")
Back to Journals » Patient Preference and Adherence » Volume 11
A critical analysis of national policies, systems, and structures of patient empowerment in England and Greece
Authors Boudioni M, McLaren S, Lister G
Received 15 June 2017
Accepted for publication 8 August 2017
Published 27 September 2017 Volume 2017:11 Pages 1657—1669
DOI https://doi.org/10.2147/PPA.S144028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Markella Boudioni,1 Susan McLaren,2 Graham Lister2
1NIHR Imperial Biomedical Research Centre & Patient Experience Research Centre, Imperial College London, 2Institute for Leadership and Service Improvement, Faculty of Health and Social Care, London South Bank University, London, UK
Background: Comparison of patient empowerment (PE) policies in European countries can provide evidence for improvement and reform across different health systems. It may also influence patient and public involvement, patient experience, preference, and adherence.
Objective: The objective of this study was to compare PE within national policies, systems, and structures in England and Greece for achieving integrated people-centered health services.
Methods: We performed a critical search and review of policy and legislation papers in English and Greek languages. This included 1) general health policy and systems papers, 2) PE, patient and/or public involvement or patients’ rights policy and legislation (1990–2015), and 3) comparative or discussion papers for England and/or Greece.
Results: A total of 102 papers on PE policies, systems, and structures were identified initially; 80 papers were included, in which 46 were policy, legislative, and discussion papers about England, 21 were policy, legislation, and discussion papers about Greece, and 13 were comparative or discussion papers including both the countries. In England, National Health Service policies emphasized patient-centered services, involvement, and empowerment, with recent focus on patients’ rights; while in Greece, they emphasized patients’ rights and quality of services, with recent mentions on empowerment. The health ombudsman is a very important organization across countries; however, it may be more powerful in Greece, because of the nonexistence of local mediating bodies. Micro-structures at trusts/hospitals are comparable, but legislation gives more power to the local structures in Greece.
Conclusion: PE policies and systems have been developed and expressed differently in these countries. However, PE similarities, comparable dimensions and mechanisms, were identified. For both the countries, comparative research and these findings could be beneficial in building connections and relationships, contributing to wider European and international developments on PE, involvement, and patients’ rights and further impact on patient preferences and adherence.
Keywords: patient empowerment, patient involvement, patients’ rights, England, Greece, national health policies
Introduction
Heart disease is the leading cause of death in women in the USA, killing 289,758 women in 2013 – that is about 1 in every 4 female deaths, according to National Vital Statistics Report.1 Despite increases in awareness about the high risk of heart disease, in one study, it was shown that only 56% of women recognize that heart disease is their number one killer.2 The absolute numbers of women living with cardiovascular disease and stroke, as well as the number of hospital discharges for heart failure and stroke, exceeded those of men.3 Although women are generally under-tested and undertreated for coronary artery disease (CAD) with increased morbidity and worse prognosis,4–6 it is only recently in 2013, for the first time since 1984, that the mortality from cardiovascular diseases has been shown to be lesser for women than men.7 The onset of ischemic heart disease (IHD) in women is typically about 10 years later than men, with the prevalence increasing rapidly post menopause.8 Stable IHD (SIHD) includes a spectrum of presentations notably:
- Patients who have suspected IHD with stable chest pain or ischemic equivalent symptoms such as dyspnea, exertional arm or jaw pain.
- Patients on chronic medical therapy after revascularization.
- Patients with positive stress tests.9
The symptoms, risk factors, pathophysiology, management and prognosis of SIHD differ significantly between men and women. In this review, we aim to provide a concise overall summary of SIHD in women with emphasis on current practices.
Pathophysiology
It is known that women have smaller coronary arteries per 100 g of left ventricular mass after correcting for body surface area,10 and their arteries have increased stiffness. But beyond these underlying anatomic differences, the pathophysiology of IHD in women is unique and extends beyond just anatomic epicardial coronary artery stenosis. In the Women’s Ischemia Syndrome Evaluation (WISE) study, nearly 60% of women with chest pain who underwent coronary angiography did not have a critical lesion (defined to be >50% luminal stenosis in a coronary artery).11 Shaw et al12 postulate that coronary microvascular and endothelial dysfunction plays a more important role in women as compared with men. Hormonal alterations coupled with pro-atherogenic risk factors result in higher prevalence of coronary microvascular dysfunction in women and are responsible for the observed ischemia paradox; despite having higher prevalence of angina, they tend to have lower prevalence of obstructive CAD and worse prognosis when compared with men.13 Any factor in addition to the underlying atheroma that diminishes the luminal flow further due to abnormal coronary reactivity such as coronary artery vasospasm, endothelial/microvascular dysfunction, autonomic nervous system adrenergic pathways or inflammation12,14,15 can be detrimental to myocardial perfusion. It has been shown that women have more diffuse non-obstructive coronary atherosclerosis and a greater frequency (twice as likely) of coronary plaque erosion and distal embolization compared with men.16–19 In the postpartum female, hormonal, vascular and shear-stress-related factors have been shown to be associated with increased risk for spontaneous coronary artery dissections.20 Hence, when evaluating women with ischemic symptoms and non- obstructive epicardial CAD, alternate mechanisms for ischemia such as endothelial dysfunction and microvascular angina should be considered.
