")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 12
A Comparison of the Process and Content of Sexual Communications Among African American Adolescent Children Living in Parent and Grandparent Headed Families
Authors Cornelius JB, Okoro F , Piper CN
Received 17 September 2020
Accepted for publication 21 November 2020
Published 7 January 2021 Volume 2021:12 Pages 1—8
DOI https://doi.org/10.2147/AHMT.S281662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Alastair Sutcliffe
Judith B Cornelius,1 Florence Okoro,1 Crystal N Piper2
1School of Nursing, University of North Carolina at Charlotte, Charlotte, NC, USA; 2Department of Public Health Sciences, University of North Carolina at Charlotte, Charlotte, NC, USA
Correspondence: Judith B Cornelius
School of Nursing, University of North Carolina at Charlotte, 9201 University City Blvd, CHHS 412B, Charlotte, NC 28223, USA
Email [email protected]
Introduction: The process of parental sexual communication has been shown to delay the sexual debut of adolescents; however, few studies have focused on extended family members such as grandparents. The purpose of this study was to compare the process and content of sexual communications among African-American adolescent children living in parent or grandparent headed families.
Methods: A secondary analysis of two de-identified datasets from 80 African-American adolescents was conducted.
Results: Findings indicated that there were no significant differences in the sexual communication process in relation to facilitators p= 0.38 and barriers p =0.23 with the discussions. There were however significant differences with adolescents’ attitudes (p = 0.04) and feelings regarding sexual abstinence (p =0.01), HIV prevention (p= 0.002) and teen pregnancy (p= 0.010).
Discussion: Researchers can use the results of this study as a beginning point in examining the sexual communication process in grandparent-headed families.
Keywords: adolescents, parents, grand parents, sexual communications, process, content
Introduction
Risky sexual behavior of ethnic minority youth is a major health concern due to the rising rates of sexually transmitted infections (STIs) including HIV/AIDS.1,2 African-American females have a higher rate of early sexual debut because they experience puberty earlier, at a time when they do not have the knowledge or cognitive ability to make well-informed decisions or understand the consequences of risky sexual behaviors.3 Due to their lack of knowledge and cognitive immaturity at early sexual debut, African American females become more vulnerable to sexual partners who exert power over them or victimize them.3 Data from the 2017 Youth Risk Behavior Survey4 indicated that black students (45.8%), when compared to white students (38.6%), reported having had engaged in sexual intercourse, were currently sexually active (31.3%); had sex with four or more persons during their lifetime (14.8%), reported using a condom the last time they had sex; (52.1%) and (7.6%) reported being forced to have sex.
While the age of first sexual intercourse is younger for African Americans (< than 15 years of age), it is an important predictor of adolescent pregnancy, and STIs.3,5 The influence of media and peers, older sexual partners, drug/alcohol use and lack of parental/custodial sexual communication and attachment, have also contributed to earlier sexual debut among minority adolescents.6 It has been hypothesized that parental sexual communication with early adolescents yields lower rates of STIs and postponement of sexual debut.6 As more adolescents begin to live in grandparent headed families, we need to study what the process of sexual communication (the ease, attitudes and feelings that adolescents have discussing sexuality topics with their parents or grandparents) is in these families. Many studies of parent-adolescent sexual communication have not analyzed parent and grandparent data separately. To our knowledge, there are no studies that differentiate the parental communication processes between adolescents from parent or grandparent-headed families. Taken together, we must identify differences in the sexual communication process based on the custodial caregiver sexual communication process with adolescents. The purpose of this manuscript was to examine the process and content of sexual communications among African-American adolescents living in parent and grandparent-headed families.
