")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 9
A comparative analysis of clinical outcomes and disposable costs of different catheter ablation methods for the treatment of atrioventricular nodal reentrant tachycardia
Authors Berman AE , Rivner H , Chalkley R, Heboyan V
Received 18 April 2017
Accepted for publication 27 July 2017
Published 6 November 2017 Volume 2017:9 Pages 677—683
DOI https://doi.org/10.2147/CEOR.S139861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Colombo
Adam E Berman,1–4 Harold Rivner,1 Robin Chalkley,1 Vahé Heboyan2
1Department of Medicine, Medical College of Georgia, 2Department of Clinical and Digital Health Sciences, College of Allied Health Sciences, 3Division of Cardiology, 4Department of Pediatrics, Medical College of Georgia, Augusta University, Augusta, GA, USA
Background: Catheter ablation of atrioventricular nodal reentrant tachycardia (AVNRT) is a commonly performed electrophysiology (EP) procedure. Few data exist comparing conventional (CONV) versus novel ablation strategies from both clinical and direct cost perspectives. We sought to investigate the disposable costs and clinical outcomes associated with three different ablation methodologies used in the ablation of AVNRT.
Methods: We performed a retrospective review of AVNRT ablations performed at Augusta University Medical Center from 2006 to 2014. A total of 183 patients were identified. Three different ablation techniques were compared: CONV manual radiofrequency (RF) (n=60), remote magnetic navigation (RMN)-guided RF (n=67), and cryoablation (CRYO) (n=56).
Results: Baseline demographics did not differ between the three groups except for a higher prevalence of cardiomyopathy in the RMN group (p<0.01). The clinical end point of interest was recurrent AVNRT following the index ablation procedure. A significantly higher number of recurrent AVNRT cases occurred in the CRYO group as compared to CONV and RMN (p=0.003; OR =7.75) groups. Cost-benefit analysis showed both CONV and RMN to be dominant compared to CRYO. Cost-minimization analysis demonstrated the least expensive ablation method to be CONV (mean disposable catheter cost = CONV US$2340; CRYO US$3515; RMN US$5190). Despite comparable clinical outcomes, the incremental cost of RMN over CONV averaged US$3094 per procedure.
Conclusion: AVNRT ablation using either CONV or RMN techniques is equally effective and associated with lower AVNRT recurrence rates than CRYO. CONV ablation carries significant disposable cost savings as compared to RMN, despite similar efficacy.
Keywords: catheter ablation, cryoablation, remote magnetic navigation, AVNRT, cost analysis
Introduction
The role of catheter ablation in the treatment of supraventricular tachycardias (SVTs) has become increasingly common worldwide. Catheter ablation offers the advantage of permanent cure of arrhythmia in a high percentage of cases.1–5 SVT represents a very common arrhythmia that is treated with catheter ablation. Among the various forms of SVT, the most common form seen clinically is atrioventricular nodal reentrant tachycardia (AVNRT). AVNRT is seen in a wide variety of populations, spanning the spectrum of age groups including pediatric and elderly patients where it may be particularly symptomatic.1
Catheter ablation of AVNRT conventionally targets the slow pathway (SP) of the atrioventricular (AV) nodal complex. While catheter ablation possesses a high level of success for the cure of AVNRT, there exists a risk of creating unintentional iatrogenic complete heart block (CHB) during energy delivery, thereby necessitating the need for implant of a permanent pacemaker.2 While undesirable in any patient, this complication is of particular significance in pediatric and adolescent patients, as their need for chronic pacing will span decades.
In an effort to minimize or even eliminate the risk of CHB during ablation of AVNRT, several modifications to the approach used during AVNRT ablation have been developed. These techniques include cryoenergy and remote magnetic navigation (RMN).3–13 Cryoablation (CYRO) utilizes freezing energy to ablate the SP of the AV nodal complex. RMN features magnetic technology that allows for very precise positioning of the ablation catheter while utilizing conventional (CONV) radiofrequency (RF) energy. The clinical cardiac electrophysiology program at the Medical College of Georgia, Augusta University Medical Center (AUMC), has experience performing catheter ablation of AVNRT using tradition manual RF ablation, CYRO, and RMN-guided techniques.