Clinical presentation
Women typically present more commonly with symptoms of angina than men but are less likely to have anatomic obstructive CAD.21–23 Among 10,003 study subjects with stable angina (5,270 women and 4,733 men) with intermediate probability of CAD enrolled in the PROMISE (Prospective Multicenter Imaging Study for evaluation of Chest Pain) trial, chest pain was equally common in men and women; however, women were more likely to characterize their chest pain as “crushing/pressure/squeezing/tightness” as opposed to men who characterized their pain as “aching/dull.”24 In addition, women were more likely to describe pain in the neck and throat than men. Younger women are less likely to report chest pain/discomfort than men, this difference declines with increasing age.25 The VIRGO study was a prospective cohort study of 2,349 (67%) women and 1,152 (33%) men aged ≤55 years hospitalized for acute myocardial infarction (MI; n=3,501) in the USA and Spain, evaluating sex differences in demographics, access to health care, cardiovascular risk and psychosocial factors, clinical presentation, pre-hospital delay and hospital management for acute MI. In this study, women presented with more symptoms, waited more than a week to seek health care than men and were more likely to not think that their symptoms were heart related.26 Because of these features, it was hypothesized that women who present to the emergency department with new-onset angina undergo less rigorous evaluation than men.27 Women usually present with higher clinical risk scores on average, but men present with higher levels of cardiac biomarkers and more classic electrocardiogram (ECG) findings.26 In the PROMISE trial, women were less likely to have a positive stress test even though they had a high burden of cardiovascular risk factors.24 This false sense of a “negative” stress test in symptomatic women with risk factors can lead to underestimating and possibly undertreating women with SIHD.24 Similarly, it has been shown that ECGs are less frequently ordered in women, resulting in misdiagnosis of MI.28 In addition, they are less likely to be admitted to a coronary care unit or to receive inpatient or outpatient cardiology consultations.29
Despite having a higher prevalence of non-obstructive CAD, women even in the absence of critical lesions not only continue to have symptoms while on anti-ischemic therapy but also have 2.5% yearly risk of major adverse cardiac events (MACEs), ie, first occurrence of death (all-cause), nonfatal MI, nonfatal stroke or heart failure hospitalization that is threefold higher than the case-matched asymptomatic reference cohort.23,30
Risk factors and risk stratification
Among participants of the PROMISE trial, women had a higher prevalence of traditional risk factors for CAD such as older age, overweight (BMI >25 kg/m2), hypertension, dyslipidemia, cerebrovascular and peripheral vascular disease, sedentary lifestyle and family history of premature CAD. The prevalence of diabetes mellitus (DM) and metabolic syndrome was similar among both sexes, while smoking was greater in men than women.24 Type II DM imparts a greater risk of IHD in women than men, primarily due to more favorable survival rates of women (than men) without DM.31 Nontraditional risk factors for IHD in women include gestational diabetes, insulin resistance/polycystic ovarian disease, pregnancy-induced hypertension, pre-eclampsia, eclampsia, menopause and autoimmune disease (systemic lupus erythematosus (SLE), rheumatoid arthritis and psoriasis; Table 1).32
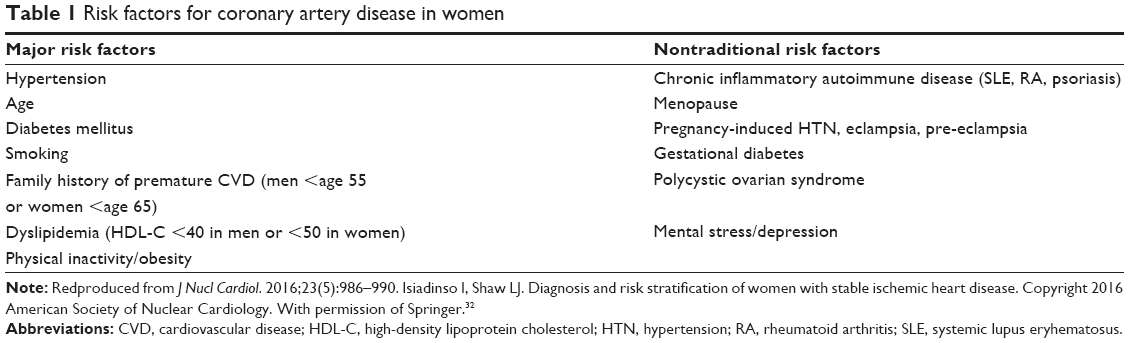 | Table 1 Risk factors for coronary artery disease in women |
Rheumatoid arthritis and SLE are linked to a significant increase in the risk of CAD.33 In the Framingham Offspring study, women with SLE between ages 34 and 44 years were 50 times more likely to have an acute MI than women without SLE.34,35 Currently, with advances in cancer therapy, there are many breast cancer survivors who are also at higher risk for CAD. Women who survive breast cancer are also at higher risk for cardiovascular disease-related mortality compared with women without breast cancer, and this increase in risk is encountered approximately 7 years after diagnosis.36
Mental stress has adverse prognostic implication in cardiovascular disease and is increasingly being recognized as a modifiable nontraditional CVD risk factor particularly in women. In the randomized, double-blind, placebo-controlled, REMIT trial that evaluated the effect of escitalopram on mental stress-induced myocardial ischemia, compared with men, women had a greater rate of myocardial stress-induced myocardial ischemia and collagen-stimulated platelet reactivity to mental stress.37 The data from REMIT suggested that women were at higher cardiovascular risk from mental stress and also highlighted the gap in current risk prediction algorithms that fail to measure an entire facet of risk.
