 |
Table 1 Examples of the Analysis Process |
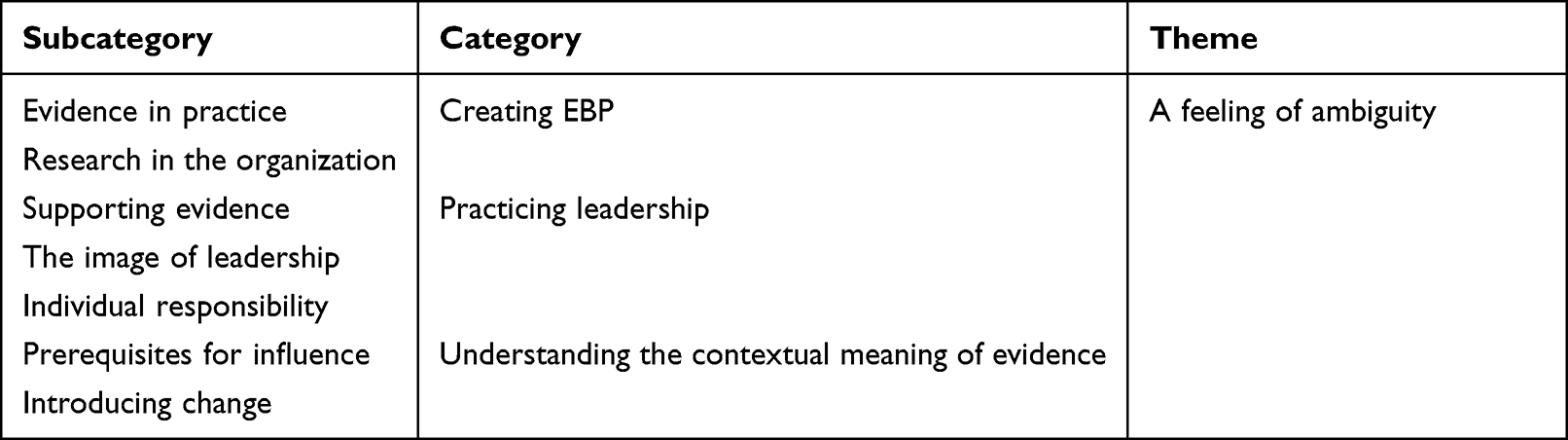 |
Table 2 Result Structure |
Results
Out of the 23 invited participants 8 participants (7 women and 1 man) agreed to participate in the study. This equals a response rate of 35%. Occupational background of participants is within nursing and its specialists. Mean experience of management is about 9 years where half of the population have less than 10 years’ experience and the other half have more than 10 years. Mean age is 49 years, 3 managers is below 50 years and 5 above.
The initial analysis phase resulted in three categories: Creating EBP, practicing leadership and understanding the contextual meaning of evidence. All were derived from six subcategories that illustrated the manifest meaning expressed in the interviews. In the second phase of the analysis a theme; “A feeling of ambiguity” emerged. This theme was interpreted as the latent meaning of the study.
Creating EBP
This category comprised the use of evidence and research results, the value assigned to, and general attitude toward its practice as reported by individual managers as well as within the primary healthcare organization. This was done based on two subcategories: “Evidence in practice” and “Research in organization”.
Evidence in Practice
Some expressed that evidence was always present in primary care due to the fact that they adhered to the given guidelines and policies. Others were more self-critical, admitting that they should make greater use of current evidence in daily practice decisions. Several were unsure about the amount of evidence used but stated that facts were a vital component in care.
In general, the participants were clear about the fact that evidence should be present. Some even stated that evidence was believed to permeate all primary healthcare levels. At the same time, they were aware that evidence should be consulted more than currently the case in their own day-to-day provision of care at the PHC.
“I think it´s important to use the facts and knowledge we´ve got … ” (Manager 1)
Research in the Organization
Managers expressed a belief that evidence was included in information such as care standards and internal treatment plans for the whole county. This kind of condensed information issued by higher level management was said to be trusted and included in PHC daily practice.
