")
Back to Journals » Journal of Pain Research » Volume 7
Voices that may not otherwise be heard: a qualitative exploration into the perspectives of primary care patients living with chronic pain
Authors Wallace L, Wexler R, McDougle L, Miser WF, Haddox JD
Received 12 February 2014
Accepted for publication 19 March 2014
Published 3 June 2014 Volume 2014:7 Pages 291—299
DOI https://doi.org/10.2147/JPR.S62317
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Lorraine S Wallace,1 Randell K Wexler,1 Leon McDougle,1 W Frederick Miser,1 J David Haddox2,3
1Department of Family Medicine, the Ohio State University, Columbus, OH, USA; 2Health Policy, Purdue Pharma L.P., Stamford, CT, USA; 3Department of Public Health and Community Medicine, Tufts University School of Medicine, Boston, MA, USA
Background: Although psychometrically sound pain assessment tools are available, there is a paucity of research that comprehensively defines chronic pain from the perspective of patients. The purpose of this study was to examine the utility of a combination of qualitative methods (Photovoice, one-on-one interviews, and focus groups) in examining the daily experiences of primary care patients living with chronic pain.
Methods: A sample of English-speaking primary care patients aged 30 years or older, who had been prescribed an opioid for long-term, noncancer pain management, participated in the study. Each patient took photographs that best reflected both his/her experiences with chronic pain and what he/she would like his/her life to be without chronic pain.
Results: Patients submitted an average of 20.2±3.1 photographs (range =8–27 photographs). Analysis of one-on-one interviews illuminated five dominant themes: daily need for multiple medications, including opioids; difficulties climbing a flight of stairs; struggling to get out of bed in the morning; extreme challenges with participating in day-to-day life activities; and experiencing feelings of hopelessness and helplessness on a regular basis. Seven themes emerged from the focus groups: undesired effects/burdens of medications, loss of/striving for independence, effect on social interactions/relationships, pain effect on activities of daily living, constant search for convenience/a better situation, interactions with physicians, and frustration/depression with pain.
Conclusion: The qualitative methods employed in this study provide deep insight into perceptions and experiences of patients living with chronic pain that is vital for informing future clinical interventions.
Keywords: opioid, Photovoice, qualitative research
A Letter to the Editor has been received and published for this article.
Background
Individuals living with chronic pain often struggle to present themselves as credible when seeking medical care because pain is invisible.1,2 Not surprisingly, it is not uncommon for patients with complaints of chronic pain to report poor-quality interactions with health care professionals.3 Because chronic pain is a highly complex phenomenon, a need exists to comprehensively define the chronic pain experience from the perspective of patients.
An extensive collection of self-administered assessment tools has been developed to capture patients’ experiences and beliefs related to a broad spectrum of psychosocial outcomes resulting from living with chronic pain. Specifically, survey-based tools can assess dimensions such as patients’ acceptance of chronic pain symptoms,4 pain management self-efficacy,5 perceptions regarding the purposes and benefits of pain medication,6 extent of pain-related anxiety,7 and recent and current pain intensity.8 In addition, qualitative data collection methods have uncovered extensive portrayals of the daily realities of patients living with chronic pain. For example, in-depth interviews with patients with chronic pain revealed not only overwhelming feelings of shame9 and frustration10 but also daily experiences of powerlessness and ambivalence.11
The Photovoice method combines photography and accompanying narratives to explore perspectives of individuals that may not otherwise be appreciated.12–14 Although Photovoice has been used predominantly to explore community-based issues to facilitate societal change,15 this method holds great promise in understanding the complexities of those living with chronic health conditions as well. For example, Photovoice was useful in enabling patients with chronic mental illness16 and families coping with a child with complex care needs17 to meaningfully depict their personal and familial circumstances through both photography and in-depth discussion.
