")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
A Correlational Study on Cardiopulmonary Endurance in Male Patients with New-Onset Type 2 Diabetes
Authors Liu BB, Niu ZR, Jia XJ, Liu XL, Lu Q
Received 6 December 2021
Accepted for publication 1 April 2022
Published 2 May 2022 Volume 2022:15 Pages 1365—1373
DOI https://doi.org/10.2147/DMSO.S352798
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ming-Hui Zou
Bin-Bin Liu,1,* Zi-Ru Niu,2,* Xiao-Jiao Jia,3 Xiao-Li Liu,3 Qiang Lu3
1Department of Functional Inspection, Qinhuangdao First Hospital, Qinhuangdao, 066000, People’s Republic of China; 2Department of Endocrinology and Metabolic Diseases, Hebei Medical University, Shijiazhuang, 050000, People’s Republic of China; 3Department of Endocrinology, Qinhuangdao First Hospital, Qinhuangdao, 066000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiang Lu, Department of Endocrinology, Qinhuangdao First Hospita l, No. 258 of Wenhua Road, Haigang District, Qinhuangdao, 066000, People’s Republic of China, Tel +86-0335-5908385, Fax: +86-0335-3032042, Email [email protected]
Background: Cardiopulmonary exercise tests (CPETs) are widely used non-invasive and reliable functional evaluation methods. This study investigated the correlation between cardiopulmonary endurance indices and plasma glucose levels and abdominal visceral fat in males with new-onset type 2 diabetes.
Methods: A total of 136 male individuals, who had been treated in the First Hospital of Qinhuangdao City, were selected to form a new-onset type 2 diabetes group (66 cases) and a control group (70 cases); individuals were divided into three groups (Q1, Q2, and Q3) from low to high according to their anaerobic threshold (AT) oxygen uptake (VO2), AT VO2/kg (VO2 per kg of body weight), peak VO2, peak VO2/kg, AT heart rate (HR), peak HR, and HR recovery after 1 minute. A cardiopulmonary exercise test was used to determine the VO2 of each group of subjects for VO2 max and AT VO2/kg, HR, and HR recovery after 1 minute. The differences in fat areas and plasma glucose levels were compared under different cardiorespiratory endurance indicators.
Results: Compared with the control group, the abdominal visceral fat (AVF) area, fasting plasma glucose (FPG), and postprandial plasma glucose (PPG) levels increased in the new-onset type 2 diabetes group. Concurrently, AT VO2, AT VO2/kg, peak VO2, peak VO2/kg, AT HR, peak HR, and 1-minute HR recovery all decreased, and the difference between the groups was statistically significant (P< 0.05). The higher the AT VO2 and peak VO2 values, the lower the PPG level (P< 0.05) and the smaller the area of abdominal visceral fat (P< 0.05). The AT VO2/kg and peak VO2/kg values were negatively correlated with the abdominal visceral fat area, while other indicators had no obvious relationship with either plasma glucose levels or the area of fat.
Conclusion: The levels of blood glucose and visceral fat are correlated with cardiopulmonary function. With the increase in blood glucose levels and visceral fat, the indices of cardiopulmonary function gradually decrease. The correlation between different cardiopulmonary function indices and blood glucose levels and visceral fat was different.
Keywords: cardiopulmonary function, type 2 diabetes, abdominal visceral fat, plasma glucose
Introduction
In recent years, there has been an increase in the incidence and prevalence of type 2 diabetes, which can cause chronic diseases of multiple tissues and organs. Studies have found that visceral obesity is related to the occurrence and development of type 2 diabetes.1 Previous research data has revealed that increased hepatic gluconeogenesis in patients with obesity can cause excessive triglyceride (TG) production and can lead to the deposition of fat in internal organs (eg, the liver or pancreas), which can trigger an inflammatory cascade and eventually damage the endocrine function.2 According to related studies, there is a correlation between the plasma glucose fluctuation index (as measured by continuous plasma glucose monitoring) and vascular endothelial function.3 Diabetes can also directly damage the structure and affect the function of the myocardium and lungs. Long-term hyperglycemia may lead to myocardial hypertrophy and fibrosis, ventricular stiffness, and myocardial dysfunction. Diabetes is also an independent risk factor for lung volume and lung dispersion.4,5
The occurrence and development of type 2 diabetes are closely related to factors such as plasma glucose levels and obesity, and the accurate monitoring of plasma glucose levels can effectively prevent, diagnose, and treat type 2 diabetes. Excessive fat deposition may increase the risk of type 2 diabetes, atherosclerosis, and cardiovascular disease, and the risk of visceral obesity is much higher than that of subcutaneous obesity. Visceral adipose tissue accurately measured by computed tomography or magnetic resonance imaging is an independent risk marker for the morbidity and mortality of cardiovascular and metabolic diseases.6,7 Cardiopulmonary exercise tests (CPETs) are widely used non-invasive and reliable functional evaluation methods. CPETs can comprehensively evaluate the cardiovascular, respiratory, muscular, and metabolic systems during exercise and are considered the gold standard for evaluating cardiopulmonary function.8 Clinically, CPETs can be used in the diagnosis, evaluation, treatment, and prognosis of diseases, along with other aspects. The purpose of this study is to use CPETs to determine related indicators and to explore the correlation between cardiopulmonary endurance and plasma glucose levels and abdominal visceral fat in males with new-onset type 2 diabetes, providing an understanding of the enhanced detection of indicators and reference content for the purpose of early type 2 diabetes prevention and diabetic complication reduction. This study confirms that encouraging reasonable exercise, increasing cardiorespiratory endurance, developing a healthy lifestyle, and maintaining a healthy weight have a positive effect on preventing the occurrence of diabetes and improving the quality-of-life of patients with the disease.
