")
Back to Journals » International Journal of General Medicine » Volume 13
A Case of Ileosigmoid Knotting in a Ghanaian Patient
Authors Li X , Zakariah SM, Shi Y
Received 23 September 2020
Accepted for publication 9 November 2020
Published 25 November 2020 Volume 2020:13 Pages 1265—1269
DOI https://doi.org/10.2147/IJGM.S279870
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Xuguang Li,1,2 Seidu Mohamadu Zakariah,2 Yongyong Shi2,3
1Department of Abdominal Surgery, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong Province, People’s Republic of China; 2Surgical Department, Lekma Hospital, Accra, Ghana; 3Department of Anesthesia, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong Province, People’s Republic of China
Correspondence: Yongyong Shi
Department of Anesthesia, The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, No. 111 Dade Road, Guangzhou, Guangdong Province, People’s Republic of China
Tel +86-13926088958
Fax +86-20-39318521
Email [email protected]
Abstract: Ileosigmoid knotting is a rare condition in which a compound volvulus causes acute intestinal obstruction. In this process, the terminal ileum wraps around the base of the mesosigmoid and sigmoid colon, forming a knot. This condition tends to rapidly progress to gangrene of both the ileum and sigmoid colon; hence, the mainstay of treatment is timely emergency surgery. In this report, we describe the case of a 20-year-old Ghanaian female patient and discuss the available surgical options regarding ileosigmoid knotting.
Keywords: ileosigmoid knotting, compound volvulus, intestinal obstruction
Introduction
Parker was the first to report ileosigmoid knotting in medical literature in 1845.1 In two separate case series, the condition was linked to populations who eat a single meal a day.2,3 The incidence of ileosigmoid knotting tends to be much higher in developing countries and among lower socioeconomic strata than in the white population.4–7 Furthermore, it occurs more commonly above the age of 40 and is approximately 4-times greater in men (80.2%) than in women.8 The mortality rate is very high in this rare but potentially fatal condition which progresses rapidly and frequently to gangrene of both the ileum and sigmoid colon, which triggers general peritonitis and septic shock.8 Due to the limitation of doctors’ experience with this condition, patients should undergo immediate surgical intervention due to speedily worsening gangrene of both the ileum and sigmoid colon. Generalized peritonitis and sepsis are the main cause of poor outcome.1,3 Application of well-known guidelines similar to the “Surviving Sepsis” treatment protocol to the resuscitation algorithm, along with prompt surgical intervention, has been demonstrated to improve survival.1,9,10
Case Report
A 20-year-old Ghanaian female peasant presented with a history of abdominal pain and absolute constipation for 5 days. She began to experience a sudden cramping pain on the hypogastrium after having a bulky meal. The pain was scored as 4 on a 10-point scale at first and other symptoms included abdominal distention, failure to pass either stool or flatus, but no vomiting or fever. Abdominal pain had intensified to 10 points and progressed to persistent and diffuse after 4 days of moderate abdominal pain. Nothing was able to relieve the pain and she was even unable to stand up either when she came to our hospital. Her usual state of health was well and she had no history of chronic disease, congenital disease, or infectious disease. She denied having any past medical or surgical history. The BMI was 16.95. She had regular menses and no history of pregnancy or childbirth.
Examination revealed severe dehydration, a pulse rate of 112 beats/min, a BP of 120/70 mmHg, and a temperature of 37.2°C. Abdominal examination revealed diffuse abdominal distension, tenderness, rebound tenderness, guarding, and absence of bowel sounds. A digital rectal examination revealed an empty rectum. Laboratory studies showed that the concentration of hemoglobin was 9.7 g/dL and of white blood cells was 21.15*10^9/L. Urine pregnancy test was negative. An ultrasound of the abdomen showed a dilated fluid-filled hypoperistaltic bowel, suggestive of small bowel obstruction. A supine abdominal radiograph showed a large gas-filled dilated bowel loop in the left mid and lower quadrants. The intestinal pneumatosis can also be seen in the upper and right lower abdomen (Figure 1). Lekma hospital has no CT or MRI scanners. A working diagnosis of intestinal obstruction with possible strangulation and peritonitis was made.
