")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
A cross-sectional survey of night-time symptoms and impact of sleep disturbance on symptoms and health status in patients with COPD
Authors Ding B , Small M, Bergström G, Holmgren U
Received 16 September 2016
Accepted for publication 10 December 2016
Published 13 February 2017 Volume 2017:12 Pages 589—599
DOI https://doi.org/10.2147/COPD.S122485
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Bo Ding,1 Mark Small,2 Gina Bergström,1 Ulf Holmgren1
1Global Medical Affairs, AstraZeneca, Gothenburg, Sweden; 2Adelphi Real World, Bollington, UK
Background: Sleep disturbance has been termed the forgotten dimension of chronic obstructive pulmonary disease (COPD), but it is clinically important as most patients are affected. This study examined the incremental burden of illness associated with sleep disturbance in COPD, with reference to health status and disease impact, and the degree of concordance between physicians and patients in reporting night-time COPD symptoms.
Methods: Real-world data from >2,500 patients with COPD consulting for routine care were derived from respiratory Disease-Specific Programs conducted in Europe, the USA, and China. Night-time COPD symptom burden was assessed from patient and physician perspectives. Patients completed the Jenkins Sleep Evaluation Questionnaire (JSEQ), COPD assessment test (CAT), and EuroQol five-dimension questionnaire (EQ-5D). A regression approach was used to analyze the relationship between sleep disturbance (JSEQ score) and health status (EQ-5D score), adjusting for confounding variables.
Results: Frequency of night-time symptoms was high and was higher when reported by patients than physicians (69.7% and 65.7%, respectively). According to the JSEQ, 73.3% of patients had trouble falling asleep, 75.3% experienced night-time awakenings, 70.6% had trouble staying asleep, and 67.7% woke after a usual amount of sleep feeling worn out. Over half (52.7%) of patients received maintenance treatment where night-time symptom relief was stated by the physician as a treatment aim. A one unit increase in JSEQ score was associated with increased CAT score (0.7 units in Europe and the USA; 0.2 units in China). Sleep disturbance was significantly associated with worse health status (odds ratio [OR]: 1.27, 95% confidence interval [CI]: 1.18, 1.36, P<0.001 for Europe; OR: 1.23, 95% CI: 1.12, 1.38, P<0.001 for the USA; and OR: 1.19, 95% CI: 1.10, 1.28, P<0.001 for China).
Conclusions: Night-time symptoms and sleep disturbance are common among patients with COPD, and sleep disturbance has a detrimental impact on COPD symptoms and health status.
Keywords: COPD, night-time symptom, sleep disturbance, health status
Introduction
The process of sleep brings about changes in breathing patterns that further challenge the already suboptimal respiratory system of individuals with chronic obstructive pulmonary disease (COPD).1 This often leads to sleep disturbance due to abnormal breathing patterns (sleep-disordered breathing) and reduced sleep quality (diminished slow wave and rapid eye movement [REM] sleep).2,3
The reduced air flow and resultant hyperinflation associated with COPD accentuates the hypoventilation normally present during sleep, particularly during the REM phase.2,4 This leads to hypoxemia and hypercapnia, both of which have been associated with increased frequency of arousals during sleep.2,3 Moreover, hypoxemia may lead to cardiovascular (CV) consequences, including cardiac arrhythmias, pulmonary hypertension, and nocturnal death.2
Aside from underlying primary sleep disorders, patients with COPD often experience disturbed sleep or poor sleep quality as a result of the emergence of COPD symptoms during the night and/or early morning.2,5,6 Dyspnea, chronic cough, and sputum production can be particularly disruptive, and of these, cough appears to be the most frequently reported.5 Survey data collected under the 2009 Respiratory Disease-Specific Program (DSP) show high rates (78%) of night-time disturbance among patients with COPD.7
The consequences of sleep disturbance and reduced sleep quality for the health of patients with COPD are wide-ranging. Compared with unaffected individuals, patients with COPD experience more fatigue and lethargy, higher levels of depression, and have a reduced overall quality of life (QoL), all of which are likely influenced by sleep disturbance.6,8,9 Sleep disturbance also leads to small, but potentially important, reductions in forced vital capacity and forced expiratory volume in 1 second (FEV1).10 In addition, the presence of night-time symptoms is associated with more daytime breathlessness, more frequent COPD exacerbations, and greater maintenance therapy use.7 Interestingly, the side effects of some COPD medications may include sleep disturbance.11 In the most severe cases of COPD, the combination of altered night-time breathing and COPD can lead to respiratory failure.1
Despite the potential impact that sleep disturbance can have on patients with COPD, this aspect of the condition is frequently overlooked. In its most recent guidance, the Global Initiative for Chronic Obstructive Lung Disease11 mentions sleep disturbance only in the context of monitoring disease progression at follow-up.9 This coupled with the current lack of a formal validated definition of night-time symptomatology, which distinguishes night-time symptoms directly related to COPD from the symptoms of disturbed sleep, may serve to perpetuate the ongoing lack of clarity surrounding this topic.9
The objectives of this cross-sectional analysis of data derived from a recent respiratory DSP were 1) to examine the proportion of patients with COPD who are affected by sleep disturbance, as quantified by the non-disease-specific Jenkins Sleep Evaluation Questionnaire (JSEQ), a validated measure of sleep quality;12 2) to report the incremental burden of illness associated with sleep disturbance, with reference to health status and disease impact; 3) to examine the degree of concordance between physicians and their patients with respect to reporting on the frequency of night-time COPD symptoms; and 4) to examine if an association exists between physician-reported treatment of night-time symptoms and the patient-reported sleep disturbances according to the JSEQ.