Ensuring the dissemination of this kind of information within the PHC was described as a managerial task. Some participants were of the opinion that the duty of ensuring compliance with EBP in the PHC was also the responsibility of the managers. This led to conflicting feelings about being responsible for EBP but not having the resources due to political decisions about resource allocation and thus experienced as being in direct conflict with the tasks assigned to the healthcare system.
The general definition of the concept of evidence was that it was trusted information built upon research results, preferably from several studies. However, the importance assigned to research in the local context differed among the participants. On the one hand, it was deemed important, while at the same time managers were obliged to remain within budgetary constraints and not waste scarce resources. On the other hand, the managers perceived a lack of interest in conducting research amongst their co-workers.
No, I can´t say that there is no interest in research. I believe that most of us are positive toward research, it´s just simply a fact that everything else needs the focus more. (Manager 4)
Practicing Leadership
This category comprises the participants’ thoughts about how to lead and the prerequisites required to implement leadership that supports EBP, as illustrated by the following three subcategories: Supporting evidence, The image of leadership and Individual responsibility.
Supporting Evidence
Here, aspects of the individual information support network were identified, which was often personified by the local chief physician. Some mentioned the administrative management system as supportive for obtaining the latest clinical guidelines.
The subcategory also contained descriptions of what was considered good general resources for evidence gathering and where their co-workers could obtain help in order to keep updated. Among the most frequently mentioned resources were membership journals from the labor unions and information from the pharmaceutical manufacturers regarding new drugs and products. The annual county review of ongoing research was also mentioned as a way for everyone to keep abreast of general local clinical research. Finally, co-workers’ own research was also described as an important resource for disseminating new knowledge among colleagues.
“It´s not like you adopt any new knowledge yourself, it comes from upper management if it’s needed.” (Manager 3)
The Image of Leadership
The personal traits that a good manager should possess included willingness to listen, sensitivity, and humbleness, but at the same time firm leadership. When describing the kind of support they received as managers from the rest of the healthcare organization, they mentioned time pressure that hindered the practical application of EBP in the day-to-day running of the PHC. Some participants stated a willingness to develop themselves, their co-workers, and their PHC to be more effective users of EBP, but experienced little support and understanding from organizational management. They expressed that the present reality of work in the PHC was the biggest challenge and they wished for change, but the above-mentioned barriers in combination with financial pressure to treat as many patients as possible with as few staff members as possible was experienced as burdensome.
“We have so much to do and so few staff. We can’t take part in training or meetings, things like that. We need to be here for the patient.” (Manager 6)
Individual Responsibility
In order to remain updated the managers stated that they rely heavily on the fact that every co-worker has some time allotted for catching up with advances in her/his field of knowledge. As managers they were aware of their role in underlining the importance of being updated and using EBP when exercising their profession. Continued studies during the whole of one’s professional career was mentioned as a prerequisite.
As well as expectations on co-workers to keep updated, the managers also stated that continuing their own research was equally important. When talking about their own responsibilities, they made some additions to the previously stated ones. The importance of independent research and reflection was stressed in the context of information gathering and evaluation. The view that the importance attributed to EBP varied greatly among HPs was also voiced. But in general, the participants believed that HPs were trained in information literacy and source criticism due to their professional education. However, the requirements for keeping updated and being able to reflect upon EBP were also experienced as being highly situation dependent both for themselves and their co-workers.
“What I sometimes feel is that when you’re tied up with work, as I am, you don’t have the time to keep updated.” (Manager 8)
Understanding the Contextual Meaning of Evidence
This category contained two subcategories labelled “Prerequisites for influence” and “Introducing change”. The aim was to describe the use of evidence in daily practice as well as the implementation of changes in routines inspired by research. It identifies perceived prerequisites for understanding the evidence and the context required to successfully reach out and promote evidence-based practice among one’s co-workers.
