")
Back to Journals » International Medical Case Reports Journal » Volume 15
A Case of Hepatitis E Virus Infection: One of Differential Diagnosis of Liver Injury in Patients Undergoing Peritoneal Dialysis
Authors Yan T, Sakai Y , Terada K, Okano S, Kawasaki S, Kashiwagi T , Iwabu M
Received 9 August 2022
Accepted for publication 6 October 2022
Published 10 October 2022 Volume 2022:15 Pages 557—561
DOI https://doi.org/10.2147/IMCRJ.S385393
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Tomohiro Yan, Yukinao Sakai, Kohsuke Terada, Sho Okano, Sayuri Kawasaki, Tetsuya Kashiwagi, Masato Iwabu
Department of Endocrinology, Metabolism and Nephrology, Graduate School of Medicine, Nippon Medical School, Tokyo, Japan
Correspondence: Yukinao Sakai, Department of Endocrinology, Metabolism and Nephrology, Graduate School of Medicine, Nippon Medical School, 1-1-5 Sendagi, Bunkyo-ku, Tokyo, 113-8603, Japan, Tel +81-03-3822-2131, Fax +81-3-3822-4865, Email [email protected]
Background: There are numerous causes of liver function disorder in patients undergoing peritoneal dialysis (PD). Infection with the Hepatitis E virus (HEV) is a rare cause of liver injury, and the behavior of HEV in patients with PD is unclear. Since patients undergoing dialysis are frequently polypharmatic, liver injury caused by HEV infection may be misdiagnosed as drug-induced liver injury.
Case Presentation: A 61-year-old woman with PD developed abrupt elevation of blood transaminase levels on a routine outpatient session. Since the patient has been receiving tolvaptan as the only new medication, we suspected tolvaptan induced liver injury. In further investigating the cause of liver injury, the blood screening test was found to be positive for HEV-IgA. The patient was diagnosed with HEV infection, and had a self-limited course.
Conclusion: When encountered with patients developing liver injury during PD, HEV infection should be included in the differential diagnosis.
Keywords: peritoneal dialysis, hepatitis E virus, HEV infection, liver injury
Introduction
There are numerous causes of liver function disorder in patients undergoing peritoneal dialysis (PD). Although it has been reported that PD results in a lower prevalence of hepatitis B and hepatitis C than hemodialysis (HD), viral hepatitis remains one of the major complications. Since patients undergoing dialysis are frequently polypharmatic due to multiple comorbidities, drug-induced liver injury should always be considered. When dealing with a liver function disorder, it is critical to determine the cause and choose the best course of treatment.
Infection with the Hepatic E virus (HEV) is a rare cause of liver injury. HEV is not a major disease in Japan, but HEV reports have increased since HEV-IgA was added to the National Health Insurance Program in 2011.1,2 It has been shown in a previous report that the prevalence of HEV is higher in patients with PD than in a healthy population.3 However, the behavior of HEV in patients with PD is still unclear because the number of reports conducted is very limited.
Heart failure is one of the comorbidities in patients with PD, and volume control to manage heart failure in patients with PD is critical because heart failure is associated with prognosis in patients with PD.4–6 We frequently use tolvaptan to treat heart failure because it is effective for volume control in patients with PD.7–9 Because hepatic failure is one of the most severe side effects of tolvaptan,10 when patients on tolvaptan develop liver injury, drug-induced liver injury is a crucial differential diagnosis to consider. In those cases, however, a thorough examination is required to rule out other possible causes. We present a case of a patient with PD who developed liver injury, the cause of which was initially thought to be tolvaptan but was later identified as an HEV infection.