To our knowledge, Photovoice has been used in just one small pilot study to explore the chronic pain-related experiences of older adults recruited from both nonclinic and clinic-based settings in the Southeastern United States.18 Therefore, to address this gap in the literature, this study examined the utility of a combination of qualitative methods (Photovoice, one-on-one interviews, and focus groups) in examining the daily experiences of primary care patients living with chronic pain.
Materials and measures
Patient recruitment
The electronic medical record database at the Ohio State University Wexner Medical Center was queried to identify a random sample of English-speaking patients meeting the following criteria: seen within the past 6 months at a clinic within the Ohio State University Wexner Medical Center primary care network, aged 30 years or older, and receiving an opioid medication for long-term, noncancer pain management for at least the past 6 months. The exclusion criterion was appearing acutely ill at time of first interview. All study procedures were approved by the institutional review board at Ohio State University.
Using a computer-generated sequence, patients (n=106) were randomly chosen to potentially participate in the study. Two strategies were used to recruit potential patients to partake in this study. First, patients were sent an individualized letter signed by his/her personal family physician, via the US Postal Service, describing the purposes of the study. Second, approximately 1 week after the initial recruitment letter mailing, a trained research assistant (RA) called potentially eligible patients to invite them to participate in the study. RAs attempted to contact each identified patient by telephone calls at varying times of day a maximum of four times. RAs were unable to contact 32 of the 106 patients on the randomized list. Of 74 patients successfully contacted by telephone, 31 (41.9%) agreed to participate in the study.
Baseline one-on-one interview
Patients (n=31) agreeing to participate in the study were scheduled for a one-on-one baseline interview with an RA to complete a sociodemographic survey and receive instructions regarding Photovoice procedures. At the interview, the ability to understand English was confirmed, as was visual acuity. None of the potentially eligible patients appeared acutely ill. Thus, all patients presenting for initial interview satisfied all criteria for participation in the study.
After each informed consent was obtained and documented, the RA orally administered sociodemographic items from the 2011 Behavioral Risk Factor Surveillance Survey to each participating patient.19 Each patient received one 27-exposure Kodak Fun-Saver® (Eastman Kodak, Rochester, NY, USA) single-use, disposable camera and was instructed on its use, the intent of the photographs, and how to document information about each photograph. Each patient was instructed not to take any photographs that threatened his/her personal safety or well-being or that violated the safety or privacy of another.
Patients were asked to take photographs that best reflected their both current experiences with chronic pain and their future desires for what they would like their lives to be without chronic pain during the following 7–10 days. Patients were given a detailed instruction sheet describing study procedures and contact information for the principal investigator (PI) if they had questions and/or concerns about the study. Patients received a postage-paid, insured envelope to return their camera to the research team within approximately 3 weeks of completion of the baseline one-on-one interview. At the conclusion of the baseline interview, each patient received a $20 supermarket gift card to compensate him/her for his/her time spent during the baseline interview.
Follow-up one-on-one interview
Once a patient’s photographs were developed and printed in duplicate on 4″×6″ glossy paper, he/she was invited to participate in a one-on-one follow-up interview with a RA. Twenty-five (80.6%) of the 31 patients partaking in the baseline interview submitted photographs and completed the follow-up one-on-one interview.
To begin the follow-up interview, the RA placed the patient’s printed photographs on the table for him/her to review. Each patient was asked to look through his/her respective photographs and to select four to six images that best represented either his/her current experiences with chronic pain or his/her future desires for what he/she would like his/her life to be without chronic pain. For each of the selected photographs, the patient provided a title, composed a brief narrative describing how the photograph depicted his/her experience with chronic pain and/or desires for the future, and discussed why he/she shared the photograph. The RA recorded the responses verbatim on paper and then attached them to the selected photographs. Each patient received a $50 supermarket gift card to compensate him/her for submitting his/her photographs and completing the follow-up one-on-one interview.
