")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
A Clinical Investigation of the Performance and Safety of Epaderm®, an Emollient Cream
Authors August S, Granier S, Tighe MP, Tbaily LW, Chowdhury S, Ahlbom H
Received 12 May 2021
Accepted for publication 2 July 2021
Published 16 July 2021 Volume 2021:14 Pages 909—920
DOI https://doi.org/10.2147/CCID.S316794
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Suzannah August, 1 Stephen Granier, 2 Mark P Tighe, 1 Lee W Tbaily, 1 Sabrina Chowdhury, 3 Henrik Ahlbom 3
1University Hospitals Dorset NHS Trust, Dorset, BH15 2JB, UK; 2Whiteladies Medical Group, Bristol, BS8 2PU, UK; 3Mölnlycke® Health Care, Gothenburg, 402 52, Sweden
Correspondence: Suzannah August Email [email protected]
Introduction: Emollients provide an occlusive barrier for dry and atopic skin, retain moisture, protect it from irritants, and form the basis of eczema treatment.
Methods and Analysis: A prospective interventional single arm study to evaluate the performance and safety of Epaderm® Cream, an emollient and cleanser containing 25% (w/w) paraffin and 5% (w/w) glycerine (thereafter, an emollient cream), in patients with dry skin conditions. The primary outcome measure was participant evaluation of skin moisturisation after treatment with an emollient cream for up to 4 weeks. Secondary outcome measures included: evaluation of skin softness using a questionnaire and of pruritus on a visual analogue scale (VAS); clinician assessment of xerosis using Overall Dry Skin (ODS) score and measurement of skin hydration using a non-invasive device (MoistureMeterEpiD, Delfin Technologies) at each visit. Sign test and Wilcoxon signed rank test were used to analyse changes from baseline.
Results: A total of 114 participants completed the study. 84.2% (80 out of 95) of participants or parents strongly agreed or agreed that the cream improved skin moisturisation at 4 weeks of treatment at the target area (p< 0.0001). 86.3% of participants agreed that skin softness improved after 4 weeks (p < 0.0001). ODS score improved from 2.1 (standard deviation (SD) 1.0) to 0.7 (SD 0.8) at 4 weeks. Skin hydration at the target area improved from 31.5 (SD 9.3) to 40.5 (SD 8.3) (p< 0.001) at 4 weeks. Mean skin itchiness reduced from 38.0 (SD 25.4) to 17.7 (SD 19.8) at 4 weeks (p< 0.0001). Ten (8.3%) adverse device events (ADEs) were reported.
Conclusion: The emollient cream was well tolerated and demonstrated significant improvements in patient-reported skin moisturisation and softness as well as in clinical measurement of xerosis and skin hydration across all age groups including infants. The emollient cream can be recommended for dry skin conditions including atopic dermatitis and psoriasis.
Keywords: emollient, Epaderm, dry skin, eczema, psoriasis, atopic dermatitis
Corrigendum for this paper has been published
Introduction and Objectives
In healthy skin, corneocytes and intercellular lipids (which form a lipid mixture of ceramides, fatty acids and cholesterol) make up the resilient lipid barrier which protects from the entry of pathogens, allergens and irritants and prevents water loss.1–3 Loss of integrity of the skin’s lipid barrier is a key factor in the development of dry skin conditions and the restoration of the barrier function is central in their management.2 In dry skin conditions, the skin’s barrier function may be impaired for a variety of reasons and there are several potential triggers for dry skin.1 Similarly to the permeability barrier, the antimicrobial skin barrier function may be compromised in dry skin conditions, notably, in atopic dermatitis, which could lead to colonisation by Staphylococcus aureus.4 Indeed, dry skin conditions have multiple causes, but common to many is the loss of skin barrier function often accompanied by genetic mutations, most commonly of the gene encoding filaggrin (FLG).5
There is a long history of the use of emollients as part of the management of dry skin conditions; they are available in various forms and aim to improve barrier function and to relieve dryness and pruritus.2 Emollients are moisturising agents which soften, moisturise and hydrate the skin. They provide an occlusive barrier for dry and atopic skin, retain moisture and protect it from irritants. Emollient therapy forms the basis of eczema treatment and guidelines recommend frequent, liberal use.6,7 Simple emollients form an occlusive layer of non-physiological lipid or oil, such as petrolatum or mineral oil, reducing water loss. Emollients may include additional ingredients such as humectants, physiological lipids and antipruritic agents. Humectants such as urea and glycerol attract and retain water in the skin. Physiological lipids such as ceramides, cholesterol and free fatty acids are believed to restore the intercellular lipid matrix.8 It is important, however, for clinicians to consider the individual nature of different skin types when choosing appropriate treatment options.
Clinical studies of the performance and safety of emollients help clinicians to determine the most suitable option for patients with dry skin conditions including atopic dermatitis and psoriasis.
Aim and Outcome Measures
The aim of this study was to confirm the performance and safety of Epaderm® Cream, an emollient and cleanser containing 25% (w/w) paraffin and 5% (w/w) glycerine (thereafter, an emollient cream), in participants with dry skin conditions, including eczema, psoriasis and other dry skin conditions requiring treatment with emollient, when used as intended in daily practice.
Primary Outcome Measure
Participant evaluation of skin moisturisation (hydration) after treatment with the emollient cream up to 4 weeks, using a questionnaire.
Secondary Outcome Measures
- Participant evaluation of skin softness after treatment at 2 and 4 weeks
- Researcher assessment using “Overall Dry Skin” (ODS) score,9 at 2 and 4 weeks
- Skin hydration using a non-invasive device, MoistureMeterEpiD, at 2 and 4 weeks
- Frequency and quantity of use of the emollient cream
- Comfort during treatment
- Time to onset of effect (moist and soft)
- Pruritus or skin itchiness using a visual analogue scale (VAS)
- Participant evaluation of overall effect
- Frequency of use of the emollient cream as a skin cleanser
- Concomitant and previous medication use and treatment
- Adverse Device Effects (ADEs)
Study Design
Prospective, observational, single-arm study of an Investigational Medical Device, the emollient cream, consisting of 25% (w/w) paraffin and 5% (w/w) glycerine, in participants ranging in age (infants (0 to 36 months old), children (3–18 years old), adults (˃18 years old)).