Methods
The respiratory DSP is a cross-sectional survey designed to provide impartial observations of real-world clinical practice from a physician and matched patient perspective.13 The survey can be viewed as four discrete stages. In Stage A, primary care and specialist physicians are screened and recruited with a view to obtaining nationally representative samples. Individual face-to-face interviews then take place with the physician (Stage B) who completes patient record forms for the next five consecutive patients with COPD or asthma–COPD overlap syndrome (ACOS) recording clinical and treatment characteristics (Stage C). In the final Stage D, patients fill out a self-completion record, with no influence or input from a health care professional. The respiratory DSP was conducted in Q4 2013 in France, Germany, Italy, Spain, the UK, and the USA and in Q4 2010 in China (from hospital-based physicians only). The respiratory DSP adhered to market research guidelines and codes of conduct; therefore, ethics approval was not necessary to obtain and was not sought. All data were anonymized and aggregated prior to receipt by Adelphi Real World.
Survey population
Patients and physicians
The patient population comprised patients aged >40 years with physician-confirmed airflow obstruction and a diagnosis of COPD, consulting for routine care. This included patients with emphysema and chronic bronchitis and those with a concomitant diagnosis of asthma (ACOS). Physicians were eligible for participation in the study if they became medically qualified between 5 and 35 years ago and were responsible for the treatment of patients with asthma and those with COPD.
Variables
General and COPD-related variables
Outcome variables were recorded directly by the patient or physician or were derived from the physician- or patient-completed questionnaires (which included the full 8-item COPD Assessment Test [CAT], GlaxoSmithKline, Brentford, UK; mean CAT score; and CAT score range [0–9, 10–19, 20–29, and 30–40]). Descriptive variables recorded by the physician included age, gender, smoking status and history, comorbidities, most recent FEV1 (% predicted), number of exacerbations in the last 12 months, and currently prescribed medications for COPD.
Physicians were asked whether “improvement of night-time symptom relief” and/or “improvement of daytime symptom relief” were key reasons for the selection of COPD medication. Both physicians and patients were asked to provide information pertaining to the frequency of night-time COPD symptoms during the past 4 weeks.
Night-time symptoms
Night-time symptom frequency was measured by the patient and the physician. Both were asked, “During the past 4 weeks, how often have you/has this patient had symptoms during the night?” There were five possible answers: not at all, less than once a week, once or twice a week, 3 to 6 times per week, or every day.
Sleep disturbance
Sleep disturbance was quantified using the JSEQ, which was completed by the patient.12 Questions related to the ease with which patients fell asleep and to the number of night-time or early awakenings they typically experienced. Feelings of persistent tiredness or exhaustion following their usual amount of sleep were also reported.
Health status and functional impairment
The health status of the patient was determined from a physician-completed three-level version of the EuroQol five-dimension questionnaire (EQ-5D-3L).14 The health dimensions of mobility, self-care, usual activities, pain/discomfort, and anxiety/depression were rated according to three response options (no problems, some problems, and extreme problems). Patients also provided information on their psychological or functional impairment. They were asked whether they had ever experienced selected emotions as a result of their COPD (constant lack of energy, tiredness through lack of sleep, sickness, anxiety, feelings of sadness/depression, difficulty expressing feelings, embarrassment about their condition, or feelings of irritability).
Statistical analyses
Patient- and physician-reported general and COPD-related variables, including night-time symptom burden, were expressed using descriptive statistics. Across all analyses, data for patients from France, Germany, Italy, Spain, and the UK were grouped collectively as “Europe”. All analyses were performed using Stata 13.1 (StataCorp LP. Stata Statistical Software: Release 13. 2013).
Sleep disturbance
The proportion of patients with sleep disturbances during the past month, assessed using the JSEQ, was evaluated in terms of overall mean score and individual item scores for 1) trouble falling asleep, 2) trouble staying asleep, 3) waking up several times per night, and 4) waking up feeling tired and worn out after a usual amount of sleep. The response alternatives were not at all (0), 1–3 days (1), 4–7 days (2), 8–14 days (3), 15–21 days (4), and 22–31 days (5). In the absence of a validated threshold JSEQ score with which to classify “high” or “low” sleep disturbance, we used the raw continuous form of the scale, ranging from no sleep disturbance (score of 0) to high sleep disturbance (score of 20 indicating between 22 and 28 days of disturbed sleep for all four items in the JSEQ).
Logistic and linear regression modeling was used to quantify the relationship between JSEQ score and health status, as measured by the EQ-5D-3L, whilst adjusting for confounding variables (including age, gender, physician-confirmed diagnosis of depression, anxiety, sleep apnea, serious CV conditions, and number of severe exacerbations in the last 12 months requiring an emergency department visit or hospitalization [as a proxy for severity]).
Health status
EQ-5D-3L responses were used to calculate a utility score, which ranged between 0 (worst health imaginable) and 1 (best health imaginable). Given that the bimodal distribution of the EQ-5D does not lend itself well to a single regression, a two-part modeling process was used. Logistic regression was first used to determine whether patients had perfect health, using the JSEQ and the confounding variables listed above as predictor variables. Standard ordinary least squares regression was then used for the patients in poor health using the same set of predictor variables. Perfect health was defined as an EQ-5D-3L score of 1 and non-perfect health <1. For the logistic regression, an odds ratio >1 represented the change in odds of a non-perfect health for a unit increase in JSEQ score. For the linear regression of JSEQ score with EQ-5D, a positive coefficient was associated with a patient with worse health status (lower EQ-5D score). A higher/lower value of the coefficient indicated a greater effect of the variable.
CAT score
The distribution of CAT scores allowed for analysis according to an ordinary least squares regression model. The predictor variables consisted of the JSEQ score and the confounding variables, as stated above. To eliminate any potential impact of the CAT sleep component on the overall measurement of health status, a 7-item version of the CAT was implemented, from which the sleep component was excluded. A positive coefficient was associated with a higher CAT score.
Concordance between physician- and patient-reported night-time COPD symptoms
Weighted kappa statistics15 were used to measure the concordance of reporting of night-time COPD symptoms by physicians and patients.
Results
Study population
Of the total patient sample from the respiratory DSP survey who had data collected within the observation period (N=4,143), 2,504 patients were eligible for inclusion in the study population (Tables 1 and 2). The majority (65.1%) of the study population were males and the mean (standard deviation [SD]) age was 64.6 (10.7) years. A high proportion (40.1%) of patients in the cohort from China had never smoked, in contrast to the patient cohorts from Europe and the USA (in which “never smoked” rates were 6.3% and 4.9%, respectively; Table 2).