Focus group sessions
On completion of a one-on-one follow-up interview, each patient was invited to partake in one of three scheduled focus group sessions. Nineteen (76.0%) of the 25 patients completing both the baseline and follow-up one-on-one interviews participated in a focus group session. Focus group sessions were held at varying times during the week at a centrally located classroom setting in Columbus, Ohio. The first focus group was held on a weeknight in the early evening, whereas the other two sessions were held midmorning (one midweek and the other on a Saturday morning). Light refreshments were served at each focus group session.
Before each session, the PI reviewed each confirmed focus group participant’s photographs and selected eight to ten representative photographs from those submitted by the confirmed participants. Electronic copies of selected photographs were displayed on a large screen using a liquid crystal display projector during the focus group.
The PI attended each focus group session and provided an overview of data collection procedures to patients. After obtaining and documenting informed consent from each participating patient, the PI introduced the focus group leader who led and facilitated each session. The facilitator was hired by the research team as a consultant on the project because of her expertise in facilitating focus groups. The facilitator had no prior knowledge of any of the patients.
The SHOWeD mnemonic method20 was used by the facilitator to steer group conversations about each displayed photograph. Specifically, the following SHOWeD items were posed to focus group participants: What do you see in this photograph? What is happening in this photograph? How does this relate to our lives? Why does this situation/issue exist? And what can we do to address these issues? Each focus group session was audio-recorded and subsequently transcribed in its entirety. At the conclusion of the focus group session, each patient received a $30 supermarket gift card to compensate him/her for his/her time. On average, patients completing all phases of this project were engaged in the study between 3–5 months in total.
Data analysis
Descriptive statistics (percentages, frequencies, mean, and standard deviation) were calculated to depict the sociodemographic characteristics of the study sample. The total number of submitted photographs submitted were tallied by patient and sorted by theme and pain characterization type. Photovoice calls for all themes generated during focus group sessions to be participant-driven, rather than investigator-driven. Grounded theory qualitative methods were used to guide data analysis and subsequent interpretation of focus group session transcripts.21
Results
One-on-one baseline and follow-up interviews
Twenty-five patients (21 women and four men) submitted photographs and completed both one-on-one interviews. Patients averaged 50.6±12.4 years of age (range =32–73 years), with most reporting their general health to be either fair or poor (n=19; 76.0%). Slightly more than half of patients were black (n=17; 68.0%); the remainder were non-Hispanic white (n=8; 32.0%). Most patients were insured through either Medicaid or Medicare (n=21; 84.0%). One patient had not completed high school, 10 (40.0%) patients were high school graduates, 9 (36.0%) had completed some college, and five (20.0%) were college graduates.
Patients submitted an average of 10.3±5.4 legible, nonduplicate photographs (range =2–21 photographs). As shown in Table 1, a total of 247 photographs, representing four main themes, were reviewed and sorted. The themes were activities of daily living, daily realities of living with chronic pain, desire for a “normal” life, and sources of comfort and/or hope. A substantial majority of photographs depicted patients’ current experiences with chronic pain (n=226; 91.5%) compared with relatively few depicting either future desires or what they would like their lives to be without chronic pain (n=21; 8.5%). Figures 1–6 depict daily life experiences of patients living with chronic pain, including “a cooler full of medicines” (see Figure 1), “a week’s worth of pills” (Figure 2), “patient central” (Figure 3), “view from inside” (Figure 4), “view from upstairs” (Figure 5), and “walking with pain” (Figure 6).