Case Presentation
A 61-year-old woman with PD for 17 months because of end-stage kidney disease caused by immunoglobin A nephropathy visited our hospital regularly with no major issues. The abrupt elevation of transaminase levels in blood test results was observed during a routine outpatient session. That day was designated as day 0. The patient was awake, with a blood pressure of 158/88 mmHg and a body temperature of 36.8 degrees Celsius. She showed no signs of fatigue, nausea, abdominal pain, diarrhea, or jaundice. The effluent of PD was not cloudy and ultrafiltration was not impaired. Blood test results revealed elevations of liver enzymes such as aspartate aminotransferase and alanine aminotransferase. On a computer tomography examination, we found a slightly enlarged liver suspected of liver injury. We did not perform a liver biopsy or ultrasound imaging. Since day −49, the patient has been receiving tolvaptan 7.5 mg/day for volume control as the only new medication. Although her liver function was normal as of day −49 and the next session on day −28, we suspected tolvaptan-induced liver injury. We immediately discontinued tolvaptan administration and consulted the Gastroenterology Department of our hospital. To further investigate the cause of liver injury, the blood screening test was positive for HEV-IgA, and the patient was diagnosed with HEV infection; other blood test results suggesting hepatic failure caused by viral and autoimmune hepatitis were negative. Table 1 displays the results from day 0.
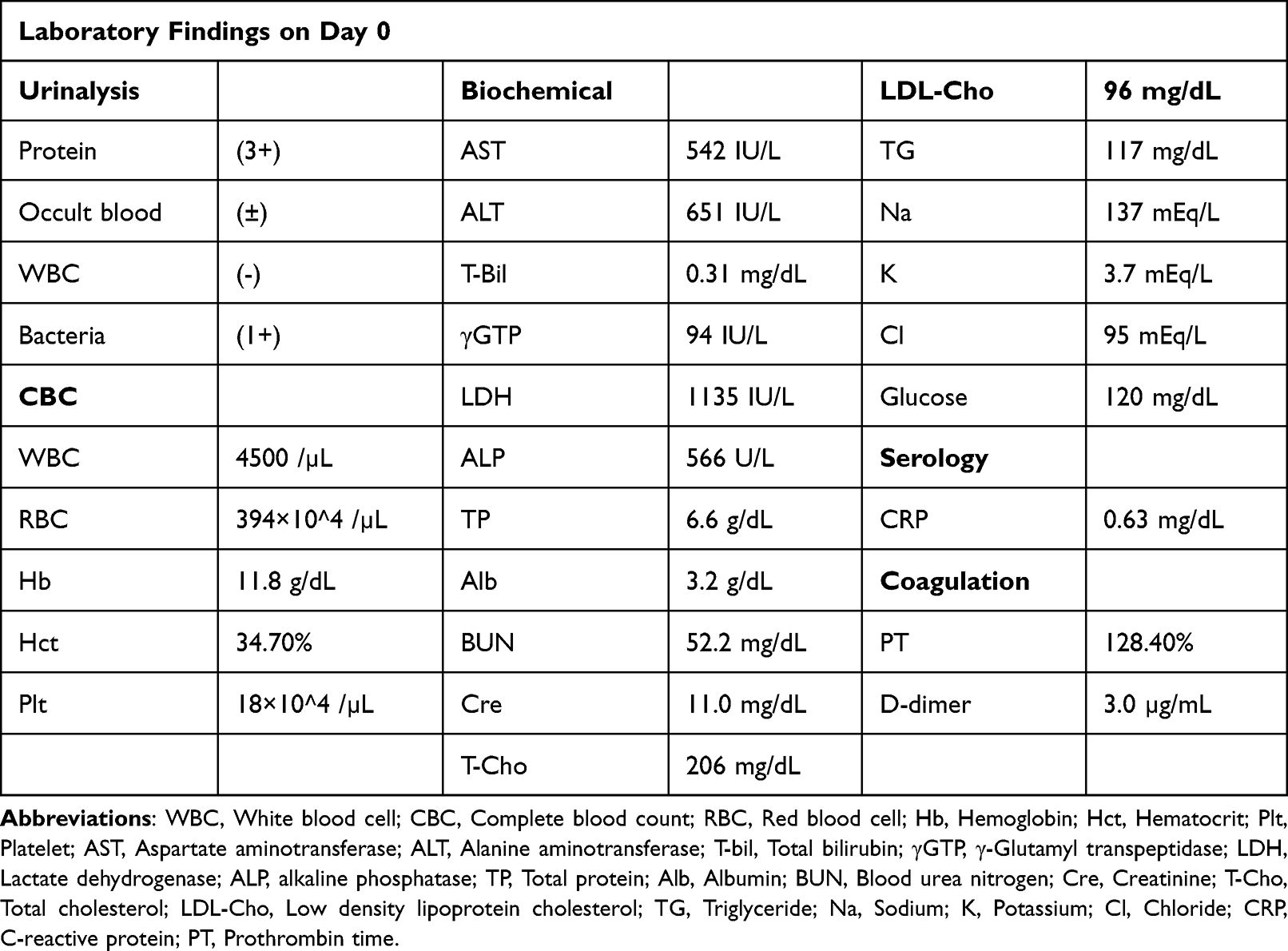 |
Table 1 Laboratory Findings on Day 0 |