Few data exist comparing the direct disposable costs associated with each of these three ablation modalities when performing AVNRT ablations. We sought to review our clinical experience with these three ablation techniques analyzing both clinical outcomes and technology-specific direct costs related to these procedures.
The objectives of this study are to 1) determine whether the clinical recurrence rate of AVNRT differed between these three ablation techniques of catheter ablation and 2) conduct a cost analysis of the disposable technologies associated with each ablation modality. To address these objectives, we retrospectively analyzed our procedural database from 2006 to 2014 identifying patients who underwent AVNRT ablation via CONV manual techniques, CYRO, and RMN guidance at the AUMC.
Methods
The Augusta University Institutional Review Board approved this retrospective, chart-review study and waived the requirement for informed consent owing to the retrospective nature of the study. All patient data were treated confidentially. To determine those patients who underwent AVNRT catheter ablation at our center, a retrospective chart review of cardiac ablation procedures occurring at our institution between 2006 and 2014 was performed. Clinical information was acquired via a retrospective chart review of both the institutional electronic medical records as well as cardiac electrophysiology laboratory source data. Clinical and procedural data were collected by two study team investigators and then vetted by a third team member to ensure accuracy. Study eligibility criteria included those patients whose physician operator, performing the ablation procedure, was experienced in at least two of the three ablation modalities included in the analysis. Furthermore, patients (n=14) were excluded from analysis due to a plurality of ablation techniques that were utilized during the same catheter ablation procedure. A total of 197 patients who underwent catheter ablation of AVNRT between July 2006 and April 2014 were identified. Clinical demographics and procedural data were then tabulated.
Electrophysiologic procedure
All patients underwent electrophysiologic (EP) testing in the fasting state after providing written informed consent for the procedure. EP testing was performed with catheters positioned in the right atrium, His bundle territory, the coronary sinus, and the right ventricle. Both programmed stimulation and burst pacing were performed in an effort to induce AVNRT. Dual AV nodal physiology was defined as a ≥50 ms increase in the AH or HA interval during programmed stimulation from the atrium or ventricle, respectively. Once tachycardia was induced, the diagnosis of AVNRT was made according to commonly accepted criteria.14 A three-dimensional (3-D) mapping with either the Carto™ (Biosense Webster; Diamond Bar, CA, USA) or Ensite™ (St Jude Medical; Minneapolis, MN, USA) mapping systems were used in all cases. Patients then underwent catheter ablation of the SP of the AV nodal complex using one of the three different ablation modalities: manual RF energy, RMN-guided RF ablation, and CYRO. These three groups were then compared as defined in the following section.
Conventional manual RF ablation
Conventional manual RF energy was delivered to the SP region of the AV nodal complex using a 4 mm tip catheter guided by both electrogram and imaging techniques. RF energy was delivered until junctional beats were noted. If fast junctional beats occurred during RF energy delivery, RF energy was discontinued and resumed following the initiation of atrial pacing so as to ensure the absence of AH or PR interval prolongation. Energy was typically delivered in temperature control mode (50°C and 30–50 W).
The end point of the procedure was documentation of no further inducible AVNRT and no greater than 1 AV nodal echo beat with and without isoproterenol challenge after at least 15 minutes of postablation testing.