Prerequisites for Influence
Here, the aim was to describe the managers perceived ability to promote the implementation and use of EBP in their PHC. Overall, they reported a lack of support, particularly from politicians responsible for healthcare management. There was a perceived lack of focus on primary healthcare on the part of county-level politicians, described as the absence of quality and cooperation between all parts of the healthcare system. Previously mentioned barriers such as lack of time, economic resources and staff were described as troublesome and as contributing to unequal conditions among PHCs. Participants expressed that they often had to deal with problems outside office hours. The daily care provided by the clinic was perceived as “firefighting” in terms of quickly resolving issues and keeping the PHC running in order to maintain the financial balance.
“You have to use your free time to come up with solutions, that’s how it is.” (Manager 6)
Introducing Change
Regarding their influence on introducing improvements and implementing change, the managers underlined the importance of slow and steady change in cooperation and communication with staff. The changes had to be relevant and the staff involved in their introduction and implementation. Any minor local development considered feasible had to be approached in this manner.
I can’t really tell if there is any kind of evaluation regarding the evidence content in guidelines. It’s more like “This is how we shall work”. And that’s what we do. (Manager 4)
A Feeling of Ambiguity
The overall theme was built upon the manifest content in all categories and subcategories. In line with the content analysis method, the theme was seen as a thread connecting the latent content of all categories and subcategories. The general feeling was one of being isolated within the organization and unable to influence the manner of the implementation of EBP. In addition, the manifest meaning of the text was interpreted as the managerial role involving dutifully promoting EBP, but the implementation appeared ineffective for various, mostly practical, reasons. There was a feeling of losing sight of the importance of allocating time and resources to engage in EBP due to the constant pressure to deliver healthcare.
Discussion
Principal Findings
The present study illuminated a reality in which managers reported a feeling of ambiguity toward evidence and EBP. Nevertheless there was an awareness of the importance of using evidence in practice and decision-making. However, the managers outlined the difficulty of being unable to fulfil the demands of maintaining production, while allowing themselves and their co-workers sufficient resources to remain updated in their profession. This was expressed as moral and physical stress by the managers.
General Discussion
As indicated by the main findings, a sense of ambiguity was dominant when the managers were asked about their impression of evidence and its use in daily practice. There was a conflict between what ultimately boils down to personal convictions related to care as opposed to the organizational need to produce health in patients. This production-oriented approach to healthcare led to feelings of being abandoned and without support within the organization when talking about and trying to implement evidence-based care. These feelings of being isolated and sometimes having little time for or interest in research are not unique, as similar findings have been reported by Morténius in her study of cultural influence upon willingness to change.14
The present study explored managers’ attitudes and the results could have an important influence on the assignment of priorities for healthcare delivery, individual research/education, and the local discussion climate. Morténius’ study highlighted the importance of managerial attitudes when steering the discussion climate toward evidence and/or research in PHCs.14 This in turn influences what is termed readiness to use EBP, which was also reflected by the concept of “Evidence-Based Practice Readiness” as described by Schaefer and Welton.5 The concept is intended to encompass every aspect of EBP by including four preferential pillars labelled: Nursing, Training, Equipping and Leadership support. Leadership support is highlighted as fundamental in setting the agenda for an EBP culture.5 Adding to this the fact that the results from the present study reveal that the managers perceived no support for or education in EBP, it becomes clear that the collective thought pattern is not very concerned about any developmental “extra activities”.