Methods and Analysis
Study Setting
Secondary care in Poole Hospital National Health Service (NHS) Foundation Trust and Primary care in three NHS general practices in Bristol.
Participants
Participants with eczema, psoriasis or other dry skin conditions who were considered suitable for treatment with emollient cream by the investigator. Full inclusion and exclusion criteria and the study protocol are available in the public domain (ClinicalTrials.gov: US National Library of Medicine).10
Recruitment
Participants were recruited by invitation to potential participants with dry skin conditions (eczema, psoriasis) identified by EMISWeb (primary care Electronic Patient Records) searches or by opportunistic identification in general practice or hospital dermatology clinics between 01 April 2019 and 25 October 2019.
The purpose of the study was explained to all participants and informed, written consent was obtained from all participants or parents of participants.
Intervention
The emollient cream, consisting of 25% (w/w) paraffin and 5% (w/w) glycerine. Patients were given advice about the importance of frequent and liberal use, backed up with a patient information leaflet on sufficient and safe use of the emollient.
Participants were asked to agree to use the study emollient frequently (at least twice daily) and liberally as their only emollient and soap substitute for the 4-week study period but could stop treatment if they were dissatisfied with the study emollient.
The amount of emollient use was determined by asking how many 500g containers of emollient cream were used over the 2- and 4-week period.
Participants were free to use other treatments such as topical steroids as usual but not to use other emollients.
Schedule of Assessment
Data was collected for each participant over a 4-week treatment period, with a visit at baseline (visit 1, day 0), at 2 weeks (visit 2, day 14) and at 4 weeks (visit 3, day 28) treatment. An evaluable participant was a participant with a baseline visit and at least one follow-up visit. Collected data was entered into an electronic Case Report Form (eCRF) using Viedoc™.
Participants were instructed not to shower or put on the emollient cream before the follow-up visits.
Information was collected on age, sex and relevant medical history at the initial visit; at 2 weeks and 4 weeks, information was collected on concomitant relevant treatment, skin disease/condition and severity. A target affected area was chosen by the investigators as an area of skin representative of the participants’ overall skin condition, ie, not the most or least affected area.
Clinician assessment of xerosis was carried out using ODS score following guidelines on the European Group on Efficacy Measurement of Cosmetics and Other Topical Products,9 where absent skin dryness = 0; faint scaling = 1; small scales = 2; small and larger scales = 3; large scales = 4.
Skin hydration was assessed by clinicians using MoistureMeterEpiD (Delfin Technologies), a device which non-invasively measured local percentage water content (0% to 100%) in the epidermis. The device was placed on the target affected area and the percentage water content was shown on the display.
Participant evaluation of skin moisturisation and softness was assessed using 5-point questionnaires and participant evaluation of pruritus was assessed using a visual analogue scale (VAS). Data were also collected on the quantity and frequency of emollient applied and ADEs.
Statistical Methods
Sign test was used to analyse change from baseline in ordered categorical and dichotomous variables and Wilcoxon signed rank test for changes in continuous variables. Analyses were based on the intention-to-treat population and confirmed by the per protocol population. All tests were two-sided with a significance level of 0.05.
The sample size calculation was based on that the investigation was looking at performance of the emollient cream measured as improved moisturisation evaluated by the participant. Assuming a power of 80% and using a sign test, a total of approximately 40 participants were needed in each subgroup: infants (0–36 months), children (3–18 years) and adults (˃18 years old).
Ethics
The investigation was performed in accordance with the ethical principles that have their origin in the Declaration of Helsinki and applicable regulatory requirements.
The study received a favorable ethical opinion from the London Riverside Research Ethics Committee and the Health Research Authority (IRAS ID: 251156). ISO 14155:2011 was followed in addition to national regulations. The study was registered at the public database ClinicalTrials.gov Identifier: NCT03738163.
Participants were free to discontinue participation from the investigation at any time, and without prejudice to further treatment. Participants were categorised as lost to follow-up when the investigation staff had performed at least one documented attempt to reach the participant, after the baseline visit.
Results
Of the 121 enrolled participants, 114 completed the study; six withdrew before the second visit so follow-up data were not available for analysis; one participant withdrew later (all seven participants withdrew for non-device-related reasons). Primary outcome data were available for 107 and 95 participants at 2 weeks and 4 weeks, respectively.
Table 1 shows participant demographics and baseline diagnoses, distribution and severity. 33 (29%) were infants ≤36 months, 40 (35%) were children from 3 to 18 years and 41 (36%) were adults (>18 years). The majority (88; 76%) had a diagnosis of atopic dermatitis or eczema, 7 (6%) psoriasis and 21 (18%) had other dry skin conditions that the investigator considered to require emollient therapy.