CYRO
CYRO of AVNRT was performed using either the 6 mm or 8 mm tip Freezor™ (Medtronic Inc., Minneapolis, MN, USA) catheters. CYRO was typically performed during AVNRT by positioning the cryocatheter in the region of the AV nodal SP complex via electrogram and imaging guidance. Cryoenergy was delivered during tachycardia and a successful location was defined as one that terminated tachycardia with block in the SP and did not result in significant AH prolongation. A series of consolidation lesions reaching –70ºC to –80ºC were placed in this region. The end point of the procedure was documentation of no further inducible AVNRT and preferably no AV nodal echo beats with and without isoproterenol challenge following at least 15 minutes of postablation testing.15
RMN-guided RF Ablation
RMN-guided catheter ablation of AVNRT was performed using the Stereotaxis™ system (Stereotaxis, Inc, St Louis, MO, USA). RF ablation was performed using either the RMT™ 4 mm or 3.5 mm open irrigation Thermocool™ catheters (Biosense Webster). An 8.5 Fr SR-0 sheath was conventionally used to promote catheter stability. RMN enabled positioning of the ablation catheter in the SP territory during sinus rhythm. RF energy was delivered at 50°C and 30–50 W using the 4 mm catheter and at 30–40 W using the open irrigation catheter. Junctional beats are not commonly observed with RF energy delivery using RMN guidance.16 Following delivery of a series of consolidation lesions, repeat EP testing was performed with and without isoproterenol infusion. Again, the procedure was deemed completed following at least 10–15 minutes of testing during which no further AVNRT could be induced while permitting up to a single AV nodal echo beat.
Procedural follow-up
All patients received a postablation electrocardiogram (ECG) to assess intervals and rhythm. Patients were then followed up as an outpatient at the discretion of the attending electrophysiologists. Patients who experienced recurrent symptomatic palpitations postablation were monitored as per clinical preference of their cardiologist. Follow-up data were assessed from scheduled clinic visits as well as analysis of repeat ECGs and outpatient monitoring performed following ablation.
End points
The primary end point of this study was documentation of recurrent AVNRT postablation. Secondary end points included development of iatrogenic CHB and cost analysis of the ablation technologies utilized in this study. Cost perspective was assessed at the hospital level and focused upon actual hospital disposable costs specific to each form of ablation. A full cost analysis of each procedure was not performed owing to the retrospective nature of this study. Disposable costs associated with each form of catheter ablation (RMN, CONV, and CRYO) were quantified using real hospital data during the year of the study’s completion.
Statistical analysis
Statistical analysis was performed using Stata™ (StataCorp, College Station, TX, USA). Continuous data are presented as mean ± standard deviation. Two-tailed tests were used and an α-level of 0.05 was considered significant. Continuous variables were compared using the one-way ANOVA test. Categorical variables were compared using the chi-square test and Fisher’s exact test. Chi-square tests and univariate logistic regression were used to determine and quantify the association between categorical demographic and clinical variables with the outcome of recurrence of AVNRT (yes or no). Multiple logistic regression models were used to assess the association of each clinical variable with the outcome of interest (recurrent AVNRT) while controlling for the others. Forward stepwise logistic regression was used to create the most parsimonious model for each of the three different ablation modalities. Cost-minimization analysis was performed according to accepted economic techniques.
Results
Patient demographics
A total of 183 patients who underwent catheter ablation of AVNRT during the specified study period at AUMC and who met entry criteria for this analysis were identified. Patients were distributed into one of three groups: CONV, RMN, and CRYO. Mean follow-up for all the three groups was 126 days. Baseline demographics are displayed in Tables 1 and 2. A significantly higher number of patients with underlying cardiomyopathy were present in the CONV ablation arm (p=0.01).
