")
Back to Journals » International Journal of Women's Health » Volume 14
A Cross-Sectional Study on the Quality of Life in Women with Endometrioma
Authors Thammasiri C , Amnatbuddee S , Sothornwit J , Temtanakitpaisan T , Buppasiri P
Received 27 September 2021
Accepted for publication 28 December 2021
Published 11 January 2022 Volume 2022:14 Pages 9—14
DOI https://doi.org/10.2147/IJWH.S341603
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Chutikarn Thammasiri, Siriruthai Amnatbuddee, Jen Sothornwit, Teerayut Temtanakitpaisan, Pranom Buppasiri
Department of Obstetrics and Gynecology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Siriruthai Amnatbuddee
Department of Obstetrics and Gynecology, Faculty of Medicine, Khon Kaen University, 123 Mittraphap Road, Muang District, Khon Kaen, 40002, Thailand
Tel +66817396331
Email [email protected]
Purpose: To evaluate the quality of life (QoL) of women with endometrioma and explore the associated factors.
Patients and Methods: A cross-sectional study was conducted between August 2020 and March 2021. A total of 99 women diagnosed with ovarian endometrioma with at least one endometriosis-associated symptom completed the Endometriosis Health Profile 30 (EHP-30) questionnaire for their QoL score before treatment for ovarian endometrioma. The questionnaire comprises a central questionnaire (30 items) and a modular questionnaire (23 items divided into 6 sections). Demographics and QoL scores were analyzed using descriptive statistics and multivariable linear regression or median regression.
Results: The mean QoL score was 35.0± 15.8 (range, 16.0± 21.2 in the social support dimension to 45.1± 24.4 in the control and powerlessness dimension). In the modular questionnaire, the highest score was in the infertility domain, while the lowest was in the relationship with the physician domain. The pain score and chronic pelvic pain (CPP) were independent correlation factors for a higher total EHP-30 score: the higher the total EHP-30, the poorer the QoL. CPP was positively correlated with the QoL score in the work domain.
Conclusion: The present study revealed that CPP was the factor associated with a worse QoL and work performance in women with endometrioma based on a disease-specific, EHP-30 questionnaire.
Keywords: endometriosis, pelvic pain, infertility, EHP-30
Introduction
Endometriosis is defined as the presence of endometrial-like tissue outside the uterus and the most frequent type is pelvic endometriosis. The disease affects approximately 1 in 10 women of reproductive age and almost half of the women with infertility. Endometriosis-associated pelvic pain (EAPP) is the most common presentation, including dysmenorrhea, chronic pelvic pain (CPP), and dyspareunia.1,2
The treatment costs for endometriosis are substantial, resulting in an economic burden similar to the estimated annual health care costs for diabetes mellitus, Crohn’s disease, and rheumatoid arthritis.3 Endometriosis, particularly EAPP, hampers daily life, sexual life, health-related quality of life (HRQoL), and work productivity.4–6 Furthermore, endometriosis-related infertility aggravates an emotional response and interferes with close relationships.7,8 A holistic approach is thus needed and should include evaluating the physical, emotional, social, and spiritual health of women with endometriosis.
East Asian women are more likely to have endometriosis than Caucasians.9 Nevertheless, most of the quality of life (QoL) studies have been conducted in Europe and the USA,10,11 and the majority of studies have assessed QoL using non-disease-specific tools.6,12,13 We, therefore, conducted a cross-sectional study to evaluate the HRQoL of Thai women with endometriosis and the associated factors using a questionnaire designed for women with endometriosis (the Endometriosis Health Profile – 30 (EHP-30) questionnaire).
Materials and Methods
The cross-sectional study was reviewed and approved by the Khon Kaen University Ethics Committee in Human Research (HE631144) before enrolling the first patient. The study was conducted between August 2020 and March 2021 at the Gynecology Outpatient Clinic at Srinagarind Hospital, Khon Kaen University, Thailand. The inclusion criteria were: (a) patients were 18 or over; (b) presentation of symptom(s) of endometriosis accompanied by ultrasonographic findings of ovarian endometrioma. The diagnosis of endometrioma was based on the transvaginal ultrasonographic (TVS) finding: ground glass echogenicity and one to four loculated without papillary structures and detectable blood flow.14 (c) hormonal treatment-free for at least 3 months; and, (d) willing to participate in the study. Women were excluded if the following were found (a) no evidence of endometriosis during surgery; (b) pelvic inflammatory disease or painful gynecological cancer diagnosed by a gynecologist; (c) psychotic disorder diagnosed by a psychiatrist; and/or (d) anti-depressive drug use affecting sexual function.