Literature Review
Parent-Adolescent Child Sexual Communications
Parents can reduce risky sexual behaviors as well as promote healthy lifestyles by effective sexual communication. Parents most often feel uncomfortable talking about sex with their adolescent children and tend to limit their topics of conversation to abstinence, therefore, never talking about contraceptive use.7,8 However, when one weighs the risks of early sexual initiation (STIs, HIV and teen pregnancy), there becomes a clear need to discuss the “hard issues.” Not only does the discussion of these topics enhance the understanding, processing, and acceptance of the messages, it allows for the repetition of content.9 Repetition of sexuality conversations increases contraceptive use, decreases the number of sex acts and delays teen debut.10 The timing of these discussions also matters. The more “on time” they are, meaning before sexual activity, the lower the sexual risk outcomes. Since more than one-third of adolescents have sex by the ninth grade, sexuality communications between parents and adolescents should occur before the age of 13.11,12
Research indicates that mothers are more likely to communicate about sex with their daughters than fathers.13,14 Proving the significance of parent-adolescent communications even further, research reveals that less frequent parent–child communication leads to less condom use.13 More parent-adolescent communication is associated with increased contraceptive use.13 This is critical since the use of condoms not only reduces the chance of pregnancy by 97% when used consistently and correctly, but also reduces the transmission of STIs and HIV.15
Current research shows that parents who approach their teens in an open and positive way can assume the sex educator role effectively, thereby, reducing the sexual consequences of their youth.16,17 For a lot of parents, sexual communications about delaying sexual relations were related to future success of their children.16,17 Reciprocal reluctance to initiate conversations exist and adolescents continue to have unmet needs. Parents believe that their adolescent children will approach them with questions, but children reported being unlikely to do so even if they had concerns.18
Grandparent-Adolescent Grandchild Sexual Communications
Nationally approximately 3 million grandparents are custodial caregivers of their grandchildren.19,20 Grandparents raising grandchildren is common among African-Americans.20,21 The number of grandparents in the United States has risen to 69.5 million individuals.22 Over 4.9 million grandparents reside with grandchildren.23 Approximately one quarter (24.2%) of African American grandparents are responsible for the custodial care of their grandchildren.24 This care sharing tradition occurs due to incarceration, substance abuse, unemployment, child neglect/abuse, teenage pregnancy, military involvement25 and now COVID-19. This provides an implication in which we need to compare how grandparents fare with the process of sexual communication as they often assume the primary caregiver role. Grandparents as young as 45 years of age are caring for their grandchildren, most of whom are living in poverty and have more feelings of isolation and depression than non-custodial grandparents.19
Few studies assess how grandparents communicate about sex and what the content of the sexual communication process is with their grandchildren.26–28 There is a lack of resources to aid grandparents with these sexual discussions.13,26–28 Research findings show that grandchildren are generally less positive about the sexual communication process than their grandparents due to reasons of embarrassment.13,26–28 Grandparents openly admit their uneasiness about sexual communications as well as their need for education to accurately relay the information.26–28
Research Questions
This study broadens the literature by exploring the nature of sexual communications among African-American adolescents and their custodial caregiver by specifically examining:
1. Is there a difference in the sexual communication process of African American adolescents relevant to the parental caregiver family (parent or grandparent) of the adolescent child?
Hypothesis: There will be a significant difference in the sexual communication process based on the parental caregiver family of the adolescent child.
2. Is there a difference in the attitudes, feelings, content, and sexual values of adolescents relevant to the sexual communications with their parental caregiver family?
Hypothesis: There will be significant differences in the attitudes, feelings, content and sexual values of adolescents based on sexual communications with the parental caregiver.
Methods
After receiving the University of North Carolina institutional review board approval, a secondary data analysis was conducted on two existing adolescent datasets to examine differences in the process and content of sexual communications with adolescents from parent and grandparent-headed families. The datasets are not freely available. The HIV Risk Reduction Survey (HRRS) was used to obtain data from African-American adolescents ages 11 to 13 years from a metropolitan area in Virginia.
The HRRS was a 50-item questionnaire which asked participants about the sexual communication process, attitudes and feelings about the process, sexuality content in the last 3 months and demographic characteristics. The sexual communication process was defined as the ease at which the adolescent felt that they could talk with the parental caregiver about sexuality topics.29,30
Process of Sexual Communication with Adolescents who live in Parent Headed Families (PHFs) and Grandparent Headed Families (GHFs)
Eight items completed by the adolescents, were used to assess the sexual communication process. The eight items related to feelings of embarrassment, being too young, to talk about sex, talking about sex would encourage sex, cannot talk about sex because they already know about it, do not need to talk because the parental caregiver will not listen, do not have enough knowledge to talk about sex, we do not talk about sex in the family, and that sex is too dirty to talk about with my parental caregiver. Each item was scored on a 5-point Likert scale ranging from (1) strongly disagree to 5 (strongly agree). Lower mean scores indicated positive agreement with the ease of sexuality discussions with the parental caregiver. The sum of the scores for the sexual communication process was 10–32. The alpha coefficients for these eight items were 0.85 for adolescents from PHFs and 0.70 for adolescents living in GHFs.