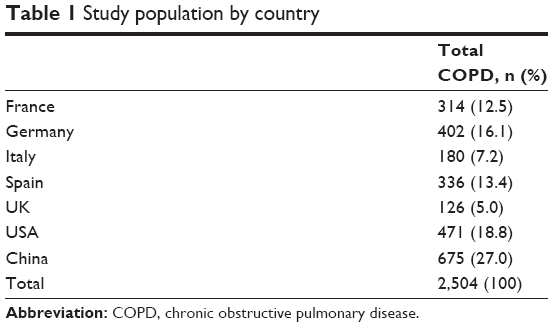 | Table 1 Study population by country |
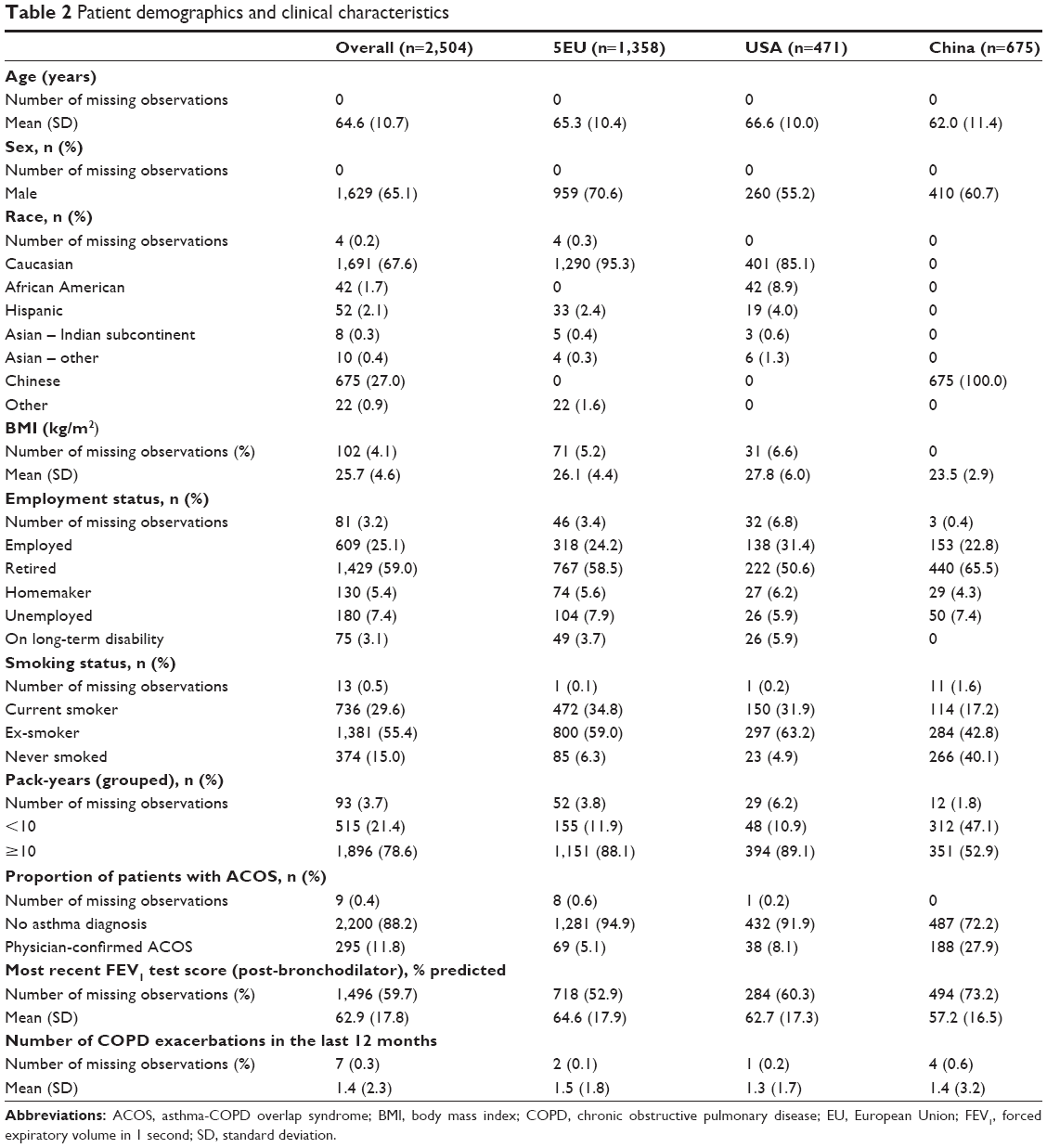 | Table 2 Patient demographics and clinical characteristics |
Clinical characteristics and COPD symptom score
For the population as a whole, the most recent mean (SD) post-bronchodilator FEV1 was 62.9% (17.8) of the predicted value (Table 2), in the range classified as moderate airflow limitation (50% ≤FEV1 <80% predicted).11 The mean (SD) number of exacerbations in the last 12 months was 1.4 (2.3). Common non-CV-related comorbidities including diabetes, arthritis, and anxiety were reported in 15.1%, 13.8%, and 12.0% of patients, respectively. Sleep apnea was reported in 5.1% of the study population. Of CV-related comorbidities, arterial hypertension was the most common and was reported in 55.2% of patients, whereas elevated cholesterol/hyperlipidemia was reported in 26.4% of patients. Serious CV conditions (a collective term encompassing angina, cardiac arrhythmia, cerebrovascular disease, and/or stroke; coagulated blood-clotting disorder; myocardial infarction; thrombosis; congestive heart failure; peripheral vascular disease; and coronary artery disease) were reported in 28.5% of patients.
COPD symptom scores were generally higher among patients in the cohort from China (mean [SD] CAT score 24.8 [6.1]) compared with the cohorts from Europe (20.5 [8.4]) and the USA (20.4 [8.6]; Table 3). Similarly, China had the greatest proportion of patients with a mean CAT score of ≥10 (98.5%) in comparison with 88.9% for Europe and 86.5% for the USA. For the entire study population, 91.2% of patients had a mean CAT score of ≥10 and 64.6% of patients had a mean CAT score of ≥20 (Table 3).