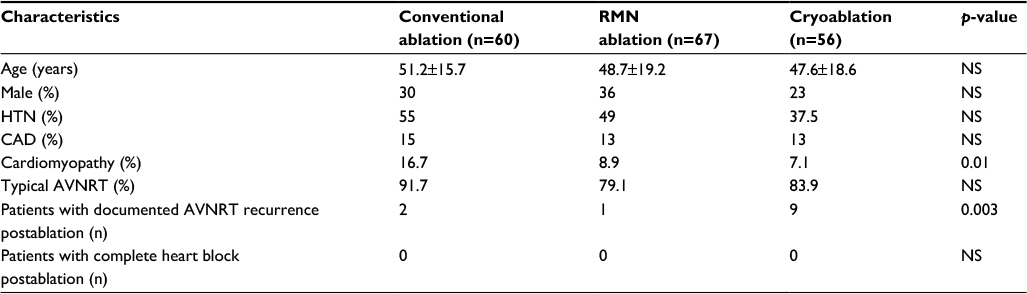 | Table 1 Baseline and postablation patient characteristics Note: Data are presented as mean ± SD. Abbreviations: AVNRT, atrioventricular nodal reentrant tachycardia; CAD, coronary artery disease; HTN, hypertension; RMN, remote magnetic navigation; NS, nonsignificant. |
 | Table 2 Baseline patient demographic data Abbreviations: RMN, remote magnetic navigation; NS, nonsignificant. |
Outcomes analysis
Table 3 displays the results of univariate logistic regression using recurrent AVNRT as the dependent variable while including the independent clinical variables mentioned in Table 1. Univariate analysis revealed CYRO to be the only predictor of the recurrence of AVNRT postablation: OR (95% CI) =7.75 (2.01, 29.8); p=0.003. Using documented recurrent AVNRT as the dependent variable, stepwise forward logistic regression was performed using the independent clinical variables in Table 1 for each of the three types of ablation modalities (CONV vs CRYO vs RMN). This revealed only CYRO and cardiomyopathy to remain in the model (χ2 LR =13.4, p=0.001 for the model). No cases of iatrogenic CHB were noted in any of the patients included in this study.
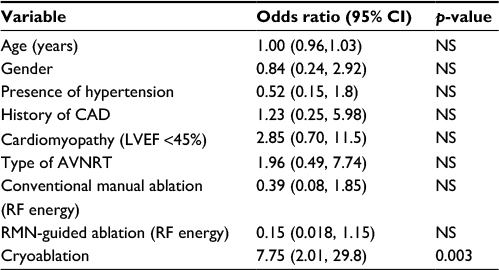 | Table 3 Results of univariate logistic regression using recurrent AVNRT as the dependent variable Abbreviations: AVNRT, atrioventricular nodal reentrant tachycardia; CAD, coronary artery disease; HTN, hypertension; LVEF, left ventricular ejection fraction; RF, radiofrequency; RMN, remote magnetic navigation; NS, nonsignificant. |
Cost analysis
We calculated our center’s disposable ablation catheter costs associated with each of the three specific different ablation modalities using hospital-specific pricing contractually in place during calendar year 2016. Costs for each ablation modality were compared using combinations of different catheters and 3-D mapping systems that were employed at our center during the timeframe encompassed by this retrospective analysis. When more than one 3-D mapping system could be used with the same dimension catheter, we included costs associated with the use of each mapping system for comparison. We then averaged the costs associated with each ablation modality for further analysis. Given the retrospective and nonrandomized nature of this study, other direct procedural costs were assumed to be constant and equal.
Disposable cost analysis revealed a substantial cost differential between different ablation/mapping modalities (Table 4). Cost-minimization analysis revealed CONV ablation to be dominant to RMN as equal procedural efficacy was observed between the two groups in our analysis. Both CONV and RMN were dominant to CRYO. Despite comparable clinical outcomes with no difference in the incidence of iatrogenic CHB, we observed a mean incremental cost associated with RMN ablation over manual CONV ablation of US$3094 per procedure.
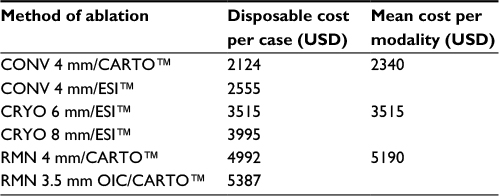 | Table 4 Disposable cost-comparison analysis of the different methods of catheter ablation of AVNRT Notes: Measurements refer to catheter tip size. ESI™ (Abbott Medical, Sylmar, CA, USA) and CARTO™ (Biosense Webster, Irvine, CA, USA) are 3-D mapping systems. Abbreviations: AVNRT, atrioventricular nodal reentrant tachycardia; CONV, conventional; CRYO, cryoablation; OIC, open irrigation catheter; RMN, remote magnetic navigation; USD, US dollars; 3-D, three-dimensional. |
Discussion
This study demonstrates our center’s observations regarding the outcomes and costs associated with a variety of ablative technologies used during the performance of catheter ablation of AVNRT. Our data support previous findings that manual RF ablation delivery is typically associated with improved long-term AVNRT outcomes when compared to CYRO. Deisenhofer et al reported on a total of 509 patients randomized either to CRYO or CONV manual ablation in a randomized controlled fashion.6 Their data revealed a significantly higher rate of AVNRT recurrence in the CRYO arm as compared to CONV ablation (9.4% vs 4.4%, p=0.029). Rodriguez-Entem et al conducted a randomized controlled trial comparing CRYO to CONV ablation.5 They found a significantly higher rate of AVNRT recurrence in the CRYO arm as compared to the CONV arm (15% vs 3.4%, p=0.029) at mean follow-up of 8 months.
