")
Back to Journals » Infection and Drug Resistance » Volume 8
Validation of a phage-open reading frame typing kit for rapid identification of methicillin-resistant Staphylococcus aureus (MRSA) transmission in a tertiary hospital
Authors Takahashi H, Seki M, Yamamoto N, Hamaguchi S, Ojima M, Hirose T, Yoshiya K, Toyokawa M, Nishi I, Ogura H, Shimazu T, Tomono K
Received 25 February 2015
Accepted for publication 23 March 2015
Published 14 May 2015 Volume 2015:8 Pages 107—111
DOI https://doi.org/10.2147/IDR.S83509
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Hiroki Takahashi,1,* Masafumi Seki,2,4,* Norihisa Yamamoto,2 Shigeto Hamaguchi,2 Masahiro Ojima,1 Tomoya Hirose,1 Kazuhisa Yoshiya,1 Masahiro Toyokawa,3 Isao Nishi,3 Hiroshi Ogura,1 Takeshi Shimazu,1 Kazunori Tomono2
1Department of Traumatology and Acute Critical Medicine, Osaka University Hospital, Suita, Osaka, Japan; 2Division of Infection Control and Prevention, Osaka University Hospital, Suita, Osaka, Japan; 3Laboratory for Clinical Investigation, Osaka University Hospital, Suita, Osaka, Japan; 4Division of Infection Control and Prevention, Tohoku Pharmaceutical University Hospital, Sendai, Japan
*These authors contributed equally to this work
Abstract: Surveillance is very important to prevent the nosocomial spread of methicillin-resistant Staphylococcus aureus (MRSA), and infection sources and routes have historically been identified using molecular and epidemiological genotyping with pulsed-field gel electrophoresis. However, phage-open reading frame typing (POT) has recently been developed. Here, we investigated whether POT would be useful to survey MRSA outbreaks and transmission. We therefore applied POT to 91 MRSA isolates detected in cultures from inpatients at our hospital between May and October 2014. Among the 91 isolates, 12 POT types comprising 38 isolated MRSA strains were considered as overlapping. Five of them were detected in different wards, whereas the remaining seven were found in the same ward, including the emergency department. Three of seven POT number 93-155-111 strains were detected in the surgical ward, and all of four POT number 93-157-61 strains were detected in the cardiosurgical ward. These data suggested that transmission of the MRSA strains with the same POT-types from the same wards was nosocomial, and that POT accurately and rapidly identified MRSA strains, which allowed effective control of infection and transmission.
Keywords: MRSA, active surveillance, POT, nosocomial transmission
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) has become a leading cause of hospital infections with high mortality rates due to MRSA bacteremia.1,2 Therefore, the surveillance of patients admitted to hospital for MRSA, usually via nasal swabs, is important.3,4 Active surveillance involves the detection and tracking of asymptomatic patients who are MRSA carriers; moreover, compelling data support to identify carriers and using contact precautions for both carriers and infected patients to reduce the spread of MRSA within hospitals and to decrease the rates of hospital-acquired MRSA infections.5
Pulsed-field gel electrophoresis (PFGE) of chromosomal DNA digested with restriction enzymes has been one of the most reliable tools for determining MRSA transmission, but phage-open reading frame typing (POT) has recently been developed for genotyping based on multiplex polymerase chain reactions (PCRs).6 This method has been applied to investigate nosocomial MRSA outbreaks, and it has high discriminatory power.7,8 Moreover, a commercial POT kit has become available in Japan, which has simplified the process.9
Here, we analyzed MRSA isolates from admitted patients and the distribution of their POT types in our hospital, and found overlapping cases suggestive of nosocomial transmission.
Materials and methods
Hospital and patient setting
The first isolate of MRSA from each affected patient in our 1,076 bed university hospital was prospectively collected between May and October 2014 and stored at −80°C. All MRSA strains were recovered on trypticase soy broth plates containing 6 mg/L oxacillin (Sigma-Aldrich Co, St Louis, MO, USA) and sub-cultured in drug-free Luria-Bertani broth.
Inpatients were defined as the patients who stayed at our hospital more than 2 days. Emergency departments in Japan are different from those in the United States; they are closer to an outpatient setting with access to inpatient facilities, and they include a critical care unit.