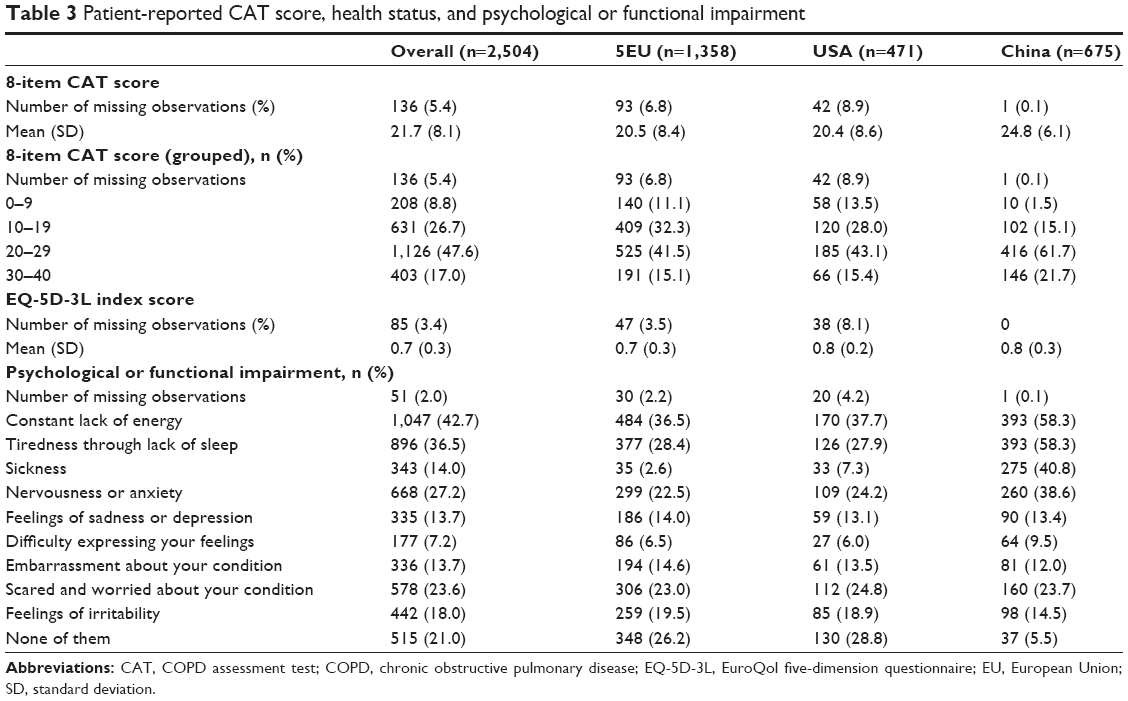 | Table 3 Patient-reported CAT score, health status, and psychological or functional impairment |
Night-time symptoms
Surveyed physicians in Europe and the USA reported that 65.7% of patients had night-time symptoms during the last 4 weeks, with 23.2% of patients experiencing night-time symptoms on a weekly or twice weekly basis. Physicians reported that 8.2% of their patients had night-time symptoms on a daily basis (Figure 1A). Corresponding patient-reported rates were generally higher, as 69.7% said that they experienced night-time symptoms during the last 4 weeks, 25.5% of patients reported night-time symptoms occurring at least once or twice per week, and 9.2% said that they experienced night-time symptoms every day (Figure 1B). Rates of agreement between physician and patient reports of the frequency of night-time symptoms were 88.9% and 85.6% (P<0.001 for both) for Europe and the USA (weighted kappa scores of 0.68 and 0.60, respectively). This indicated borderline moderate–substantial concordance between physicians and patients as sources of information. The mean (SD) JSEQ score for the entire study population was 6.1 (4.8). Night-time awakening was the most common characteristic of sleep disturbance, which was reported as occurring at least 1–3 times in the last 28 days in 75.3% of patients (Table 4).
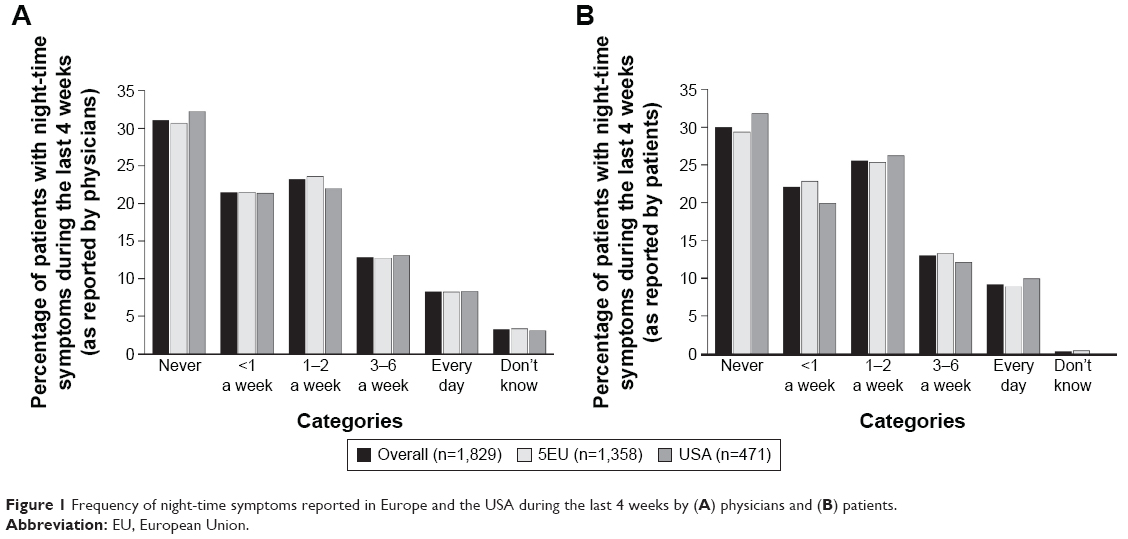 | Figure 1 Frequency of night-time symptoms reported in Europe and the USA during the last 4 weeks by (A) physicians and (B) patients. |
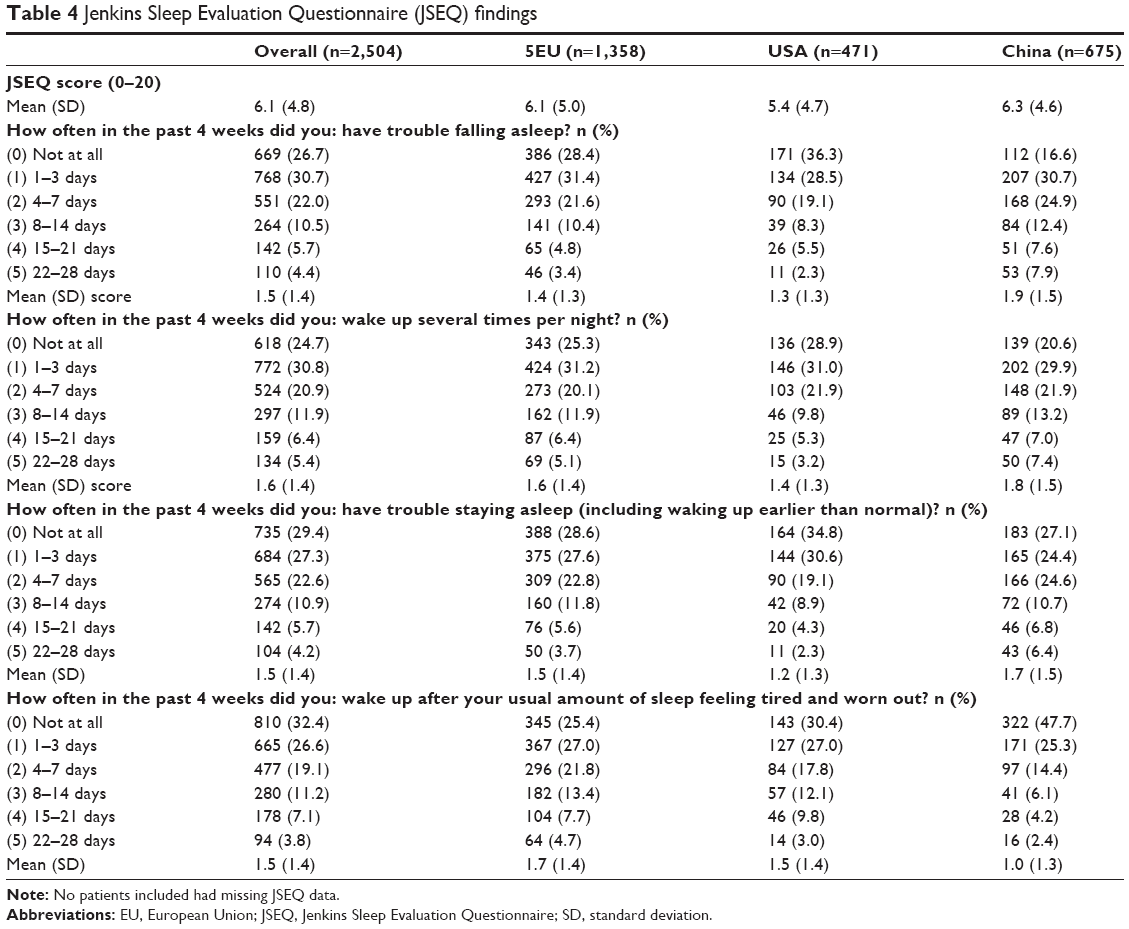 | Table 4 Jenkins Sleep Evaluation Questionnaire (JSEQ) findings |
Health status and psychological or functional impairment