Women with stable angina can be stratified as low, intermediate or high risk based on their age and risk factors. Women without high-risk features at the age of ≥50 years are considered low risk, ≥60 years are considered intermediate risk and those ≥70 years are considered high risk. However, the addition of risk factors such as uncontrolled DM, peripheral arterial disease (PAD), chronic kidney disease, cerebrovascular disease, chronic obstructive lung disease, functional disability or exercise capacity <5 metabolic equivalents (METS) can reclassify patients from low- to intermediate- or intermediate- to high-risk status.38 Many middle-aged women are shown to have low 10-year risk but high lifetime risk for cardiovascular disease.39 Overall, mortality rates increase with increasing number of traditional risk factors from 1.5% for low-risk patients to 9% for high-risk patients with 2 or more risk factors.40
The impact of the risk factors is much more adverse in women and thus places them at a higher CAD risk, as compared with men. For example, the risk of MI is much higher in women who are smokers and diabetic compared with men.41–43 Diabetes also provides greater prognostic information in women than any of the other classic risk factors and is the only risk factor predictive of angiographic coronary lesions in women presenting with chest pain.44 Hypertension is differentially related to IHD according to menopausal status: it is predictive of higher risk in premenopausal women than in postmenopausal women.45 Overall, the evidence for menopause as a risk factor for IHD in women is weak.46 As opposed to men, for whom low-density lipoprotein (LDL) cholesterol is more predictive, low high-density lipoprotein (HDL) cholesterol is a stronger coronary risk factor in women, and levels below 30 mg/dL are strongly associated with increased cardiovascular mortality.47 In women, fasting triglyceride levels greater than 400 mg/dL and the total cholesterol (TC) and HDL cholesterol ratio of ≥3.2 indicate increased risk.48 A family history of premature CAD is also seen more frequently in women than in men with CAD.30 Even mildly reduced renal function is associated with increased CAD risk in women: 5% increase in risk for every 10 mL/min decrease in glomerular filtration rate.49
Screening for CAD in women
The Framingham risk score underestimates risk stratification in women, and classified greater than 90% women as low risk.50 The Reynold risk score was later utilized for risk stratification in women and improved risk re-stratification in women.51 The 2013 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines recommend using pooled cohort equations every 4–6 years as the screening test to estimate 10-year risk for atherosclerotic cardiovascular disease among African-American and White men and women aged 40–79 years.52 Using the risk factors of age, total and HDL cholesterol, systolic BP, DM and current smoking status, 10-year risk is considered low if the estimated risk is calculated to be <7.5% and high if ≥7.5%. Those considered at high risk should undergo vigorous prevention management strategies (lipid management, weight reduction and exercise). If, after quantitative risk assessment, treatment decision still remains ambiguous, family history, hs-CRP, coronary artery calcium (CAC) score or Ankle Brachial Index can be taken into account to help with management.
Selection of diagnostic testing in women
A large array of diagnostic tests is available to the treating clinician to exclude significant CAD in the low-to-intermediate pretest probability patient. Test choice is mainly driven by the patient’s ability to exercise, the interpretability of the electrocardiogram and the additional ancillary data required for a cardiac imaging examination. An algorithm from the AHA consensus statement highlights the basic diagnostic approach to women with stable angina.38
Exercise ECG
For symptomatic women who are at intermediate risk with a normal baseline ECG and can exercise (>5 METS), an exercise ECG stress test should be the initial diagnostic test (class I recommendation).38 Exercise ECG has a lower sensitivity and specificity for the detection of obstructive CAD in women compared with men;53 however, with integration of the Duke Treadmill Score, exercise ECG stress test becomes highly accurate in predicting IHD in women.12,54,55 In a cohort of women, every unit increase in the Duke Treadmill Score is associated with lower mortality by 9% and each increase in MET exercise capacity lowers mortality by 17%.54,55
Role of echo stress and myocardial perfusion imaging (MPI)
Stress echocardiography (with exercise or dobutamine) can be utilized as a diagnostic and prognostic tool among patients with either abnormal ECGs at baseline or those who cannot exercise (class I recommendation). In women, compared with exercise ECG stress testing alone, exercise echocardiography is more sensitive and specific.53,56,57 The overall diagnostic accuracy and prognostic value of stress echocardiography and stress MPI are very similar.58,59 Breast tissue artifacts can decrease the specificity of single-photon emission computerized tomography (SPECT) MPI among women when compared with men (94% for men and 74% for women, P<0.01).60,61 However, use of attenuation correction, prone imaging, evaluation of left ventricular ejection fraction (LVEF) and wall motion can improve diagnostic accuracy in women.38
Stress MPI positron emission tomography (PET) has improved spatial resolution, better image quality and increased diagnostic accuracy for the detection of obstructive CAD in obese women.62 In addition to perfusion imaging, PET gives insight into the absolute coronary blood flow and calculation of myocardial flow reserve (MFR). Diminished MFR (defined as <1.9–2.0) indicates vascular abnormality and microvascular dysfunction particularly in women with non-obstructive CAD.63 In premenopausal young women, the concern for radiation exposure should lead to either stress imaging via echocardiogram or perfusion CMR. High IHD risk women with stable symptoms may also be referred for stress imaging for functional assessment of ischemic burden and to guide post-test, anti-ischemic therapeutic decision-making.