Samples of nasal swabs for MRSA culture were taken on admission and every 7 days thereafter. Therefore, “imported” means that MRSA was isolated on admission (usually within 48 hours), in contrast, in the case that MRSA was not isolated on admission, but isolated at 48 hours after admission (usually 7 days later) was called “acquired”.
The Research Ethics Committee of Osaka University approved this study (accession number 11159).
Genotyping using the POT kit
The POT methodology was originally described by Suzuki et al.10 We used the Cica Geneus Staph POT KIT (Kanto Chemical, Tokyo, Japan) according to the manufacturer’s instructions to analyze MRSA isolates from our patients. In brief, the POT kit comprised three multiplex PCRs with two reaction mixtures, and the output was determined by the presence or absence of 22 targets (Table 1). The band size of these products was estimated by the positive control of mixtures 1 and 2 as in Table 1; therefore, we could confirm each band size without DNA molecular markers after the first electrophoresis was performed. The results are expressed as three POT scores calculated in a binary manner. According to the manufacturer, the target of the POT kit also includes small genomic islets and SCCmec elements. Based on the manufacturer’s insert for the POT kit, we anticipated that the presence or absence of POT1-1, POT1-2, POT1-3, POT1-4, and POT1-7 targets would predict SCCmec types I–VI.11
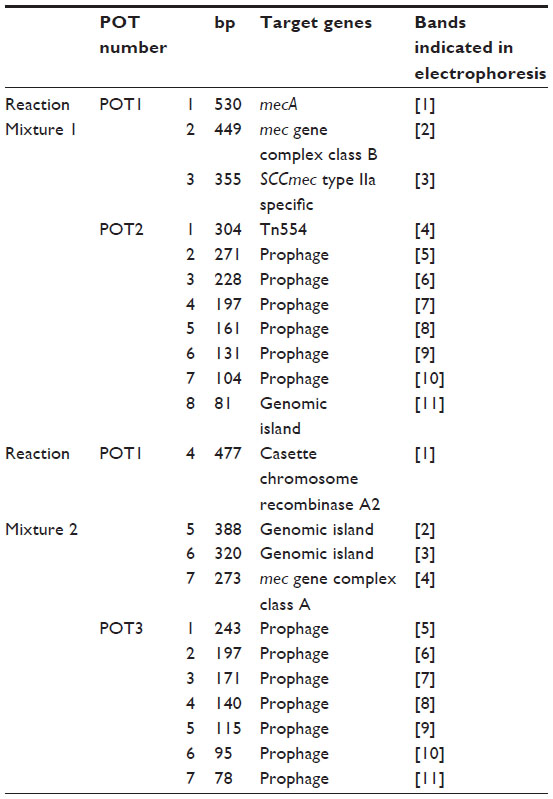 | Table 1 Target genes of the kit for POT typing |
Results
POT types and overlapping cases
We analyzed the POT types of 91 MRSA isolates and the characteristics of the patients. The POT types were estimated by each electrophoretic analysis of 12 PCR products including S. aureus specific femA gene (Figure 1). Suitably sized amplicons were found for each isolate. We translated the electrophoretic data to POT numbers, and determined the POT type of each isolate.
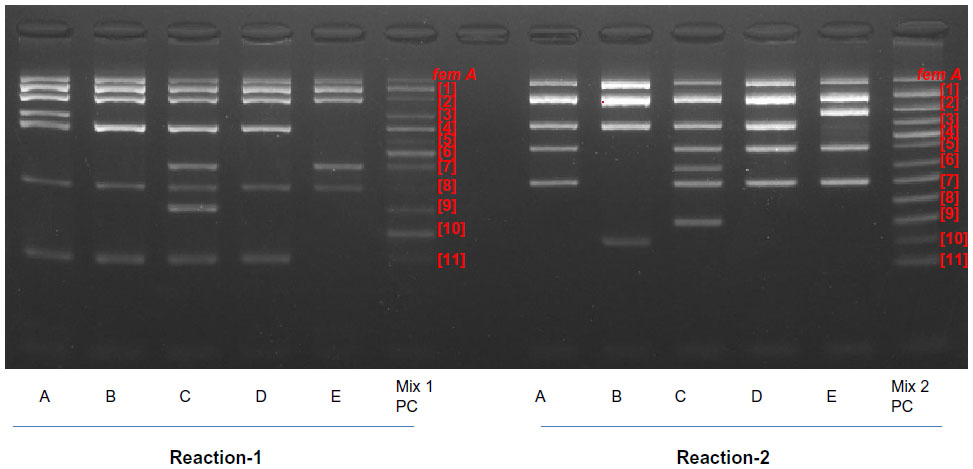 | Figure 1 Representative phage-open reading frame typing electrophoretic profiles. |
Among 91 isolates, 38 strains were shown and found as 12 overlapped POT types (Tables 2 and 3). Seven of the 12 overlapping POT types were found in the same wards as follows: POT numbers 106-137-2, 106-137-80, and 106-9-2 (n=2 each) were isolated from the emergency ward, POT number 93-191-125 (n=2) was isolated from the dermatology ward, and POT number 93-213-109 was isolated from the neurology ward. In addition, two and three isolates with POT number 93-155-111 types were from the otolaryngological and surgical wards, respectively. All strains with POT number 93-157-61 (n=4) were isolated only from the cardiosurgical ward (Table 3). We found more than one overlapping POT type in the emergency, dermatology, neurological, otolaryngological, surgical, and cardiosurgical wards.