The overall mean (SD) health status for the entire population, in terms of EQ-5D-3L score, was 0.7 (0.3). Patients in the USA and China showed a marginally better health status (0.8) compared with those in Europe (0.7; Table 3). Tiredness through lack of sleep was reported in 36.5% of the population as a whole, with more than half (58.3%) of patients surveyed in China reporting such an impairment (Table 3). A constant lack of energy was reported by 42.7% of patients overall.
Logistic regression analysis of patients in Europe revealed a significant association between increased sleep disturbance, as measured using the JSEQ, and worse health status (EQ-5D-3L score: <1; OR: 1.27, 95% CI: 1.18, 1.36, P<0.001). Similar associations were also found for patients surveyed in the USA (OR: 1.23, 95% CI: 1.12, 1.38, P<0.001) and China (OR: 1.19, 95% CI: 1.10, 1.28, P<0.001; Table 5).
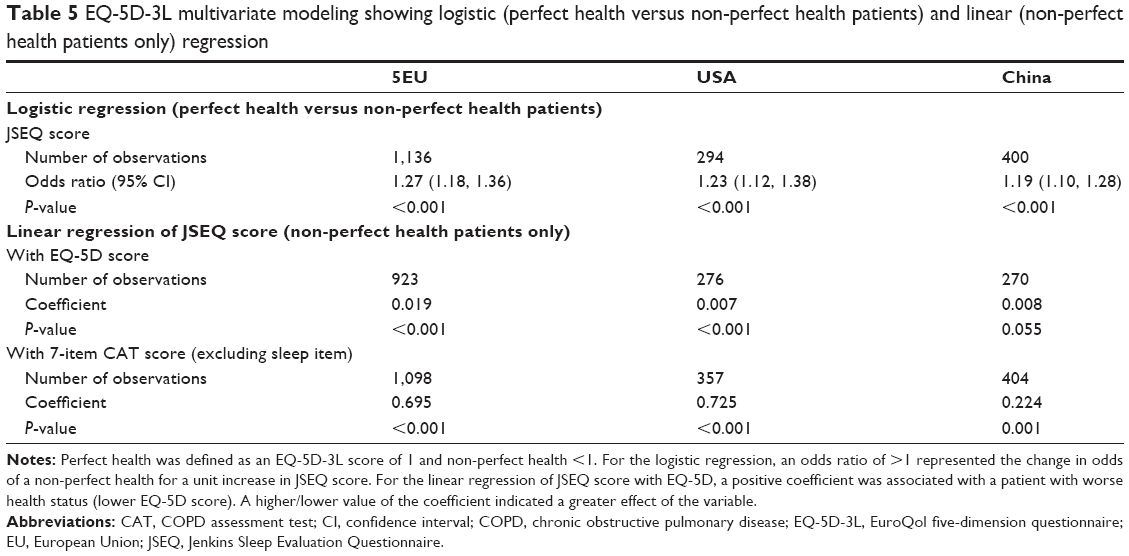 | Table 5 EQ-5D-3L multivariate modeling showing logistic (perfect health versus non-perfect health patients) and linear (non-perfect health patients only) regression |
Symptoms
Linear regression analysis revealed a significant association between JSEQ score and the adapted 7-item CAT score, showing that increasing sleep disturbances had a significant impact on COPD symptoms (Europe, coefficient: 0.695, P<0.001; USA, coefficient: 0.725, P<0.001; China, coefficient: 0.224, P=0.001; Table 5). Therefore, for patients surveyed in Europe and the USA, an increase of 1 in JSEQ score was associated with a 0.7 increase in the CAT score, indicating a greater effect of sleep disturbance on the CAT score than was observed in patients surveyed in China.