Subjects and Methods
Subjects
A total of 66 male subjects diagnosed with new-onset type 2 diabetes in the First Hospital of Qinhuangdao City and 70 subjects with normal plasma glucose levels were selected to undergo voluntary CPETs. This study was approved by the ethics committee of the First Hospital of Qinhuangdao City, and all subjects signed an informed consent form.
Selection Criteria
The selection criteria were as follows: 1) no uncontrolled diabetes or hypertension, 2) no typical unstable angina within the previous month, 3) no serious arrhythmia, 4) no chronic heart failure, 5) no acute myocardial infarction within the previous 3 months, 6) no physical disorder, 7) no serious liver, kidney, lung, or chest disease, 8) no lower extremity arteriosclerosis obliterans, and 9) no participation in any professional medical rehabilitation or sports training during the previous 6 months.
Method
General Information
Height, weight, systolic and diastolic plasma pressure, and waist circumference were measured using conventional methods. The formula used for calculating body mass index (BMI) was BMI=weight (kg)/height (m2). All subjects underwent abdominal scanning with a Ge (Signa Excite 1.5T HD echo speed) MRI under fasting conditions to determine visceral fat. After fasting for 8 hours, the subjects were given 75 g of anhydrous glucose dissolved in 250–300 mL of water to drink within 5–10 minutes on an empty stomach. Venous blood was collected on an empty stomach and 2 hours after taking the sugar mixture. Fasting plasma glucose (FPG) and 2-hour postprandial plasma glucose (PPG) levels were measured. Fasting venous blood samples were reserved for testing TG, cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, etc.
Grouping Method
According to the presence or absence of new-onset type 2 diabetes, individuals were assigned to the control group (70) or the new-onset type 2 diabetes group (66). General data and cardiopulmonary function indices were compared; individuals were divided into three groups according to the third quantile from low to high (Q1, Q2, and Q3) depending on the anaerobic threshold (AT) oxygen uptake (VO2), AT VO2/kg, peak VO2, peak VO2/kg, AT heart rate (HR), peak HR, and 1-minute HR recovery. The differences in fat areas and plasma glucose levels under different cardiopulmonary endurance indicators were compared.
Cardiopulmonary Function Index Measurement
The CPETs were conducted by professionals, and the system was calibrated before testing using a cardiopulmonary exercise tester. According to the maximum power expected by the tester, the scheme corresponding to the tester was selected, and the gas metabolism indices, such as oxygen uptake during continuous exercise, were observed. Concurrently, the changes in heart rate were monitored. The VO2 max was determined when the incremental exercise load increased and exercise continued with no increase in oxygen intake for more than 30 seconds, ie, the VO2 plateau appeared. The AT was defined as the VO2 when aerobic metabolism during exercise did not require anaerobic metabolism to supplement energy, ie, the highest VO2 before the occurrence of lactic acidosis. The V-slope method was used to determine the AT, ie, the inflection point of the slope of the carbon dioxide emission curve compared with the VO2 curve was the reference point for the position of the AT value. For the subjects in each group, the VO2, VO2/kg (VO2 per kg of body weight), HR, and HR after 1 minute of recovery were obtained at VO2 max and AT, respectively. The test was stopped when the exercise took more than 6 minutes to reach the VO2 platform and was maintained for more than 30 seconds while meeting other target requirements, such as the AT.
Statistical Analysis
A statistical analysis was performed using the SPSS 13.0 software. The measurement data were expressed as  ±s, an independent sample t-test was used for the comparisons between the groups and an analysis of variance test was used for comparisons between the three groups. A single-factor analysis and a correlation analysis were used to evaluate the correlation between two indicators. A P-value of <0.05 was considered statistically significant.
±s, an independent sample t-test was used for the comparisons between the groups and an analysis of variance test was used for comparisons between the three groups. A single-factor analysis and a correlation analysis were used to evaluate the correlation between two indicators. A P-value of <0.05 was considered statistically significant.