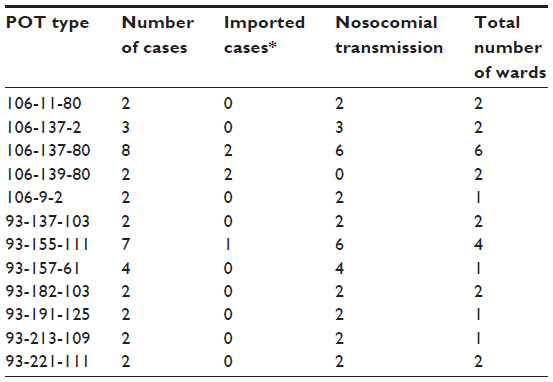 | Table 2 Overlapping POT types |
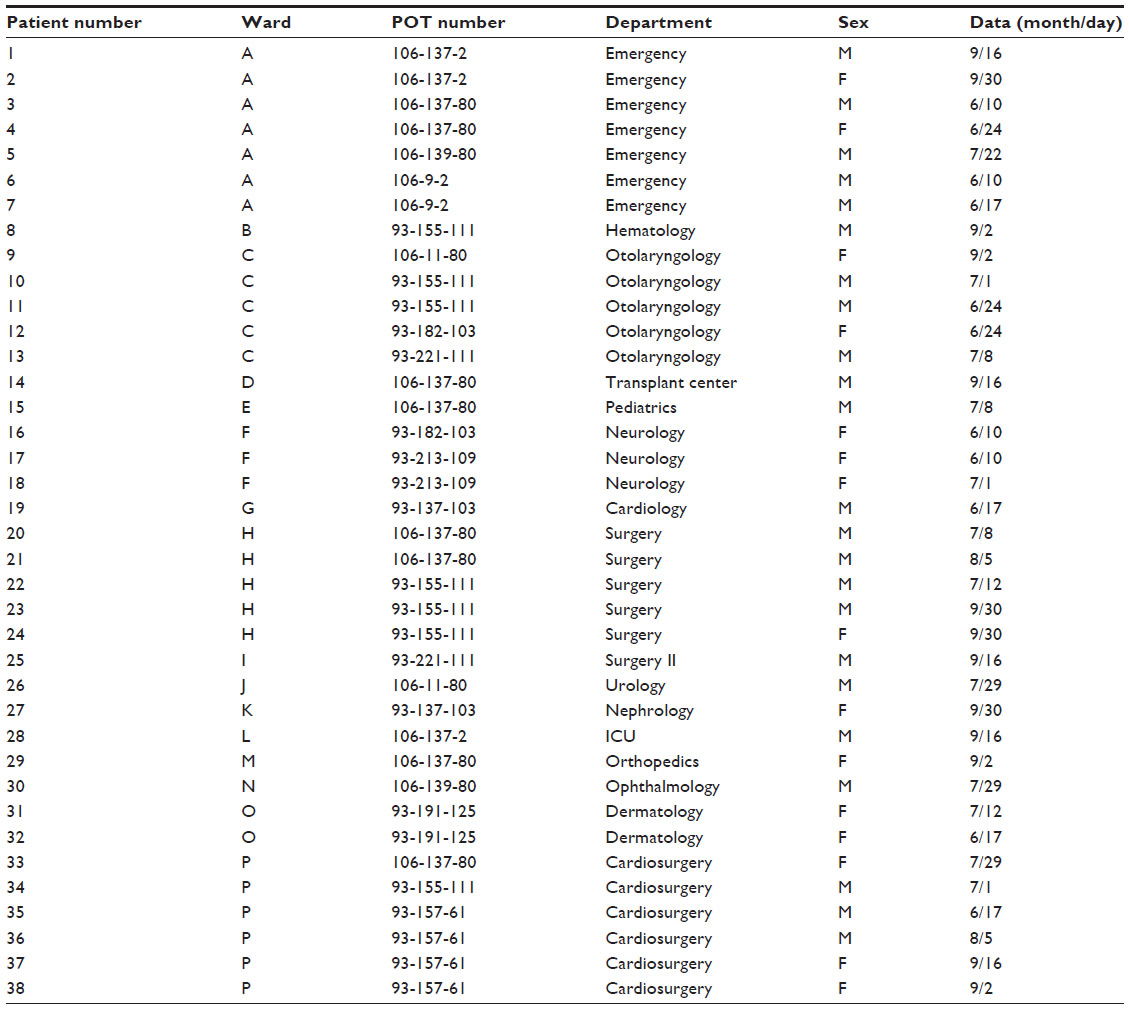 | Table 3 Profiles of patients defined as having nosocomial infection |
These overlapping isolates from the same wards were detected within approximately 1 month, which suggested nosocomial transmission within the wards.
In addition, POT number 93-155-111, POT number 106-137-80, POT number 106-137-2, and POT number 93-155-111 were isolated on the same day. Among them, POT number 93-155-111 was also isolated from the same ward (surgical ward) and it suggested this POT type was potentially brought into the surgical ward from the other wards by the patients or the medical staff. The other three POT types were isolated on the same day, but from different wards. These results suggested that these three POT types may have spread and been circulating in our hospital.
Discussion
We analyzed MRSA nosocomial transmission using POT genotyping. The POT kit, especially the POT1 score, predicted SCCmec type and closely correlated with other standard genotyping methods such as multilocus sequence typing.9 The discriminatory power of the POT kit should be higher than that of other genotyping methods including PFGE as shown in a previous study of a nosocomial outbreak in which the findings of the POT kit closely correlated with those of other genotyping methods.12
We found that 12 POT types comprising 38 of 91 isolated MRSA strains were overlapped. Five of 12 overlapping POT types were detected in the different wards, but the other seven of 12 overlapped POT types were from the same wards. More than one overlapping POT type was identified in the emergency, dermatology, neurological, otolaryngological, surgical, and cardiosurgical wards, indicating that these locations were the sources of the nosocomial MRSA transmission.
