")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
A Comparison of the Real-Life Clinical Effectiveness of the Leading Licensed ICS/LABA Combination Inhalers in the Treatment for COPD
Authors Ming SWY, Haughney J , Ryan D , Small I, Lavorini F , Papi A , Singh D, Halpin DMG , Hurst JR , Patel S, Ochel M, Kocks J, Carter V, Hardjojo A , Price DB
Received 28 May 2020
Accepted for publication 26 October 2020
Published 26 November 2020 Volume 2020:15 Pages 3093—3103
DOI https://doi.org/10.2147/COPD.S263745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Simon Wan Yau Ming,1 John Haughney,2 Dermot Ryan,3 Iain Small,4 Federico Lavorini,5 Alberto Papi,6 Dave Singh,7 David MG Halpin,8 John R Hurst,9 Shishir Patel,10 Matthias Ochel,10 Janwillem Kocks,1,11,12 Victoria Carter,1 Antony Hardjojo,1 David B Price1,2
1Observational and Pragmatic Research Institute, Singapore, Singapore; 2Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Aberdeen, UK; 3Optimum Patient Care, Cambridge, UK; 4Peterhead Health Centre, Aberdeen, UK; 5Department of Experimental and Clinical Medicine, Careggi University Hospital, Florence, Italy; 6University of Ferrara, Ferrara, Italy; 7University of Manchester, Manchester University NHS Foundation Trust, Manchester, UK; 8Royal Devon and Exeter Hospital, Exeter, UK; 9UCL Respiratory, University College London, London, UK; 10Chiesi Limited, Manchester, UK; 11General Practitioners Research Institute, Groningen, the Netherlands; 12University of Groningen, University Medical Center Groningen, GRIAC Research Institute, Groningen, the Netherlands
Correspondence: David B Price
Centre of Academic Primary Care, Division of Applied Health Sciences, University of Aberdeen, Polwarth Building, Foresterhill, Aberdeen AB25 2ZD, UK
Tel +65 6802 9724
Email [email protected]
Introduction: The Fostair® 100/6 (BDP/FF) pressurized metered-dose inhaler, delivering an extrafine formulation, is licensed for asthma and COPD in the UK. However, its real-life effectiveness for COPD has not been evaluated. This study compared the clinical effectiveness of BDP/FF against other licensed ICS/LABA combination inhalers: the Seretide® Accuhaler® (FP/SAL) and the Symbicort® Turbohaler® (BUD/FF).
Methods: A matched historical cohort study was conducted using records of patients with diagnostic codes for COPD from the Optimum Patient Care Research Database (OPCRD). Patients who had received BDP/FF as their first ICS/LABA were matched 1:1 with patients who had received FP/SAL or BUD/FF, resulting in two matched comparisons. Additional analysis was conducted on patients who had never had diagnostic codes for asthma. Noninferiority in terms of the proportion of patients with moderate/severe COPD exacerbations on the different inhalers in the following year was assessed. Noninferiority was achieved if the upper CI limit were ≤ 1.2.
Results: This study included 537 and 540 patient pairs in the BDP/FF vs FP/SAL cohort and the BDP/FF vs BUD/FF cohort, respectively. The proportion of patients with COPD exacerbations in the BDP/FF group was not significantly different from either the FP/SAL (68.7% vs 70.2%, AOR 0.89, 95% CI 0.67– 1.19) or BUD/FF group (68.5% vs 69.4%, AOR 0.79, 95% CI 0.58– 1.08). Noninferiority of BDP/FF in preventing COPD exacerbations was fulfilled in both comparisons. In patients without asthma, BDP/FF was also noninferior to BUD/FF (proportion with COPD exacerbations, 67.8% vs 64.7%, AOR 0.79, 95% CI 0.51– 1.1997). Additionally, a significantly lower proportion of patients prescribed BDP/FF had COPD exacerbations than FP/SAL (64.8% vs 73.7%, AOR 0.64 95% CI 0.43– 0.96).
Conclusion: Initiating ICS/LABA treatment of COPD with extrafine-formulation BDP/FF was noninferior in preventing moderate/severe exacerbations compared to FP/SAL and BUD/FF.
Keywords: metered-dose inhaler, dry-powder inhaler, chronic obstructive pulmonary disease, treatment efficacy, cost-effectiveness
Plain-Language Summary
The Fostair® (BDP/FF) inhaler has been licensed for asthma and chronic obstructive pulmonary disease (COPD) treatment in the UK. The medicine is delivered as very small particles, which helps delivery to the lungs. However, how well BDP/FF works for COPD treatment has been studied only in controlled clinical trials, but not in real-life clinical practice settings. We aimed to assess how well BDP/FF prevents COPD exacerbations compared to other similar products licensed in the UK: Seretide® (FP/SAL) and Symbicort® (BUD/FF). General practice records stored in the Optimum Patient Care Research Database (OPCRD) were used in this study. The proportion of patients with COPD exacerbations in the year the inhalers were started were compared across the different groups. In patients prescribed BDP/FF, 68.7% experienced exacerbations compared to 70.2% prescribed FP/SAL. In the other comparison, 68.5% and 69.4% of patients prescribed BDP/FF and BUD/FF, respectively, experienced exacerbations. Therefore, prescription of BDP/FF led to comparable prevention of COPD exacerbations compared to prescription of FP/SAL or BUD/FF. Furthermore, BDP/FF was associated with better outcomes than FP/SAL within the group of patients without a previous history of asthma (35.2% vs 26.3% without exacerbations).