Results
Table 1 shows the general demographic characteristics of each group, along with the comparison results for abdominal visceral fat, plasma glucose levels, and CPET indicators. The results reveal that, compared with the normal plasma glucose group, the abdominal area, FPG, and PPG levels increased in males with new-onset type 2 diabetes. Concurrently, the AT VO2, AT VO2/kg, peak VO2, peak VO2/kg, AT HR, peak HR, and HR within 1 minute of recovery decreased in the indicators for cardiopulmonary function. The difference was statistically significant (P<0.05).
 |
Table 1 Comparison of General Information, Abdominal Visceral Fat, Plasma Glucose, CPET, and Other Indicators |
Fat Area and Plasma Glucose Levels Under Different Cardiorespiratory Endurance Indicators
A comparison of the plasma glucose and abdominal visceral fat levels in the AT VO2 tertile grouping was conducted. As shown in Figure 1, the comparison between different AT VO2 levels reveals that the higher the AT VO2 value, the lower the PPG level (P<0.05), while the comparison between the groups shows no statistical difference between abdominal visceral fat and FPG levels (P>0.05).
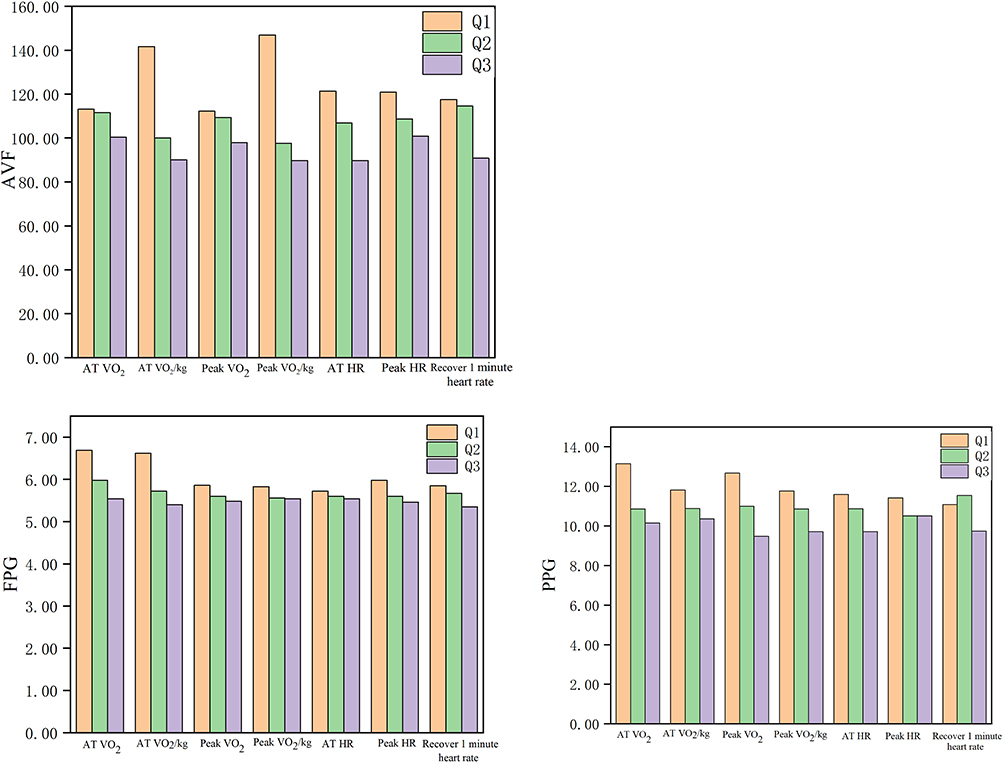 |
Figure 1 Comparison of AVF, FPG, and PPG levels among three quantile groups of cardiopulmonary function indexes. Abbreviations: AT, anaerobic threshold; VO2, oxygen uptake; VO2/kg, VO2 per kg of body weight; HR, AT heart rate; AVF, abdominal visceral fat; FPG, fasting plasma glucose; PPG, postprandial plasma glucose. |
A comparison of the plasma glucose and abdominal visceral fat levels of each group in the AT VO2/kg tertile group was conducted. As shown in Figure 1, the comparison between different AT VO2/kg levels shows that the higher the AT VO2/kg value, the smaller the area of abdominal visceral fat (P<0.05). There was no significant difference in FPG and PPG levels between the groups (P>0.05).
A comparison of the plasma glucose and abdominal visceral fat levels of each group in the peak VO2 tertile group was conducted. As shown in Figure 1, the comparison of different peak VO2 levels shows that the higher the peak VO2 value, the lower the PPG level (P<0.05). There was no significant difference in abdominal visceral fat or FPG levels between the groups (P>0.05).
A comparison of the plasma glucose and abdominal visceral fat levels of each group in the peak VO2/kg tertile grouping was conducted. As shown in Figure 1, the comparison of different peak VO2/kg levels reveals that the higher the peak VO2/kg value, the smaller the abdominal visceral fat area (P<0.05). There was no significant difference in FPG or PPG levels (P>0.05).
A comparison of plasma glucose and abdominal visceral fat levels among the three quantile groups of AT HR was conducted. As shown in Figure 1, with an increase in AT HR, the abdominal visceral fat, FPG, and PPG levels revealed a downward trend, although the differences were not statistically significant (P>0.05).