Patient comorbidities included hypertension, renal and iron deficiency anemia, insomnia, and restless legs syndrome. The patient had no experience with blood transfusion, and the patient’s family did not have any history of liver injury. She did not consume any apparent contaminated water or raw meat such as swine, deer, and wild boar. The patient had not visited any countries with a known risk of developing HEV infection. In terms of medications, the patient was taking tolvaptan 7.5 mg/day, furosemide 160 mg/day, trichlormethiazide 4 mg/day, pramipexole 0.25 mg/day, amlodipine 7.5 mg/day, telmisartan 80 mg/day, zolpidem 5 mg/day, lansoprazole 15 mg/day, epinastine 20 mg/day, lanthanum carbonate hydrate 1500 mg/day, evocalcet 2 mg/day, sodium ferrous citrate 50 mg/day, and Clostridium butyricum MIYAIRI. We did not treat her HEV infection because lowering transaminase levels were already observed when we diagnosed the HEV infection with positive HEV-IgA on day 14, with no new symptoms. Additionally, we did not resume the usage of tolvaptan after the development of HEV infection as tolvaptan did not increase the urinary volume. The patient’s hepatic failure has not relapsed as of day 91. Figure 1 shows the course of HEV infection of the patient.
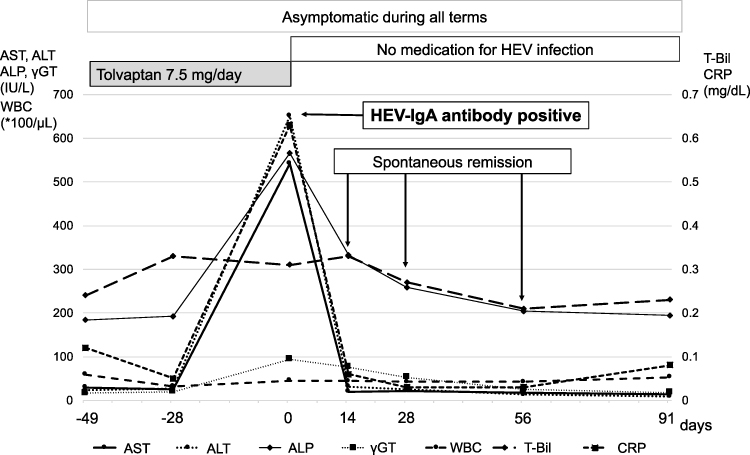 |
Figure 1 The patient’s clinical course. Abbreviations: HEV, Hepatitis E virus; WBC, White blood cell; AST, Aspartate aminotransferase; ALT, Alanine aminotransferase; T-bil, Total bilirubin; γGTP, γ-Glutamyl transpeptidase; CRP, C-reactive protein. |
Patient Approval
Institutional Review Board (IRB) approval was not required for this case study. The patient has approved the use of her medical information in this case report and has approved the final text of this manuscript. She has signed a consent form indicating her approval.