The cause of nosocomial transmission is usually explained as ineffective precautions and lower standards, but unique and specific situations are occasionally suspected.
For example, we previously described that nosocomial transmission and outbreaks of multi-drug resistant Pseudomonas aeruginosa occurred during transesophageal echography in cardiosurgical wards and with the use of bronchoscopes in the intensive care unit.13,14
We could not culture MRSA from these devices, although we suspected that otolaryngeal scopes were the cause of MRSA transmission, and MRSA became undetectable in the otolaryngological wards after intervention by our infection-control team, especially the handling and washing process of the otolaryngeal scopes when we discovered the outbreak of MRSA in this ward. The specific situations of wards where outbreaks occur should be analyzed, and immediate intervention should be applied similar POT-type drug-resistant bacteria, including MRSA isolated from the same wards. This was one of the cases that showed the usefulness of the POT kit.
Because the POT kit consists of two multiplex PCR reactions and electrophoresis can be accomplished within 6 hours without nucleotide sequencing, its simple and rapid platform is promising for not only investigations of outbreaks but also for non-outbreak epidemiological surveillance. The POT types of MRSA can be routinely analyzed in the clinical laboratory using POT kits. We plan to apply not only the numbers of MRSA isolation, but also their POT type information to call medical staff’s attention to MRSA spread and circulating problems in our hospital in the near future. Further analysis and practical use is needed.