After obtaining written informed consent, participants were interviewed, and their medical records examined. Interviews were conducted to establish patient baseline characteristics (age, educational level, marital status, occupation, duration since first symptoms, duration from first symptoms to diagnosis, symptoms of endometriosis, ultrasonographic findings, and EAPP pain score). Participants were then asked to complete the Endometriosis Health Profile-30 (EHP-30) questionnaire Thai version. The EHP-30 was developed by Jones et al in 2001. It is a disease-specific, reliable, valid questionnaire for measuring the effects of endometriosis on HRQoL, especially on the physical, psychological and social aspects.15 The questionnaire consists of a central section comprising 30 items and a modular section comprising 23 items distributed into 6 sections (Work – Section A, Relationship with Children – Section B, Sexual Relations – Section C, Relationship with Physician – Section D, Treatment – Section E, and Infertility – Section F. The score ranged between 0 (Best QoL) and 100 (Worst QoL). The primary outcome was the QoL score, and secondary outcomes were the factors associated with QoL. Infertility was defined as being unable to conceive after having regular unprotected intercourse for one year.
The data were analyzed using STATA/SE version 10.0 for a descriptive analysis of the demographics and multivariate linear regression analysis to explore the correlation between factors and the QoL score. Statistical significance was attributed when p < 0.05, with a confidence interval (CI) of 95%. For EHP 30 score, univariable analysis by simple linear regression was performed to assess the relationships between demographic data and QoL score. Covariates with p values ≤ 0.20 in the univariable analysis were eligible for multivariable, multiple linear regression modeling. For non-normal distribution data, Spearman’s rank, Kruskal–Wallis and Mann–Whitney test were performed to assess the relationships between demographic data and QoL score in Modular questionnaire as appropriate. Covariates with p values ≤ 0.20 in the univariable analysis were eligible for multivariable, median regression modeling.