Current treatment of COPD and reason for medication prescription
In Europe and the USA, the physician responsible for treatment decisions was a pulmonologist or equivalent for 56.9% and 53.7% of patients respectively. All patients surveyed in China received care from a hospital-based respiratory specialist (Table 6). The majority of patients were receiving maintenance treatment, with an inhaled corticosteroid/long-acting β2-agonist (LABA) combination accounting for 30.5% of current treatment regimens, triple therapy accounting for 24.7%, and long-acting muscarinic antagonists (LAMAs) accounting for 13.4%. LAMA/LABA combination therapy accounted for 6.0% of current treatment (Table 6). The relatively high “other” category among patients surveyed in China reflected high prescribing of xanthine that was not observed in Europe or the USA. Overall, in just over half (52.7%) of patients, physicians stated that they made their treatment choice on the basis of night-time symptoms, with this proportion notably higher among the cohort from China (69.9%; Table 6). Targeting daytime symptoms was cited as the reason for current treatment choice in 65.7% of patients, rising to 76.9% of patients in China.
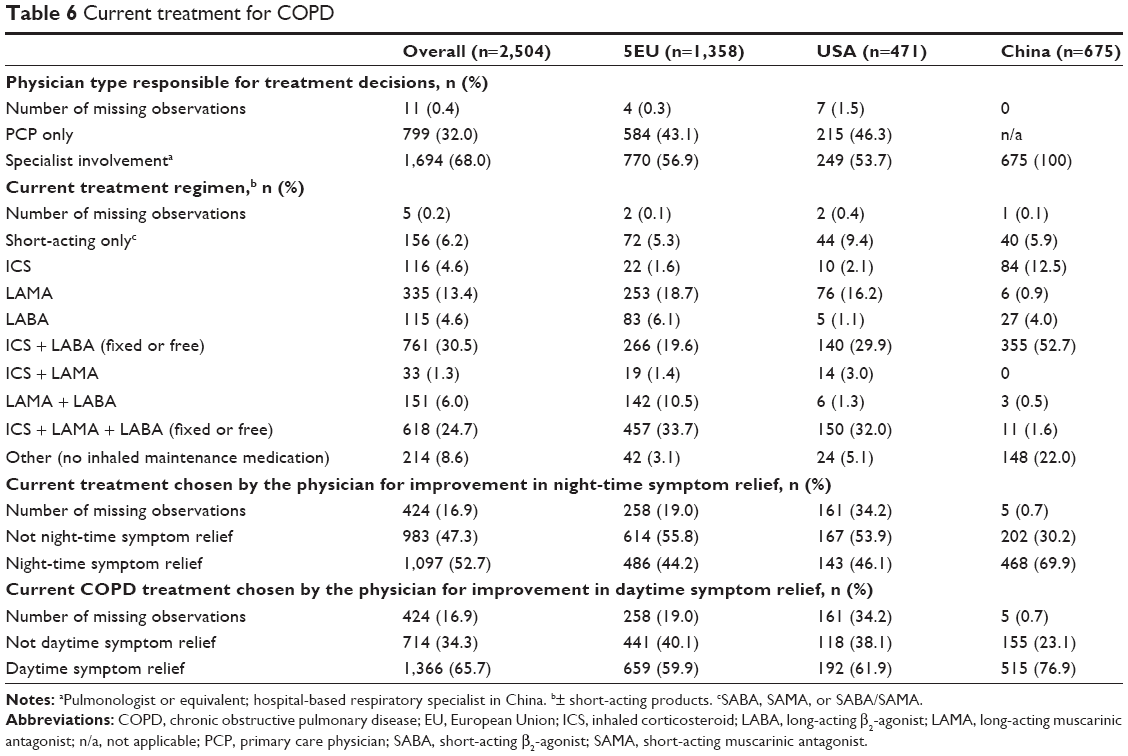 | Table 6 Current treatment for COPD |
Discussion
This study examined the effect of sleep disturbance on symptoms and health status among patients with COPD managed in a real-world treatment setting and surveyed as part of a respiratory DSP. Our findings show that the majority (≥66%) of patients had at least some night-time symptoms and associated sleep disturbance over a monthly period, with ≥8% of patients experiencing night-time symptoms on a daily basis.
Quality of sleep was quantified using the validated JSEQ instrument, on which a mean score of 6.1 was recorded for our study population as a whole. However, it should be noted that JSEQ is not a COPD-specific instrument and other non-COPD reasons may also have contributed to the sleep quality reported in this study. JSEQ scores were generally similar between the geographical regions tested, with the cohort from the USA showing a slightly lower score (5.4) than that from Europe or China, indicative of marginally better sleep quality. Previous research in a middle-aged population determined that a JSEQ score ≥3 was sufficient to identify patients with frequent sleep complaints (indicative of sleep disturbance at least once a week during the previous month).16 Across JSEQ categories, the proportion of the total population surveyed in our study with a JSEQ score ≥3 ranged from 20.6% to 23.6%, with night-time awakening representing the most common characteristic of sleep disturbance. This may tie in with patient-reported psychological or functional scores, which were highest for “constant lack of energy” (42.7%) and “tiredness through lack of sleep” (36.5%).