The current study has limitations. Information about the clinical diagnosis or disease severity was not addressed. In addition, the short-term study proceeded at a single institution. Nevertheless, we consider that the epidemiological findings demonstrated that the POT method is useful.
In conclusion, we validated the new POT kit as a practical genotyping tool for MRSA surveillance, especially active surveillance to protect against nosocomial outbreaks. Our data will expand the database of epidemiological information on MRSA at our hospital, as well as in the region and nationwide.
Disclosure
This study was supported by Grant-in-Aid for Scientific Research 26461158 (to MS) from the Japanese Society for Promotion of Science. The authors have no other conflicts of interest to disclose.
References
American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416. | |
Isobe M, Uejima E, Seki M, et al. Methicillin-resistant Staphylococcus aureus bacteremia at a university hospital in Japan. J Infect Chemother. 2012;18(6):841–848. | |
Taguchi H, Matsumoto T, Ishikawa H, Ohta S, Yukioka T. Prevalence of methicillin-resistant Staphylococcus aureus based on culture and PCR in inpatients at a tertiary care center in Tokyo, Japan. J Infect Chemother. 2012;18(5):630–636. | |
Takahashi Y, Takesue Y, Uchino M, et al. Value of pre- and postoperative meticillin-resistant Staphylococcus aureus screening in patients undergoing gastroenterological surgery. J Hosp Infect. 2014;87(2):92–97. | |
Ghazal SS, Hakawi AM, Demeter CV, Joseph MV, Mukahal MA. Intervention to reduce the incidence of healthcare-associated methicillin-resistant Staphylococcus aureus infection in a Tertiary Care Hospital in Saudi Arabia. Infect Control Hosp Epidemiol. 2011;32(4):411–413. | |
Suzuki M, Tawada Y, Kato M, et al. Development of a rapid strain differentiation method for methicillin-resistant Staphylococcus aureus isolated in Japan by detecting phage-derived open-reading frames. J Appl Microbiol. 2006;101(4):938–947. | |
Nada T, Yagi T, Ohkura T, et al. Usefulness of phage open-reading frame typing method in an epidemiological study of an outbreak of methicillin-resistant Staphylococcus aureus infections. Jpn J Infect Dis. 2009;62(5):386–389. | |
O’Sullivan MV, Kong F, Sintchenko V, Gilbert GL. Rapid identification of methicillin-resistant Staphylococcus aureus transmission in hospitals by use of phage-derived open reading frame typing enhanced by multiplex PCR and reverse line blot assay. J Clin Microbiol. 2010;48(8):2741–2748. | |
Maeda T, Saga T, Miyazaki T, et al. Genotyping of skin and soft tissue infection (SSTI)-associated methicillin-resistant Staphylococcus aureus (MRSA) strains among outpatients in a teaching hospital in Japan: application of a phage-open reading frame typing (POT) kit. J Infect Chemother. 2012;18(6):906–914. | |
Suzuki M, Matsumoto M, Takahashi M, Hayakawa Y, Minagawa H. Identification of the clonal complexes of Staphylococcus aureus strains by determination of the conservation patterns of small genomic islets. J Appl Microbiol. 2009;107(4):1367–1374. | |
Kondo Y, Itoh T, Ma XX, et al. Combination of multiplex PCRs for staphylococcal cassette chromosome mec type assignment: rapid identification system for mec, ccr, and major differences in junkyard regions. Antimicrob Agents Chemother. 2007;51(1):264–274. | |
Moriyama H, Matsuda C, Shibata H, Nishimura N, Hirose M, Nagai A. [Usefulness of phage ORF typing, a rapid genotyping method as a molecular and epidemiological method for detecting methicillin resistant Staphylococcus aureus]. Kansenshogaku Zasshi. 2012;86(2):115–120. Japanese. | |
Seki M, Machda H, Yamagishi Y, Yoshida H, Tomono K. Nosocomial outbreak of multidrug-resistant Pseudomonas aeruginosa caused by damaged transesophageal echocardiogram probe used in cardiovascular surgical operations. J Infect Chemother. 2013;19(4):677–681. | |
Machida H, Seki M, Yoshioka N, et al. Correlation between outbreaks of multidrug-resistant Pseudomonas aeruginosa infection and use of bronchoscopes suggested by epidemiological analysis. Biol Pharm Bull. 2014;37(1):26–30. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.