Our study confirms the utility of RMN-guided RF ablation for the treatment of AVNRT. Wood et al performed a randomized controlled trial of RMN-guided RF ablation of AVNRT compared to manual RF energy delivery.17 In this study of 71 patients, there was no significant difference in acute success rates between the two groups (RMN 91% vs CONV 87%; p=NS). Bauerfeind et al reported on a registry of cases comparing the acute success of AVNRT ablation using RMN versus CONV ablation.18 Their data revealed a 100% acute success rate of ablation with RMNversus 97% acute success rate with CONV ablation (p=NS). Limitations of both of these studies, however, include a lack of follow-up data with respect to recurrent tachycardia. Our data support durable long-term freedom from recurrent AVNRT with both CONV and RMN ablation.
In addition, our study includes the largest number of patients in the literature comparing all three of these ablation modalities. A study published by Akca et al revealed no significant difference in acute procedural success in a total of 69 patients undergoing AVNRT ablation with either RMN, CRYO, or CONV ablation.12 However, their study was also characterized by non standardized follow-up.
RMN-guided AVNRT ablation has been demonstrated to be safe and effective.17–23 In addition, the precision of RMN-guided catheter delivery has the potential benefit of lower risk of permanent AV nodal injury. In this study, RMN was not associated with an increased risk of recurrence, only CYRO was. However, RMN-guided catheter ablation was associated with a significantly higher procedural disposable cost (Table 3). Hence, when one examines the three modalities employed at our center during AVNRT ablation, CONV manual RF ablation emerges as an efficacious and cost-saving technique. The creation of iatrogenic CHB remains a significant potential complication of AVNRT ablation.2 In an effort to mitigate this risk, CYRO has been advocated owing to its low risk of permanent and irreversible AV nodal injury.24,25 However, as seen in this study and others, this additive safety margin is accompanied by potentially lower long-term freedom from recurrent arrhythmia. Substantial cost savings were reported with CONV manual RF ablation with either mapping system as compared to both CRYO and RMN techniques.26
Limitations
This study is retrospective in nature and, as such, is susceptible to potential selection bias on the part of the operators whose cases were included in the study. Given the nonrandomized nature of this study, operators retained the latitude to select among the three ablation modalities in each individual patient’s circumstance. Nonetheless, these data represent a “real-world” population of patients whose baseline demographics only slightly differed from each other. Operator experience with the RMN system was limited to a single operator who utilizes the Stereotaxis™ system at our program. While CRYO is typically advocated in the young, our sample CRYO population comprised largely similarly aged adults as the CONV and RMN arms. An additional limitation of this retrospective study would be the natural improvement in skill set of the operators with increasing clinical experience in performing each ablation modality over the 9-year period analyzed in this study. While this limitation may apply to a reduction in arrhythmia recurrence, no cases of iatrogenic CHB occurred during the study period independent of the ablation modality utilized. At our center, CYRO continues to be the energy delivery source of choice for selected populations. However, RMN ablation has been used less frequently in more recent years owing to the increase in cost noted with this technology when compared to CONV ablation. In addition, RMN was unavailable at our center until 2010; therefore, all procedures performed prior to that were manual using either RF or CRYO.