Results
Of the 126 women who were screened, 99 had endometrioma and were recruited to the study. All patients completed the questionnaire, and the resulting baseline characteristics are summarized in Table 1. The mean age was 35.2±7.3 years. The mean age of menarche was 13 ±1.7 years while the median time of first symptoms to diagnosis was 5.0 years (range, 0–18 years). The most common symptoms associated with endometriosis were dysmenorrhea (97.0%). Pain score ranged between 3 and 10 and two-thirds of participants had severe pain.
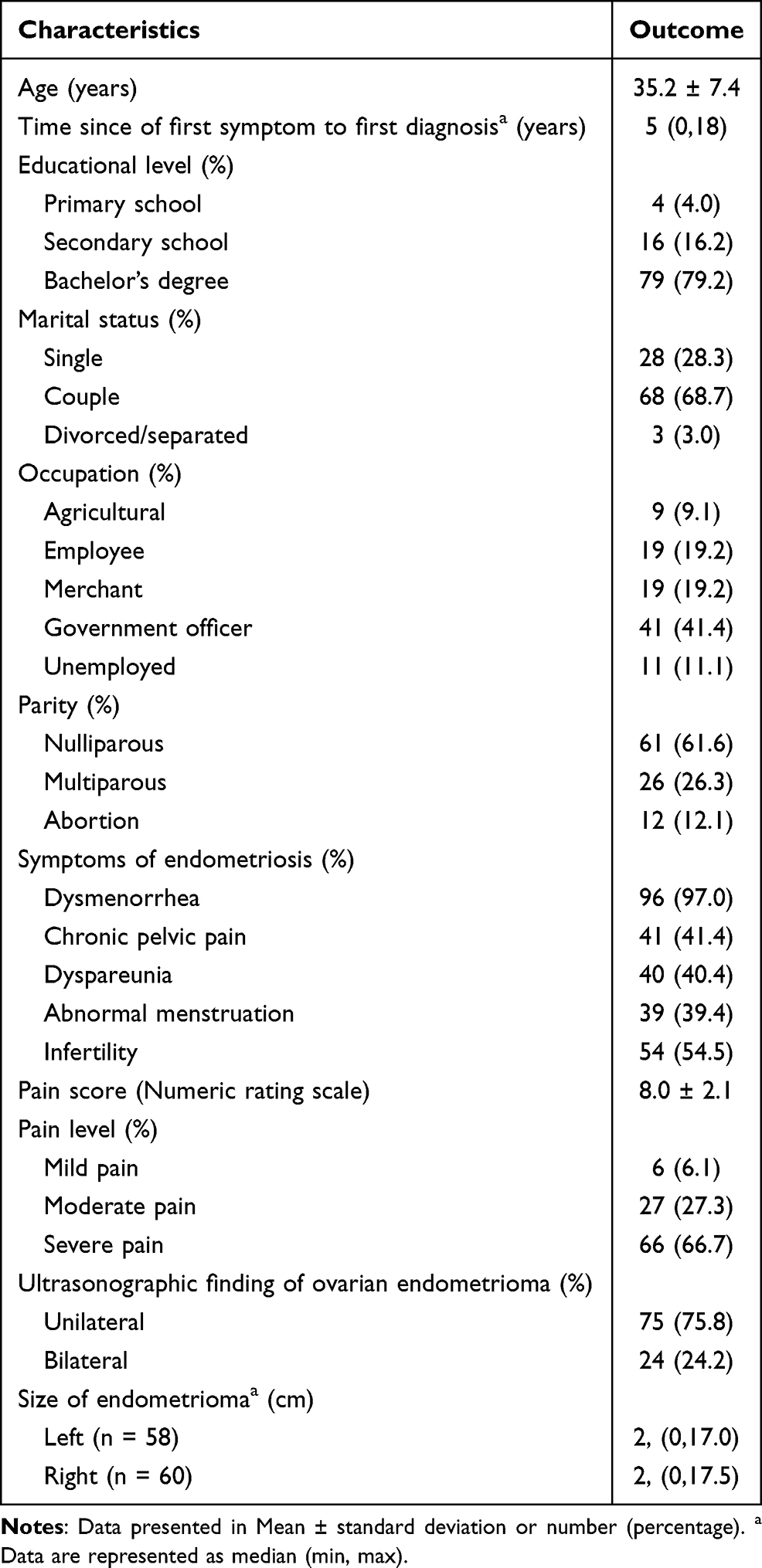 |
Table 1 Baseline Characteristics of Patients with Endometriosis (n = 99) |
The EHP-30 score for both the central and modular questionnaires was transformed into a scoring system that ranged between 0 and 100. The mean score of the central questionnaire or mean QoL score was 35.0±15.9. The maximum mean score of 45.1±24.4 was in the Control and Powerlessness dimension, while the minimum mean score of 16.0±21.2 was in the Social Support dimension. As 81.8% of the women with endometriosis reported they had to lie down because of the pain, 77.8% generally felt unwell, and 73.7% found it difficult to exercise or do leisure activities because of pain in daily life activities. These items were in the Control and Powerlessness together with Pain dimensions. Table 2 shows the QoL of Modular questionnaires. The maximum median score was 34.4 (IQR 6.3, 50.0) in the Infertility section. Of these, 69.9% of the respondents felt worried about the chances of not having children or more children, and 53.4% felt inadequate because they may not/have not been able to have children.
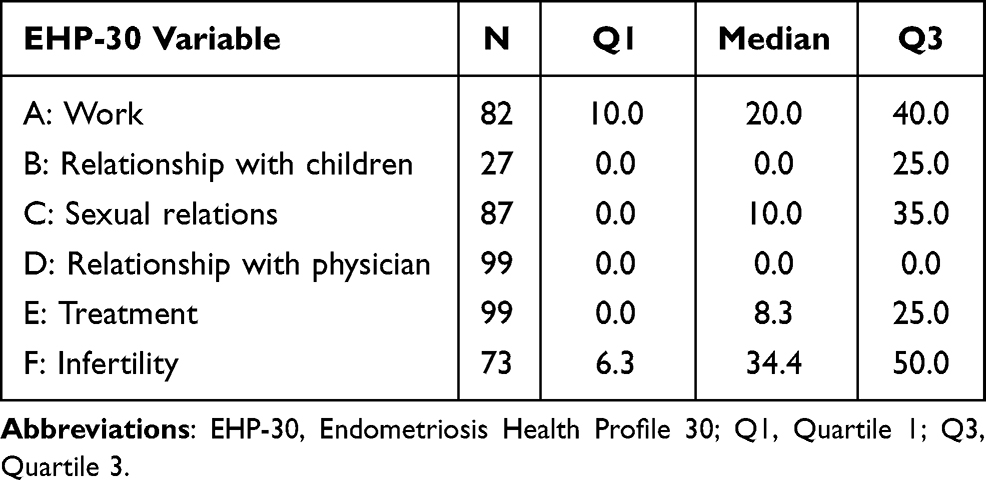 |
Table 2 Descriptive Statistics for the Modular EHP-30 Questionnaires |
The univariable analysis revealed that age, marital status, body mass index (BMI), CPP, and pain score were correlated with the QoL score. However, in the multivariable linear regression analysis, only the pain score and CPP were associated with the total EHP-30 score (Table 3).