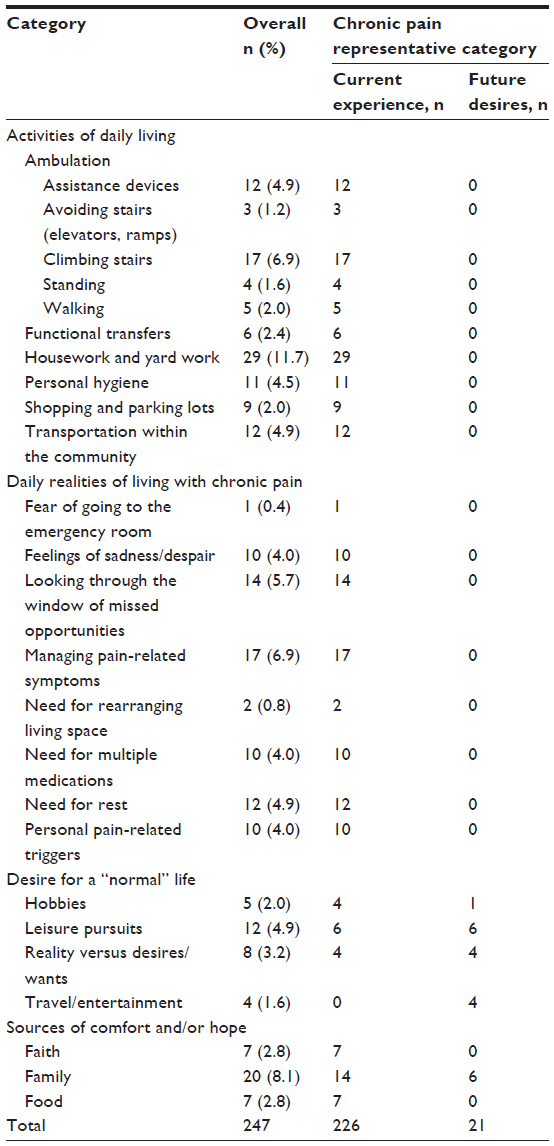 | Table 1 Summary of patients’ photographs overall and by chronic pain representative category |
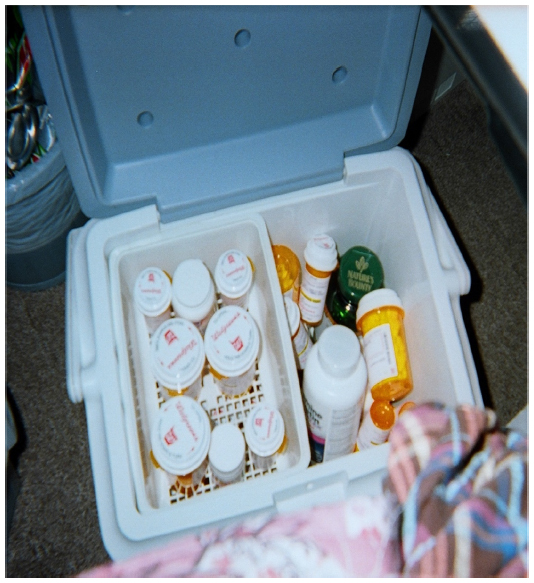 | Figure 1 “I am dependent on pain medications. But, they make me very drowsy and keep me from doing what I really want.” |
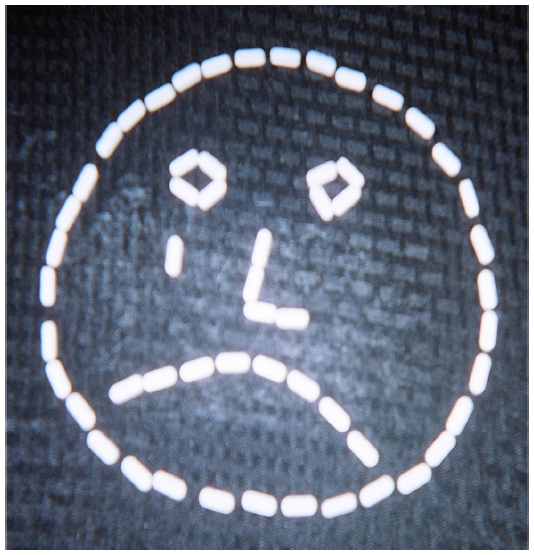 | Figure 2 “I feel like a ‘slave’ to pills. But, they help me get through.” |
 | Figure 3 “I spend most of my time in this corner of my house. Everything that I need is here. However, there are lots of things in my home that I don’t have easy access to.” |
 | Figure 4 “The community center is in my view. Chronic pain prevents me from going where I want. Pain leads to isolation.” |
 | Figure 5 “I stay upstairs a lot because the stairs are difficult. I keep everything I need in my room.” |
 | Figure 6 “I would normally wear the red heels, but with the pain I have to wear the white tennis shoes.” |
Focus group sessions
Nineteen patients participated in one of the three scheduled focus groups (focus group 1, n=7; focus group 2, n=7; focus group 3, n=5). Collectively, seven themes emerged across focus group sessions: undesired effects/burdens of medications, loss of/striving for independence, effect on social interactions/relationships, pain effect on activities of daily living, constant search for convenience/a better situation, interactions with physicians, and frustration/depression with pain.