CAC score and coronary computed tomography angiography (CCTA)
CAC score has a sensitivity of 96%–100% and specificity of 40%–66% in detecting obstructive CAD in women.41,42 It provides incremental value to the Framingham risk equation and pooled cohort equation in the evaluation of asymptomatic women who may benefit from aggressive lipid-targeted therapy.50 The diagnostic accuracy of CCTA is similar among men and women, with a sensitivity of 85%–99% and specificity of 64%–90%.64–66 For symptomatic women at intermediate IHD risk who have equivocal or intermediate ECG stress test results, CCTA is a valuable diagnostic modality. In premenopausal young women, CCTA dose reduction to <3 mSv should be considered.
Invasive coronary angiography
According to the 2014 ACC/AHA guidelines,67 coronary angiography is useful for patients with presumed SIHD who have limiting ischemic symptoms despite guideline-directed medical therapy (GDMT) and who are candidates for coronary revascularization. Patients with SIHD with high-risk features on noninvasive testing should be considered for cardiac catheterization to define coronary anatomy.67 This is especially important since the 10-year mortality in women increases with increasing CAD severity.68 However, there are a number of studies demonstrating lower utilization rates of coronary angiography and revascularization in women, thus resulting in lower rates of aggressive evaluation and management leading to poorer outcomes.69,70 Among patients with stable chest pain, white women with 1- to 3-vessel CAD have 1.67- to 2.02-fold higher in-hospital mortality than white men.71
Despite worse symptoms, women referred for coronary angiography for suspected CAD usually have less extensive coronary disease than men, as judged by the number of diseased vessels, suggesting greater degree of microvascular disease in women.72 Hence, tests of vascular dysfunction such as magnetic resonance spectroscopy might be more helpful in women to demonstrate vascular dysfunction and identify those at high risk for poor cardiovascular outcomes.73,74 Nevertheless, the exclusion of significant epicardial CAD with a high level of confidence can be important for high-quality diagnosis and patient management. The diagnosis of IHD in women poses unique challenges to physicians, and further study is needed to identify appropriate diagnostic and therapeutic strategies for women with normal angiograms but persistent chest pain.
Management
Despite strong evidence that the pathophysiology of SIHD differs between the sexes, studies specifically geared toward answering clinical questions about the management of SIHD in women are lacking.67 The same GDMT is recommended for both men and women, with the goal of improving survival and quality of life. Unfortunately, multiple studies have shown that women receive less GDMT than men, in particular, aspirin and beta-blockers. This disparity probably contributes to greater risk associated with IHD in women than men.75,76
Lifestyle changes such as daily exercise, weight loss and dietary restrictions including reduced intake of saturated fats (<7% of total calories), trans-fatty acid (<1% of total calories) and cholesterol (<200 mg/day) are pivotal for decreasing IHD risk. A moderate-to-high dose of a statin therapy should be started in addition to lifestyle modifications, especially among intermediate- and high-risk women.67 Statins in addition to reducing lipids also have a pleiotropic effect. They improve endothelial dysfunction77,78 and have proven benefit in coronary microcirculation.79 Statins and angiotensin-converting enzyme inhibitors (ACEIs) together potentiate these effects. ACEIs have also shown to improve coronary flow reserve (CFR) particularly in women with low CFR.80 Aspirin therapy should be used indefinitely in patients with SIHD but is not recommended for primary prevention of IHD among women aged <65 years.
Beta-blockers should be prescribed as initial therapy for relief of symptoms in patients with SIHD. Long-term beta-blocker therapy reduces ischemic burden and threshold in patients with SIHD and improves survival in patients with left ventricular dysfunction or history of MI.81–83 Other anti-ischemic agents include calcium channel blockers, long-acting nitrates and ranolazine should be prescribed for relief of symptoms when beta-blockers are contraindicated or cause unacceptable side effects. Patients on beta-blockers have been shown to have an average of 0.31 fewer angina episodes per week than patients on calcium channel blockers84 and lower risk of discontinuation due to adverse effects. If there is persistent anginal symptoms despite being on maximum tolerated dosage of beta-blockers, then add-on therapy with other anti-ischemic agents is recommended.67 In a pilot randomized control trial, ranolazine in particular has shown improvement in angina and possibly myocardial ischemia particularly among women with low CFR.85
Hormone replacement therapy has shown benefit in reducing perimenopausal symptoms, emotional well-being and osteoporosis in postmenopausal women; however, it is not recommended for reducing cardiovascular risk or improving clinical outcomes in women.86,87 In fact, a recent meta-analysis including 22 studies involving 43,637 women showed that in relatively healthy postmenopausal women, combined continuous hormone therapy increased the risk of a coronary event, venous thromboembolism and stroke. Estrogen-only therapy increased the risk of venous thromboembolism and stroke but did not increase the risk of coronary events.88 Hormone replacement therapy, selective estrogen receptor modulators, antioxidant vitamins (vitamins C and E, beta carotene) and folic acid do “not” prevent IHD in women and may be harmful. Revascularization with coronary artery bypass graft or percutaneous coronary intervention is recommended if maximum GDMT fails.