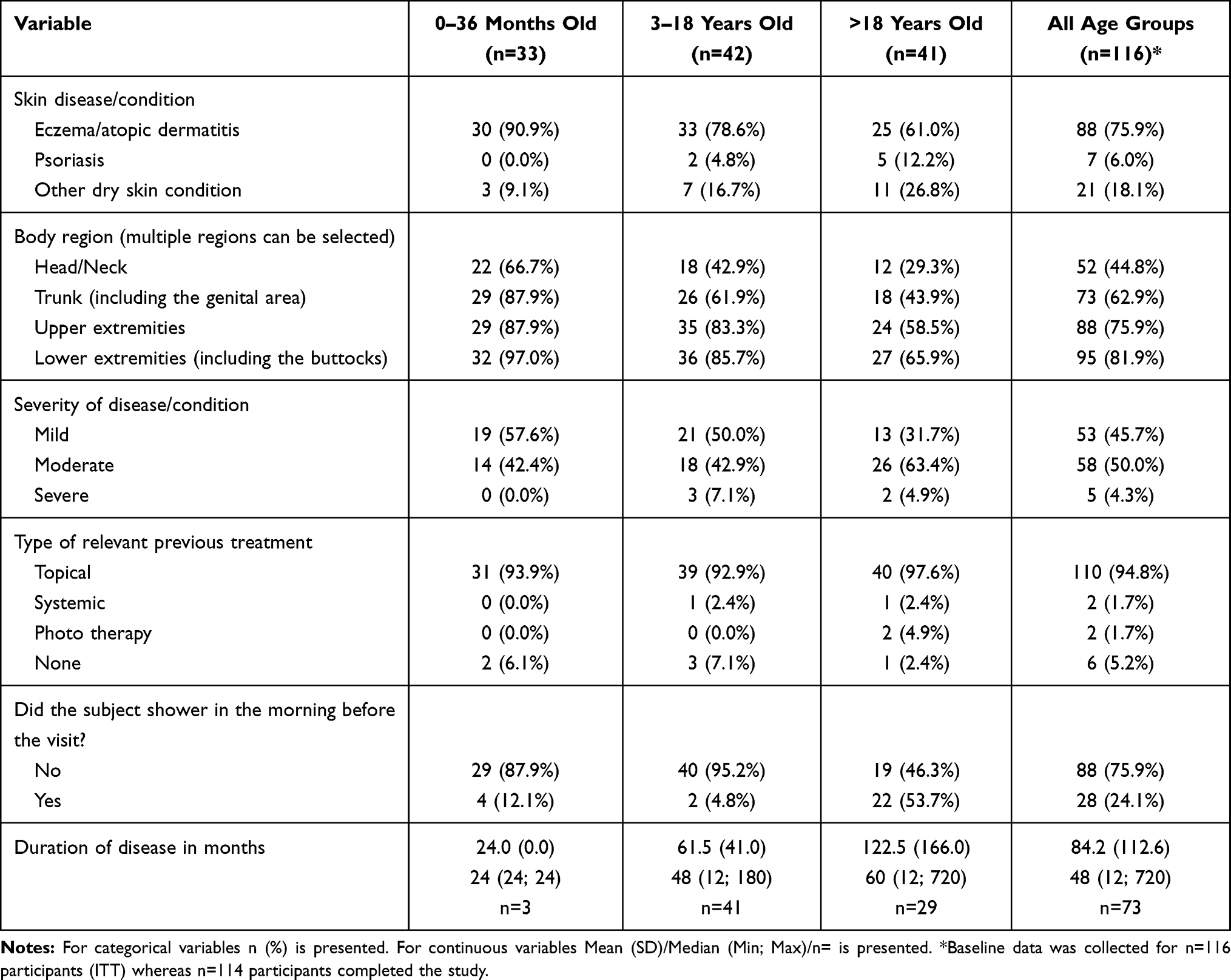 |
Table 1 Demographics and Baseline Values (ITT) |
82.2% and 88.4% of participants reported applying the emollient cream at least every day at 2 and 4 weeks, respectively. The most common frequency of application was twice daily as reported by 58.9% of participants at 4 weeks. The emollient cream was used as a skin cleanser in 64.2% and 76.9% of all participants and children ≤3 years, respectively.
Primary Outcome
The primary outcome was the patient’s or parent’s self-reported evaluation of skin moisturisation at up to 4 weeks after using the emollient cream.
77.6% (83/107) and 84.2% (80/95) of participants strongly agreed or agreed that skin moisturisation had improved after 2 and 4 weeks of treatment at the target area and this was represented across all age groups (Table 2). This change from baseline was statistically significant for all participants as well as for each age group at 2 (p<0.0001) and 4 weeks (p<0.0001).
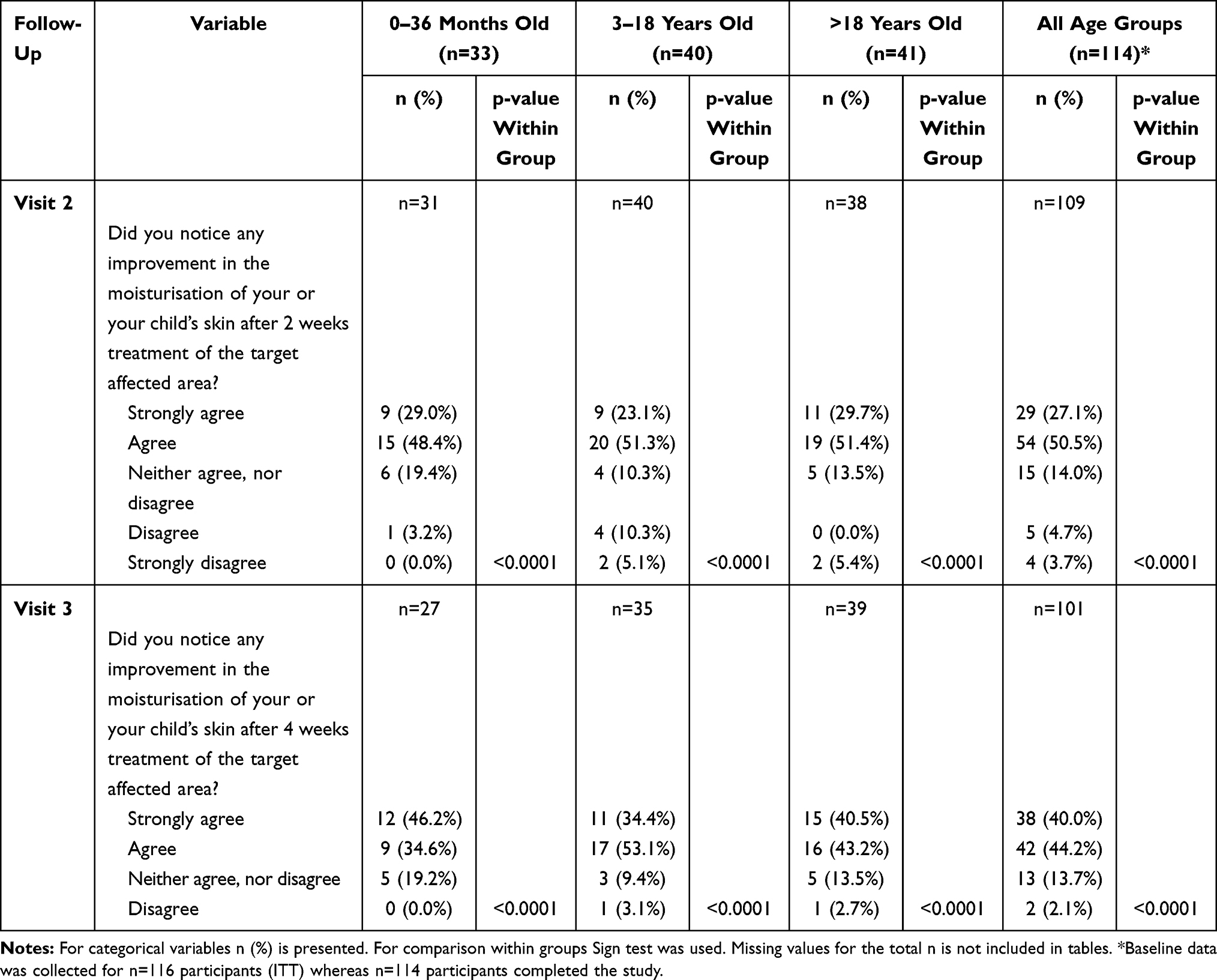 |
Table 2 Primary Endpoint: Skin Moisturisation (ITT) |
Secondary Outcomes
86.3% of participants strongly agreed or agreed that skin softness improved after 4 weeks of treatment located at the target affected area (p<0.0001) and this change was reported in all age groups (p<0.0001) (Table 3).