Undesired effects/burdens of medication
The photograph of prescription bottles conjured up lengthy discussion concerning emotions about medication. The discussion was mostly negative in nature and revolved around the notion that medication seemed to hurt more than help. The following quotation exhibits ambivalent feelings about taking medication and what medication does (and does not do) for them: “I’m 46 years old, and I take more pills than my grandparents ever did. If you don’t take them, you’ll be a lot sadder than that.”
Loss of/striving for independence
When viewing photographs expressing pain, many patients, across focus groups, commented on the idea of either losing their independence or striving for independence. The following quotations typify the frustration patients feel when experiencing loss of independence resulting from pain-related restrictions and also describe how patients may strive to be independent despite living with chronic pain: “And then having to ask for help is another big huge step you need to feel inside, and sometimes that really overwhelms you.” And: “I don’t like anybody’s help. I just don’t want anybody’s help.”
Effect on social interactions/relationships
The influence that living with chronic pain has on relationships was evident. Mostly, patients expressed how relationships with family members, children, friends, and the general public have been affected by their experiences. Many patients talked about relationships with their children or grandchildren. Mothers were reliant on their children to help take care of the household and younger siblings; grandchildren were constantly wondering why their grandparents could no longer play with them or take them on vacation. Throughout the discussion, negative and positive recollections of experiences in these areas were told, including: “being a single mom of two, it pretty much disables me, and I feel terrible because I have to look at my 17-year-old son and say, ‘Do you mind watching your brother, I need to go lay down.’ Or, you know, ‘I can’t take my son to the park, can you take him for me?’ I feel like I put a big huge responsibility on my 17-year-old, but there’s not much I can do.” And: “Even if someone invites me to their house, I say, ‘Do you have stairs?’ And I want to know what I have to do because if they say, ‘I have stairs. More than five.’ I say, ‘You can come see me.’”
Pain effect on activities of daily living
A photograph showing a pair of high-heeled shoes elicited talk about limitations concerning one’s social life, activities, and hobbies. Concurrently, a patient mentioned that pain not only impedes what you do for fun but also inhibits performance at your job. The following quotations reveal some of the feelings that were expressed concerning these life changes: “Now, let me explain to you the reasoning in that …. Prior to my chronic pain, I was rocking them heels. On a constant basis, so my closet is like full of those. Now, they’re full of K-Swiss and Nikes. You know, my cousin is like, ‘Yeah go get those heels, come wear them.’ I can’t. So, I try to put them on and try to be cute and before long, the flip-flops or the tennis shoes are on.” And: “I’m a cook at a nursing home. I cook for 200 people, and that big pan there – I handle some pretty heavy duty stuff. It’s wearin’ and tearin’ my hands up, but I’m too young to retire. I don’t want to retire, I want to work. I have to find solutions for myself. I wrote my supervisor and she got me this three-tiered cart so when I lift up heavy pots and pans, I put them on the cart instead of carrying them. So that helps a lot.”