One further limitation of our study was that all procedures were performed with the assistance of 3-D electroanatomic mapping. The use of 3-D mapping may significantly increase the disposable costs of the procedure, but may decrease fluoroscopic exposure and enhance the precision of ablation lesion delivery. A head-to-head comparison of direct costs associated with 3-D versus non-3-D mapping procedures would help clarify outcomes and costs associated with these two ablation techniques.
Inherent to the nature of retrospective studies, clinical follow-up is not necessarily standardized and therefore it is possible that some cases of AVNRT recurrence were either under-recognized or not treated at our center. Future prospective randomized studies comparing these three ablation modalities used for the treatment of AVNRT would further define the comparative efficacy and cost benefits of these technologies.
Conclusion
Both CONV and RMN-guided RF ablation of AVNRT are safe and effective for the treatment of AVNRT. Despite an excellent safety profile, CRYO was associated with a higher rate of recurrent tachycardia postablation. Cost-minimization analysis of our data surrounding disposable costs suggests a potentially significant cost savings associated with CONV RF ablation as compared to either CRYO or RMN-guided RF ablation without sacrificing patient safety or procedural efficacy. Further studies examining the cost-effectiveness of these different ablation modalities when treating both AVNRT and other arrhythmia substrates appear warranted given the potential opportunity for significant procedural cost savings without sacrificing safety and/or efficacy as was observed in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Page RL, Joglar JA, Caldwell MA. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia. J Am Coll Cardiol. 2016;67(13):e27–e115. | ||
Hintringer F, Hartikainen J, Davies DW, et al. Prediction of atrioventricular block during radiofrequency ablation of the slow pathway of the atrioventricular node. Circulation. 1995;92(12):3490–3496. | ||
Chan NY, Choy CC, Lau CL, et al. Cryoablation versus radiofrequency ablation for atrioventricular nodal reentrant tachycardia: patient pain perception and operator stress. Pacing Clin Electrophysiol. 2011;34:2–7. | ||
Chan NY, Mok NS, Lau CL, et al. Treatment of atrioventricular nodal re-entrant tachycardia by cryoablation with a 6 mm-tip catheter vs. radiofrequency ablation. Europace. 2009;11(8):1065–1070. | ||
Rodriguez-Entem FJ, Expósito V, Gonzalez-Enriquez S, Olalla-Antolin JJ. Cryoablation versus radiofrequency ablation for the treatment of atrioventricular nodal reentrant tachycardia: results of a prospective randomized study. J Interv Card Electrophysiol. 2013(6);36:41–45. | ||
Deisenhofer I, Zrenner B, Yin YH, et al. Cryoablation versus radiofrequency energy for the ablation of atrioventricular nodal reentrant tachycardia (the CYRANO Study): results from a large multicenter prospective randomized trial. Circulation. 2010;122:2239–2245. | ||
Kimman GP, Theuns DA, Szili-Torok T, Scholten MF, Res JC, Jordaens LJ. CRAVT: a prospective, randomized study comparing transvenous cryothermal and radiofrequency ablation in atrioventricular nodal re-entrant tachycardia. Eur Heart J. 2004;25(24):2232–2237. | ||
Zrenner B, Dong J, Schreieck J, et al. Transvenous cryoablation versus radiofrequency ablation of the slow pathway for the treatment of atrioventricular nodal re-entrant tachycardia: a prospective randomized pilot study. Eur Heart J. 2004;25(24):2226–2231. | ||
Schwagten B, Knops P, Janse P, et al. Long-term follow-up after catheter ablation for atrioventricular nodal reentrant tachycardia: a comparison of cryothermal and radiofrequency energy in a large series of patients. J Interv Card Electrophysiol. 2011;30:55–61. | ||