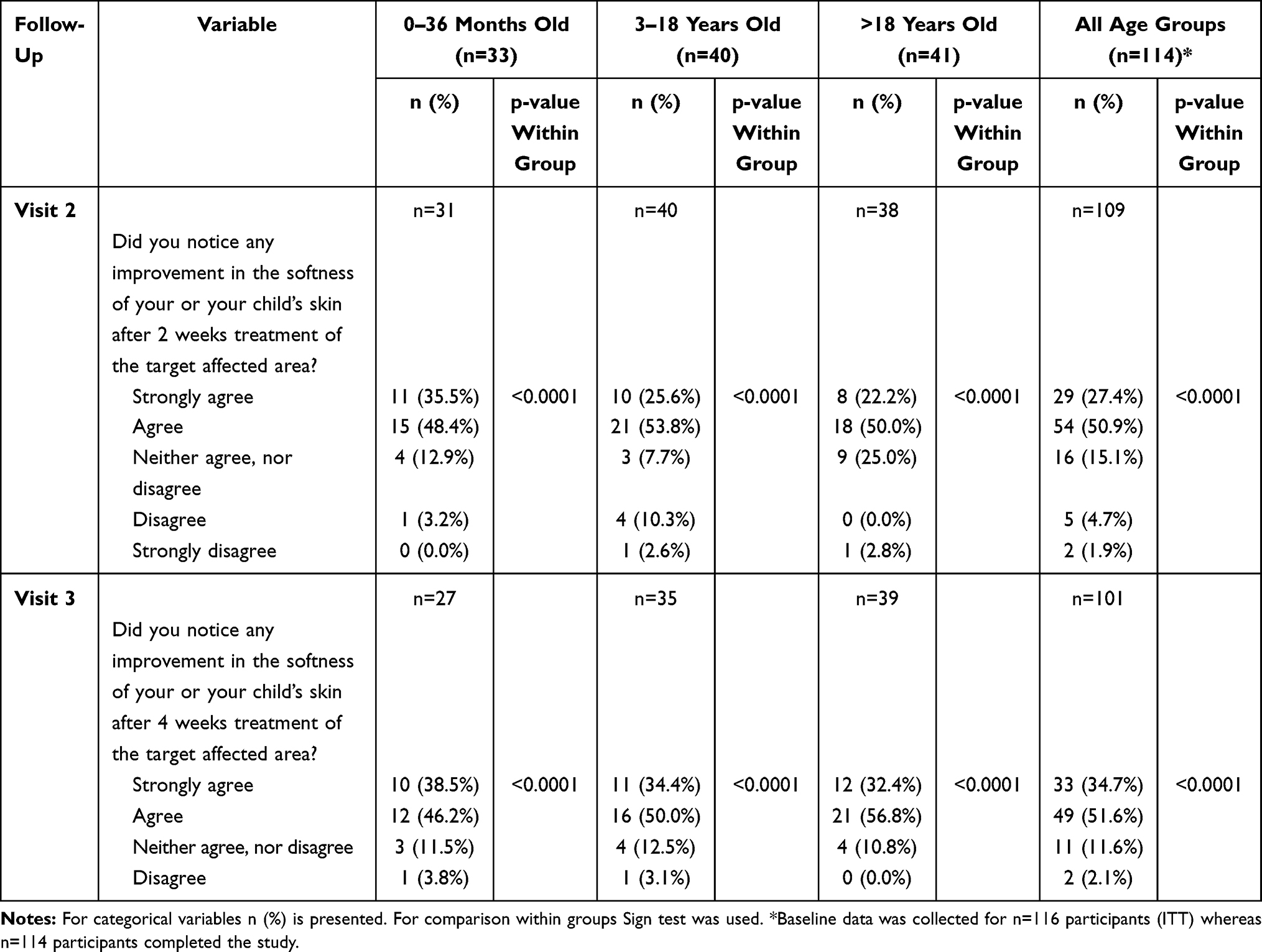 |
Table 3 Secondary Endpoints: Skin Softness (ITT) |
Clinician evaluation using ODS score changed from 2.1 (SD 1.0) to 1.2 (SD 1.1) and 0.7 (SD 0.8) at 2 and 4 weeks respectively (p<0.0001) (Table 4). Xerosis at the target affected area was evaluated by clinicians at the baseline visit and was evenly distributed between the following categories: faint scaling, faint roughness and dull appearance; small scales in combination with a few larger scales, slight roughness, whitish appearance; and small and larger scales uniformly distributed, definite roughness, slight redness and possibly few superficial cracks. A total of nine participants displayed dominating large scales, advanced roughness, redness, eczematous changes and cracks at the baseline visit. Improvement of scales or lesions occurred during the subsequent follow-up visits whereby the number of lesions decreased to 2 at week 2 and no lesions were present after 4 weeks of the emollient cream application. 29.5% (n=31) of the participants had no lesions at the second follow-up visit compared to 2% at baseline. Further skin improvement was confirmed by the absence of lesions in 50.5% (n=47) of all participants after 4 weeks of the emollient cream application (Table 5).