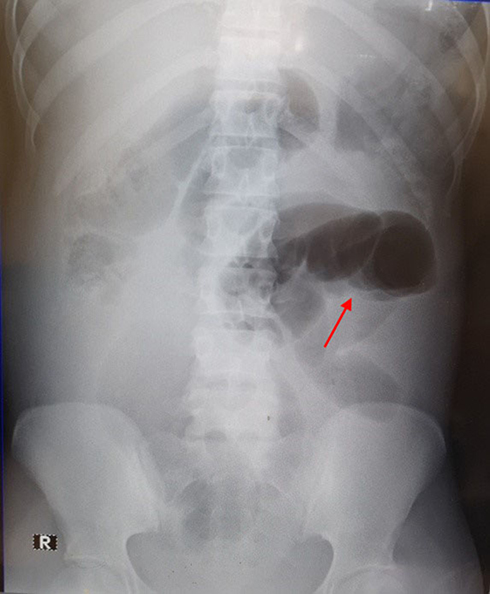 |
Figure 1 Supine abdominal radiograph showed a large gas-filled dilated bowel loop in the left mid and lower quadrants. The intestinal pneumatosis (arrow) can also be seen in the upper and right lower abdomen. |
After aggressive resuscitation, an exploratory laparotomy was performed. The peritoneal cavity contained about one and a half litres of foul smelling hemorrhagic fluid. The terminal ileum had encircled the base of the mesosigmoid and sigmoid colon with a 360° clockwise twist, strangulating it (Figure 2). The mesentery of the ileum was also twisted around along with the ileum, resulting in gangrene of the distal three feet of the ileum up to the ileocaecal junction, which belongs to Type I of ileosigmoid knotting.2,3,6 The sigmoid colon was gently untwisted and the ileal knot opened. One-meter long non-viable distal ileum and sigmoid colon were resected. Colorectal (descending colon) anastomosis and ileostomy procedure (blind terminal ileum which is just 2 cm away from ileocaecal valve) were performed (Figure 3). An abdominal drain tube was placed in the pelvic cavity. Fortunately, she still had a one and a half meters long segment of viable small intestine. After 24 hours, the passage of stool and flatus were through the stoma and oral feeding was initiated. Drainage was removed after 72 hours. The postoperative course was uneventful and she was discharged after 10 days. Finally, the patient returned for a reversal of the ileostomy after 6 weeks, which was aslso uneventful.
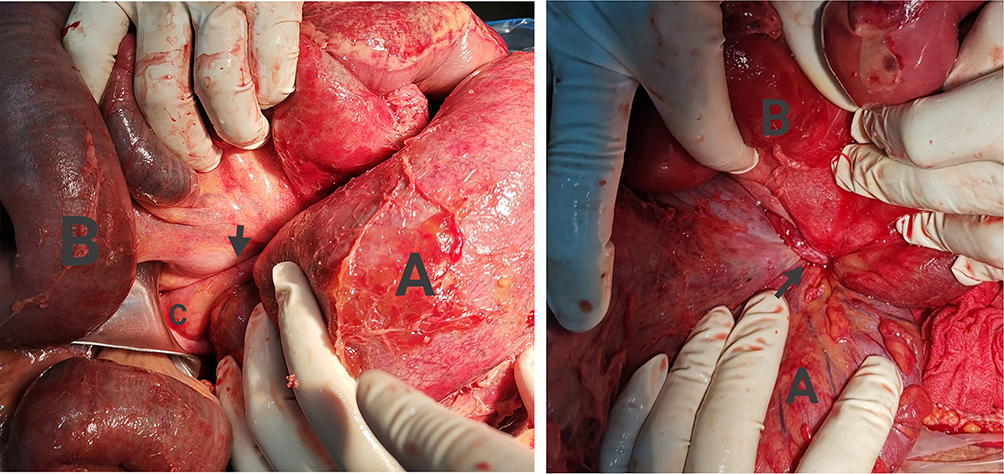 |
Figure 2 Intraoperative photographs show (A) gangrenous sigmoid colon, (B) gangrenous ileum loop and (C) cecum. Arrow: terminal ileum. |
 |
Figure 3 Postoperative photograph shows the surgical specimen (A: gangrenous sigmoid colon; B: gangrenous ileum loop). |
Discussion
The cardinal symptom of ileosigmoid knotting is abdominal pain, which is characteristically sudden in onset, usually accompanied by vomiting and abdominal distension, and which quickly intensifies in severity until it reaches a state of constant ache. Patients may present in hypovolemic shock, as this occurs early in the disease process. Findings often present on examination of the abdomen are distension, generalized tenderness, and guarding, with bowel sounds often diminished or absent. Plain supine and erect radiographs show a wide, dilated sigmoid colon, and fluid levels in the small intestine. Preoperative diagnosis is difficult as clinical and X-ray features are not specific to ileosigmoid knotting and occur in other conditions that cause generalized peritonitis.1,2 Factors that can lead to ileosigmoid knotting include: 1) Long sigmoid colon on a narrow pedicle; 2) Long small intestinal mesentery and freely mobile ileum; and 3) Intake of high bulky diet with an empty small intestine.1–3,5,6,11,12 When a semi-liquid bulky meal progresses into the proximal jejunum, it increases the mobility of the small intestine and the heavier segments of the proximal jejunum fall into the left lower quadrant. The empty loops of ileum and distal jejunum twist in a clockwise rotation and wrap around the base of a narrow sigmoid colon. With increasing peristalsis, the intertwisting of the two parts of the intestine occurs, leading to a vicious torsion giving rise to compression and a double loop obstruction. Strangulation and gangrene of the ileum and sigmoid colon occur rapidly due to the tightness of the knot and involvement of the mesentery.1–3,11–14 These processes distinctly explain why ileosigmoid knotting appears to have a higher chance to occur among populations who eat one meal a day, such as people in Uganda and Muslims during the Ramadan fast. When this condition occurs, both the sigmoid colon and the loops of ileum become distended.2 The sigmoid colon becomes markedly distended with air and fluid.14 As a result of strangulation, the loops of ileum become congested and infarction ensues. Then the ileal gangrene may extend to the terminal ileum, occasionally involving the cecum. The types of ileosigmoid knotting have been described:2,3,6 Type I: the ileum (active component) wraps itself around the sigmoid colon (passive component) in a clockwise or anticlockwise direction. Type II: the sigmoid colon acts as the active component. Type III: the ileocecal segment wraps itself around the sigmoid colon. Type I is the most common. Ileosigmoid knotting is a rare but lethal condition, yet it is difficult to diagnose because of its infrequent morbidity, atypical symptomatic features of the disease, and non-specific abdominal radiographic findings. This condition is diagnosed preoperatively in less than 20% of the patients1–3,11–20 because its clinical features, such as abdominal pain, distention, vomiting, constipation, and the radiographic findings, are common in bowel obstruction.1,3,15