Pregnancy and CAD
CAD occurs 3–4 times more often in pregnant women than the age-matched nonpregnant women The incidence of acute coronary syndrome (ACS) in pregnancy is 1 in 10,000 but this increases to 3 per 10,000 deliveries in women 40 years or older.89 Coronary atherosclerosis is the primary etiology of ACS in the antepartum period, and coronary artery dissection is the dominant etiology in the postpartum period. Literature regarding SIHD in pregnancy is limited, but with increasing maternal age more and more pregnant patients with SIHD might be encountered, warranting practitioners to recognize and carefully manage these patients.
Gaps in knowledge and future directions
Women undergo hormonal changes throughout their lifespan starting from menarche to menopause and pregnancy. Many of these biological changes may affect the vulnerability of women for CAD and are incompletely understood currently. Other disease states such as autoimmune disease and vascular dysfunction that alter risk for CAD in women are interconnected with these changes. Future discovery work must be targeted toward unraveling these complex interactions and developing disease-modifying targets.
At the same time, we need to gain deeper insights into factors accounting for disparities in care of women with SIHD and implementation of science research addressing those factors. Finally, improved enrollment of women in large cardiovascular prevention and intervention trials is needed to gain a greater understanding of sex differences in therapeutic effects and perhaps a more nuanced sex-specific approach to managing SIHD in men and women.
Conclusion
Cardiovascular disease is the leading cause of death in women. Pathophysiology of IHD in women includes epicardial coronary artery, endothelial dysfunction, coronary vasospasm, plaque erosion and spontaneous coronary artery dissection. Angina is the most common presentation of SIHD in women. Diagnostic testing can be used effectively to risk stratify women. GDMT should be used effectively for symptom and ischemia management. Despite robust evidence regarding the adverse outcomes seen in women with IHD, there still remains a knowledge gap in sex-specific cardiovascular diagnostics and therapeutics.
Disclosure
The authors report no conflicts of interest in this work.
References
Xu J, Murphy SL, Kochanek KD, Bastian BA. Deaths: final data for 2013. Natl Vital Stat Rep. 2016;64(2):1–119. | ||
Mosca L, Hammond G, Mochari-Greenberger H, Towfighi A, Albert M; American Heart Association Cardiovascular Disease and Stroke in Women and Special Populations Committee of the Council on Clinical Cardiology, Council on Epidemiology and Prevention, Council on Cardiovascular Nursing, Council on High Bloo. Fifteen-year trends in awareness of heart disease in women: results of a 2012 American Heart Association National Survey. Circulation. 2013;127(11):1254–1263. | ||
Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics – 2011 update: a report from the American Heart Association. Circulation. 2011;123(4):e18–e209. | ||
Mosca L, Barrett-Connor E, Wenger NK. Sex/gender differences in cardiovascular disease prevention: what a difference a decade makes. Circulation. 2011;124(19):2145–2154. | ||
Mosca L, Benjamin EJ, Berra K, et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women-2011 update: a guideline from the American Heart Association. Circulation. 2011;123:1243. | ||
Mosca L, Banka CL, Benjamin EJ, et al. Evidence-based guidelines for cardiovascular disease prevention in women: 2007 update. J Am Coll Cardiol. 2007;49(11):1230–1250. | ||
Writing Group Members, Mozaffarian D, Benjamin EJ, et al. Executive summary: heart disease and stroke statistics – 2016 update: a report from the American Heart Association. Circulation. 2016;133(4):447–454. | ||
Vittinghoff E, Shlipak MG, Varosy PD, et al. Risk factors and secondary prevention in women with heart disease: the Heart and Estrogen/progestin Replacement Study. Ann Intern Med. 2003;138(2):81–89. | ||
Dai X, Busby-Whitehead J, Forman DE, Alexander KP. Stable ischemic heart disease in the older adults. J Geriatr Cardiol. 2016;13(2):109. | ||
Kucher N, Lipp E, Schwerzmann M, Zimmerli M, Allemann Y, Seiler C. Gender differences in coronary artery size per 100 g of left ventricular mass in a population without cardiac disease. Swiss Med Wkly. 2001;131(41/42):610–615. | ||
Merz CNB, Kelsey SF, Pepine CJ, et al. The Women’s Ischemia Syndrome Evaluation (WISE) study: protocol design, methodology and feasibility report. J Am Coll Cardiol. 1999;33(6):1453–1461. | ||
Shaw LJ, Bugiardini R, Merz CNB. Women and ischemic heart disease: evolving knowledge. J Am Coll Cardiol. 2009;54(17):1561–1575. | ||
Merz CNB. Women and ischemic heart disease. JACC Cardiovasc Imaging. 2011;4(1). | ||