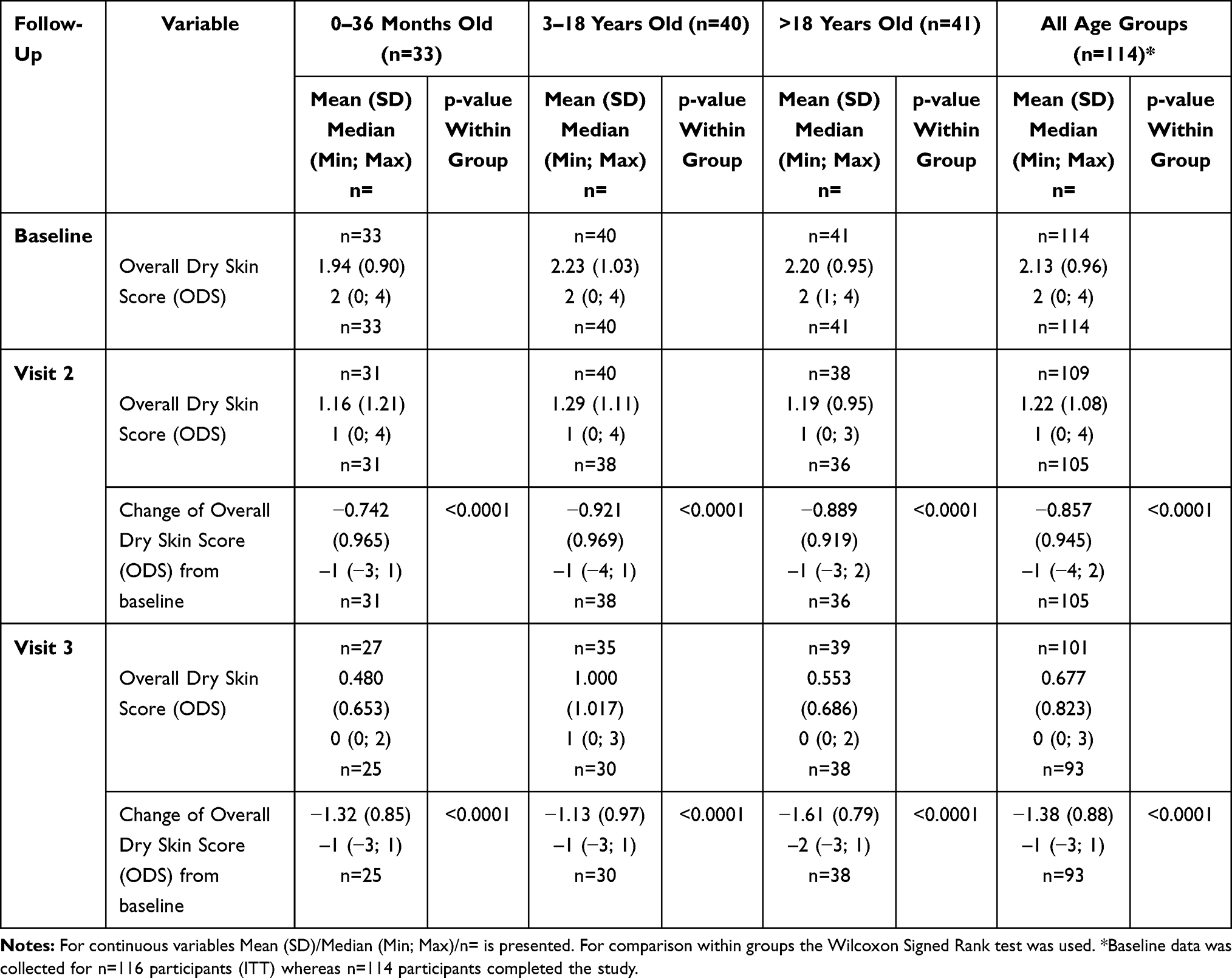 |
Table 4 Secondary Endpoints: Overall Dry Skin Score (ITT) |
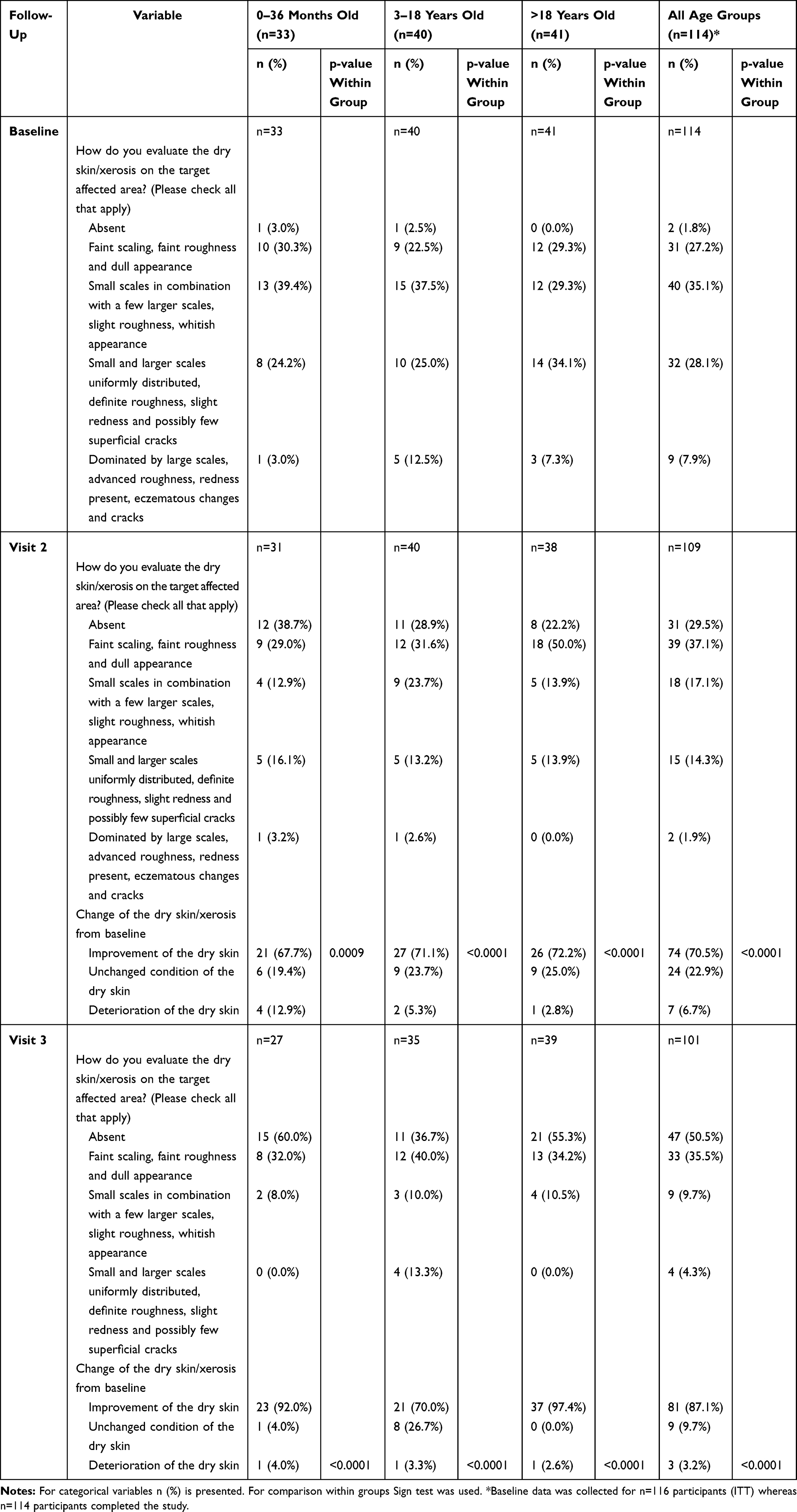 |
Table 5 Secondary Endpoints: Evaluation of Dry Skin/Xerosis (ITT) |
Skin hydration at the target area, measured using a Moisture Meter EpiD, improved from 31.5 (SD 9.3) to 38.6 (SD 11.2) (p<0.001) and 40.5 (SD 8.3) (p<0.001) at 2 and 4 weeks, respectively, in all