Adolescents’ Attitudes About Discussing Abstinence in PHFs and GHFs
Five items, completed by adolescents, were used to examine their attitudes about discussing abstinence with their parent or grandparent. These five items asked the adolescents if they felt that talking about abstinence will reduce STD/AIDS and pregnancy, talking about sex will make them feel closer to their parents or grandparents, that the parental caregiver will not listen or I will not listen if they talked about sex, that they would feel embarrassed talking with them (parental caregiver) about abstinence, and my parents or grandparents would be embarrassed if we talked about abstinence. Each item was scored on a 5-point Likert scale from (1) strongly disagree to strongly agree (5). Higher mean scores indicated positive attitudes about discussing abstinence with the parental caregiver. The sum of the scores ranged from 16 to 40. The alpha coefficients for these seven items were 0.65 for adolescents living in PHFs and 0.78 for adolescents living in GHFs.
Adolescents’ Feelings About Discussing Sexuality Topics in PHFs and GHFs
Twelve items completed by the adolescents, were used to examine their feelings about the sexuality process with their parental caregiver. The adolescents responded to questions that explored their feelings about talking with their parental caregiver on a 5-point Likert scale ranging from 1 (very bad idea) to 5 (very good idea), or 1 (disapprove strongly) to 5 (approve strongly). The items referred to sexual abstinence, HIV prevention and teen pregnancy. The sum of the scores ranged from 53 to 80. The alpha coefficients for these 12 items were 0.78 for adolescents living in PHFs and 0.75 for those living in GHFs.
Sexual Values of Adolescents Living in PHFs and GHFs
Five items answered by the adolescents were used to examine how they valued being in relationships, having sex, and being a virgin. The questions were: 1) I am too young to have sex, (2) a boy should be in a serious relationship before having sex, (3) a girl should be in a serious relationship before having sex, (4) being a virgin is good, and (5) I am proud to be remain a virgin during my teenage years. The responses required a response on a 5-point Likert scale from (1) strongly disagree to (5) strongly agree. The alpha coefficient for these items was 0.78 for adolescents living with both types of families.
Sexual Communication Topics Within the Past 3 Months
Based on previous research with adolescents, recall of sexual activity is commonly examined at 3 months.31 Thirteen questions addressed topics of sexuality communication with the parental caregiver, which occurred within the past 3 months. With these questions adolescents were given the choice to circle: (1) no (2) yes or (3) do not know.
The remaining seven questions allowed respondents to provide demographic data. Gender, church attendance, level of education, living arrangements, parents/grandparents– age, marital status and education were examined.
Data Analysis
The computer software, SPSS, was used to reveal descriptive statistics on each survey item included in this study. Except for the first 8 survey items (sexual communication process), higher mean scores indicated greater agreement with each item. We examined for differences among the individuals using t-tests and set the level of significance at p < 0.05. Spearmon rho was used to examine relationships among the sexual communication process.
Results
Sample
The sample consisted of 80 African American adolescents, 11–13 years of age, (mean 12.3 years SD 1.7) from two community-based organizations in the southeast region of the United States. Forty adolescents lived in PHFs and the other 40 lived in GHFs. The participants were primarily female (75%) and in the 7th grade (73%).
The majority of adolescents from PHFs lived with both parents (75%) who ranged in age from 31 to 59 years (mean 35 years SD 17.5), who had attended college (68%) and were employed full time (95%). Approximately half of the adolescents from GPHs lived with both grandparents (55%), who ranged in age from 48 to 79 years old (mean 64.5years SD 15.8 years). The majority of the grandparents were retired (83%) and had attended or completed high school (38%). All of the study participants attended church regularly (every Sunday and once or twice doing the week).
Sexual Communication Process
There were no significant differences with the facilitators (p =0.38) and barriers (p = 0.23) to the sexual communication process (see Table 1). Based on individual item analysis: adolescents from PHFs strongly agreed that they were embarrassed to talk about sex; cannot talk about sex because they already know about sex however identified that they did not have enough knowledge to discuss sex. They also agreed that they did not discuss sex in the family because it was too dirty to talk about. Equally both groups of adolescents believed that they did not need to talk about sex because their parental caregiver would not listen to them. One significant difference among the groups was that adolescents from GHFs believed that talking about sex would encourage sex (t= 4.65 p = 0.00) when compared to adolescents living in PHFs.