A comparison of the plasma glucose and abdominal visceral fat levels of the peak HR tertile groups was conducted. As shown in Figure 1, with an increase in peak HR, the abdominal visceral fat, FPG, and PPG levels revealed a downward trend, although the differences were not statistically significant (P>0.05). Figure 1 shows that, with an increase in the 1-minute HR recovery, the abdominal visceral fat, FPG, and PPG levels followed a downward trend, but the differences were not statistically significant (P>0.05).
Finally, a single-factor correlation analysis of plasma glucose levels, abdominal visceral fat, and cardiopulmonary function indices was conducted. As shown in Table 2, among the main indicators of cardiopulmonary function in males with new-onset type 2 diabetes, the AT VO2/kg and peak VO2/kg values are negatively correlated with the area of abdominal visceral fat, while the remaining indicators are related to the area of fat and FPG levels. There was no obvious relationship between the PPG level.
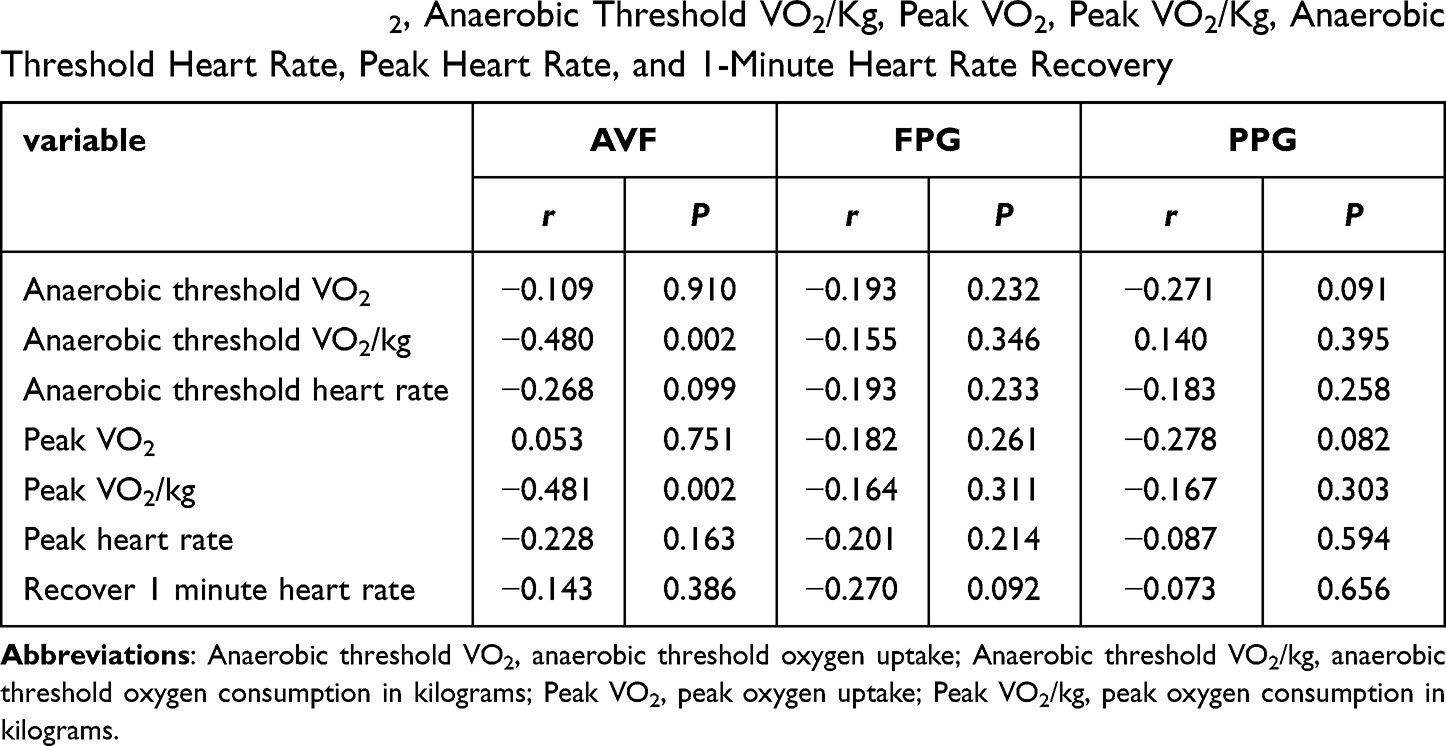 |
Table 2 Single-Factor Correlation Analysis of Plasma Glucose and Abdominal Visceral Fat with Anaerobic Threshold VO2, Anaerobic Threshold VO2/Kg, Peak VO2, Peak VO2/Kg, Anaerobic Threshold Heart Rate, Peak Heart Rate, and 1-Minute Heart Rate Recovery |
Discussion
Type 2 diabetes is the most common chronic metabolic disease worldwide. When the pancreatic β-cell function is defective, insulin secretion is insufficient or insulin resistance occurs, and the body cannot maintain glucose homeostasis, which results in hyperglycemia.9 The main characteristics of patients with type 2 diabetes are obesity or a higher percentage of body fat, higher insulin resistance in patients with obesity,10 and a correlation between epicardial fat deposition and insulin resistance.7 Studies have shown that the amount of abdominal visceral fat is related to the occurrence and development of type 2 diabetes and cardiovascular disease. Furthermore, visceral obesity has a long-term effect on the structure of the heart, leading to high plasma pressure, diabetic cardiomyopathy, etc.11 Han et al12 compared the Chinese visceral adiposity index (CVAI) with the waist-to-height ratio, waist circumference, and body mass index to explore the relationship between CVAI and type 2 diabetes. The results confirmed that the CVAI was more accurate in predicting type 2 diabetes, so this index may be a reliable and applicable indicator for identifying people at high risk of the disease. Tanaka et al13 conducted a study on 80 male patients with type 2 diabetes and found that abdominal visceral fat and plasma sphingosine 1-phosphate levels were significantly positively correlated. The current study revealed that, compared with the normal plasma glucose group, the abdominal visceral fat area, FPG, and PPG levels increased in males with new-onset type 2 diabetes, and the difference between the groups was statistically significant (P<0.05).