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by declining lung function associated with high morbidity and health-care burden.1 In the UK alone, an estimated 1.2 million people have COPD, with a much larger population remaining undiagnosed.2,3 COPD accounts for 1.4 million general practice (GP) consultations yearly and one in eight emergency attendances.4
Inhaled corticosteroid (ICS) is administered to reduce the risk of subsequent COPD exacerbation.5 Evidence from clinical trials has suggested efficacy of an ICS administered in combination with a long-acting β-agonist (LABA) for patients with moderate/severe COPD.6,7 The Fostair® 100/6 (BDP/FF) pressurized metered-dose inhaler (pMDI) has been licensed for patients with severe COPD (Forced Expiratory Volume in 1 second [FEV1] <50% predicted normal) and a history of exacerbations who have significant symptoms, despite regular therapy with long-acting bronchodilators.8 Other licensed ICS/LABA combination inhalers for COPD include the Seretide® Accuhaler® 500/50 (FP/SAL) dry-powder inhaler (DPI) and the Symbicort® Turbohaler® 200/6 and 400/12 (BUD/FF) DPI. BDP/FF, FP/SAL, and BUD/FF were the most commonly used ICS/LABA combination inhalers in the UK at the inception of this study.
The extrafine formulation of BDP/FF results in greater deposition to smaller airways, allowing for lower dosage for similar effects, thus subsequently reducing potential side effects compared to non-extrafine inhaler formulations.9–12 The efficacy of BDP/FF has been previously demonstrated in randomized controlled trials (RCTs). The FUTURE trial showed BDP/FF to be equivalent to FP/SAL in improving breathlessness scores and superior at improving FEV1 and St George’s Respiratory Questionnaire (SGRQ) scores, despite lower ICS dosage.13 Another trial also showed BDP/FF to be noninferior to BUD/FF in improving predose morning FEV1.11 Complementing the results from RCTs, a study in a real-life setting demonstrated BDP/FF to be noninferior to FP/SAL in preventing symptom exacerbation in patients with asthma at equal or lower dosage.14 However, there is a lack of studies investigating the effectiveness of BDP/FF in COPD patients. Investigation of the clinical effectiveness of each ICS/LABA may be beneficial in guiding treatment of COPD patients requiring an ICS/LABA combination inhaler.
The current study aimed to assess the noninferiority of initiating BDP/FF compared to FP/SAL and BUD/FF in terms of proportion of patients free from moderate/severe COPD exacerbations.
Methods
Study Design
This was a historical matched cohort study encompassing a 1-year baseline period prior to the index date for characterization of patients for matching and a 1-year outcome period after the index date to identify outcomes (Figure 1). The index date was defined as the date of first prescription of a BDP/FF pMDI, FP/SAL DPI, or BUD/FF DPI.
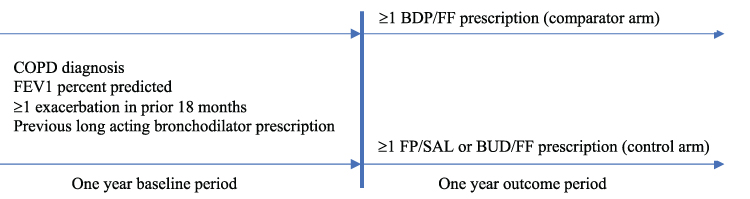 |
Figure 1 Study design. |
Data Source
Data for this study were obtained from the Optimum Patient Care Research Database (OPCRD; www.opcrd.co.uk), which comprises medical records of >7 million patients from over 700 GP practices across the UK.15 The OPCRD is approved by the Health Research Authority of the UK National Health Service for clinical research use (Research Ethics Committee reference 15/EM/0150).
Medication Studied
ICS/LABA combination inhalers with sufficient data in the OPCRD at the inception of this study — BDP/FF, FP/SAL, and BUD/FF — were chosen for this study. The BDP/FF investigated in this study was Fostair® , an ICS/LABA combination inhaler, containing 100 µg beclometasone dipropionate and 6 µg formoterol fumarate per inhalation in a pMDI device.16 The FP/SAL investigated in this study was the Seretide® Accuhaler® 500 DPI, containing 500 µg fluticasone propionate and 50 µg salmeterol xinafoate per inhalation in a DPI device.17 The BUD/FF investigated was the Symbicort® Turbohaler® , containing either 200 µg budesonide and 6 µg formoterol fumarate dihydrate (Symbicort 200/6) or 400 µg budesonide and 12 µg formoterol fumarate dihydrate (Symbicort 400/12) per inhalation in a DPI device.18,19 As the recommended dosage for BUD/FF is two puffs twice daily of 200/6 or one puff of 400/12, we assumed equal BUD/FF dosage in both groups and thereby combined them.
Inclusion Criteria
Inclusion and exclusion criteria and patient flow are presented in Table 1. Patients included were ≥35 years old with COPD diagnosis confirmed by spirometry reading (FEV1/Forced Vital Capacity [FVC] <0.7) and had at least one moderate to severe exacerbation within the 18 months prior to the index. They must also have had available data encompassing the entire baseline and outcome periods, had one or more prescriptions of LABA, LAMA, or unlicensed ICS/LABA combination inhaler in the 2 years prior to the index, and had received two or more prescriptions of the same licensed ICS/LABA combination inhaler during the outcome period (including initial prescription). Patients were excluded if they were recorded in the database to be nonsmoking or if there were no documentation of smoking status.
Patients were included if they had postbronchodilator FEV1% predicted <55% at any time prior to index. As a typical bronchodilator response is around 12%, patients with FEV1% predicted of 55% are expected to reflect patients with trough FEV1 predicted of 50% (reflecting the indication for BDP/FF).
Alternative comparison groups were selected excluding patients who had ever had a diagnostic code for asthma. This alternative comparison group was selected to investigate patients who had been treated with ICS/LABA specifically for COPD and not for asthma.