Attitudes and Feelings About the Sexual Communication Process
There was a significant difference among adolescents’ attitudes toward the sexual communication process (p =0.04) (see Table 1). Based on individual item analysis, adolescents from PHFs had more positive attitudes (t=2.10 p= 0.048) about the sexual communication process when compared to adolescents from GHFs. The adolescents from PHFs agreed that talking about abstinence with their parents would reduce their chances of STIs/HIV and pregnancy and that these discussions would bring them closer to their parents. When compared to adolescents from GHFs, adolescents from PHFs strongly agreed that their parents would be embarrassed if they discussed abstinence with them (t = 2.929, p = 0.000) and that discussing abstinence with their parental caregiver would result in a lower likelihood of STIs/AIDS risks (t = 1.986, p = 0.050).
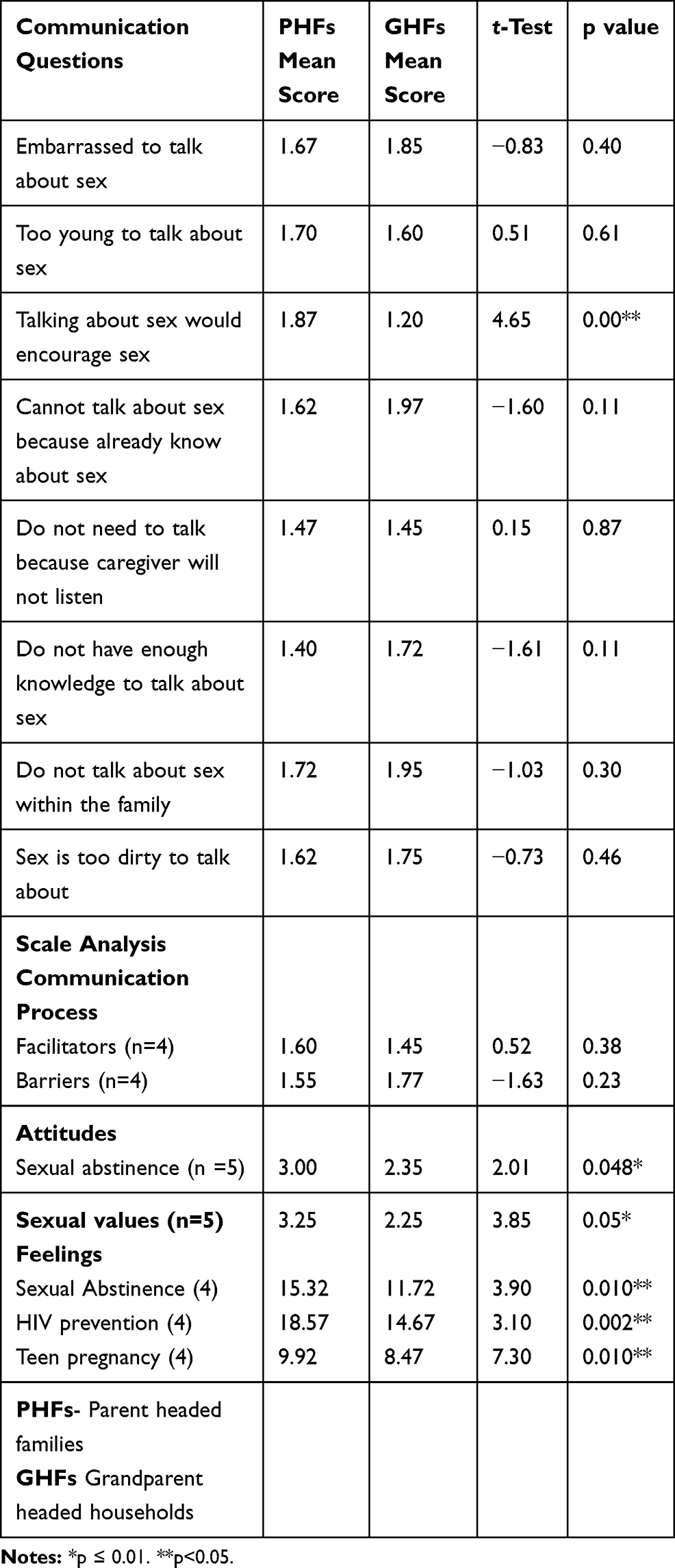 |
Table 1 Sexual Communication Process |
There were significant differences in how adolescents felt regarding discussions about sexual abstinence (p = 0.10), HIV prevention (p = 0.02), and teen pregnancy (p =0.10) as shown in Table 1. Adolescents from PHFs felt more positive discussing sexual abstinence (mean = 15.32), HIV/STI prevention (mean = 18.57), and teen pregnancy (mean = 9.92) when compared to adolescents from GHFs.