von Mering GO, Arant CB, Wessel TR, et al. Abnormal coronary vasomotion as a prognostic indicator of cardiovascular events in women: results from the National Heart, Lung, and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation (WISE). Circulation. 2004;109(6):722–725. | ||
Wong TY, Klein R, Sharrett AR, et al. Retinal arteriolar narrowing and risk of coronary heart disease in men and women: the Atherosclerosis Risk in Communities Study. JAMA. 2002;287(9):1153–1159. | ||
Burke AP, Kolodgie FD, Farb A, Weber D, Virmani R. Morphological predictors of arterial remodeling in coronary atherosclerosis. Circulation. 2002;105(3):297–303. | ||
Burke A, Kolodgie F, Farb A, Virmani R. Gender differences in coronary plaque morphology in sudden coronary death. Circulation. 2003;108(17):165–165. | ||
Burke AP, Farb A, Malcom G, Virmani R. Effect of menopause on plaque morphologic characteristics in coronary atherosclerosis. Am Heart J. 2001;141(2):S58–S62. | ||
Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque. J Am Coll Cardiol. 2006;47(8s1):C13–C18. | ||
Tweet MS, Hayes SN, Pitta SR, et al. Clinical features, management, and prognosis of spontaneous coronary artery dissection. Circulation. 2012;126(5):579–588. | ||
Kennedy JW, Killip T, Fisher LD, Alderman EL, Gillespie MJ, Mock MB. The clinical spectrum of coronary artery disease and its surgical and medical management, 1974–1979. The Coronary Artery Surgery study. Circulation. 1982;66(5 pt 2):III16–III23. | ||
Diamond GA, Staniloff HM, Forrester JS, Pollock BH, Swan H. Computer-assisted diagnosis in the noninvasive evaluation of patients with suspected coronary artery disease. J Am Coll Cardiol. 1983;1(2):444–455. | ||
Douglas PS, Hoffmann U, Patel MR, et al. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med. 2015;372(14):1291–1300. | ||
Hemal K, Pagidipati NJ, Coles A, et al. Sex differences in demographics, risk factors, presentation, and noninvasive testing in stable outpatients with suspected coronary artery disease: insights from the PROMISE Trial. JACC Cardiovasc Imaging. 2016;9(4):337–346. | ||
Canto JG, Rogers WJ, Goldberg RJ, et al. Association of age and sex with myocardial infarction symptom presentation and in-hospital mortality. JAMA. 2012;307(8):813–822. | ||
Bucholz EM, Strait KM, Dreyer RP, et al. Sex differences in young patients with acute myocardial infarction: a VIRGO study analysis. Eur Heart J Acute Cardiovasc Care. Epub 2016 Aug 2. | ||
Bellasi A, Raggi P, Merz CB, Shaw LJ. New insights into ischemic heart disease in women. Cleve Clin J Med. 2007;74(8):585. | ||
Arnold AL, Milner KA, Vaccarino V. Sex and race differences in electrocardiogram use (the National Hospital Ambulatory Medical Care Survey). Am J Cardiol. 2001;88(9):1037–1040. | ||
Roger VL, Farkouh ME, Weston SA, et al. Sex differences in evaluation and outcome of unstable angina. JAMA. 2000;283(5):646–652. | ||
Gulati M, Cooper-DeHoff RM, McClure C, et al. Adverse cardiovascular outcomes in women with nonobstructive coronary artery disease: a report from the Women’s Ischemia Syndrome Evaluation Study and the St James Women Take Heart Project. Arch Intern Med. 2009;169(9):843–850. | ||
Barrett-Connor EL, Cohn BA, Wingard DL, Edelstein SL. Why is diabetes mellitus a stronger risk factor for fatal ischemic heart disease in women than in men? The Rancho Bernardo Study. JAMA. 1991;265(5):627–631. | ||
Isiadinso I, Shaw LJ. Diagnosis and risk stratification of women with stable ischemic heart disease. J Nucl Cardiol. 2016;23(5):986–990. | ||
Salmon JE, Roman MJ. Subclinical atherosclerosis in rheumatoid arthritis and systemic lupus erythematosus. Am J Med. 2008;121(10):S3–S8. | ||
Manzi S, Meilahn EN, Rairie JE, et al. Age-specific incidence rates of myocardial infarction and angina in women with systemic lupus erythematosus: comparison with the Framingham Study. Am J Epidemiol. 1997;145(5):408–415. | ||
Sharma K, Gulati M. Coronary artery disease in women: a 2013 update. Glob Heart. 2013;8(2):105–112. | ||
Bradshaw PT, Stevens J, Khankari N, Teitelbaum SL, Neugut AI, Gammon MD. Cardiovascular disease mortality among breast cancer survivors. Epidemiology. 2016;27(1):6–13. | ||
Samad Z, Boyle S, Ersboll M, et al. Sex differences in platelet reactivity and cardiovascular and psychological response to mental stress in patients with stable ischemic heart disease: insights from the REMIT study. J Am Coll Cardiol. 2014;64(16):1669–1678. | ||
Mieres JH, Gulati M, Bairey Merz N, et al. Role of noninvasive testing in the clinical evaluation of women with suspected ischemic heart disease: a consensus statement from the American Heart Association. Circulation. 2014;130(4):350–379. | ||
Marma AK, Berry JD, Ning H, Persell SD, Lloyd-Jones DM. Distribution of 10-year and lifetime predicted risks for cardiovascular disease in US adults: findings from the National Health and Nutrition Examination Survey 2003 to 2006. Circ Cardiovasc Qual Outcomes. 2010;3(1):8–14. | ||