Discussion
HEV Infection
HEV is a small non-enveloped virus belonging to the genus Hepacivirus in the Hepeviridae family. HEV has a positive-sense, single-stranded, RNA genome.11,12 Around 20 million HEV infections occur every year in the world, and HEV is one of the most common causes of acute viral hepatitis in most regions.12 HEV has four genotypes, which are HEV1 to HEV4.11,12 HEV1 and HEV2 are only found in humans and spread through contaminated water in many developing countries; HEV1 infections are prevalent in Asia, whereas HEV2 infections are in Africa and Mexico.11,12 HEV3 and HEV4 are found in many mammals, including humans, including pigs, wild boars, and deer, and infections in humans occur in both developed and developing countries.11,12 HEV3 and HEV4 infections are linked to the consumption of raw or undercooked pork, which infect people sporadically through food in industrialized countries.11,12 Human-to-human transmission of HEV3 and HEV4 occurs only via bloodborne transmission in industrialized countries, and there have been reports of transfusion-related HEV infections.12–14 Whereas HEV-IgM and HEV-RNA are utilized in most countries to diagnose HEV infection, HEV-IgA measurement is common in Japan since it was covered by the National Health Insurance Program in 2011.1,2 HEV-IgA is slightly more specific than HEV-IgM and is more useful than HEV-RNA in terms of specificity and duration.6,7,15 In our case, the patient had not undergone a blood transfusion before and was diagnosed with HEV-IgA alone, and therefore the genotype is unknown.
In most cases, HEV infection is asymptomatic.13,14 Acute HEV3 and HEV4 infections typically last 4–6 weeks and are self-limited, with symptoms including jaundice, malaise, anorexia, nausea, abdominal pain, fever, and arthralgia.4 When treated, patients with acute HEV3 infection appear to be sensitive to ribavirin monotherapy.4 HEV3 may develop chronic HEV in solid-organ transplant recipients.4,13 HEV may be misdiagnosed as drug-induced liver injury, and a UK study found that 13% of presumed drug-induced liver injury was acute HEV3 infection.16 There is a previous report that liver enzyme levels can predict the possibility of HEV.17 In light of the literature, our patient had AST 542 IU/L, ALT 651 IU/L, and ALP 566 U/L, with R-value of 8.26, supporting the diagnosis of HEV.
HEV Infection and PD
Reportedly, HD patients have a high prevalence of HEV-IgG positivity rate compared to patients with PD,8 and they may be acquired by blood contamination.10 In contrast, it is said that HEV infection is more common in patients with PD than in healthy individuals.18 The patient in our case was asymptomatic and had a self-limited course. Ultrafiltration and solute removal by PD were not affected during the observation. On the other hand, HEV poses a risk to pregnant women and elderly people with liver disease who may develop fulminant HEV infection.12,13 Although PD has a lower risk of bloodborne infection than HD as a modality, HEV infection is a disease that should not be overlooked. Because patients undergoing dialysis are often polypharmatic, HEV infection may be misdiagnosed as drug-induced liver injury. There have been very few reports of HEV among patients with PD, and its clinical behavior is still unknown. More research, including reports on aggravation risk factors, is required.
Limitations
The virus genotype and infection route are unknown in this case. Although serological diagnosis using HEV-IgA is a well-established test in Japan, IgM class antibody was not identified and the effects of drug-induced liver injury, including tolvaptan, cannot be ruled out either.
Conclusion
When encountered with patients developing liver injury during PD, HEV infection should be included in the differential diagnosis.
IRB Approval
This study did not require IRB approval, and the final manuscript was approved by the patient.