Sexual Values
There was a significant difference in the sexual values of adolescents from PHF when compared to those from GHPs (p = 0.05) (see Table 1). Adolescents from PHFs when compared to adolescents from GHFs valued being a virgin (t = 3.85 p < 0.05); were proud to remain a virgin during teenage years (t = 4.65 p < 0.05) and believed that it is important for a girl to be in a committed relationship before engaging in sexual activity (t= 1.98 p < 0.05). Adolescents from GHFs strongly agreed that a boy should be in a serious relationship before sex rather than the girl (t = 2.92 p = 0.03), and that they were too young to have sex (t = 1.87 p < 0.05) when compared to adolescents from PHFs.
Sexual Communication Content Discussed Within the Previous 3 Months
The content of sexual communications discussed within the previous 3 months is shown in Table 2. There were significant differences in the adolescents’ responses based on the family type. Adolescents from GHFs indicated that topics such as sexual intercourse, birth control, HIV prevention, condoms (giving condoms before going out, taught how to use condoms), and the importance of not using drugs and alcohol were discussed more frequently when compared to adolescents living in parent headed households.
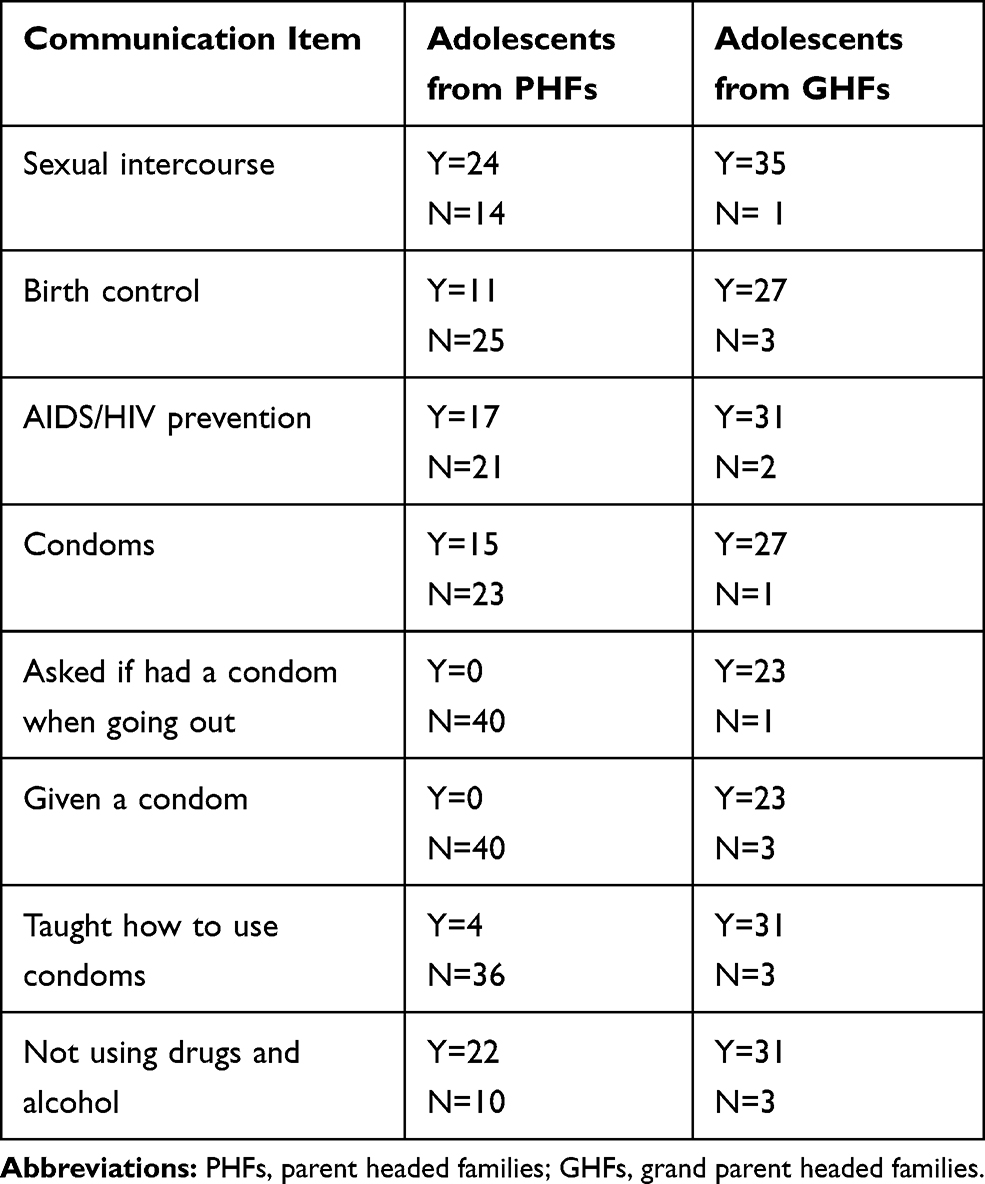 |
Table 2 Sexual Communication Content with Parental Caregiver Within the Past 3 Months |
Discussion
The goals of this study were to compare the process and content of sexuality communications (attitudes, feelings and values) among adolescents 11 to 13 years of age living in parent or grandparent headed families. From our analysis, adolescents from PHFs when compared to adolescents from GHFs were more positive about the openness of sexual communication with their parental caregiver. Adolescents from PHFs agreed that they felt closer to their parents when discussing sexual abstinence, which they felt resulted in a reduction of teen pregnancies and STI/AIDS infection rates. Similar to other research, discussions about sexual abstinence are reported to occur more often with adolescents who live with their parents29 when compared to grandparents. A close, satisfying parent–child relationship is crucial in delaying sexual activity and increasing the use of birth control. Adolescents with this type of relationship use condoms more consistently and have fewer risk-taking behaviors.30 In this study, the adolescents from GHFs reported more discussions about condom use when compared to adolescents to living in PHFs. The timing of these communications with adolescents living in PHFs may be occurring too late. In one study, Overbeek et al.31 identified that parent–child communications about sex occur “after the fact,” when the child is already sexually active. When parental caregivers educate their teens who they believe are sexually active, a buffering effect results in a delay or cessation of sexual activity.31