Daviglus ML, Stamler J, Pirzada A, et al. Favorable cardiovascular risk profile in young women and long-term risk of cardiovascular and all-cause mortality. JAMA. 2004;292(13):1588–1592. | ||
Willett WC, Green A, Stampfer MJ, et al. Relative and absolute excess risks of coronary heart disease among women who smoke cigarettes. N Engl J Med. 1987;317(21):1303–1309. | ||
Hu FB, Stampfer MJ, Solomon CG, et al. The impact of diabetes mellitus on mortality from all causes and coronary heart disease in women: 20 years of follow-up. Arch Intern Med. 2001;161(14):1717–1723. | ||
Barrett-Connor E, Wingard DL. Sex differential in ischemic heart disease mortality in diabetics: a prospective population-based study. Am J Epidemiol. 1983;118(4):489–496. | ||
Juutilainen A, Kortelainen S, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Gender difference in the impact of type 2 diabetes on coronary heart disease risk. Diabetes Care. 2004;27(12):2898–2904. | ||
Gierach GL, Johnson BD, Merz CNB, et al. Hypertension, menopause, and coronary artery disease risk in the Women’s Ischemia Syndrome Evaluation (WISE) study. J Am Coll Cardiol. 2006;47(3s1):S50–S58. | ||
Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA. 2007;297(13):1465–1477. | ||
Bass KM, Newschaffer CJ, Klag MJ, Bush TL. Plasma lipoprotein levels as predictors of cardiovascular death in women. Arch Intern Med. 1993;153(19):2209–2216. | ||
ASSESSMENT R. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302(18):1993–2000. | ||
Reis SE, Olson MB, Fried L, et al. Mild renal insufficiency is associated with angiographic coronary artery disease in women. Circulation. 2002;105(24):2826–2829. | ||
Michos ED, Nasir K, Braunstein JB, et al. Framingham risk equation underestimates subclinical atherosclerosis risk in asymptomatic women. Atherosclerosis. 2006;184(1):201–206. | ||
Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: the Reynolds Risk Score. JAMA. 2007;297(6):611–619. | ||
Goff DC, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2935–2959. | ||
Kwok Y, Kim C, Grady D, Segal M, Redberg R. Meta-analysis of exercise testing to detect coronary artery disease in women. Am J Cardiol. 1999;83(5):660–666. | ||
Alexander KP, Shaw LJ, DeLong ER, Mark DB, Peterson ED. Value of exercise treadmill testing in women. J Am Coll Cardiol. 1998;32(6):1657–1664. | ||
Gulati M, Arnsdorf MF, Shaw LJ, et al. Prognostic value of the duke treadmill score in asymptomatic women. Am J Cardiol. 2005;96(3):369–375. | ||
Cheitlin MD, Armstrong WF, Aurigemma GP, et al. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography). J Am Coll Cardiol. 2003;42(5):954–970. | ||
Marwick TH, Anderson T, Williams MJ, et al. Exercise echocardiography is an accurate and cost-efficient technique for detection of coronary artery disease in women. J Am Coll Cardiol. 1995;26(2):335–341. | ||
Fleischmann KE, Hunink MG, Kuntz KM, Douglas PS. Exercise echocardiography or exercise SPECT imaging? A meta-analysis of diagnostic test performance. JAMA. 1998;280(10):913–920. | ||
Schinkel AF, Bax JJ, Geleijnse ML, et al. Noninvasive evaluation of ischaemic heart disease: myocardial perfusion imaging or stress echocardiography? Eur Heart J. 2003;24(9):789–800. | ||
Bokhari S, Shahzad A, Bergmann SR. Superiority of exercise myocardial perfusion imaging compared with the exercise ECG in the diagnosis of coronary artery disease. Coron Artery Dis. 2008;19(6):399–404. | ||
Shaw LJ, Vasey C, Sawada S, Rimmerman C, Marwick TH. Impact of gender on risk stratification by exercise and dobutamine stress echocardiography: long-term mortality in 4234 women and 6898 men. Eur Heart J. 2005;26(5):447–456. | ||
Bateman TM, Heller GV, McGhie AI, et al. Diagnostic accuracy of rest/stress ECG-gated Rb-82 myocardial perfusion PET: comparison with ECG-gated Tc-99m sestamibi SPECT. J Nucl Cardiol. 2006;13(1):24–33. | ||
Shaw LJ, Hage FG, Berman DS, Hachamovitch R, Iskandrian A. Prognosis in the era of comparative effectiveness research: where is nuclear cardiology now and where should it be? J Nucl Cardiol. 2012;19(5):1026–1043. | ||
Meijboom WB, Meijs MF, Schuijf JD, et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol. 2008;52(25):2135–2144. | ||
Miller JM, Rochitte CE, Dewey M, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008;359(22):2324–2336. | ||
Meijboom WB, Weustink AC, Pugliese F, et al. Comparison of diagnostic accuracy of 64-slice computed tomography coronary angiography in women versus men with angina pectoris. Am J Cardiol. 2007;100(10):1532–1537. | ||
Fihn SD, Blankenship JC, Alexander KP, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64(18):1929–1949. | ||
Sharaf B, Wood T, Shaw L, et al. Adverse outcomes among women presenting with signs and symptoms of ischemia and no obstructive coronary artery disease: Findings from the National Heart, Lung, and Blood Institute–sponsored Women’s Ischemia Syndrome Evaluation (WISE) angiographic core laboratory. Am Heart J. 2013;166(1):134–141. | ||