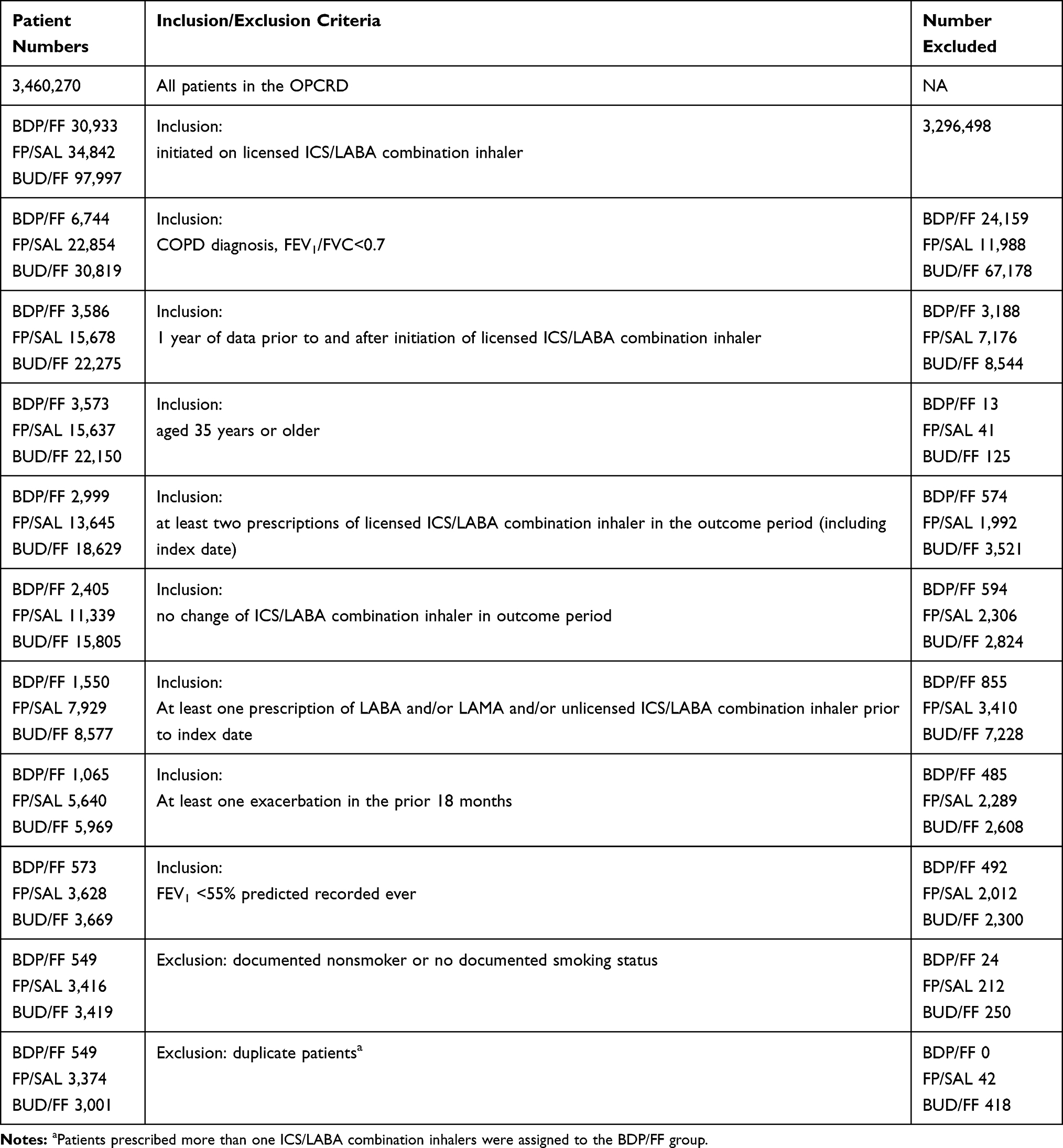 |
Table 1 Patient Flow and Inclusion and Exclusion Criteria |
Outcome Assessments
The primary outcome of this study was the proportion of patients with moderate/severe COPD exacerbations, defined as any of: 1) unscheduled respiratory related hospital admission or A&E attendance, 2) acute OCS prescriptions (definition provided in the online supplementary material), or 3) antibiotic prescriptions with a respiratory consultation in the 1-year outcome period.
Matching
Patients on BDP/FF pMDI were matched 1:1 with patients on FP/SAL and patients on BUD/FF, resulting in two matched comparisons. Patients who had been prescribed more than one type of ICS/LABA combination inhalers on separate occasions were selected only once during the comparison. The selected index patient event was the prescription of BDP/FF to maximize the number of matched pairs. Variables for matching were selected based on the standardized difference and bias potential on the proportion of patients with an exacerbation between the treatment arms and clinical relevance. The final matching variables consisted of age, smoking status, FEV1% predicted, and number of exacerbations during the baseline year. Patients in the additional analysis, excluding patients with an asthma diagnosis, were matched in the same manner.
Statistical Analysis
Based on a previous study,20 if there is a true difference in AOR in favor of BDP/FF compared to the standard difference of 1.2, 552 patients in each group are required to be 80% sure that the upper limit of a one-sided 97.5% CI will exclude a difference in favor of the predefined noninferiority margin of 20%.
Analysis was performed with SPSS version 23, SAS version 9.3, Stata SE version 14 (StataCorp, College Station, TX, USA), and Microsoft Office Excel 2013, as appropriate. Forest plots were generated using DistillerSR, an online tool from Evidence Partners.
Standardized mean difference (SMD) was calculated to quantify differences in baseline characteristics between compared treatment groups. An SMD ≥10 indicated sufficient imbalance between the groups. SMD was utilized over p-value, as it is unaffected by sample size and is thus a better way to judge imbalance.
Primary Outcome Analysis
Adjusted proportions of patients within each treatment group recording any exacerbations in the outcome period was calculated using a generalized linear model with binomial distribution and logit link (logistic regression). Conditional logistic regression analysis was performed on the matched data set, taking matching into account for matched pairs.
Selection of factors for adjustment started with a model with exposure as the only explanatory variable. Variables were added one by one from the highest individual bias potential and kept in the model if there was a change in estimate of at least 2% relative to the prior model.