Constant search for convenience/ a better situation
Two specific locations emerged in which participants elaborated on their search for convenience: at home and while shopping. Setting up a bedroom to have all that is needed within grasp was common in this group, explained as stemming from mobility limitations resulting from chronic pain. “I had one of my girlfriends come over, and she said, ‘Your bedroom is like an apartment.’ And I said, ‘Yeah, I got my microwave, my refrigerator, everything right here. Because when I was on my back, didn’t nobody gonna come. So, when somebody came, I had them bring up everything I needed.’” And: “See, that’s where I’m going. Since I’ve been dealing with all this pain, I will go at the least conspicuous time, where I’m thinking it’s probably two people in there. You know what I’m saying? I go in and get my shopping done.”
Interactions with physicians
Although several participants expressed that their doctor “understands” their pain, many comments were more negative in nature. These comments expressed a want for physicians to communicate with each other more and to try to understand what medication or procedures a patient has tried already. Many individuals also felt their physician did not understand their feelings toward taking medication and just assumed they were seeking out more prescriptions. “It would be fine … I think it would be neat to see if a doctor could maybe experience a little bit of what a person goes through. Especially if you’re in a wheelchair or with me …migraines … having to lay down in a dark room for hours upon hours just so you can get some kind of small relief, just to even get up and make dinner for your kids. Or to the point where … some way of making them experience it for a day or spend a day with a person and go through what they go through every day. And maybe then they’ll start realizing it’s just not medicine, its other things with people’s bodies that takes over them.”
Frustration/depression with pain
The narratives told by patients often pointed to an overall frustration with their current state of health. These instances focused on the difficulty staying positive despite pain, pain as interference in life, questioning why one has to live with pain, and a lack of understanding from others regarding the pain that one is experiencing. “Sometimes you wonder, why does it happen to you? Why does it have to happen to you? Why can’t it happen … you know, you don’t want it to happen to other people, but you just want to be able to say, you know, I deserve better than this. Why did it happen to me? Why do I have to go through it?” And: “When they say, you look good, but you don’t feel good, it’s their diminishing, denying, not understanding what’s going on inside. You can’t see pain. You can see manifestations of it, maybe.”
Discussion
Our findings provide rich insight into the daily lives of primary care patients living with chronic pain. Cameras served as a valuable mechanism to enable patients to capture meaningful images to show and then subsequently describe their personal stories regarding daily realities of living with chronic pain. Simply having the opportunity to voice and share their personal experiences, in both individual and group formats, was both therapeutic and empowering for many patients in knowing they were not alone in their struggles with chronic pain. Ultimately, findings from this study could not only provide health care providers with greater understanding regarding the challenges faced by their patients living with chronic pain but also increase their empathy toward them as well.
Nearly 250 unique, nonduplicate photographs were submitted by 25 patients. Photographs provided a means of depicting specifically how chronic pain affects patients’ lives. Most photographs represented either activities of daily living or daily realities of living with chronic pain. Nearly one-fifth of the photographs portrayed some aspect of ambulation, with many patients taking pictures of both stairs inside their residence and at various outside locations. Extreme difficulty in climbing stairs was a common thread voiced throughout both one-on-one interviews and focus group sessions. Similarly, a large number of photographs depicted patients’ inability to complete everyday housework and yard work activities. In addition, patients’ took many photographs representing their attempts and strategies to manage their pain-related symptoms, including sleeping and resting.
One-quarter of the submitted photographs represented patients’ desire for a “normal” life or sources of comfort and/or hope. Many patients took photographs of leisure pursuits they once enjoyed that are now limited or curtailed because of chronic pain. Patients also described how chronic pain kept them close to home and limited their ability to travel and explore new surroundings. Although patients commonly spoke of their families as a source of hope, they also described feelings of sadness because chronic pain often limited their ability to engage with family and friends as much as they would like.
Although photographs represented many diverse situations and obstacles, perhaps the most important finding was that the great majority of photographs depicted patients’ current experiences with chronic pain. Patients took very few photographs portraying their future desires for what they would like their lives to be like without chronic pain. These findings underscore not only the all-encompassing “now” nature of chronic pain but also the inability of these patients to focus on the future. Importantly, patients’ inability to move beyond “now” may negatively affect areas of health care other than pain management. In particular, the management and prevention of future consequences of other chronic diseases (eg, diabetes, hypertension) may be complicated by a focus only on the present. For example, a primary care physician could face significant barriers in counseling a hypertensive patient with chronic pain who is “now”-focused to control sodium intake if salty food is one their few sources of pleasure and immediate gratification.