When leadership was discussed, the participants in the present study emphasized the importance of good communication and conveying a feeling of inclusion when implementing new practices. This fitted well with the description of the managerial role as a mediator between the organization and the commonalities found in the literature, in this case local HPs and the management of the organization.14,16 While not directly transferable to Sonnino’s definition of complete management styles, a shift could be seen among the task oriented and relational attitudes of our participants when discussing implementation of evidence and the subsequent change. This is very similar to the shift in orientation mentioned by Sonnino.16 Although a part of all management strategies, this way of shifting between relational and task oriented leadership is a huge endeavor, as it places demands upon a number of either naturally achieved or learned intrapersonal skills such as listening, empathy, altruism, and technical as well as strategic knowledge.16 Despite the fact that staff in managerial positions are required to switch between styles and roles in order to best navigate between commonalities and interests,16 our participants described the experience of being “caught” between expectations from staff and organizational goals within the local context. Thus the same emotions that seem to be significant for good leadership, such as altruism and empathy, also appear to be a source of internal frustration and ambiguity, where managers feel as if their hands are tied, which was also evident in the present study. As discussed earlier, EBP implementation research has shown that modern managers mainly rely upon good knowledge of EBP and intrapersonal skills such as communication and empathy to achieve the best results.14,16,17
Manny complex organizations is ruled by what literature states as “Institutional logics”29 which rests upon the notion of two competing ways of viewing management: professionalism and managerialism.29 This pattern of thought is true and most evident in healthcare,29 the statements of our participants also show consciousness about although not expressively. The professional management rests upon credentials of earned expertise and professional certification, while the managerial management rests upon a formally assigned hierarchy and focuses upon efficacy.29 This difference is obvious amongst our participants when talking about being torn between organizational and patient-oriented goals. One could see this as a prolonged hesitation about how to choose between staff/patient needs and the organizational demands of the management styles each PHM employs. In other words, the case is most often that a manager who is trained according to professional management styles has to act and enforce the policies of healthcare according to the managerial attitudes of the organization.
Concerning the collection and use of evidence, there was a general feeling that one should be more updated or receive more help to facilitate effective dissemination of information in order to better grasp EBP in terms of local recommendations and best practice. Although this could be seen as a consequence of a lack of resources, such as time allocated to research, that may be only a part of the problem. A study by Spehar et al24 describes a more fundamental shortcoming in the training of prospective managers related to their previous clinical profession. As it is not unusual for managers to have been recruited from clinical staff, the authors report differences in ambition between nurses and doctors, where nurses more often strive to reach a higher level of leadership as part of their career development, while doctors might see a leadership position as somewhat outside their original comfort-zone and not as important for career development.24 In addition, managers in Sweden lack a uniform managerial education and are usually recruited from either the nursing staff or doctors. To further complicate matters, this staff recruitment of managers most likely makes them susceptible to inherited thoughts and practices6 regarding the use of evidence. This in turn brings us to the aim of the present study, namely to investigate the influence of managerial attitudes in the use of evidence.
Although not directly stated by the participants in the present study, the need to be familiar with research coupled with the lack of time to read research-related materials was described as a barrier to the growth of research in primary care. There were statements that mentioned the possible correlation between educational level and interest in developing research activities. This agrees with Meza’s description of the influence of the managerial role in interpreting the prerequisites for EBP and promoting its incorporation into daily practice in the local context.17 Further support for the managers role was found in the discussion of the organizational culture and its influence on willingness to change, ie openness to change, among primary healthcare staff by Morténius et al.14 Although a number of factors influence the readiness to change as well as the general research interest among primary healthcare staff, Morténius et al mentioned the historical disinterest in and low priority of research which in itself is a somewhat self-fulfilling prophecy that was actually corroborated on numerous occasions by our participants when mentioning a general disinterest in research among their co-workers.