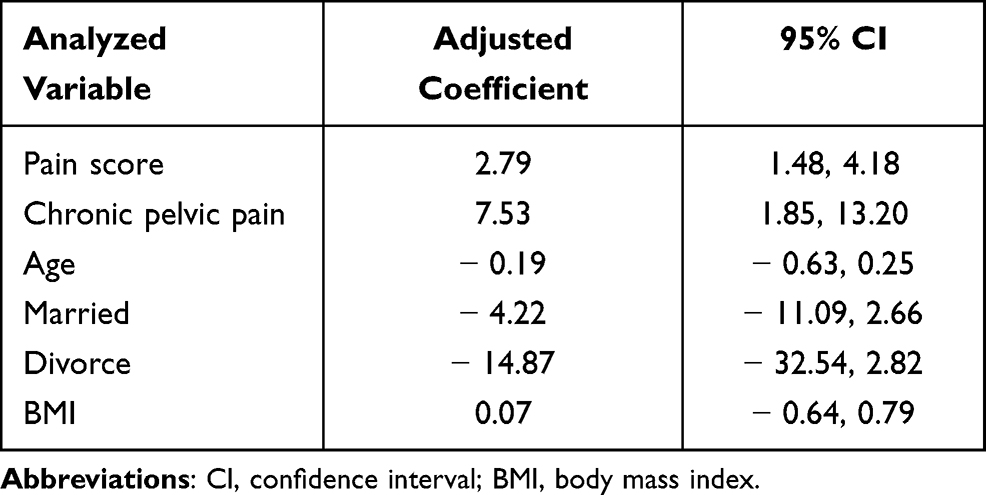 |
Table 3 Multivariable Linear Regression Analysis of the Clinical Factors Correlated with the Weighted Overall EHP-30 Score (n=99) |
In the multivariable analysis of the clinical factors and the modular questionnaire, CPP was positively associated with the QoL score in Section A -Work domain (see Table 4). While in Sections B, C, D, E, and F (Relationship with Children, Sexual Relations domain, Relationship with Physician, Treatment and Infertility, respectively), no variable was significantly correlated with the QoL score.
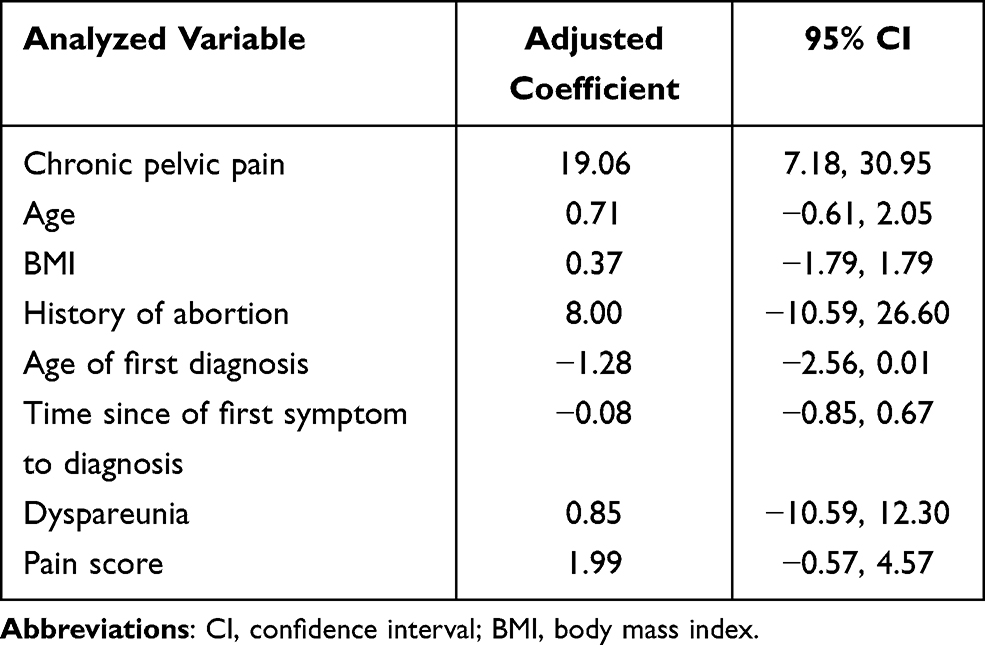 |
Table 4 Median Regression for Analysis of Clinical Factors Correlated with Weighted Scores for Section A: Work (n = 82) |
When considering the work domain, women with CPP had around six times the odds of often/always absent from work or unable to do duties than those without (Odd ratio 6.26, 95% CI 1.84–21.19).