Photographs displayed during focus groups prompted many rich discussions surrounding the complex realities of living with chronic pain, including undesired effects/burdens of medications, loss of/striving for independence, effect on social interactions/relationships, pain effect on activities of daily living, constant search for convenience/a better situation, interactions with physicians, and frustration/depression. In synthesizing focus group findings, the following overarching question emerged as a most critical one to address: “What can be done to improve these patients’ functioning and quality-of-life?”
Unfortunately, many patients foresee no hope for the future and were dissatisfied not only with their current functional status but also with the adverse effects stemming from taking large amounts of opioid medications on a regular basis.
Although physicians are often frustrated in treating patients with complaints of chronic pain and governmental agencies try to reduce “pill mills”,22,23 our results also highlight that patients are equally frustrated by the medications, adverse effects, limited activity, and disability resulting from chronic pain. Patients often felt their physician did not understand their ambivalence toward taking medications and just assumed they were seeking out more prescriptions. Unfortunately, a perception such as this could have serious negative repercussions on the entire patient–physician relationship, which in turn could affect other aspects of general health care. Thus, the trusting relationship between the primary care provider and patient with chronic pain must be established over time in most incidences.
There are two major strengths of this study. First, in-depth data collection methods (Photovoice, one-on-one interviews, and focus groups) were employed to capture real-life realities of patients living with chronic pain. Second, our sample was drawn from a diverse pool of primary care patients exclusively, distinct from patients cared for by pain physicians. This is important because a substantial proportion of adult primary care appointments involve patients with chronic pain complaints.24,25
Limitations
Our findings should be considered within the context of several potential limitations. First, this study was conducted in large metropolitan city in a Midwestern state. Therefore, the experiences described may represent only those encountered by this patient population. By design, this qualitative study was not intended to obtain widely generalizable results; rather, it was intended to provide a rich, in-depth picture of individual patients’ experiences in living with chronic pain. Second, our sample included a relatively small number of men. Therefore, we are unable to determine whether our findings would have varied had our study included an equal number of men and women. Third, nearly a quarter (n=6) of patients who submitted photographs and completed both one-on-one interviews did not participate in a focus group session. However, our attrition rate was slightly better than a similar population of chronic pain patients.18 Although it is unknown whether focus group findings would have been different had all patients participated, data saturation was reached at the conclusion of the third focus group. Fourth, although we collected and recorded key demographic information from each patient, it would have been worthwhile to obtain other pertinent information as well (eg, depression history before the onset of chronic pain, employment status, and so on). Last, our sample was limited to patients receiving an opioid medication for long-term, noncancer pain management exclusively. Recognizing that many patients with significant pain manage with nonopioid medications and/or alternative modalities, future studies should focus on this patient population as well.
Conclusion
Patients in this study were able to record photographs to help bring their daily experiences of living with chronic pain to life. Given differing communication preferences among patients, a combination of qualitative methods, including Photovoice, may enable and empower some patients to more effectively relate their chronic suffering to health care professionals caring for them.
Disclosure
Dr. Haddox is a full-time employee of Purdue Pharma, L.P. The authors report no other conflicts of interest. This study was funded by Purdue Pharma, L.P.