Noninferiority of BDP/FF pMDI was achieved if the upper bound of the 95% CI for odds of patients reporting COPD exacerbations was no more than 20% higher than the odds in the comparator groups (ie, the higher CI was <1.20). The noninferiority limit was predetermined based on a study assessing COPD as the outcome.21 Superiority of BDP/FF was then claimed if the proportion was significantly lower at p=0.05.
Ethics
This study complied with all local and international laws and regulations, including ICH E6 guidelines for Good Clinical Practices, and governed by the Anonymous Data Ethics Protocols and Transparency (ADEPT) committee. This study was registered on the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP) database (EUPAS9142), and the study protocol was approved by the ADEPT committee (ADEPT1016).
Results
Patient Demographics
After applying the inclusion and exclusion criteria, 549, 3374, and 3001 patients prescribed BDP/FF pMDI, FP/SAL DPI, and BUD/FF DPI respectively, were identified. Unmatched background demographics for these subjects are presented in Table S1 of the online supplementary material. Following matching, the final study population consisted of 537 pairs of patients in the BDP/FF pMDI vs FP/SAL DPI cohort and 540 pairs in the BDP/FF pMDI vs BUD/FF DPI cohort. Matched baseline characteristics of both cohorts are presented in Table 2. Demographic characteristics were mostly balanced between groups in both pairs; however, fewer patients in the BDP/FF groups had been prescribed SABA compared to the FP/SAL (75.4% vs 83.2%) or BUD/FF (75.6% vs 82.2%) groups. The BDP/FF group also had more patients with modified Medical Research Council (mMRC) dyspnea scores of 3 or 4 (indicating severe breathlessness) than the FP/SAL group (25.2% vs 21.3%), but fewer than the BUD/FF group (24.7% vs 25.8%). Proportions of patients who had moderate/severe COPD exacerbations were 91.4% and 91.1% in each matched cohort, respectively. The exploratory analysis cohort (subjects without history of asthma diagnosis) consisted of 315 and 314 pairs of subjects in the respective matched cohorts. Baseline characteristics for patients in the exploratory analysis cohort are presented in Table S2 of the online supplementary material.
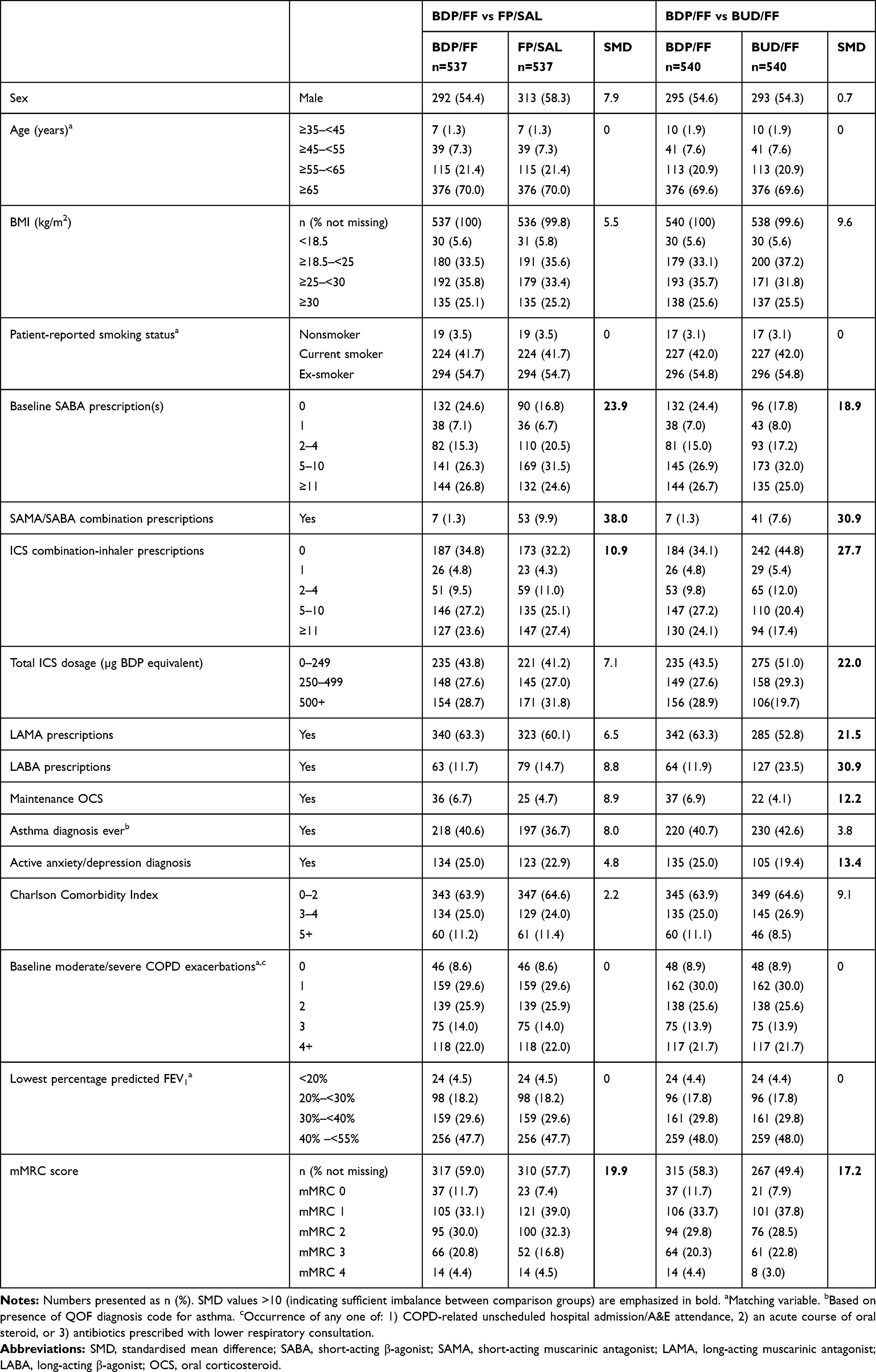 |
Table 2 Matched Baseline Patient Characteristics |
Prevention of COPD Exacerbations
Patients with Asthma Diagnosis Included
In the BDP/FF vs FP/SAL matched pair, the proportions of patients who had at least 1 COPD exacerbation were 68.7% and 70.2% respectively (AOR 0.89; 95% CI 0.67–1.19). The proportions of patients in the BDP/FF vs BUD/FF pair were 68.5% and 69.4% respectively (AOR 0.79; 95% CI 0.58–1.08). As the upper limits of the 95% CI in both pairs were lower than the pre-defined noninferiority margin of 1.2, BDP/FF was noninferior to both FP/SAL and BUD/FF in preventing subsequent exacerbations (Figure 2). Unadjusted OR are provided in the online supplementary material (Table S3).