As touched upon earlier in this discussion, some of the managers voiced concern about being unable to find time to keep updated. The clinical reality did not seem to allow time for a reflective work approach as required by the EBP process. This is troublesome in terms of engaging in EBP, as it is a process that requires extensive resources if performed with the intent of improving the outcome of each patient.6 This lack of time forces managers to rely upon premade solutions and treatment plans, hence obliging them to place a high degree of trust in the system. This is supported by data from the present study, where participants stated that they strongly relied on the fact that information such as internal guidelines and policies already contained sufficient evidence to enable them to recommend the best available therapy options. However, this insight was not always without self-criticism and came with the awareness that they ought to make use of research evidence to a higher degree than is the case in reality, which is referred to as “clinical pathways” in earlier studies. This is a pragmatic and common way of relying upon information and clinical material prepared in advance for a particular therapy, diagnosis etc.6 It is a conventional but not optimal way of practicing EBP. Instead, EBP should be considered a process of constructing individualized and updated care tailored to each patient.6
In addition to clinical pathways, Youngblut and Brooten also describe what was deemed trustworthy evidence by their participants, who took the number of studies and their source or origin into account.6 The aforementioned study as well as the present one indicates that there is frequently a willingness to make decisions based on established clinical pathways. This together with the variance in what is considered good and trustworthy evidence is both interesting and somewhat worrying because of the ripple effect in the use or non-use of treatment therapies. Another concern is the possible delay or even inability to respond to new research evidence in primary healthcare. These concerns were to some extent considered by the participants in our study because they experienced research to be extensive and hard to get a grip on and that it should be treated as a special interest for those inclined to perform it. This lack of interest in research was highlighted by our participants and believed to be the result of different educational levels as well as age at graduation among the managers and top management.
There was a consensus that good evidence consisted of clinically tried and tested information. This concurs with the definition stated by Youngblut et al6 where the most important evidence is derived directly from research. In the minds of the participants in our study, the concept of evidence was naturally and closely connected to, and sometimes equated with, research and research implementation, both of which are positively charged and welcome concepts that should be promoted. In spite of this positive mind-set, a dichotomy was observed between the positive attitude and the importance assigned to promoting research in the local context. Instead, the view of research seemed to be that it is something that should be driven by and initiated on a central level in the region, rather than in one’s own PHC. This isolationist way of thinking was also present in the article by Morténius et al, where the participants saw the clinic as more or less autonomous in questions regarding local development.14 The isolationistic mindset could also be observed in the perception of research as something that should be integrated and not something to be participated in, but also in the expressed lack of cooperation within the entire healthcare system in terms of research and education.
Conclusion
The presence of clashing institutional logics could be sensed, although not clearly expressed by a number of participants on numerous occasions, especially when discussing the need for evidence and the ability to autonomously implement it in practice. A perceived conflict in terms of the allocation of resources could be identified when the managers mentioned their own awareness of being unable to use evidence as much as expected. Their perception of being able to allocate sufficient time to efficiently use and retain evidence-based knowledge in their profession conflicted with the demand for economic balance in the PHC in the form of a high number of patient visits. A strict organizational implementation of EBP seems to have become a consequence of knowledge dissemination that should be treated as a way of streamlining care and shortening treatment paths. This way of producing care places additional strain on an already pandemic-exhausted healthcare system and increases the stress on managers who already experience stressful environments with a high workload.
Strengths and Weaknesses of the Study
One strength of the study is its contribution to the collective knowledge of managers with different occupational backgrounds in an area not previously investigated sufficiently. Furthermore, it is one of few studies to illustrate the vulnerability of a healthcare system that aims to rely on evidence as confirmatory background knowledge to established clinical pathways, instead of using evidence to increase patient utility and HPs’ specialist knowledge.
One weakness of the study might be the somewhat small sample size. However, this may not necessarily be a hindrance due to the richness of the content of each interview and the willingness of each participant to share information. Even a small sample might be deemed adequate if selected with care and if the data are considered good enough. The recruitment of participants and data collection were complicated by the dreaded pandemic that afflicted – and still in 2022 afflicts – the world and led to unusual circumstances such as telephone interviews and all the weaknesses associated with that data collection method. Furthermore, it would not be farfetched to assume that the pandemic influenced the willingness to participate due to the high workload among potential participants.
In qualitative research it is always difficult to completely demonstrate trustworthiness. The concept of trustworthiness in the present study is inspired by the thoughts discussed in Graneheim and Lundman’s article.28 Therefore, in this particular case trustworthiness was ensured by the following three factors. First, the recruitment of participants, who were all employed as managers in the county where the study took place. Second, all the authors were involved in every step of the analysis process. Third, the authenticity was strengthened by complete citations from the participants to support the overall theme.