Wang Yining et al’s14 study reported that the difference in peak VO2 between the diabetes group and the control group was both statistically significant and correlated. Reasonable exercise improved the plasma glucose levels of patients with diabetes and enhanced their cardiopulmonary function. The current study found that the indicators of cardiorespiratory endurance for patients with type 2 diabetes were related to both abdominal visceral fat and plasma glucose levels. Moreover, compared with the normal plasma glucose group, the patients with type 2 diabetes had reduced cardiorespiratory function and endurance.15 Type 2 diabetes can cause a loss of cardiopulmonary function adaptability and exercise endurance and can aggravate plasma pressure responses during exercise.16 Peak VO2 is the most scientific and accurate indicator of cardiopulmonary function,17 which reflects the heart’s reserve function. VO2/kg is an objective evaluation indicator that excludes the influence of weight differences. Gürdal et al18 divided 43 subjects into a group with diabetes and a normal control group. The results showed that the exercise capacity of the patients with diabetes was reduced significantly; their peak VO2, AT VO2, and peak HR all decreased, while their resting HR increased. HbA1c was negatively correlated with maximal VO2. However, a study found that, compared with the normal control group, there was no difference in the peak VO2 of relatively young patients with well-controlled type 2 diabetes with a course of fewer than 5 years and with no clinical complications or comorbidities.19 The AT VO2 levels in patients with type 2 diabetes were lowered in patients with microalbuminuria, but no abnormality was observed in patients without albuminuria.20 At the start of exercise, the adjustment of the supply of oxygen to the whole body was partly dependent on changes in HR. O’Connor et al21 found that elderly males with type 2 diabetes had slower HR dynamics, and diabetes and peak HR were negatively correlated. As diabetes worsened, peak HR decreased with an average reduction of 2.5–3.1%.22 The current study found that, compared with the normal plasma glucose group, the AT VO2, AT VO2/kg, peak VO2, peak VO2/kg, AT HR, peak HR, and 1-minute HR recovery levels all decreased, and the difference between the groups was statistically significant (P<0.05).
Previous studies have found that scientific and reasonable exercise therapy is an effective means for patients with type 2 diabetes to control their condition and reduce complications. The importance of exercise therapy in the treatment of type 2 diabetes has been recognized clinically, and the application of exercise therapy in the treatment of the disease has been the focus of increasing attention.23 Exercise improved insulin sensitivity in patients with type 2 diabetes and regulated glucose metabolism to lower plasma glucose levels; the principle of lowering plasma glucose is that the receptor affinity is enhanced (fat/muscle and insulin receptors) to increase intracellular glucose transporter activity and expression. This enhances insulin and tissue sensitivity and increases peak VO2. Under these combined effects, plasma glucose levels are reduced further.24 Concurrently, the researchers demonstrated that controlling the intensity of exercise was very important. For example, moderate-intensity exercise in patients with type 2 diabetes can improve insulin sensitivity, but strenuous exercise can cause hypoglycemia. Therefore, patients with diabetes must regulate their exercise intensity and control their own plasma glucose levels and diabetes by using professional and scientific exercise treatment programs.25
Lynch et al26 implemented walking exercise interventions on 40 postmenopausal women with obesity; their body weight, total fat mass, visceral adipose tissue areas, and subcutaneous adipose tissue areas decreased significantly, while their peak VO2 increased. Among them, the reduction in abdominal visceral fat was related closely to the improvement in VO2 max levels. Among 74 non-obese, non-diabetic males, subjects with a large area of abdominal visceral fat had significantly lower anaerobic thresholds and VO2 max levels. There were no significant differences in HR, peak HR, or plasma pressure after exercise.27 The area of abdominal visceral fat was significantly negatively correlated with exercise tolerance. Karstoft et al28 undertook interval walking training with subjects with type 2 diabetes and found that their VO2 max increased by 16.1%±3.7%, while their glucose levels decreased. Glycosylated hemoglobin, cholesterol, and insulin resistance were reduced in patients with type 2 diabetes mellitus undergoing aerobic and resistance training, and peak oxygen uptake increased significantly.29 Moreover, when remotely monitored by application and heart rate band, the cardiopulmonary endurance of the intervention group increased more than that of the control group.30 Cardiopulmonary health was found to be negatively correlated with insulin resistance. The better the cardiopulmonary function, the lower the degree of insulin resistance, and the plasma glucose level tended to be normal.31 After using drugs to improve insulin resistance in patients with type 2 diabetes, plasma glucose levels decreased, and peak VO2 increased significantly by 7%.32,33 Essentially, the current study is consistent with the above research. The higher the AT VO2 and peak VO2 values, the lower the PPG level (P<0.05), while the higher the AT VO2/kg and peak VO2/kg values, the smaller the abdominal visceral fat area (P<0.05). The AT VO2/kg and peak VO2/kg values were negatively correlated with the area of abdominal visceral fat, while other indicators demonstrated no obvious relationship with plasma glucose levels or the area of fat.