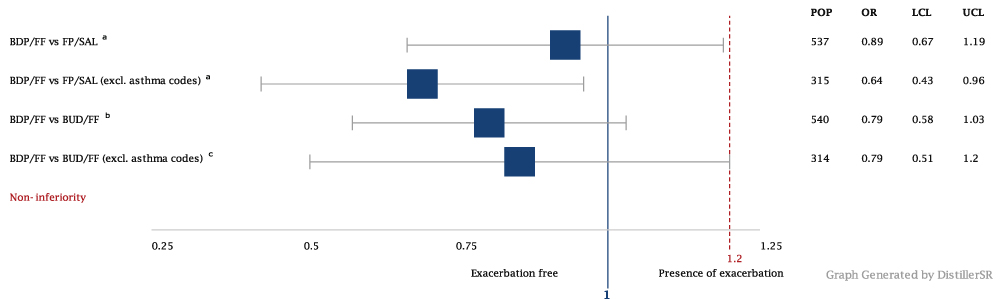 |
Figure 2 Odds ratios for COPD exacerbation between BDP/FF and FP/SAL or BUD/FF. |
Patients with Asthma Diagnosis Excluded
Among patients who never had an asthma diagnosis, proportions of those prescribed BDP/FF and BUD/FF who had at least one COPD exacerbation in the outcome period were 67.8% vs 64.7%, respectively (AOR 0.79, 95% CI 0.51–1.1997), thus also fulfilling the noninferiority criterion for prevention of COPD. However, in addition to being noninferior, BDP/FF was also superior to FP/SAL within this comparison group (64.8% vs 73.7%, AOR 0.64, 95% CI 0.43–0.96).
Discussion
Summary of Findings
In this real-life observational study, the Fostair® 100/6 (extrafine formulation BDP/FF) pMDI was found to be noninferior to both the Seretide® Accuhaler® 500/50 (FP/SAL) DPI and the Symbicort® Turbohaler® 200/6 (two puffs twice daily dose) and 400/12 (one puff twice daily dose) (BUD/FF) DPI in terms of the proportion of patients experiencing a COPD exacerbation within a year since treatment initiation.
To the best of our knowledge, this is the first study to evaluate the clinical effectiveness of BDP/FF pMDI compared with other ICS/LABA combination inhalers for management of COPD within a real-life setting. This study adds evidence to the current literature, which has established the efficacy of extrafine formulation BDP/FF for the management of COPD via RCTs.11, 13, 22,23 The observed efficacy of BDP/FF may also be partly due to the extrafine formulation, which has been demonstrated to be advantageous over fine-particle ICS in both asthma24 and COPD.25
The National Institute for Health and Care Excellence (NICE) guidelines for COPD recommend consideration of ICS/LABA in patients with features of asthma or a higher blood-eosinophil count.26 This study showed that in a real-life setting, BDP/FF has an advantage over FP/SAL in COPD patients without asthma.
Strengths and Weaknesses
The current study investigated the effectiveness of BDP/FF within a real-life observational setting. RCTs employ inclusion and exclusion criteria to ensure high internal validity for the investigation of the investigational products’ efficacy at the cost of their external generalizability.27 Real-life studies complement RCTs by enabling investigation on a wider range of subjects, including those typically excluded in RCTs. Therefore, our results may be more representative of patients managed in real-life health-care practice.28 Regardless, this study’s inclusion criteria reflected the population of COPD patients indicated for BDP/FF, thus supporting the findings from previous RCTs with real-life evidence.7,11
Another strength of this study is the observation of outcomes of initiating ICS/LABA-combination inhalers over a 1-year outcome period. Therefore, any transient or seasonal changes that may have affected outcomes were minimized.
The limitation of this study is inherent to its nature as a historical study. Despite extensive quality control and validation, records collected in the OPCRD were not initially collected for research, but for routine clinical purposes. As such, some degree of inaccuracy and incompleteness may be present. Also inherent to retrospective studies is the inability to control for potential confounders and variables not recorded in the database.
After applying all inclusion and exclusion criteria, the number of matched pairs in both comparison groups (n=537 and 540) fell short of the number required to be 80% sure that the upper limit of a one-sided 97.5% CI will exclude a difference in favor of the predefined noninferiority margin of 20%. However, the upper bound of the CIs of both comparison groups still fell under 1.20. We used different adjustment variables for each comparison pair in our analysis for the OR for COPD exacerbation. This was conducted as each matched comparison pair was drawn from different patient populations. However, this may have included a risk of overfitting to our statistical models.