In our study, almost three-quarters of patients had experienced at least one JSEQ category of night-time sleep disturbance, as evidenced by a JSEQ score >0. Such problems included trouble falling asleep, waking up several times per night, trouble staying asleep, and feeling tired and worn out after having the usual amount of sleep. This figure is consistent with that reported in a previous COPD DSP survey in which 78% of patients with COPD in five European countries reported night-time disturbance (JSEQ score >0 within last 28 days).7 In both studies, sleep disturbance was accompanied by a relatively high frequency of night-time symptoms, with the frequency of symptoms likely to be underestimated, to varying degrees, if reported by the physician rather than the patient. Generally, however, our study found moderate–substantial rates of concordance between physician and patient reports of night-time symptoms. This level of agreement is perhaps surprising, given the apparent lack of physician awareness surrounding night-time symptoms that has been reported in the literature.2,9 It is possible that the “awareness” reported herein reflects the direct questioning of physicians about night-time symptoms, specifically. The proportion of physicians who prescribed medication with the alleviation of night-time symptoms in mind did not correlate with the purported high rate of symptom recognition.
In the overall population, current medication was prescribed for improvement in night-time symptom relief in only half of the patients (52.7%). This rate was substantially higher in the cohort from China (69.9%) and may be reflective of the country’s health care system, where patient consultations typically occur in hospitals when patients are symptomatic and are more suggestive of emergency care than routine visits. Although the majority of the overall population was considered symptomatic (>91% of patients had CAT scores of ≥10), patients from China demonstrated a higher symptom burden than other regions, as evidenced by almost all patients (98.5%) showing a CAT score ≥10, and this may have driven the need for medication for both night-time and daytime symptom relief.
That deficits in sleep quality persisted, even when emergence of night-time symptoms was recognized and medication given, is cause for concern. “Tiredness through lack of sleep” was reported in more than half (58.3%) of patients surveyed in China, despite the acknowledged higher rates of targeted medication prescribing in this cohort versus the overall population. This may suggest that physicians generally lack clear understanding of the burden of night-time symptoms and are not prescribing the most appropriate medications. The possibility that physicians were knowingly prescribing medication for sleep disturbance that was unrelated to COPD cannot be discounted. By including confounding variables, we were able to determine with some confidence whether physicians chose treatment for night-time symptoms because of patients’ complaints of sleep disturbance. However, we were unable to adjust for therapeutic effects, and results should, therefore, be interpreted with a certain degree of caution.
Regular disturbance of sleep, possibly as a result of the emergence of night-time COPD symptoms, is linked with deficits in sleep efficiency (the ratio of estimated total sleep time and total time spent in bed) and impaired sleep quality among patients with COPD.2,9,17 Sleep-quality deficits have been shown to affect the vast majority of patients with COPD, with rates in excess of 70% reported in the literature.18,19 If left unmanaged, evidence suggests that sleep deficiencies will gradually encroach upon daytime activities. Impaired sleep quality has been associated with low daytime energy levels, chronic fatigue, daytime sleepiness, and impairments in patient-reported QoL.2 It is likely of course that the cycle of interrupted sleep and daytime lethargy is self-perpetuating, with a retrospective analysis of sleep quality in patients with severe COPD identifying daytime hypoxemia as a predictor of sleep efficiency.17
We were able to demonstrate a strong and significant relationship between the increasing frequency of sleep disturbance according to JSEQ score, and worsening health status, as measured by the EQ-5D-3L. Such findings are in broad agreement with previous studies, which have linked sleep disturbance, and poor sleep quality in particular, with deficits in the QoL of patients with COPD of varying severity.5,18–22 There is some evidence to directly link the severity of COPD disease progression with sleep quality and, ultimately, QoL or health status.20
The CAT has been used previously to show the impact of COPD on health status in the context of night-time or early-morning symptoms in a cross-sectional survey of 1,239 patients with COPD, identified using US medical and pharmacy claims data.5 The emergence of either symptom type was significantly associated with poorer health status (in terms of CAT score). In our study, we used a modified version of the CAT, in which the original sleep component was excluded, as a measurement for COPD symptoms. The CAT scores indicated that the majority (>91%) of the population were symptomatic (CAT score ≥10). Regression analyses showed a significant association between JSEQ score and 7-item CAT score, indicating that increasing sleep disturbance had a significant impact on COPD symptoms. However, it could be argued that the reverse is also true, with progressively more symptomatic patients being associated with an increasing number of sleep complaints.17
The findings from this study should be interpreted in light of certain limitations. The most recent mean post-bronchodilator FEV1 for the whole population (62.9% of predicted) was in the range associated with moderate airflow limitation (50% ≤FEV1 <80% predicted) and therefore it may be less likely that these patients will have sleep-related issues.11 However, spirometry data were missing for 59.7% of patients. The survey also included only those patients who were consulting their physician and, as such, the generalizability of the findings to the COPD population as a whole is unknown. Furthermore, our study enrolled patients presenting within both primary and specialist care settings and was not designed to evaluate potential differences in night-time symptoms and sleep disturbance between these two groups. Given the reasonable assumption that patients managed under specialist care were more severely affected by COPD, higher rates of sleep disturbance may perhaps have been anticipated among these patients.
The quality of our data was reliant on accurate reporting of information by physicians and patients. The prospective consecutive sampling approach was designed to limit patient selection bias. However, its success was highly dependent on the integrity of the participating physician and adherence to this instruction could not be verified. In addition, for many patients treatment decisions were made by primary care physicians rather than respiratory specialists, which may have affected outcomes.