The purpose of this study was to explore and identify the correlation between cardiorespiratory endurance indices and blood glucose levels and visceral fat in newly diagnosed type 2 diabetic male patients to provide more indicators for early prevention of diabetes and its complications and has a certain novelty. This study had the following limitations: all subjects were from the same area, the sample size was small, and the results of the study had certain limitations under external verification. Regarding the area and sample size of the research objects, it is anticipated that future research will involve multiregional and large-scale studies. Through the literature review, it was found that the results and conclusions of this study were of reference value because, in other existing similar studies, the results were consistent with the current study based on similar sample sizes. For example, in the article ‘Excess Visceral Adipose Tissue Worsens the Vascular Endothelial Function in Patients with Type 2 Diabetes Mellitus’, Akira Kurozumi et al,34 selected 71 patients with type 2 diabetes. The results of their study showed that excessive abdominal visceral fat in patients with type 2 diabetes led to the deterioration of vascular endothelial function, which further affected cardiopulmonary function in those patients. Furthermore, their study also proved a correlation between abdominal visceral fat and cardiopulmonary function in patients with type 2 diabetes which is consistent with the conclusions of the present study. In the article “Related Research on Cardiopulmonary Endurance of Men with Pre-diabetic Obesity in Men with Abdominal Obesity”, Liu Defeng et al35 assessed 73 subjects using CPETs; the results showed a correlation between the cardiopulmonary function indices of patients with diabetes and intra-abdominal fat, which is consistent with the results of the present study. In the article ‘Study on the Effect of Obesity on Cardiopulmonary Endurance of Patients with Type 2 Diabetes’, Bi Lina et al36 selected 87 patients with type 2 diabetes for CPETs. The results showed that cardiopulmonary endurance was correlated with the degree of obesity in patients, which is consistent with the conclusions of the current research. However, as the present study was conducted on male patients with type 2 diabetes, further research is needed to determine whether the results for female patients would differ.
Conclusions and Outlook
In summary, this study demonstrated that visceral fat and blood glucose levels increased in men with newly diagnosed type 2 diabetes, while cardiorespiratory endurance decreased. Moreover, blood glucose and visceral fat levels were correlated with cardiopulmonary function. With the increase in blood glucose levels and visceral fat, the indices of cardiopulmonary function decreased gradually. Therefore, the detection and control of visceral fat and blood glucose levels are not only beneficial to the health of diabetic patients but also helpful in identifying heart and lung function abnormalities relatively early, which is of great significance in preventing the occurrence of cardiopulmonary diseases. Patients with type 2 diabetes need to implement scientific and reasonable physical exercise to lower plasma glucose levels and abdominal visceral fat, increase VO2 levels, and strengthen cardiorespiratory endurance to prevent diabetes, cardiovascular disease, and other metabolic diseases. Additionally, medical/health institutions and the public should be aware of the relationship between cardiopulmonary endurance, BMI, abdominal visceral fat, and other chronic diseases, including diabetes. Indicators such as cardiopulmonary endurance, BMI, and abdominal visceral fat are effective reference indicators for the early detection and prevention of chronic diseases, including diabetes and cardiovascular disease. Therefore, it is important for medical and health professionals to acquire skills in evaluating (during daily physical examinations) an individual’s risk of diabetes by referencing the relationship between the above indicators, to promptly guide patients in improving their diets and lifestyles for diabetes prevention.
Comprehensive thinking should be applied when treating patients with type 2 diabetes. In addition to taking drugs to control plasma glucose levels, auxiliary methods, such as exercise therapy and dietary adjustment, should also be widely implemented to protect patients from other complications as much as possible and improve their quality-of-life. In addition to patients with diabetes, healthy people should also focus on their own comprehensive health status, develop a healthy lifestyle, actively exercise, and improve their diet to prevent the occurrence of diabetes.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was conducted in accordance with the declaration of Helsinki. And it was conducted with approval from the Ethics Committee of our Hospital.