As data on medication usage were not captured in the OPCRD,29 the current study was unable to control completely for adherence to prescribed ICS/LABA in this study. It is well established that despite its impact on the outcome of inhaler treatment, poor adherence is common among asthma and COPD patients.30,31 Therefore, future observational studies evaluating the effectiveness of inhalers might consider stratifying patients by their adherence to their prescribed ICS/LABA inhalers. A possible proxy for the measurement of adherence from clinical records includes medication possession ratio, defined as the ratio between the actual and expected number of medications prescribed.30–32
The current study was unable to account for proper use and handling of inhaler devices, which are vital for optimal delivery of drugs to the lungs.33 Poor inhaler technique is known to be very common among patients with COPD, especially in a real-life setting.34–36 Even though BDP/FF is now licensed with a DPI device, this study analyzed the real-world performance of an extrafine-formulation BDP/FF pMDI. Regardless, this study shows that in a real-life setting, where imperfect inhaler-handling techniques might exist, in addition to the potential imperfect adherence to therapy, the BDP/FF pMDI was not inferior to FP/SAL or BUD/FF DPI.
Lastly, despite the noninferiority and superiority observed when comparing BDP/FF against BUD/FF and FP/SAL in the exploratory analysis group of patients without asthma, further investigation is required, as this exploratory group was not sufficiently powered for a noninferiority analysis.
Future Studies
COPD is a complex disorder with multiple underlying phenotypes that may respond differently to therapy.37 In this study, we observed differential responses to BDP/FF compared to FP/SAL among COPD patients without asthma. Further investigation on the differential responses to FDC ICS/LABA by other phenotypic markers, such as peripheral blood eosinophil level is of interest.
The scope of our current study was limited to FDC ICS/LABA licensed for COPD in the UK at the time of this study’s conception. Future studies may be conducted to repeat our analyses for comparison of BDP/FF with other licensed ICS/LABA combinations, such as FF/Vilanterol FDC (Relvar Ellipta). Our current study also focused on the comparative effectiveness of BDP/FF pMDI. Drug tolerability for BDP/FF pMDI may also be considered for the outcome of subsequent studies.
Conclusion
This study showed that in a real-life practice setting, the extrafine-formulation BDP/FF pMDI was found to be noninferior to both FP/SAL DPI and BDP/FF DPI in terms of the proportion of patients with COPD exacerbations within 1-year after ICS/LABA combination/inhaler prescription. Lastly, within patients without a history of asthma, our results suggested that initiation of BDP/FF may be associated with a lower proportion of patients with subsequent COPD exacerbations compared to initiation with FP/SAL.
Abbreviations
BDP, beclometasone dipropionate; BUD, budesonide; COPD, chronic obstructive pulmonary disease; DPI, dry-powder inhaler; ENCePP, European Network of Centres for Pharmacoepidemiology and Pharmacovigilance; ERS, European Respiratory Society; FEV1, forced expiratory volume in 1 second; FF, formoterol; GOLD, Global Initiative for Chronic Obstructive Disease; GP, general practitioner; ICS, inhaled corticosteroid; LABA, long-acting β-agonist; LAMA, long-acting muscarinic antagonist; mMRC, modified Medical Research Council; OPCRD, Optimum Patient Care Research Database; pMDI, pressurized metered-dose inhaler; SABA, short-acting β-agonist; SAL, salbutamol; SAMA, short-acting muscarinic antagonist.
Data-Sharing Statement
All relevant data are within the paper and its Supporting Information files. The data set supporting the conclusions of this article was derived from the UK Optimum Patient Care Research Database (www.opcrd.co.uk). We do not have permission to give public access to these databases; however, researchers may request access for their own purposes. The OPCRD has ethical approval from the National Health Service (NHS) Research Authority to hold and process anonymized research data (Research Ethics Committee reference 15/EM/0150).
Ethics Approval
This study was approved by the Anonymised Data Ethics Protocols and Transparency (ADEPT) committee, the independent scientific advisory committee for the OPCRD commissioned by the Respiratory Effectiveness Group. The study was designed, implemented, and registered in accordance with the criteria of the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (registration EUPAS9142).
Acknowledgments
The authors extend their thanks to Dr Kevin Gruffydd-Jones for his clinical and scientific input in the conduct and writing of this study. Dave Singh is supported by the National Institute for Health Research (NIHR) Manchester Biomedical Research Centre (BRC).
Author Contributions
The overall conduct of this study was supervised by DBP. All authors made a significant contribution to the work reported, whether is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This study was funded by Chiesi Limited. The sponsor is involved in the design and presentation of the study.
