")
Back to Journals » Journal of Blood Medicine » Volume 5
Update on argatroban for the prophylaxis and treatment of heparin-induced thrombocytopenia type II
Authors Grouzi E
Received 11 February 2014
Accepted for publication 8 July 2014
Published 13 August 2014 Volume 2014:5 Pages 131—141
DOI https://doi.org/10.2147/JBM.S38762
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Elisavet Grouzi
Department of Transfusion Service and Clinical Hemostasis, “Agios Savvas” Regional Cancer Hospital, Athens, Greece
Abstract: Heparin-induced thrombocytopenia (HIT) is a rare but potentially severe complication of heparin therapy that is strongly associated with venous and arterial thrombosis (HIT and thrombosis syndrome, HITTS), which requires urgent detection and treatment with a nonheparin anticoagulant. Argatroban, a synthetic direct thrombin inhibitor, is indicated for the treatment and prophylaxis of thrombosis in patients with HIT, including those undergoing percutaneous coronary intervention. Argatroban has a relatively short elimination half-life of approximately 45 minutes, which is predominantly performed via hepatic metabolism. It is derived from L-arginine that selectively and reversibly inhibits thrombin, both clot-bound and free, at the catalytic site. Argatroban anticoagulation has been systematically studied in patients with HIT and HITTS and proved to be a safe and effective agent for this indication. The current review presents the pharmacology of argatroban, data regarding monitoring of the agent, and an overview of the results of the major clinical trials assessing argatroban anticoagulation in HIT patients. Additionally, data from recent clinical trials with argatroban use in more special indications such as in percutaneous coronary intervention, liver dysfunction, renal replacement therapy, and intensive care medicine, are reviewed. The approved initial dosage of argatroban for adults with HIT or HITTS is 2 µg/kg/minute for patients with normal hepatic function and 0.5 µg/kg/minute for patients with hepatic dysfunction. There is evidence that a reduced initial dose may also be advisable for patients with heart failure, multiple organ dysfunction, severe anasarca, or after cardiac surgery. Given this information, argatroban can be effectively used in treating HIT with monitoring of activated partial thromboplastin time.
Keywords: argatroban, HIT, direct thrombin inhibitor
Introduction to the clinical problem of HIT type II
Heparin-induced thrombocytopenia (HIT) is a side effect of unfractionated heparin (UFH) and of low molecular weight heparin (LMWH) as well, and it is distinguished into two clinical forms, HIT type I and HIT type II. HIT type I is a benign nonimmune form with a reversible mild thrombocytopenia, which usually resolves despite persistent heparin treatment.1–3 On the other hand, HIT Type II is the most severe complication of heparin therapy; it is an immune-mediated drug adverse reaction that is associated with a high risk of venous and arterial thrombosis (HIT and thrombosis syndrome, HITTS), despite a low platelet count. It is this type that may lead to severe thrombosis, amputation, and in some cases death. For the purpose of this review, the term HIT refers to the immune-mediated type II that can cause paradoxical thrombosis, as it is usually refered in the recent literature.