One meaningful finding of this study was that adolescents from GHFs thought that they were too young to discuss sexual issues with their parental caregiver but felt that their caregivers believed that they were not too young to participate in sexual behaviors. Adolescents who experience precocious puberty may be at risk from sexual coercion from older partners, depression, and substance use. Copeland et al.32 found that early puberty developers have increased sexual risk behaviors when compared to their on-time peers. The need to begin sexual communications before puberty is vital to the mental and sexual health of adolescents.
Despite the differences between these two groups, there was one similarity worth noting. More adolescents from GHFs did not value being a virgin and were not proud to remain a virgin throughout their teen years when compared to adolescents from PHFs. This finding could be explained by the content of sexual communications that is occurring in GHFs. Over the past 3 months, adolescents from GHFs reported more discussions about sexual intercourse and condoms instead of abstinence. Reasons for why grandparents are providing care to their grandchildren could be related to the negative consequences of the risky behaviors of their own children hence reasons why they discussed sexual content (ie, condoms and birth control) more often. Although adolescents reported being embarrassed when their grandparents discussed sexuality topics with them the timing and repetition of these discussions are important.33 If sexual topics are introduced by grandparents at age-appropriate levels and are spoken of more than once, then the adolescents may begin to feel more comfortable with the sexual communication process.
On the contrary, adolescents from PHFs strongly agreed that a girl should be in a serious relationship before having sex. This is consistent with other research about what motivates girls to delay their sexual debut. Long-Middleton et al.34 found that younger girls feared the incidences of HIV in the African American community while boys have not. As a result, younger girls found abstinence to be a motivator in delaying their sexual activity.
Presently, we know very little about the long-term consequences of sexual communications on the sexual health of minority youth being raised by grandparents. Indeed, a greater explanation of how this process occurs in GHFs is warranted. As the nation begins to address plans to end COVID- 19 and the HIV epidemic, health care organizations are planning strategies to eradicate these diseases. We can begin by targeting those who are sexually inactive (anticipators) to provide them with primary prevention tools. This will allow them to be educated before engaging in sexual activity rather than implementing interventions after sexual patterns are established.35 If parents or grandparents are uncomfortable with open sexual communications with their adolescent children, they are placing them at risk for teen pregnancy and STIs including HIV.