To some extent, an abdominal/pelvic computed tomography (CT) scan will show the whirl sign which is due to the twisted intestine and sigmoid mesocolon, with the medial deviated cecum and descending colon,8,21 however this investigation is not suitable for patients who are hemodynamically unstable and those admitted at a hospital without this facility in Africa. What is more, the mortality figures are generally related to the duration of symptoms, the presence or absence of gangrene, and general status of the patient, including the presence of septic shock,2,3,6 and the outcome may depend on the time of presentation and intervention.22 Diagnostic laparotomy is ideally suitable for patients with ileosigmoid knot as a means of improving diagnostic accuracy, reducing the risks of general peritonitis and septic shock. In our case, since the patient had features of generalized peritonitis and hemodynamic instability, we performed an urgent emergency laparotomy after aggressive fluid resuscitation.
In most cases, gangrenous bowel was encountered, whereas in rare cases both small and large bowels were assessed to be viable in surgery.6 The core essence of the surgery to ileosigmoid knotting is obstruction relief, resection of the necrotic bowel loops, and excision of redundant sigmoid colon to remove the induced factors. Therefore, the following surgical procedures are available according to the intraoperative situation:22 1) Ileum Derotation + Sigmoidectomy + Colostomy; 2) Ileum Derotation + Sigmoidectomy + Colorectostomy; 3) Ileectomy + Enteroenterostomy + Sigmoidectomy + Colostomy; 4) Ileectomy + Enteroenterostomy + Sigmoidectomy + Colorectostomy; and 5) Ileectomy + End Ileostomy + Sigmoidectomy + Colorectostomy. Of the above-mentioned procedures, the most commonly performed one was Ileectomy + Enteroenterostomy + Sigmoidectomy + Colostomy. The rates of both gangrene and mortality are still very high in spite of early suspicion and prompt surgical intervention. Recurrent volvulus or repeat knotting from redundancy of the loop may cause gangrene after surgery. Therefore, if the small intestine is viable, resection is not indicated; but if the sigmoid colon is viable, resection should still be performed to decrease the risk of recurrence.23
In our case, both sigmoid and the terminal ileum were gangrenous. After ileal resection, we found that the stump was only 2 cm from the ileocaecal junction. Under the circumstances, enteroenterostomy should be avoided because the short distance to ileocecal valve increased the pressure of stomas. Enterocolonostomy was not a safer option either, because both intestinal wall edema and severe septic condition are risk factors to anastomotic leakage. However, an ileostomy contributes to decreasing the pressure of intestine, excluding residues to the colon and avoiding a colostomy. Therefore, we performed Ileectomy + End Ileostomy + Sigmoidectomy + Colorectostomy in this case. Avoiding a colostomy is always welcome, as it reduces the morbidity, because reversing enterostomy is much easier and safer than reversing colostomy.6,11 As enterostomy was the case in our patient, primary colorectal anastomosis was acceptable.15 The surgical procedure ultimately should be determined by the local expertise available and decided on a patient-by-patient basis.
Conclusion
Ileosigmoid knotting is an uncommon cause of acute intestinal obstruction where the ileum wraps around the base of the redundant sigmoid colon and mesosigmoid. Better understanding of this condition, more timely surgical intervention after aggressive fluid resuscitation, and a more effective operative procedure including resection of gangrenous bowel with or without primary anastomosis have optimized the survival of the patients who have suffered from ileosigmoid knotting. We share our experience and the available surgical options in Ghana for improving other doctors’ recognition of this condition.