Opel A, Murray S, Kamath N, et al. Cryoablation versus radiofrequency ablation for treatment of atrioventricular nodal reentrant tachycardia: cryoablation with 6-mm-tip catheters is still less effective than radiofrequency ablation. Heart Rhythm. 2010;7:340–343. | ||
Collins KK, Dubin AM, Chiesa NA, Avasarala K, Van Hare GF. Cryoablation versus radiofrequency ablation for treatment of pediatric atrioventricular reentrant tachycardia: initial experience with 4-mm cryocatheter. Heart Rhythm. 2006;3:564–570. | ||
Akca F, Schwagten B, Theuns DA, Takens M, Musters P, Szili-Torok T. Safety and feasibility of single-catheter ablation using remote magnetic navigation for treatment of slow-fast atrioventricular nodal reentrant tachycardia compared to conventional ablation strategies. Acta Cardiol. 2013;68(6):559–567. | ||
Kerzner R, Sánchez JM, Osborn JL, et al. Radiofrequency ablation of atrioventricular nodal reentrant tachycardia using a novel magnetic guidance system compared with a conventional approach. Heart Rhythm 2006;3(3):261–267. | ||
Knight BP, Ebinger M, Oral H, et al. Diagnostic value of tachycardia features and pacing maneuvers during paroxysmal supraventricular tachycardia. J Am Coll Cardiol. 2000;36(2):574–582. | ||
Eckardt LL, Leal M, Hollis Z, Tanega J, Alberte C. Cryoablation for AVNRT: importance of ablation endpoint criteria. J Cardiovasc Electrophysiol. 2012;23(7):729–734. | ||
Ricard P, Latcu DG, Yaïci K, Zarqane N, Saoudi N. Slow pathway radiofrequency ablation in patients with AVNRT: junctional rhythm is less frequent during magnetic navigation ablation than with the conventional technique. Pacing Clin Electrophysiol. 2010;33(1):11–15. | ||
Wood MA, Orlov M, Ramaswamy K, Haffajee C, Ellenbogen K. Remote magnetic versus manual catheter navigation for ablation of supraventricular tachycardias: a randomized, multicenter trial. Pacing Clin Electrophysiol. 2008;31(10):1313–1321. | ||
Bauerfeind T, Akca F, Schwatgen B, et al. The magnetic navigation system allows safety and high efficacy for ablation of arrhythmias. Europace. 2011;13(7):1015–1021. | ||
Zhang YX, Lu CY, Xue Q, Li K, Yan W, Zhou SH. Radiofrequency catheter ablation of atrioventricular nodal reentrant tachycardia guided by magnetic navigation system: a prospective randomized comparison with conventional procedure. Chin Med J (Engl). 2012;125(1):16–20. | ||
Ernst S, Ouyang F, Linder C, et al. Initial experience with remote catheter ablation using a novel magnetic navigation system: magnetic remote catheter ablation. Circulation. 2004;109(12):1472–1475. | ||
Kim S-H, Oh Y-S, Kim D-H, et al. Long-term outcomes of remote magnetic navigation for ablation of supraventricular tachycardias. J Interv Card Electrophysiol. 2015;43(2):187–192. | ||
Thornton AS, Janse P, Theuns DAMJ, et al. Magnetic navigation in AV nodal re-entrant tachycardia study: early results of ablation with one- and three-magnet catheters. Europace. 2006;8(4):225–230. | ||
Shurrab M, Danon A, Crystal A, et al. Remote magnetic navigation for catheter ablation of atrioventricular nodal reentrant tachycardia: a systematic review and meta- analysis. Expert Rev Cardiovasc Ther. 2013;117(7):829–836. | ||
Hanninen M, Yeung-Lai-Wah N, Massel D, et al. Cryoablation versus RF ablation for AVNRT: a meta-analysis and systematic review. J Cardiovasc. Electrophysiol. 2013;24(12):1354–1360. | ||
Santangeli P, Proietti R, Di Biase L, Bai R, Natale A. Cryoablation versus radiofrequency ablation of atrioventricular nodal reentrant tachycardia. J Interv Card Electrophysiol. 2014;39(2):111–119. | ||
Muennig P, Bounthavong M. Cost-Effectiveness Analysis in Health. 3rd ed. San Francisco, CA: John Wiley; 2016. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.