Maynard C, Litwin PE, Martin JS, Weaver WD. Gender differences in the treatment and outcome of acute myocardial infarction: results from the Myocardial Infarction Triage and Intervention Registry. Arch Intern Med. 1992;152(5):972–976. | ||
Daly C, Clemens F, Lopez Sendon JL, et al. Gender differences in the management and clinical outcome of stable angina. Circulation. 2006;113(4):490–498. | ||
Shaw LJ, Shaw RE, Merz CN, et al. Impact of ethnicity and gender differences on angiographic coronary artery disease prevalence and in-hospital mortality in the American College of Cardiology-National Cardiovascular Data Registry. Circulation. 2008;117(14):1787–1801. | ||
Bell MR, Berger PB, Holmes DR, Mullany CJ, Bailey KR, Gersh BJ. Referral for coronary artery revascularization procedures after diagnostic coronary angiography: evidence for gender bias? J Am Coll Cardiol. 1995;25(7):1650–1655. | ||
Bugiardini R, Merz CNB. Angina with “normal” coronary arteries: a changing philosophy. JAMA. 2005;293(4):477–484. | ||
Johnson BD, Shaw LJ, Buchthal SD, et al. Prognosis in women with myocardial ischemia in the absence of obstructive coronary disease: results from the National Institutes of Health-National Heart, Lung, and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation (WISE). Circulation. 2004;109(24):2993–2999. | ||
Frishman WH, Heiman M, Soberman J, Greenberg S, Eff J. Celiprolol International Angina Study Group. Comparison of celiprolol and propranolol in stable angina pectoris. Am J Cardiol. 1991;67(8): 665–670. | ||
Narahara KA, Group TBI. Double-blind comparison of once daily betaxolol versus propranolol four times daily in stable angina pectoris. Am J Cardiol. 1990;65(9):577–582. | ||
Pizzi C, Manfrini O, Fontana F, Bugiardini R. Angiotensin-converting enzyme inhibitors and 3-hydroxy-3-methylglutaryl coenzyme A reductase in cardiac Syndrome X: role of superoxide dismutase activity. Circulation. 2004;109(1):53–58. | ||
Kayikcioglu M, Payzin S, Yavuzgil O, Kultursay H, Can LH, Soydan I. Benefits of statin treatment in cardiac syndrome-X1. Eur Heart J. 2003;24(22):1999–2005. | ||
Chen J, Hsu N, Wu T, Lin S, Chang M. Long-term angiotensin-converting enzyme inhibition reduces plasma asymmetric dimethylarginine and improves endothelial nitric oxide bioavailability and coronary microvascular function in patients with syndrome X. Am J Cardiol. 2002;90(9):974–982. | ||
Pauly DF, Johnson BD, Anderson RD, et al. In women with symptoms of cardiac ischemia, nonobstructive coronary arteries, and microvascular dysfunction, angiotensin-converting enzyme inhibition is associated with improved microvascular function: a double-blind randomized study from the National Heart, Lung and Blood Institute Women’s Ischemia Syndrome Evaluation (WISE). Am Heart J. 2011;162(4):678–684. | ||
Gan SC, Beaver SK, Houck PM, MacLehose RF, Lawson HW, Chan L. Treatment of acute myocardial infarction and 30-day mortality among women and men. N Engl J Med. 2000;343(1):8–15. | ||
Blomkalns AL, Chen AY, Hochman JS, et al. Gender disparities in the diagnosis and treatment of non–ST-segment elevation acute coronary syndromes: large-scale observations from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the American College of Cardiology/American Heart Association Guidelines) national quality improvement initiative. J Am Coll Cardiol. 2005;45(6):832–837. | ||
Kernis SJ, Harjai KJ, Stone GW, et al. Does beta-blocker therapy improve clinical outcomes of acute myocardial infarction after successful primary angioplasty? J Am Coll Cardiol. 2004;43(10):1773–1779. | ||
Heidenreich PA, McDonald KM, Hastie T, et al. Meta-analysis of trials comparing β-blockers, calcium antagonists, and nitrates for stable angina. JAMA. 1999;281(20):1927–1936. | ||
Mehta PK, Goykhman P, Thomson LE, et al. Ranolazine improves angina in women with evidence of myocardial ischemia but no obstructive coronary artery disease. J Cardiovasc Imaging. 2011;4(5):514–522. | ||
Smith SC, Benjamin EJ, Bonow RO, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation endorsed by the World Heart Federation and the Preventive Cardiovascular Nurses Association. J Am Coll Cardiol. 2011;58(23):2432–2446. | ||
Patel MR, Spertus JA, Brindis RG, et al. ACCF proposed method for evaluating the appropriateness of cardiovascular imaging. J Am Coll Cardiol. 2005;46(8):1606–1613. | ||
Marjoribanks J, Farquhar C, Roberts H, Lethaby A, Lee J. Long-term hormone therapy for perimenopausal and postmenopausal women. Cochrane Database Syst Rev. 2017;1:CD004143. | ||
James AH, Jamison MG, Biswas MS, Brancazio LR, Swamy GK, Myers ER. Acute myocardial infarction in pregnancy: a United States population-based study. Circulation. 2006;113(12):1564–1571. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.