Consent to Participate
Written informed consent was obtained from all participants.
Disclosure
The authors declare they have no conflicts of interest to disclose.
References
1. Martínez-Sánchez FD, Vargas-Abonce VP, Rocha-Haro A, et al. Visceral Adiposity Index is associated with Insulin Resistance, impaired Insulin Secretion, and β-cell dysfunction in subjects at risk for Type 2 Diabetes. Diabetes Epidemiol Management. 2021;2:100013. doi:10.1016/J.DEMAN.2021.100013
2. Lechner K, McKenzie AL, Kränkel N, et al. High-Risk Atherosclerosis and Metabolic Phenotype: the Roles of Ectopic Adiposity, Atherogenic Dyslipidemia, and Inflammation. Metab Syndr Relat Disord. 2020;18(4):176–185. doi:10.1089/met.2019.0115
3. Torimoto K, Okada Y, Mori H, et al. Relationship between fluctuations in glucose levels measured by continuous glucose monitoring and vascular endothelial dysfunction in type 2 diabetes mellitus. Cardiovasc Diabetol. 2013;12(1):1. doi:10.1186/1475-2840-12-1
4. Uribe-Heredia G, Arroyo-Espliguero R, Viana-Llamas MC, et al. Type 2 Diabetes Mellitus, Glycated Hemoglobin Levels, and Cardiopulmonary Exercise Capacity in Patients With Ischemic Heart Disease. Journal of Cardiopulmonary Rehabilitation and Prevention. 2020;40(3):167–173. doi:10.1097/HCR.0000000000000451
5. Pitocco D, Fuso L, Conte EG, et al. The Diabetic Lung - A New Target Organ? Rev Diabet Stud. 2012;9(1):23–35. doi:10.1900/RDS.2012.9.23
6. Neeland IJ, Ross R, Després JP, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes Endocrinol. 2019;7(9):715–725. doi:10.1016/S2213-8587(19)30084-1
7. Levelt E, Pavlides M, Banerjee R, et al. Ectopic and Visceral Fat Deposition inLean and Obese Patients With Type 2 Diabetes. J Am Coll Cardiol. 2016;68(1):53–63. doi:10.1016/j.jacc.2016.03.597
8. Herdy AH, Ritt LE, Stein R, et al. Cardiopulmonary Exercise Test: background, Applicability and Interpretation. Arq Bras Cardiol. 2016;107(5):467–481. doi:10.5935/abc.20160171
9. Galicia-Garcia U, Benito-Vicente A, Jebari S, et al. Pathophysiology of Type 2 Diabetes Mellitus. Int J Mol Sci. 2020;21(17):6275. doi:10.3390/ijms21176275
10. Patwardhan V, Khadilkar A, Chiplonkar S, et al. Dyslipidemia and Fat Distribution in Normal Weight Insulin Resistant Men. J Assoc Physicians India. 2019;67(7):26–29.
11. González N, Moreno-Villegas Z, González-Bris A, et al. Regulation of visceral and epicardial adipose tissue for preventing cardiovascular injuries associated to obesity and diabetes. Cardiovasc Diabetol. 2017;16(1):44. doi:10.1186/s12933-017-0528-4
12. Han M, Qin P, Li Q, et al. Chinese visceral adiposity index: a reliable indicator of visceral fat function associated with risk of type 2 diabetes. Diabetes Metab Res Rev. 2021;37(2):e3370. doi:10.1002/dmrr.3370
13. Tanaka S, Kanazawa I, Sugimoto T. Visceral fat accumulation is associated with increased plasma sphingosine-1-phosphate levels in type 2 diabetes mellitus. Diabetes Res Clin Pract. 2018;143:146–150. doi:10.1016/j.diabres.2018.07.003
14. Wang YN, Tian L, Di FS. The effect of cardiopulmonary exercise test in guiding precision exercise of patients with type 2 diabetes. J Tianjin Med Univ. 2020;2(3):222–225.
15. Jin L, Min G, Wei C, et al. Exercise training on chronotropic response and exercise capacity in patients with type 2 diabetes mellitus. Exp Ther Med. 2017;13(3):899–904. doi:10.3892/etm.2017.4084
16. Regensteiner JG. Type 2 diabetes mellitus and cardiovascular exercise performance. Rev Endocr Metab Disord. 2004;5(3):269–276. doi:10.1023/b:
17. Liu JM, Liu HJ. The basic concept of cardiopulmonary exercise test and its clinical significance. Chin J Tuberculosis Respir. 2012;35(12):954–956. doi:10.3760/cma.j.issn.1001-0939.2012.12.027
18. Gürdal A, Kasikcioglu E, Yakal S, et al. Impact of diabetes and diastolic dysfunction on exercise capacity in normotensive patients without coronary artery disease. Diab Vasc Dis Res. 2015;12(3):181–188. doi:10.1177/1479164114565631
19. Caron J, duManoir GR, Labrecque L, et al. Impact of type 2 diabetes on cardiorespiratory function and exercise performance. Physiol Rep. 2017;5(4):e13145. doi:10.14814/phy2.13145
20. Chun-Wing LA, Kwok-Wing LM, Tat-Chi LG, et al. Altered exercise gas exchange as related to microalbuminuria in type 2 diabetic patients. Chest. 2004;125(4):1292–1298. doi:10.1378/chest.125.4.1292.