Discussion
Endometriosis is a chronic disease diminishing the QoL and requiring long-term care.10,16 The most cited symptoms of endometriosis reported in our study were dysmenorrhea (97.0%), infertility (54.5%), and CPP (41.4%). In addition, the average pain score was relatively high (8.0±2.1) compared to previous reports.5,17 Thus, evaluation of QoL is crucial for this chronic disease, especially using a disease-specific questionnaire with greater sensitivity to health status changes.10,12
In the present study, the average score for the Central questionnaire was 35.0±15.8, which agrees with a multicenter study conducted among Asian women from 6 countries receiving dienogest for whom the EHP-30 mean score before treatment ranged between 20.0±24.1 and 35.7±25.6 in each dimension.18 However, these scores were relatively lower than the prior Brazilian study in women with ovarian endometriosis using the same questionnaire (mean score 61.6±18.4).16 Moreover, Rindos et al11 found that the pre-operative EHP-30 score for American women, who had undergone a laparoscopic excision of endometriosis, was 52.1 (IQR 39.2,68.3), which is also higher than our study. The differences may represent the geographical variation of QoL, potentially due to differences in culture and beliefs.
When considering each dimension, the Control and Powerlessness dimension in the current study had the highest mean score (45.1±24.4). To compare, a study in the USA also reported that Control and Powerlessness score was the highest dimension at 37.8 (95% CI: 35.5, 40.1).19 The most cited item for this dimension was women with endometriosis who generally felt unwell (77.8%).
We observed that the highest scores from the modular questionnaire were related to the impact on Infertility (34.4, IQR 6.3, 50.0), Work (20.0, IQR10.0, 40.0), and Sexual Relations (10.0, IQR 0.0, 35.0). The highest mean score on Infertility was similar to a report from previous 135 study of Asian women.18 Nevertheless, in a study of Brazilian women found that the Sexual Relations domain had the highest mean score in the Modular questionnaire.16 The difference may be explained by cultural and lifestyle diversity since the QoL assessment mainly depends on an individual perspective. Given that most of the participants in our cohort were partnered and two-thirds were nulliparous, it is understandable that infertility was the most concern that most affected their QoL.
The multivariable analysis revealed that the pain score and CPP were independently correlated with a higher total EHP-30 score, indicating a poorer QoL. These findings are consistent with previous reports that found menstrual pain and chronic non-menstrual pain negatively impacted and limited daily life activities and work performance.20–22 Pain symptoms were repeatedly reported as a harmful factor of life with endometriosis, and several studies report a negative correlation between pain and QoL.23,24 In this study, 81.8% of women with endometriosis reported they had to lie down or go to bed because of the pain, and 73.7% found it difficult to exercise or do leisure activities because of the pain. A negative impact of pain on sport and exercise has also been demonstrated by Fourquet et al.4
CPP, defined as cyclical or noncyclical pain of at least 6 months’ duration, was positively associated with QoL in the work domain. Women with CPP in this study were more likely to be absent from work or unable to do their duties than those without. A multicenter cross-sectional study in Europe reported pelvic pain and disease severity are the major causes of work productivity loss in women with endometriosis.5 A critical narrative review also reported pain symptoms had a negative impact on work productivity, and limited women’s ability to perform work and related activities.22 CPP was reported as the important component of the disease that affected QoL, physical and mental health in women suffering from endometriosis.25–28
To our knowledge, this is the first study in Thailand exploring the QoL and its associated factors using a disease-specific questionnaire in women with endometriosis. We achieved a complete response rate, resulting in a low attrition bias. The study power was sufficient to include all variables in the models, the post hoc power of the study for assessing the associated variables was 0.99. However, the study is not without weaknesses: (a) EHP-30 has no established cut-off value to indicate a low QoL; (b) data regarding the mean EHP-30 score in Thai women were unavailable; and, (c) a larger-scale study is needed to confirm the impact of endometriosis on QoL. (d) although ultrasonography has good discriminatory power in recognizing endometrioma, without the pathological confirmation, the diagnosis may not be completely ascertained.29 Furthermore, we are unable to discriminate the origin of EAPP and infertility whether these symptoms are caused by endometrioma itself or other comorbidities such as superficial and deep infiltrating endometriosis.