Funding
This study was not funded.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Inagaki Y, Oshiro Y, Hasegawa N, et al. Clinical features of hepatitis E virus infection in Ibaraki, Japan: autochthonous hepatitis E and acute-on-chronic liver failure. Tohoku J Exp Med. 2015;235(4):275–282. doi:10.1620/tjem.235.275
2. Kanayama A, Arima Y, Yamagishi T, et al. Epidemiology of domestically acquired hepatitis E virus infection in Japan: assessment of the nationally reported surveillance data, 2007–2013. J Med Microbiol. 2015;64(7):752–758. doi:10.1099/jmm.0.000084
3. Rivera M, Mateos ML, Teruel JL, Marcen R, Ortuno J. Hepatitis E virus markers in a peritoneal dialysis population. Perit Dial Int. 2000;20(5):576–577. doi:10.1177/089686080002000516
4. Teitelbaum I. Ultrafiltration failure in peritoneal dialysis: a pathophysiologic approach. Blood Purif. 2015;39(1–3):70–73. doi:10.1159/000368972
5. Wang AY, Brimble KS, Brunier G, et al. ISPD cardiovascular and metabolic guidelines in adult peritoneal dialysis patients part II - management of various cardiovascular complications. Perit Dial Int. 2015;35(4):388–396. doi:10.3747/pdi.2014.00278
6. Wang AY, Wang M, Lam CW, Chan IH, Lui SF, Sanderson JE. Heart failure in long-term peritoneal dialysis patients: a 4-year prospective analysis. Clin J Am Soc Nephrol. 2011;6(4):805–812. doi:10.2215/CJN.07130810
7. Mori T, Kurasawa N, Ohsaki Y, et al. Role of chronic use of tolvaptan in patients with heart failure undergoing peritoneal dialysis. Adv Perit Dial. 2016;32:39–45.
8. Mori T, Oba I, Koizumi K, et al. Beneficial role of tolvaptan in the control of body fluids without reductions in residual renal function in patients undergoing peritoneal dialysis. Adv Perit Dial. 2013;29:33–37.
9. Hiramatsu T, Hobo A, Hayasaki T, Kabu K, Furuta S. A pilot study examining the effects of tolvaptan on residual renal function in peritoneal dialysis for diabetics. Perit Dial Int. 2015;35(5):552–558. doi:10.3747/pdi.2013.00290
10. Khan MY, Rawala MS, Siddiqui M, Abid W, Aslam A. Tolvaptan-induced liver injury: who is at risk? A case report and literature review. Cureus. 2019;11(4):e4842. doi:10.7759/cureus.4842
11. Kamar N, Bendall R, Legrand-Abravanel F, et al. Hepatitis E. Lancet. 2012;379(9835):2477–2488. doi:10.1016/S0140-6736(11)61849-7
12. Sridhar S, Lau SK, Woo PC. Hepatitis E: a disease of reemerging importance. J Formos Med Assoc. 2015;114(8):681–690. doi:10.1016/j.jfma.2015.02.003
13. Colson P, Coze C, Gallian P, Henry M, De Micco P, Tamalet C. Transfusion-associated hepatitis E, France. Emerg Infect Dis. 2007;13(4):648–649. doi:10.3201/eid1304.061387
14. Matsubayashi K, Nagaoka Y, Sakata H, et al. Transfusion-transmitted hepatitis E caused by apparently indigenous hepatitis E virus strain in Hokkaido, Japan. Transfusion. 2004;44(6):934–940. doi:10.1111/j.1537-2995.2004.03300.x
15. Wang CH, Tschen SY, Schalasta G, Pillot J, Jahn G, Flehmig B. Anti-hepatitis E virus markers in hemodialysis patients. Nephron. 1996;72(2):343–345. doi:10.1159/000188878
16. Takahashi M, Kusakai S, Mizuo H, et al. Simultaneous detection of immunoglobulin A (IgA) and IgM antibodies against hepatitis E virus (HEV) is highly specific for diagnosis of acute HEV infection. J Clin Microbiol. 2005;43(1):49–56. doi:10.1128/JCM.43.1.49-56.2005
17. El-Mokhtar MA, Ramadan HK, Thabet MM, et al. The unmet needs of hepatitis E virus diagnosis in suspected drug-induced liver injury in limited resource setting. Front Microbiol. 2021;12:737486. doi:10.3389/fmicb.2021.737486
18. Davern TJ, Chalasani N, Fontana RJ, et al. Acute hepatitis E infection accounts for some cases of suspected drug-induced liver injury. Gastroenterology. 2011;141(5):
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.