21. O’Connor E, Green S, Kiely C, et al. Differential effects of age and type 2 diabetes on dynamic vs. peak response of pulmonary oxygen uptake during exercise. J Appl Physiol. 2015;118(8):1031–1039. doi:10.1152/japplphysiol.01040.2014
22. Green S, Egaña M, Baldi JC, et al. Cardiovascular control during exercise in type 2 diabetes mellitus. J Diabetes Res. 2015;2015:654204. doi:10.1155/2015/654204
23. Yang D, Yang Y, Li Y, et al. Physical Exercise as Therapy for Type 2 Diabetes Mellitus: from Mechanism to Orientation. Ann Nutr Metab. 2019;74(4):313–321. doi:10.1159/000500110
24. Duvivier BM, Schaper NC, Hesselink MK, et al. Breaking sitting with light activities vs structured exercise: a randomised crossover study demonstrating benefits for glycaemic control and insulin sensitivity in type 2 diabetes. Diabetologia. 2017;60(3):490–498. doi:10.1007/s00125-016-4161-7
25. Amanat S, Ghahri S, Dianatinasab A, et al. Exercise and Type 2 Diabetes. Adv Exp Med Biol. 2020;1228:91–105. doi:10.1007/978-981-15-1792-1_6
26. Lynch NA, Nicklas BJ, Berman DM, et al. Reductions in visceral fat during weight loss and walking are associated with improvements in VO(2 max). J Appl Physiol. 2001;90(1):99–104. doi:10.1152/jappl.2001.90.1.99
27. Shioya-Yamada M, Shimada K, Nishitani-Yokoyama M, et al. Association Between Visceral Fat Accumulation and Exercise Tolerance in Non-Obese Subjects Without Diabetes. J Clin Med Res. 2018;10(8):630–635. doi:10.14740/jocmr3403w
28. Karstoft K, Winding K, Knudsen SH, et al. The effects of free-living interval-walking training on glycemic control, body composition, and physical fitness in type 2 diabetic patients: a randomized, controlled trial. Diabetes Care. 2013;36(2):228–236. doi:10.2337/dc12-0658.
29. Bassi D, Mendes RG, Arakelian VM, et al. Potential Effects on Cardiorespiratory and Metabolic Status After a Concurrent Strength and Endurance Training Program in Diabetes Patients - a Randomized Controlled Trial. Sports Med Open. 2016;2:31. doi:10.1186/s40798-016-0052-1
30. Li J, Wei D, Liu S, et al. Efficiency of an mHealth App and Chest-Wearable Remote Exercise Monitoring Intervention in Patients With Type 2 Diabetes: a Prospective, Multicenter Randomized Controlled Trial. JMIR Mhealth Uhealth. 2021;9(2):e23338. doi:10.2196/23338
31. Chartrand DJ, Larose E, Poirier P, et al. Visceral adiposity and liver fat as mediators of the association between cardiorespiratory fitness and plasma glucose-insulin homeostasis. Am J Physiol Endocrinol Metab. 2020;319(3):E548–E556. doi:10.1152/ajpendo.00251.2020
32. Kadoglou NP, Iliadis F, Angelopoulou N, et al. Beneficial effects of rosiglitazone on novel cardiovascular risk factors in patients with type 2 diabetes mellitus. Diabet Med. 2008;25(3):333–340. doi:10.1111/j.1464-5491.2007.02375.x
33. Kadoglou NP, Iliadis F, Sailer N, et al. Exercise training ameliorates the effects of rosiglitazone on traditional and novel cardiovascular risk factors in patients with type 2 diabetes mellitus. Metabolism. 2010;59(4):599–607. doi:10.1016/j.metabol.2009.09.002
34. Kurozumi A, Okada Y, Arao T, et al. Excess Visceral Adipose Tissue Worsens the Vascular Endothelial Function in Patients with Type 2 Diabetes Mellitus. Intern Med. 2016;55(21):3091–3095. doi:10.2169/internalmedicine.55.6940
35. Liu DF, Jia XJ, Liu XL, et al. Correlative study on cardiopulmonary endurance in male pre-diabetic patients with abdominal obesity. Hebei Med. 2021;43(11):1689–1692. doi:10.3969/j.issn.1002-7386.2021.11.021
36. Bi LN, Zheng X, Qi YY, et al. The effect of obesity on the cardiopulmonary endurance of type 2 diabetic patients. Chin General Practice. 2021;24(27):3420–3423. doi:10.12114/j.issn.1007-9572.2021.00.496
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.