STI rates have dramatically risen over the past few decades36,37 while rates of teen pregnancy have decreased.38 The number of adolescents living with grandparents has changed family dynamics with the process of sexual communication. No study has been conducted on how this affects adolescents’ life learning experiences with sexual health. How or when adolescents should receive sexual education from their parental caregiver remains one of the unknowns? The present study is one of a few that has examined the sexual communication process, content, attitudes, feelings and sexual values among African-American adolescents from parent and grandparent headed families.
Limitations
While this study is a direct attempt at closing this literature gap, there are a few limitations, which should be noted. First, the study only included adolescents aged 11–13 from one geographical region of the US who attended church regularly; therefore, findings cannot be generalized to all adolescents. There were few male participants in the study which may have skewed the findings. There were major educational differences between the adolescents’ caregivers education, which could have contributed to differences in the sexual communication process and content. Second, the sample of the original study was one of convenience. The choice to not have a randomized sample may have produced biased responses altering our findings. Third, this secondary analysis relied upon a database of self-report which represents a cause for caution, due to possible socially desirable responses. Last, the measure of sexual communication content would have been stronger if there were a continuum of responses instead of yes, no or do not know.
Nonetheless, this study provides needed insight into the status of family sexuality communications, especially inter-generational communication, among African Americans. The results imply assistance is needed for parents, but more importantly for grandparents, to help decide what and when to discuss sexual topics with their adolescents so they may benefit from these communications rather than be embarrassed by them. This study has provided a starting point in which to investigate parent/grandparent-child sexuality communication processes based on the perceptions of adolescents, however, additional research using larger, randomized, more representable samples would add to the generalizability of these findings. Further studies should intently continue to explore how different parental units can promote safe sex behaviors.
Conclusion
With this secondary data analysis, the sexual communication process between adolescents from PHFs and GHFs were compared. Given that the results showed inconsistencies between the two groups, it can be hypothesized that there are actual differences in the communication processes relevant to the parental caregiver. It was also noted that the adolescents expressed that their grandparents spoke more frequently to them about sexual issues when compared to adolescent living in PHFs. With that in mind, the significance of educating parents and/or grandparents in addition to their adolescent children on sexual health topics remains vital.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Centers for Disease Control and Prevention. STDs in racial and ethnic minorities. Sexually Transm Dis Surveill. 2017;2018.
2. Ritchwood TD, Bishu KG, Egede LE. Trends in healthcare expenditure among people living with HIV/AIDS in the United States: evidence from 10 Years of nationally representative data. Int J Equity Health. 2017;16:188. doi:10.1186/s12939-017-0683-y
3. Zuckerman D. Early Puberty in Girls. National Center for Health Research; 2019.
4. Centers for Disease Control and Prevention. Youth risk behavior survey: Data summary and trends report. 2018b.
5. Magnusson B, Nield J, Lapane K. Age at first intercourse and subsequent partnering among adult women in the United States: a cross sectional study. BMC Pub Health. 2015;15:98. doi:10.1186/s12889-015-1458-2
6. ACT for Youth. Youth Statistics: Sexual Health; 2019.
7. Ashcraft A, Murray P. Talking to parents about adolescent sexuality. Ped Clinics North Am. 2017;64(2):305–320. doi:10.1016/j.pcl.2016.11.002
8. Grossman J, Jenkins L, Richer A. Parents‘ perspectives on family sexuality communication from middle to high school. Int J Envir Res Public Health. 2018;15(1):107. doi:10.3390/ijerph15010107
9. Burns JC, Caldwell CH. Breaking the ice! Predictors about communication between nonresident African American fathers and sons about sex. J Am Assoc Nurse Pract. 2015;28(2):84–90.
10. Hadley W, Lansing A, Barker D et al. The longitudinal impact of a family-based communication intervention on observational and self-reports of sexual communication. J Child Fam Stud. 2019;27(4):1098–1109. doi:10.1007/s10826-017-0949-4
11. Grossman JM, Charmaraman L, Erkut S. Do as I say, not as I did: how parents talk with early adolescents about sex. J of Fam Iss. 2016;37(2):177–197. doi:10.1177/0192513X13511955
12. Allen KR, Lavender-Stott ES. Family contexts of informal sex education: young men’s perceptions of first sexual images. Fam Rel. 2015;64(3):393–406. doi:10.1111/fare.12128
13. Flores D, Barroso J. 21st century parent-child sex communication in the United States: a process review. J Sex Res. 2017;54(4–5):532–548. doi:10.1080/00224499.2016.1267693
14. Wisnieski D, Sieving R, Grawick A. Parent and family influences on young women’s romantic and sexual decisions. Sex Educ. 2015;15(2):144–157.