Disclosure
David Price has board membership with Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Circassia, Mylan, Mundipharma, Napp, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, and Teva Pharmaceuticals, consultancy agreements with Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Mylan, Mundipharma, Napp, Novartis, Pfizer, Teva Pharmaceuticals, and Theravance, grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute) from AKL Research and Development, AstraZeneca, Boehringer Ingelheim, British Lung Foundation, Chiesi, Circassia, Mylan, Mundipharma, Napp, Novartis, Pfizer, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Teva Pharmaceuticals, Theravance, and UK National Health Service, Zentiva (Sanofi Generics), has received payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mylan, Merck, Mundipharma, Novartis, Pfizer, Regeneron Pharmaceuticals, Sanofi Genzyme, and Teva Pharmaceuticals, payment for manuscript preparation from Mundipharma, Teva Pharmaceuticals, payment for the development of educational materials from Mundipharma, Novartis, payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Circassia, Mundipharma, Napp, Novartis, and Teva Pharmaceuticals, funding for patient enrolment or completion of research from Chiesi, Novartis, Teva Pharmaceuticals, Zentiva (Sanofi Generics), stock/stock options from AKL Research and Development, which produces phytopharmaceuticals, owns 74% of the social enterprise Optimum Patient Care (Australia and UK), 74% of Observational and Pragmatic Research Institute (Singapore), has a 5% shareholding in TimeStamp, which develops adherence-monitoring technology, is peer reviewer for grant committees of the Efficacy and Mechanism Evaluation Programme and Health Technology Assessment, and was an expert witness for GlaxoSmithKline. Dermot Ryan has received support to attend meetings, delivered educational events on behalf of, or provided consultancy to AstraZeneca, Chiesi, CGS, Teva, Trudell Medical, Novartis, BI, Optimum Patient Care, Meda/Mylan, Stallergenes, and GSK, and also reports personal fees from Optimum Patient Care, GSK, and Regeneron and nonfinancial support from Novartis, AstraZeneca, BI, and Mylan outside the submitted work. John R Hurst has received personal payment and payment to his institution (UCL), including research grants, reimbursement for advisory work and educational activities, and support to attend meetings from pharmaceutical companies that make medicines to treat COPD, which includes AstraZeneca, Boehringer Ingelheim, Chiesi and Novartis. There is no direct conflict of interest with this work. Dave Singh acquired sponsorship to attend international meetings, honoraria for lecturing or attending advisory boards, or research grants from various pharmaceutical companies, including Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Genentech, GlaxoSmithKline, Glenmark, Johnson and Johnson, Merck, Mundipharma, NAPP, Novartis, Pfizer, Peptinnovate, Pulmatrix, Skypharma, Takeda, Teva, Therevance, and Verona. Federico Lavorini has received in the last 5 years honoraria for lecturing or attending advisory boards from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Hikma, Menarini International, Mundipharma, Novartis, Orion Pharma, Teva, and Trudell International. David MG Halpin has received sponsorship to attend international meetings and honoraria for lecturing, attending advisory boards, and preparing educational materials from AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Novartis, Pfizer, Sanofi, and Teva. John Haughney reports grants and research supports from AstraZeneca and Boehringer Ingelheim and honoraria or consultation fees from AstraZeneca, Boehringer Ingelheim, Cipla, Chiesi, and Teva. Alberto Papi has received grants, personal fees, and nonfinancial support from AstraZeneca, Chiesi Farmaceutici, GlaxoSmithKline, Boehringer Ingelheim, Edmondpharma, Foondazione Maugeri, Merck Sharp & Dohme, Menarini, Novartis, Zambon, Teva, Pfizer, Takeda, Sanofi/Regeneron, Roche, and Mundipharma. Janwillem Kocks reports grants and personal fees from AstraZeneca, grants and personal fees from Boehringer Ingelheim, grants from Chiesi, grants and personal fees from GSK, grants and personal fees from Novartis, and grants from Mundi Pharma and Teva outside the submitted work. Iain Small reports personal fees from Chiesi, AstraZeneca, and NAPP, and other from BMJ Group and Pfizer outside the submitted work. Shish Patel and Matthias Ochel are employed by Chiesi, the sponsor of the study. Simon Wan Yau Ming, Victoria Carter, and Antony Hardjojo are employees of the Observational and Pragmatic Research Institute, which has conducted paid research on respiratory disease on behalf of the following organizations in the past 5 years: Anaxys, AstraZeneca, Boehringer Ingelheim, British Lung Foundation, Chiesi, Circassia (formerly Aerocrine), GlaxoSmithKline, Harvey Walsh, Mapi, Morningside Healthcare, Mundipharma, Mylan (formerly Meda), Napp, Novartis, Orion, Plymouth University, Regeneron, Respiratory Effectiveness Group, Roche, Sanofi, Takeda, Teva, University of East Anglia, and Zentiva (a Sanofi company). The authors report no other conflicts of interest in this work.
References
1. Price D, Chisholm A, Ryan D, Crockett A, Jones R. The use of roflumilast in COPD: a primary care perspective. Primary Care Respiratory j. 2010;19(4):342–351. doi:10.4104/pcrj.2010.00066
2. Chronic obstructive pulmonary disease (COPD) statistics. Available from: https://statistics.blf.org.uk/copd.
3. Chronic obstructive pulmonary disease in over 16s: diagnosis and management. Available from: https://www.nice.org.uk/guidance/cg101.
4. Stockton-on-tees Borough Council. Joint Strategic Needs Assessment. 2009.
5. Price D, Yawn B, Brusselle G, Rossi A. Risk-to-benefit ratio of inhaled corticosteroids in patients with COPD. Primary Care Respiratory j. 2013;22(1):92–100. doi:10.4104/pcrj.2012.00092
6. Price D, West D, Brusselle G, et al. Management of COPD in the UK primary-care setting: an analysis of real-life prescribing patterns. Int J Chron Obstruct Pulmon Dis. 2014;9:889–904. doi:10.2147/COPD.S62750
7. Nannini LJ, Poole P, Milan SJ, Kesterton A. Combined corticosteroid and long-acting beta(2)-agonist in one inhaler versus inhaled corticosteroids alone for chronic obstructive pulmonary disease. Cochrane Database Systematic Reviews. 2013;8:Cd006826.
8. EMC. Fostair 100/6 inhalation solution. Available from: https://www.medicines.org.uk/emc/product/6318/smpc.
9. Scichilone N, Battaglia S, Sorino C, et al. Effects of extra-fine inhaled beclomethasone/formoterol on both large and small airways in asthma. Allergy. 2010;65(7):897–902. doi:10.1111/j.1398-9995.2009.02306.x
10. Scichilone N, Benfante A, Morandi L, Bellini F, Papi A. Impact of extrafine formulations of inhaled corticosteroids/long-acting beta-2 agonist combinations on patient-related outcomes in asthma and COPD. Patient Relat Outcome Meas. 2014;5:153–162.