Ethics and Consent Statement
Institutional ethical approval is not required to publish the case reports. Written informed consent was obtained from the study participant for the case details and associated images publication.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Puthu D, Rajan N, Shenoy GM, Pai SU. The ileosigmoid knot. Dis Colon Rectum. 1991;34(2):161–166. doi:10.1007/BF02049992
2. Shepherd JJ. Ninety-two cases of ileosigmoid knotting in Uganda. Br J Surg. 1967;54(6):561–566. doi:10.1002/bjs.1800540615
3. Alver O, Oren D, Tireli M, et al. Ileosigmoid knotting in Turkey. Review of 68 cases. Dis Colon Rectum. 2014;99(12):1139–1147. doi:10.1007/BF02052263
4. Hashimoto T, Yamaguchi J, Fujioka H, et al. Two cases of ileosigmoid knot: the youngest reported patient and CT findings. Hepatogastroenterology. 2004;51:771–773.
5. Miller BJ, Borrowdale RC. Ileosigmoid knotting: a case report and review. Aust N Z J Surg. 1992;62(5):402–404. doi:10.1111/j.1445-2197.1992.tb07213.x
6. Atamanalp SS, Oren D, Başoğlu M, et al. Ileosigmoidal knotting: outcome in 63 patients. Dis Colon Rectum. 2004;47(6):906–910. doi:10.1007/s10350-004-0528-9
7. Fouquet V, Berrebi D, De Lagausie P, et al. Ileosigmoid knotting in a child. The first case report in a French girl. Gastroenterol Clin Biol. 2006;30(12):1414–1416. doi:10.1016/S0399-8320(06)73574-6
8. Machado NO. Ileosigmoid knot: a case report and literature review of 280 cases. Ann Saudi Med. 2009;29(5):402–406. doi:10.4103/0256-4947.55173
9. Mallick IH, Winslet MC. Ileosigmoid knotting. Colorectal Dis. 2004;6(4):220–225. doi:10.1111/j.1463-1318.2004.00361.x
10. Chakma SM, Singh RL, Parmekar MV, et al. Ileosigmoid knot - a surgeon’s nightmare. J Clin Diagn Res. 2013;7:2986–2987.
11. Akgun Y. Management of ileosigmoid knotting. Br J Surg. 1997;84:672–673.
12. Kakar A, Bhatnagar BN. Ileo-sigmoid knotting: a clinical study of 11 cases. Aust N Z J Surg. 1981;51(5):456–458. doi:10.1111/j.1445-2197.1981.tb05984.x
13. Roy M, Roy S. Ileosigmoid knot. J Indian Med Assoc. 1973;60:50–53.
14. Young WS, White A, Grave GF. The radiology of ileosigmoid knot. Clin Radiol. 1978;29(2):211–216. doi:10.1016/S0009-9260(78)80241-4
15. Raveenthiran V. The ileosigmoid knot: new observations and changing trends. Dis Colon Rectum. 2001;44(8):1196–1200. doi:10.1007/BF02234644
16. Gibney EJ, Mock CN. Ileosigmoid knotting. Dis Colon Rectum. 1993;36(9):855–857. doi:10.1007/BF02047383
17. Johnson CD. An unusual volvulus--the ileosigmoid knot. Postgrad Med J. 1986;62(723):47–49. doi:10.1136/pgmj.62.723.47
18. Kedir M, Kotisso B, Messele G. Ileosigmoid knotting in Gondar teaching hospital north-west Ethiopia. Ethiop Med J. 1998;36:255–260.
19. Pendse AK, Khamesra HL, Babel AL. Ileosigmoid knotting. J Indian Med Assoc. 1981;77:161–162.
20. Vaez-Zadeh K, Dutz W. Ileosigmoid knotting. Ann Surg. 1970;172(6):1027–1033. doi:10.1097/00000658-197012000-00016
21. Shimizu R, Hoshino Y, Irie H, et al. Ileosigmoid knot at week 13 of pregnancy: report of a case. Int Surg. 2014;99(3):230–234. doi:10.9738/INTSURG-D-14-00011.1
22. Mbanje C, Mungazi SG, Muchuweti D, et al. Ileo-sigmoid knotting: the Parirenyatwa hospital experience. S Afr J Surg. 2020;58:70–73.
23. Mungazi SG, Mutseyekwa B, Sachikonye M. A rare occurrence of viability of both small and large bowel in ileosigmoid knotting: a case report. Int J Surg Case Rep. 1967;54:1–3. doi:10.1016/j.ijscr.2018.05.024
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.