15. Marfatia YS, Pandya I, Mehta K. Condoms: past, present, and future. Ind J Sex Trans Dis AIDS. 2015;36(2):133–139. doi:10.4103/0253-7184.167135
16. Widman L, Choukas-Bradley S, Nesi NS, Garrett J. K. Parent- adolescent sexual communication and adolescent safer sex behaviors: a meta-analysis. JAMA Pediatr. 2016;170(1):52–61. doi:10.1001/jamapediatrics.2015.2731
17. Murray A, Ellis M, Castellanos T, Gaul Z, Sutton M, Sneed C. Sexual health discussions between African-American mothers and mothers of Latino descent and their children. Sex Educ. 2014;14(5):597–608. doi:10.1080/14681811.2014.908767
18. Harris A. Parent-adolescent sexual communication. Nurs Womens Health. 2016;20(2):211–217. doi:10.1016/j.nwh.2016.01.002
19. American Association of Retired People. Grandparents report success in raising grandchildren. 2018.
20. Cancino A. More Grandparents Raising Their Grandchildren. Associated Press; 2016.
21. Bretha E, Crewe S. Parenthood in the twenty-first century: African American grandparents as surrogate parents. J Human Beh Soc Environ. 2013;23(2):178–192. doi:10.1080/10911359.2013.747348
22. Kropf N, Kelly S Why more grandparents are raising their grandchildren. 2017
23. Jayson S More grandparents than ever. 2017.
24. United States Census Bureau. Grandparents and Grandchildren. Census Blogs; 2016.
25. Grandfacts State Fact Sheets. 2017. Available from: http://www.grandfamilies.org/State-Fact-Sheets.
26. Cornelius J, LeGrand S, Jemmott L. African-American grandparents and adolescent grandchildren’s sexuality communication. J Fam Nurs. 2008;14(3):333–346. doi:10.1177/1074840708321336
27. Cornelius J, LeGrand S, Jemmott L. African American grandfamilies’ attitudes and feelings about sexual communication: focus group results. J Assoc Nurses AIDS Care. 2009;20(2):133–140. doi:10.1016/j.jana.2008.10.007
28. Cornelius J, Xiong P. Generational differences in the sexual communication process of African American grandparent and parent caregivers of adolescents. J Spec Ped Nur. 2015;20(3):203–209. doi:10.1111/jspn.12115
29. Hall K, McDermott S, Komro K, Santelli J. The state of sex education in the United States. J Adol Health. 2016;58(6):595–597. doi:10.1016/j.jadohealth.2016.03.032
30. Ritchwood T, Penn D, Peasant C, Albritton T, Corbie-Smith G. Condom use self- efficacy among younger rural adolescents: the influence of parent-teen communication and knowledge of and attitudes toward condoms. J Early Adol. 2017;37(2):267–283. doi:10.1177/0272431615599065
31. Napper L, Fisher D, Reynolds G, Johnson M. HIV risk behavior self-report reliability at different recall periods. AIDS Behav. 2010;14(1):152–161.32. doi:10.1007/s10461-009-9575-5
32. Copeland W, Shanahan L, Miller S, Costello E, Angold A, Maughan B. (Outcomes of early pubertal timing in young women: a prospective population-based study). Am J Psychiatry. 2010;167(10):1218–1225. doi:10.1176/appi.ajp.2010.09081190
33. Overbeek G, van de Bongardt D, Baams L. Buffer or brake? The role of sexuality-specific parenting in adolescents’ sexualized media consumption and sexual development. J Adol. 2013;47(7):1427–1439. doi:10.1007/s10964-018-0828-3
34. Long-Middleton E, Burke P, Lawrence C, Blanchard L, Amudala N, Rankin S. Understanding motivations for abstinence among adolescent young women: insights into effective sexual risk reduction strategies. J Ped Health Care. 2012;27(5):342. doi:10.1016/j.pedhc.2012.02.010
35. Planned parenthood: New CDC report on U.S. teen’s sexual behavior illustrates adolescents’ need for sex education and effective birth control. 2017.
36. American Sexual Health Association. New CDC Data Show That STD Rates Continue to Rise; 2019.
37. Samoff E, Mobley V Here’s why sexually transmitted infection rates are so high, according to STI experts. 2019.
38. Pew Research Center (2019). Why is the Teen Birth Rate Falling?; 2019.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.