Unanswered Questions and Future Research
The present study focused on managers and their experiences. Future research might include HPs and others who contribute to the care chain and their experiences of working with EBP.
Further research areas of interest could be to investigate the reasons why HPs in primary healthcare decide to apply for a managerial position. In the existing literature it is stated that there is some indication of a difference due to the person’s original professional category.16 Another suggestion for further research would be to continue the investigation by exploring how evidence and EBP are viewed by other groups of co-workers.
Implications
In terms of transferability, the results of the present study might be seen as a precursor to expanding the qualitative research on individuals’ experience of information dissemination at all levels of healthcare. The insight gained by starting from the individual may add to the pre-existing corpus of study reports.
The practical implications of the present study are that managers on all levels need to reflect on and discuss the meaning of evidence and EBP in order to find a middle ground between economically mandated production and the softer values of patient and staff care. This could be achieved by advancing the local discussion of and reflection on EBP and its concepts among co-workers.
Ethics
The study has been approved by the Swedish ethics committee in Lund (Dnr: 2017/281). Participants was informed that participation included consent to publish anonymous data and results on a group level. Consent to participate in this study was received by the confirmation to participate by each participant.
Acknowledgments
The first author would like to thank Sara Gabrielsson at Lund University for valuable input during the writing of this article.
Disclosure
Mr Tobias Abelsson received ordinary salary and payment of article processing charge from Region Halland. Article written without other influence upon creation of the article. The authors declare no other conflicts of interest in this work.
References
1. Mackey A, Bassendowski S. The history of evidence-based practice in nursing education and practice. J Prof Nurs. 2017;33(1):51–55. doi:10.1016/j.profnurs.2016.05.009
2. Albarqouni L, Hoffmann T, Glasziou P. Evidence-based practice educational intervention studies: a systematic review of what is taught and how it is measured. BMC Med Educ. 2018;18(1):177. doi:10.1186/s12909-018-1284-1
3. Oyinlola JO, Campbell J, Kousoulis AA. Is real world evidence influencing practice? A systematic review of CPRD research in NICE guidances. BMC Health Serv Res. 2016;16:299. doi:10.1186/s12913-016-1562-8
4. Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS. Evidence based medicine- what it is and what it isn´t. BMJ. 1996;312(7023):71–72. doi:10.1136/bmj.312.7023.71
5. Schaefer JD, Welton JM. Evidence based practice readiness: a concept analysis. J Nurs Manag. 2018;26(6):621–629. doi:10.1111/jonm.12599
6. Youngblut JM, Brooten D. Evidence-based nursing practice why is it important. AACN Clin Issues. 2001;12(4):468–476. doi:10.1097/00044067-200111000-00003
7. Greenhalgh T, Howick J, Maskrey N. Evidence Based Medicine Renaissance G. Evidence based medicine: a movement in crisis? BMJ. 2014;348:g3725. doi:10.1136/bmj.g3725
8. Sibbald SL, Wathen CN, Kothari A, Day AM. Knowledge flow and exchange in interdisciplinary primary health care teams (PHCTs): an exploratory study. J Med Libr Assoc. 2013;101(2):128–137. doi:10.3163/1536-5050.101.2.008
9. Abelsson T, Mortenius H, Bergman S, Karlsson AK. Quality and availability of information in primary healthcare: the patient perspective. Scand J Prim Health Care. 2020;38(1):33–41. doi:10.1080/02813432.2020.1718311
10. der Zijpp TJ, Niessen T, Eldh AC, et al. A bridge over turbulent waters: illustrating the interaction between managerial leaders and facilitators when implementing research evidence. Worldviews Evid Based Nurs. 2016;13(1):25–31. doi:10.1111/wvn.12138
11. Gifford WA, Squires JE, Angus DE, et al. Managerial leadership for research use in nursing and allied health care professions: a systematic review. Implementat Sci. 2018;13(1):1–23. doi:10.1186/s13012-018-0817-7
12. Abelsson T, Mortenius H, Karlsson AK, Bergman S, Baigi A. Evidence-based practice in primary healthcare from the managerial point of view - a national survey. BMC Health Serv Res. 2021;21(1):1014. doi:10.1186/s12913-021-07023-w
13. Musinguzi C, Namale L, Rutebemberwa E, Dahal A, Nahirya-Ntege P, Kekitiinwa A. The relationship between leadership style and health worker motivation, job satisfaction and teamwork in Uganda. J Healthc Leadersh. 2018;10:21–32. doi:10.2147/JHL.S147885
14. Mortenius H, Baigi A, Palm L, Fridlund B, Bjorkelund C, Hedberg B. Impact of the organisational culture on primary care staff members’ intention to engage in research and development. J Health Organ Manag. 2015;29(2):234–251. doi:10.1108/JHOM-03-2013-0067
15. Rea G. Factors affecting the adoption of evidence-based management among US healthcare administrators. Am J Manag. 2018;18(1):36–47.