11. Calverley PM, Kuna P, Monso E, et al. Beclomethasone/formoterol in the management of COPD: a randomised controlled trial. Respir Med. 2010;104(12):1858–1868. doi:10.1016/j.rmed.2010.09.008
12. Vehring R, Lechuga-Ballesteros D, Joshi V, Noga B, Dwivedi SK. Cosuspensions of microcrystals and engineered microparticles for uniform and efficient delivery of respiratory therapeutics from pressurized metered dose inhalers. ACS j Surfaces Colloids. 2012;28(42):15015–15023. doi:10.1021/la302281n
13. Singh D, Nicolini G, Bindi E, et al. Extrafine beclomethasone/formoterol compared to fluticasone/salmeterol combination therapy in COPD. BMC Pulm Med. 2014;14:43. doi:10.1186/1471-2466-14-43
14. Price D, Small I, Haughney J, et al. Clinical and cost effectiveness of switching asthma patients from fluticasone-salmeterol to extra-fine particle beclometasone-formoterol: a retrospective matched observational study of real-world patients. Primary Care Respiratory j. 2013;22(4):439–448. doi:10.4104/pcrj.2013.00088
15. OPCRD. The Optimum Patient Care Research Database (OPCRD). Available from: https://opcrd.co.uk/.
16. EMC. Fostair 100/6 inhalation solution. Available from: https://www.medicines.org.uk/emc/medicine/21006/SPC/Fostair+100+6+inhalation+solution/.
17. EMC. Seretide 100, 250, 500 accuhaler. Available from: https://www.medicines.org.uk/emc/medicine/2317.
18. EMC. Symbicort turbohaler 200/6 inhalation powder. Available from: https://www.medicines.org.uk/emc/medicine/4821.
19. EMC. Symbicort turbohaler 400/12, inhalation powder. Available from: https://www.medicines.org.uk/emc/medicine/11882.
20. Hagedorn C, Kassner F, Banik N, Ntampakas P, Fielder K. Influence of salmeterol/fluticasone via single versus separate inhalers on exacerbations in severe/very severe COPD. Respir Med. 2013;107(4):542–549. doi:10.1016/j.rmed.2012.12.020
21. Magnussen H, Disse B, Rodriguez-Roisin R, et al. Withdrawal of inhaled glucocorticoids and exacerbations of COPD. N Engl J Med. 2014;371(14):1285–1294. doi:10.1056/NEJMoa1407154
22. Wedzicha JA, Singh D, Vestbo J, et al. Extrafine beclomethasone/formoterol in severe COPD patients with history of exacerbations. Respir Med. 2014;108(8):1153–1162. doi:10.1016/j.rmed.2014.05.013
23. Singh D, Vezzoli S, Petruzzelli S, Papi A. The efficacy of extrafine beclomethasone dipropionate-formoterol fumarate in COPD patients who are not “frequent exacerbators”: a post hoc analysis of the FORWARD study. Int J Chron Obstruct Pulmon Dis. 2017;12:3263–3271. doi:10.2147/COPD.S141416
24. van der Molen T, Postma DS, Martin RJ, et al. Effectiveness of initiating extrafine-particle versus fine-particle inhaled corticosteroids as asthma therapy in the Netherlands. BMC Pulm Med. 2016;16(1):80. doi:10.1186/s12890-016-0234-0
25. Sonnappa S, Martin R, Israel E, et al. Risk of pneumonia in obstructive lung disease: A real-life study comparing extra-fine and fine-particle inhaled corticosteroids. PLoS One. 2017;12(6):e0178112. doi:10.1371/journal.pone.0178112
26. National Institute for Health and Care Excellence. Chronic obstructive pulmonary disease in over 16s: diagnosis and management; 2018. Available from: https://www.nice.org.uk/guidance/ng115.
27. Roche N, Reddel HK, Agusti A, et al. Integrating real-life studies in the global therapeutic research framework. Lancet Respiratory Medicine. 2013;1(10):e29–30.
28. Roche N, Reddel H, Martin R, et al. Quality standards for real-world research. Focus on observational database studies of comparative effectiveness. Ann Am Thorac Soc. 2014;11(Suppl 2):S99–104. doi:10.1513/AnnalsATS.201309-300RM
29. Dekhuijzen PNR, Batsiou M, Bjermer L, et al. Incidence of oral thrush in patients with COPD prescribed inhaled corticosteroids: effect of drug, dose, and device. Respir Med. 2016;120:54–63. doi:10.1016/j.rmed.2016.09.015
30. Covvey JR, Mullen AB, Ryan M, et al. A comparison of medication adherence/persistence for asthma and chronic obstructive pulmonary disease in the United Kingdom. Int J Clin Pract. 2014;68(10):1200–1208. doi:10.1111/ijcp.12451
31. Mueller S, Wilke T, Bechtel B, Punekar YS, Mitzner K, Virchow JC. Non-persistence and non-adherence to long-acting COPD medication therapy: A retrospective cohort study based on a large German claims dataset. Respir Med. 2017;122:1–11. doi:10.1016/j.rmed.2016.11.008
32. Steiner JF, Prochazka AV. The assessment of refill compliance using pharmacy records: methods, validity, and applications. J Clin Epidemiol. 1997;50(1):105–116. doi:10.1016/S0895-4356(96)00268-5
33. Wright J, Brocklebank D, Ram F. Inhaler devices for the treatment of asthma and chronic obstructive airways disease (COPD). Qual Saf Health Care. 2002;11(4):376–382. doi:10.1136/qhc.11.4.376
34. Melani AS, Bonavia M, Cilenti V, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105(6):930–938. doi:10.1016/j.rmed.2011.01.005
35. Molimard M, Raherison C, Lignot S, et al. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2017;49:2. doi:10.1183/13993003.01794-2016
36. Haughney J, Price D, Barnes NC, Virchow JC, Roche N, Chrystyn H. Choosing inhaler devices for people with asthma: current knowledge and outstanding research needs. Respir Med. 2010;104(9):1237–1245. doi:10.1016/j.rmed.2010.04.012
37. Montuschi P, Malerba M, Santini G, Miravitlles M. Pharmacological treatment of chronic obstructive pulmonary disease: from evidence-based medicine to phenotyping. Drug Discov Today. 2014;19(12):1928–1935. doi:10.1016/j.drudis.2014.08.004
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.