Conducted in a real-world setting and covering a broad geographical area, our study revealed the widespread occurrence of night-time symptoms and sleep disturbance in patients with COPD. Importantly, disrupted sleep was associated with the worsening of both symptoms and health status, serving to underline the importance of an effective management strategy that directly addresses sleep disturbances. While physicians may acknowledge that the majority of patients with COPD experience night-time respiratory symptoms (≥66% over a 4-week period), this doesn’t always appear to translate into disease-management practice, given that only 53% of patients currently receive medication specifically targeting night-time symptomatology. This research provides further evidence of the need to address night-time symptoms and associated sleep disturbances (in addition to the detrimental daytime symptoms of dyspnea and breathlessness) in order to bring about improvements in patients’ QoL.
Conclusion
Night-time COPD symptoms and sleep disturbance are common among patients with COPD, and sleep disturbance has a detrimental impact on symptoms, health status, and QoL. The burden of COPD night-time symptoms needs to be considered relative to that of COPD daytime symptoms in order to fully understand its impact on patients’ lives. This study shows that despite physicians acknowledging that most patients with COPD experience night-time symptoms, this does not appear to translate into disease management practice and highlights the clinical need to address night-time symptoms with tailored treatment approaches.
Acknowledgments
This study was supported by AstraZeneca. Medical writing support was provided by Caroline Shepherd and Thomas Owens of Complete Medical Communications, funded by AstraZeneca.
The authors wish to thank Stuart Blackburn, a senior statistician and employee of Adelphi Real World, who provided analytical support.
Author contributions
All authors contributed to conception and design of the study/analyses. MS carried out data and statistical analyses and data acquisition. All authors participated in data interpretation and manuscript drafting, reviewing, and development.
Disclosure
Ulf Holmgren, Gina Bergström, and Bo Ding are employees of AstraZeneca. Mark Small is an employee of Adelphi Real World. The authors report no other conflicts of interest in this work.
References
Zamarron C, Garcia PV, Morete E, del Campo MF. Association of chronic obstructive pulmonary disease and obstructive sleep apnea consequences. Int J Chron Obstruct Pulmon Dis. 2008;3(4):671–682. | ||
McNicholas WT, Verbraecken J, Marin JM. Sleep disorders in COPD: the forgotten dimension. Eur Respir Rev. 2013;22(129):365–375. | ||
Cormick W, Olson LG, Hensley MJ, Saunders NA. Nocturnal hypoxaemia and quality of sleep in patients with chronic obstructive lung disease. Thorax. 1986;41(11):846–854. | ||
Krachman S, Minai OA, Scharf SM. Sleep abnormalities and treatment in emphysema. Proc Am Thorac Soc. 2008;5(4):536–542. | ||
Stephenson JJ, Cai Q, Mocarski M, Tan H, Doshi JA, Sullivan SD. Impact and factors associated with nighttime and early morning symptoms among patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2015;10:577–586. | ||
Budhiraja R, Siddiqi TA, Quan SF. Sleep disorders in chronic obstructive pulmonary disease: etiology, impact, and management. J Clin Sleep Med. 2015;11(3):259–270. | ||
Price D, Small M, Milligan G, Higgins V, Gil EG, Estruch J. Impact of night-time symptoms in COPD: a real-world study in five European countries. Int J Chron Obstruct Pulmon Dis. 2013;8:595–603. | ||
Breslin E, van der SC, Breukink S, et al. Perception of fatigue and quality of life in patients with COPD. Chest. 1998;114(4):958–964. | ||
Agusti A, Hedner J, Marin JM, Barbe F, Cazzola M, Rennard S. Night-time symptoms: a forgotten dimension of COPD. Eur Respir Rev. 2011;20(121):183–194. | ||
Phillips BA, Cooper KR, Burke TV. The effect of sleep loss on breathing in chronic obstructive pulmonary disease. Chest. 1987;91(1):29–32. | ||
Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Diseases (GOLD); 2016 [updated 2016]. Available from: http://www.goldcopd.org. Accessed June 16, 2016. | ||
Jenkins CD, Stanton BA, Niemcryk SJ, Rose RM. A scale for the estimation of sleep problems in clinical research. J Clin Epidemiol. 1988;41(4):313–321. | ||
Anderson P, Benford M, Harris N, Karavali M, Piercy J. Real-world physician and patient behaviour across countries: Disease-Specific Programmes – a means to understand. Curr Med Res Opin. 2008;24(11):3063–3072. | ||
Rabin R, de CF. EQ-5D: a measure of health status from the EuroQol Group. Ann Med. 2001;33(5):337–343. | ||
Cohen J. Weighted kappa: nominal scale agreement with provision for scaled disagreement or partial credit. Psychol Bull. 1968;70(4):213–220. | ||
Lallukka T, Rahkonen O, Lahelma E, Arber S. Sleep complaints in middle-aged women and men: the contribution of working conditions and work-family conflicts. J Sleep Res. 2010;19(3):466–477. | ||
McSharry DG, Ryan S, Calverley P, Edwards JC, McNicholas WT. Sleep quality in chronic obstructive pulmonary disease. Respirology. 2012;17(7):1119–1124. | ||
Nunes DM, Mota RM, de Pontes Neto OL, Pereira ED, de Bruin VM, de Bruin PF. Impaired sleep reduces quality of life in chronic obstructive pulmonary disease. Lung. 2009;187(3):159–163. | ||
Scharf SM, Maimon N, Simon-Tuval T, Bernhard-Scharf BJ, Reuveni H, Tarasiuk A. Sleep quality predicts quality of life in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2010;6:1–12. | ||
Dignani L, Toccaceli A, Lucertini C, Petrucci C, Lancia L. Sleep and quality of life in people with COPD: a descriptive-correlational study. Clin Nurs Res. 2015;25(4):432–447. | ||
Soler-Cataluna JJ, Sauleda J, Valdes L, et al. [Prevalence and perception of 24-hour symptom patterns in patients with stable chronic obstructive pulmonary disease in Spain]. Arch Bronconeumol. 2016;52(6):308–316. Spanish. | ||
Hynninen MJ, Pallesen S, Nordhus IH. Factors affecting health status in COPD patients with co-morbid anxiety or depression. Int J Chron Obstruct Pulmon Dis. 2007;2(3):323–328. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.