16. Sonnino RE. Health care leadership development and training: progress and pitfalls. J Healthc Leadersh. 2016;8:19–29. doi:10.2147/JHL.S68068
17. Meza RD, Triplett NS, Woodard GS, et al. The relationship between first-level leadership and inner-context and implementation outcomes in behavioral health: a scoping review. Implement Sci. 2021;16(1):69. doi:10.1186/s13012-021-01104-4
18. Bergren MD, Maughan ED. Data and information literacy: a fundamental nursing competency. NASN Sch Nurse. 2020;35(3):140–142. doi:10.1177/1942602X20913249
19. Giannitrapani KF, Rodriguez H, Huynh AK, et al. How middle managers facilitate interdisciplinary primary care team functioning. Healthc. 2019;7(2):10–15. doi:10.1016/j.hjdsi.2018.11.003
20. Nieuwboer MS, van der Sande R, van der Marck MA, Olde Rikkert MGM, Perry M. Clinical leadership and integrated primary care: a systematic literature review. Eur J Gen Pract. 2019;25(1):7–18. doi:10.1080/13814788.2018.1515907
21. Bianchi M, Bagnasco A, Bressan V, et al. A review of the role of nurse leadership in promoting and sustaining evidence-based practice. J Nurs Manag. 2018;26(8):918–932. doi:10.1111/jonm.12638
22. Morsiani G, Bagnasco A, Sasso L. How staff nurses perceive the impact of nurse managers’ leadership style in terms of job satisfaction: a mixed method study. J Nurs Manag. 2017;25(2):119–128. doi:10.1111/jonm.12448
23. Birken S, Clary A, Tabriz AA, et al. Middle managers’ role in implementing evidence-based practices in healthcare: a systematic review. Implement Sci. 2018;13(1):149. doi:10.1186/s13012-018-0843-5
24. Spehar I, Sjovik H, Karevold KI, Rosvold EO, Frich JC. General practitioners’ views on leadership roles and challenges in primary health care: a qualitative study. Scand J Prim Health Care. 2017;35(1):105–110. doi:10.1080/02813432.2017.1288819
25. Haig BD. Exploratory factor analysis, theory generation, and scientific method. Multivariate Behav Res. 2005;40(3):303–329. doi:10.1207/s15327906mbr4003_2
26. Levin A. The Cochrane Collaboration. Ann Intern Med. 2001;135(4):309–312. doi:10.7326/0003-4819-135-4-200108210-00035
27. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
28. Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualitative content analysis: a discussion paper. Nurse Educ Today. 2017;56:29–34. doi:10.1016/j.nedt.2017.06.002
29. Gibeau É, Langley A, Denis J-L, van Schendel N. Bridging competing demands through co-leadership? Potential and limitations. Hum Relat. 2019;73(4):464–489. doi:10.1177/0018726719888145
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.