Conclusion
By using the disease-specific questionnaire, the present study revealed that endometriosis has an impact on various aspects of women suffering from endometriosis. CPP and the pain score were the factors associated with a worse QoL. While CPP is positively associated with lower QoL in the work domain.
Data Sharing Statement
No further data will be shared.
Details of Ethics Approval
Ethical approvals were obtained from Khon Kaen University Ethics Committee in Human Research based on the Declaration of Helsinki and the ICH Good Clinical Practice Guidelines (HE631144). The study was registered in the Thai Clinical Trials Registry (TCTR20200821001) before enrollment.
Acknowledgments
We would like to acknowledge Mr. Bryan Roderick Hamman for editing the manuscript via Publication Clinic KKU, Thailand.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Dunselman GAJ, Vermeulen N, Becker C, et al. ESHRE guideline: management of women with endometriosis. Hum Reprod. 2014;29(3):400–412. doi:10.1093/humrep/det457
2. Kiesel L, Sourouni M. Diagnosis of endometriosis in the 21st century. Climacteric. 2019;22(3):296–302. doi:10.1080/13697137.2019.1578743
3. Simoens S, Dunselman G, Dirksen C, et al. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Hum Reprod. 2012;27(5):1292–1299. doi:10.1093/humrep/des073
4. Fourquet J, Gao X, Zavala D, et al. Patients’ report on how endometriosis affects health, work, and daily life. Fertil Steril. 2010;93(7):2424–2428. doi:10.1016/j.fertnstert.2009.09.017
5. Nnoaham KE, Hummelshoj L, Webster P, et al. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertil Steril. 2011;96(2):366–373.e8. doi:10.1016/j.fertnstert.2011.05.090
6. Gallagher JS, DiVasta AD, Vitonis AF, Sarda V, Laufer MR, Missmer SA. The Impact of endometriosis on quality of life in adolescents. J Adolesc Health. 2018;63(6):766–772. doi:10.1016/j.jadohealth.2018.06.027
7. Denny E, Mann CH. Endometriosis-associated dyspareunia: the impact on women’s lives. J Fam Plann Reprod Health Care. 2007;33(3):189–193. doi:10.1783/147118907781004831
8. Matasariu R. Psycho-social aspects of quality of life in women with endometriosis. Acta Endocrinol Buchar. 2017;13(3):334–339. doi:10.4183/aeb.2017.334
9. Yamamoto A, Johnstone EB, Bloom MS, Huddleston HG, Fujimoto VY. A higher prevalence of endometriosis among Asian women does not contribute to poorer IVF outcomes. J Assist Reprod Genet. 2017;34(6):765–774. doi:10.1007/s10815-017-0919-1
10. Fourquet J, Báez L, Figueroa M, Iriarte RI, Flores I. Quantification of the impact of endometriosis symptoms on health-related quality of life and work productivity. Fertil Steril. 2011;96(1):107–112. doi:10.1016/j.fertnstert.2011.04.095
11. Rindos NB, Fulcher IR, Donnellan NM. Pain and quality of life after laparoscopic excision of endometriosis. J Minim Invasive Gynecol. 2020;27(7):1610–1617.e1. doi:10.1016/j.jmig.2020.03.013
12. Jia SZ, Leng JH, Shi JH, Sun PR, Lang JH. Health-related quality of life in women with endometriosis: a systematic review. J Ovarian Res. 2012;5(1):29. doi:10.1186/1757-2215-5-29
13. Comptour A, Pereira B, Lambert C, et al. Identification of predictive factors in endometriosis for improvement in patient quality of life. J Minim Invasive Gynecol. 2020;27(3):712–720. doi:10.1016/j.jmig.2019.05.013
14. Van Holsbeke C, Van Calster B, Guerriero S, et al. Endometriomas: their ultrasound characteristics. Ultrasound Obstet Gynecol. 2010;35(6):730–740. doi:10.1002/uog.7668