participants. Similar statistically significant improvements were found in all three age groups (Table 6).
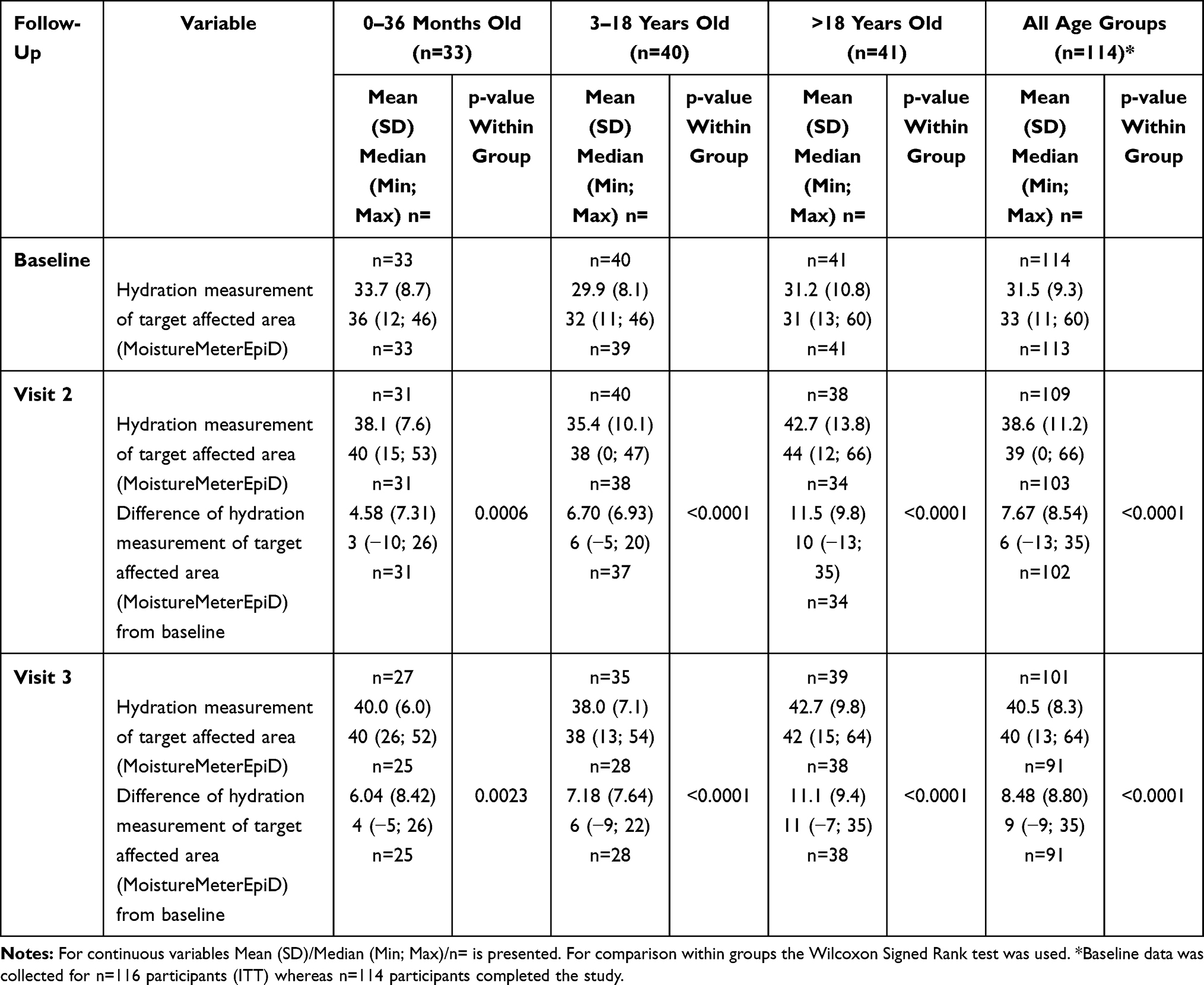 |
Table 6 Secondary Endpoints: Hydration Measurement of Target Affected Area (ITT) |
Mean skin itchiness measured on a 100-point VAS reduced from 38.0 (SD 25.4) to 25.1 (SD 23.4) (p<0.0001) and 17.7 (SD 19.8) (p<0.0001) in all participants at 2 and 4 weeks respectively (Table 7).