References
Newton BJ, Southall JL, Raphael JH, Ashford RL, LeMarchand K. A narrative review of the impact of disbelief in chronic pain. Pain Manag Nurs. 2013;14(3):161–171. | |
Werner A, Malterud K. It is hard work behaving as a credible patient: encounters between women with chronic pain and their doctors. Soc Sci Med. 2003;57(8):1409–1419. | |
Upshur CC, Bacigalupe G, Luckmann R. “They don’t want anything to do with you”: patient views of primary care management of chronic pain. Pain Med. 2010;11(12):1791–1798. | |
McCracken LM, Vowles KE, Eccleston C. Acceptance of chronic pain: component analysis and a revised assessment method. Pain. 2004;107(1–2):159–166. | |
Nicholas MK. The pain self-efficacy questionnaire: Taking pain into account. Eur J Pain. 2007;11(2):153–163. | |
Schieffer BM, Pham Q, Labus J, et al. Pain medication beliefs and medication misuse in chronic pain. J Pain. 2005;6(9):620–629. | |
McCracken LM, Dhingra L. A short version of the Pain Anxiety Symptoms Scale (PASS-20): preliminary development and validity. Pain Res Manag. 2002;7(1):45–50. | |
Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994;23(2):129–138. | |
Werner A, Isaksen LW, Malterud K. ‘I am not the kind of woman who complains of everything’: illness stories on self and shame in women with chronic pain. Soc Sci Med. 2004;59(5):1035–1045. | |
Dow CM, Roche PA, Ziebland S. Talk of frustration in the narratives of people with chronic pain. Chronic Illn. 2012;8(3):176–191. | |
Råheim M, Håland W. Lived experience of chronic pain and fibromyalgia: women’s stories from daily life. Qual Health Res. 2006;16(6):741–761. | |
Wang C, Burris MA. Photovoice: concept, methodology, and use for participatory needs assessment. Health Educ Behav. 1997;24(3):369–387. | |
Wang C, Burris MA, Ping XY. Chinese village women as visual anthropologists: a participatory approach to reaching policymakers. Soc Sci Med. 1996;42(10):1391–1400. | |
Wang C, Burris MA. Empowerment through photo novella: portraits of participation. Health Educ Q. 1994;21(2):171–186. | |
Hergenrather KC, Rhodes SD, Cowan CA, Bardhoshi G, Pula S. Photovoice as community-based participatory research: a qualitative review. Am J Health Behav. 2009;33(6):686–698. | |
Thompson NC, Hunter EE, Murray L, Ninci L, Rolfs EM, Pallikkathayil L. The experience of living with chronic mental illness: a photovoice study. Perspect Psychiatr Care. 2008;44(1):14–24. | |
Woodgate RL, Edwards M, Ripat J. How families of children with complex care needs participate in everyday life. Soc Sci Med. 2012;75(10):1912–1920. | |
Baker TA, Wang CC. Photovoice: use of a participatory action research method to explore the chronic pain experience in older adults. Qual Health Res. 2006;16(10):1405–1413. | |
Centers for Disease Control and Prevention. 2011 Behavioral Risk Factor Surveillance Survey. Available at: http://www.cdc.gov/brfss/questionnaires/pdf-ques/2011brfss.pdf. Accessed January 2, 2013. | |
Wallerstein N. Empowerment education: Freire’s ideas applied to youth. Youth Policy. 1987;9:11–15. | |
Strauss AC, Corbin JM. Basics of Qualitative Research: Grounded Theory Procedures and Techniques. London: Sage Publishers; 1990. | |
Dobscha SK, Corson K, Flores JA, Tansill EC, Gerrity MS. Veterans affairs primary care clinicians’ attitudes toward chronic pain and correlates of opioid prescribing rates. Pain Med. 2008;9(5):564–571. | |
Nwokeji ED, Rascati KL, Brown CM, Eisenberg A. Influences of attitudes on family physicians’ willingness to prescribe long-acting opioid analgesics for patients with chronic nonmalignant pain. Clin Ther. 2007;29 Suppl:2589–2602. | |
Caudill-Slosberg MA, Schwartz LM, Woloshin S. Office visits and analgesic prescriptions for musculoskeletal pain in US: 1980 vs 2000. Pain. 2004;109(3):514–519. | |
Olsen Y, Daumit GL, Ford DE. Opioid prescriptions by US primary care physicians from 1992 to 2001. J Pain. 2006;7(4):225–235. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.