15. Jones G, Kennedy S, Barnard A, Wong J, Jenkinson C. Development of an endometriosis quality-of-life instrument: the endometriosis health profile-30. Obstet Gynecol. 2001;98(2):258–264. doi:10.1016/s0029-7844(01)01433-8
16. Florentino AVDA, Pereira AMG, Martins JA, Lopes RGC, Arruda RM. Quality of life assessment by the Endometriosis Health Profile (EHP-30) questionnaire prior to treatment for ovarian endometriosis in Brazilian women. Rev Bras Ginecol Obstet. 2019;41(09):548–554. doi:10.1055/s-0039-1693057
17. Warzecha D, Szymusik I, Wielgos M, Pietrzak B. The impact of endometriosis on the quality of life and the incidence of depression—A cohort study. Int J Environ Res Public Health. 2020;17(10):3641. doi:10.3390/ijerph17103641
18. Techatraisak K, Hestiantoro A, Ruey S, et al. Effectiveness of dienogest in improving quality of life in Asian women with endometriosis (ENVISIOeN): interim results from a prospective cohort study under real-life clinical practice. BMC Women's Health. 2019;19(1):68. doi:10.1186/s12905-019-0758-6
19. Soliman AM, Coyne KS, Zaiser E, Castelli-Haley J, Fuldeore MJ. The burden of endometriosis symptoms on health-related quality of life in women in the United States: a cross-sectional study. J Psychosom Obstet Gynecol. 2017;38(4):238–248. doi:10.1080/0167482X.2017.1289512
20. Schindler AE. Dienogest in long-term treatment of endometriosis. Int J Women's Health. 2011;3:175–184. doi:10.2147/IJWH.S5633
21. De Graaff AA, D’Hooghe TM, Dunselman GAJ, et al. The significant effect of endometriosis on physical, mental and social wellbeing: results from an international cross-sectional survey. Hum Reprod. 2013;28(10):2677–2685. doi:10.1093/humrep/det284
22. Culley L, Law C, Hudson N, et al. The social and psychological impact of endometriosis on women’s lives: a critical narrative review. Hum Reprod Update. 2013;19(6):625–639. doi:10.1093/humupd/dmt027
23. Bernuit D, Ebert AD, Halis G, et al. Female perspectives on endometriosis: findings from the uterine bleeding and pain women’s research study. J Endometr. 2011;3(2):73–85. doi:10.5301/JE.2011.8525
24. Tripoli TM, Sato H, Sartori MG, de Araujo FF, Girão MJ, Schor E. Evaluation of quality of life and sexual satisfaction in women suffering from chronic pelvic pain with or without endometriosis. J Sex Med. 2011;8(2):497–503. doi:10.1111/j.1743-6109.2010.01976.x
25. Mathias SD, Kuppermann M, Liberman RF, Lipschutz RC, Steege JF. Chronic pelvic pain: prevalence, health-related quality of life, and economic correlates. Obstet Gynecol. 1996;87(3):321–327. doi:10.1016/0029-7844(95)00458-0
26. Grandi G, Xholli A, Ferrari S, Cannoletta M, Volpe A, Cagnacci A. Intermenstrual pelvic pain, quality of life and mood. Gynecol Obstet Invest. 2013;75(2):97–100. doi:10.1159/000343997
27. Cagnacci A, Della Vecchia E, Xholli A. Chronic pelvic pain improvement: impact on quality of life and mood. Gynecol Endocrinol. 2019;35(6):502–505. doi:10.1080/09513590.2018.1540571
28. Pokrzywinski RM, Soliman AM, Chen J, et al. Achieving clinically meaningful response in endometriosis pain symptoms is associated with improvements in health-related quality of life and work productivity: analysis of 2 Phase III clinical trials. Am J Obstet Gynecol. 2020;222(6):
29. Exacoustos C, Manganaro L, Zupi E. Imaging for the evaluation of endometriosis and adenomyosis. Best Pract Res Clin Obstet Gynaecol. 2014;28(5):655–681. doi:10.1016/j.bpobgyn.2014.04.010
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.