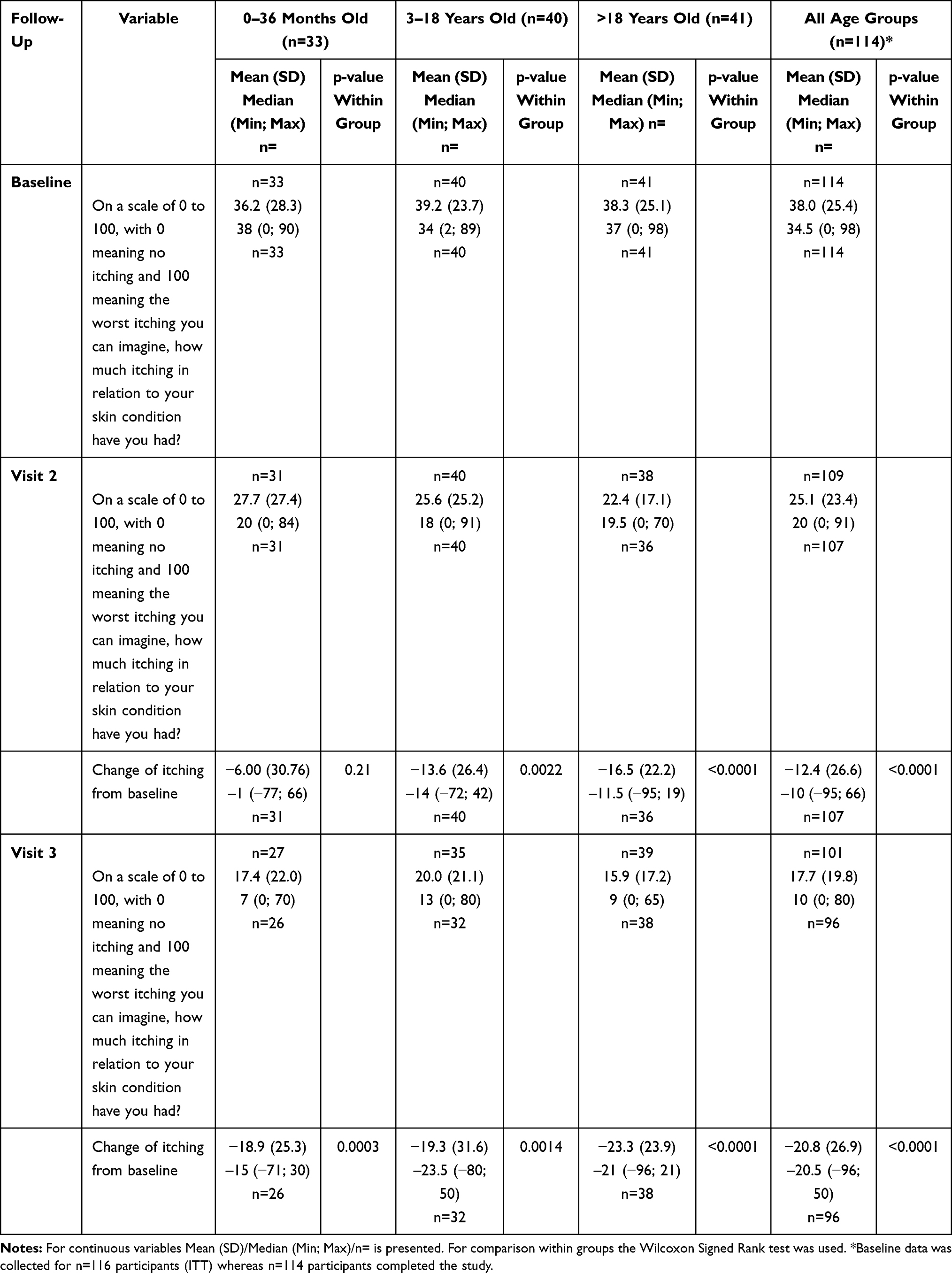 |
Table 7 Secondary Endpoints: Amount of Itching (ITT) |
Participants were asked about the time to improvement of skin moisturisation or softness and 71.0% reported improvement within 2 weeks at visit 2% and 5.3% reported no improvement at all at visit 3.
The overall effect of the emollient cream was rated good to excellent in 83.2% of all participants and 88.5% of children ≤3 years.
90.9% of participants reported no further flares of their skin condition during the 4-week study period.
Ten ADEs were recorded in 10 participants (8.3% out of 121 enrolled participants); 3 in infants ≤3 years, 4 in children aged 3–18 years and 3 in the adult group. All ADEs were related to an inflammatory rash or hypersensitivity reaction. During the study, no serious adverse events (SAEs) in relation to the investigational device were reported. One device deficiency was reported where the participant did not attend the follow-up visits due to an intermittent rash which subsequently self-resolved.
Discussion
Clinicians have a large range of emollients to choose from when treating patients with dry skin conditions. It is not clear whether any emollients are superior to others. In their 2017 review, which included an evaluation of clinical studies ranging from those comparing an investigational product with a placebo to comparisons with no treatment, van Zuuren et al concluded that participants found investigational products to be more effective in reducing eczema and symptoms of itch compared to control. While most moisturisers showed some beneficial effects, there was generally no evidence that one moisturiser is superior to another.11
Hon et al (2018) reviewed current classes of emollients in the market and their clinical efficacy in atopic dermatitis. Clinical data included studies relating to plant-derived products (such as coconut oil and aloe vera), animal products (such as lanolin and horse oil) and emollients with special additives such as ceramides, ectoin or antimicrobial peptides. The authors emphasised an importance of an appropriate emollient for patients with atopic dermatitis which may significantly improve compliance with emollient treatment.12
In this study, the emollient cream was found to be well tolerated and showed improvements in patient-reported skin moisturisation and softness, clinical measurements of xerosis and skin hydration in participants with dry skin conditions, including children and infants. Improvements were observed after 2 weeks of treatment. The participants’ assessments of the strong positive effect of the emollient cream on their skin condition were confirmed by the subjective clinicians’ evaluation and use of an objective tool, MoistureMeter EpiD.
The broad eligibility criteria allowed for “real world” data to be captured, representative of real life dermatological practice in both primary care and in a hospital setting.
This was a single arm study so outcomes could be a result of reversion to the mean. However, most participants were recruited by invitation because they had a record of a dry skin condition and there is no indication that many were experiencing flares of their condition at the time of assessment. It is possible that the clinical intervention to encourage frequent and liberal use of the cream may have had an important impact on the observed benefits of this treatment, although this should be standard practice in advising patients with dry skin conditions. Other specific study interventions such as the use of a MoistureMeter EpiD and the frequency of follow-up may have improved concordance with the treatment recommendations.
The study was carried out in one secondary care hospital and three urban general practices. It is possible that these study populations may not be representative of all populations, including patients from different socio-economic, educational and ethnic backgrounds. A relatively small number of participants were enrolled in the psoriasis cohort and it is possible that the performance of the cream may vary depending on the underlying skin condition.
Skin hydration and clinical assessment of xerosis were assessed on a single target area and these may have been different if measured on a more or lesser affected area.
Conclusions
The study showed that the emollient cream was well tolerated and demonstrated significant improvements in patient-reported skin moisturisation and softness as well as in clinical measurement of xerosis and skin hydration across all age groups, including infants, when applied liberally as often as required. Based on the data, the emollient cream can be recommended as part of the management regime of dry skin conditions including atopic dermatitis and psoriasis in children and adults.
Data Sharing Statement
The authors do not intend to share any individual deidentified participant data in this manuscript.
Acknowledgments
We would like to thank all the participants, administrative staff and clinicians who contributed to this study.
Funding
Mölnlycke® Health Care AB was the study sponsor and funded the research.
Disclosure
Dr Stephen Granier reports payment to practice (Whiteladies Medical Group) for conducting research studies from NIHR approved non-commercial and commercial research. Whiteladies Medical Group is a shareholder of these GP-based federations for One Care and GP Care Bristol, Whiteladies Medical Group also receives notional rent and rental income from Hobb & Butts Pharmacy. He is the director of SJG Medical Ltd providing healthcare consultancy to companies including AXA Health and Healthwest PCN collaboration of practices, consultancy fees from Public Health England. In addition, Dr Granier also holds pension and ISA investments in tracker funds (UK, US and global) that have holdings in pharmaceutical and biomedical companies and direct investments in Alphabet and Amazon shares, outside the submitted work; and he is a member of the RCGP Overdiagnosis Group. The authors report no other conflicts of interest in this work.
References
1. Andriessen A. Prevention, recognition and treatment of dry skin conditions. Br J Nurs. 2013;22(1):26–30. doi:10.12968/bjon.2013.22.1.26
2. Holden C, English J, Hoare C, et al. Advised best practice for the use of emollients in eczema and other dry skin conditions. J Dermatolog Treat. 2002;13(3):103–106. doi:10.1080/09546630260199442
3. Cork M. The importance of skin barrier function. J Dermatolog Treat. 1997;8(sup1):S7–S13. doi:10.3109/09546639709160948
4. Elias P, Schmuth M. Abnormal skin barrier in the etiopathogenesis of atopic dermatitis. Curr Opin Allergy Clin Immunol. 2009;9(5):437–446. doi:10.1097/ACI.0b013e32832e7d36
5. Irvine A, McLean W, Leung D. Filaggrin mutations associated with skin and allergic diseases. N Engl J Med. 2011;365(14):1315–1327. doi:10.1056/NEJMra1011040
6. NICE. Clinical guideline 57. Atopic eczema in under 12s: diagnosis and management; 2007. Available from: https://wwwniceorguk/guidance/cg57/chapter/1-Guidance#treatment.
7. Primary Care Dermatology Society. Atopic eczema; 2016. Available from: https://www.pcds.org.uk/clinical-guidance/atopic-eczema.
8. Moncrieff G, Cork M, Lawton S, Kokiet S, Daly C, Clark C. Use of emollients in dry-skin conditions: consensus statement. Clin Exp Dermatol. 2013;38(3):231–238. doi:10.1111/ced.12104
9. Serup J. EEMCO guidance for the assessment of dry skin (xerosis) and ichthyosis: clinical scoring systems. Skin Res Technol. 1995;1(3):109–114. doi:10.1111/j.1600-0846.1995.tb00029.x
10. Mölnlycke Health Care AB. A prospective post market clinical follow-up investigation with Epaderm® cream to confirm performance and safety parameters. Available from: https://clinicaltrials.gov/ct2/show/NCT03738163. Identifier: NCT03738163.
11. van Zuuren E, Fedorowicz Z, Christensen R, Lavrijsen A, Arents B. Emollients and moisturisers for eczema. Cochrane Database Syst Rev. 2017;2(2). doi:10.1002/14651858.CD012119.pub2
12. Hon K, Kung J, Ng W, Leung T. Emollient treatment of atopic dermatitis: latest evidence and clinical considerations. Drugs Context. 2018;7:212530. doi:10.7573/dic.212530
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.