It is well known that HIT is a prothrombotic condition mediated most frequently by immunoglobulin G platelet-activating antibodies (often called “HIT antibodies”) against multimolecular complexes of the platelet factor 4 (PF4) and heparin, which form on the surface of platelets.1–8 The resultant multimolecular immune complexes bind to the FcγIIa (immunoglobulin G) receptors of platelets,6 inducing platelet activation, release of procoagulant platelet-derived microparticles, platelet consumption, and thrombocytopenia.3 The final result of the process is marked generation of thrombin, which can cause venous and arterial thromboses that are the clinical hallmark of HIT. The antibody–antigen complexes also activate monocytes, leading to tissue factor production and endothelial injury, which contributes further to thrombosis.2,6,9,10
Thrombocytopenia usually occurs 5–14 days after first introduction of heparin therapy. However, there are exceptions, with HIT at times developing either early, namely after a recent previous exposure to heparin, or late after heparin exposure. For patients receiving heparin or having received heparin within the previous 2 weeks and for whom their clinicians consider the risk of HIT to be >1%, the American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (9th Edition) suggest that platelet count monitoring must be performed every 2–3 days from day 4 to day 14 (or until heparin is stopped, whichever occurs first).8 Patients at >1% risk of HIT are postoperative patients receiving prophylactic or therapeutic doses of UFH and cardiac surgery patients. Guidelines from the Haemostasis and Thrombosis Task Force of the British Committee for Standards in Haematology suggest almost the same course of action, with the addition that patients who are to receive any heparin should have a baseline platelet count.7
The risk of HIT is related to the type of heparin used, the clinical characteristics of the patient, and his/her medical history.3,5,10 It can occur after any exposure to heparin, including heparin flushes and heparin-coated catheters. Surgical patients have a higher risk than medical patients, possibly because of the release of cytokines during tissue injury.2,5,8,10 Older patients, women, and patients undergoing orthopedic surgery are at increased risk. On the other hand, the recent observation that HIT antibodies can develop in healthy persons after exposure to heparin suggests that some people may be predisposed to antibody formation.11 Moreover, B-cell tolerance to epitopes recognized by HIT antibodies is probably established early in life, possibly explaining why only 3% of patients given heparin experience HIT. Just recently, data from an experimental study suggest that PF4/heparin-specific B-cell tolerance can be broken down by an inflammatory stimulus.12 Thus, the inflammatory milieu associated with tissue trauma may account for the increased incidence of HIT antibodies and clinical HIT in patients given heparin during cardiac surgery or orthopedic surgery. This fact is consistent with the previously observed atypical immune-response features of HIT patients, such as rapid generation and loss of anti-PF4/heparin antibodies produced by most patients exposed to heparin for the first time.12,13
The risk of HIT is also related to the duration of heparin exposure and the length of the heparin molecule.1,2,5,10 The UFH (molecular weight 3.000–30.000 Da) carries a higher risk (1.0%–5.0%) than LMWH (molecular weight 2.000–9.000 Da), which is associated with a risk of 0.1%–1.0%. Fondaparinux (molecular weight 1.700 Da) is associated with a negligible risk of heparin-induced thrombocytopenia. In a recent multicenter randomized trial comparing UFH with LMWH (dalteparin) for thromboprophylaxis in 3,746 critically ill patients, only 17 patients (0.5%) developed HIT based on serotonin-release assay-positive result.14 HIT-associated thrombosis occurred in ten of 17 patients (58.8%) (8:1:1 venous:arterial:both). Moreover, HIT antibodies examined by enzyme-linked immunosorbent assay were less frequent among patients receiving dalteparin versus UFH (13.5% versus 27.3%, P<0.001).
Thrombocytopenia is common in hospitalized patients receiving UFH, but only a minority develop HIT. However, rapid and accurate diagnosis is paramount to avoid the perils of misdiagnosis.10,15 Clinical evaluation may be guided by scoring systems such as the 4Ts pretest clinical score and HIT Expert Probability score.16,17 Laboratory tests include immunoassays, such as the PF4/heparin enzyme-linked immunosorbent assay, and functional tests such as the 14C-serotonin release assay and heparin-induced platelet activation assay.7,8,15 The commercially available immunoassays are most widely accessible to the clinicians because they can be done in most hospital laboratories; they have high sensitivity but modest specificity, especially if the test is only marginally positive. Moreover, the functional assays are more specific, but they are technically demanding. Recently, Cuker15 proposed an evidence-based Bayesian approach to the diagnosis of HIT that integrates the 4Ts score and immunoassay testing – the two most widely used diagnostic tools in current practice – to facilitate estimation of the posttest probability of HIT and possibly to guide clinical decision making.
HIT may have life-threatening complications, such as deep-vein thrombosis, pulmonary embolus, myocardial infarction, cerebral sinus thrombus, stroke, adrenal vein thrombosis, limb gangrene, and acute limb ischemia. Venous thrombotic events predominate over arterial events in a ratio of 4:1.3,10 Less-common manifestations include acute systemic reaction and necrotizing lesions at the heparin-injection sites. The mortality associated with heparin-induced thrombocytopenia is approximately 5%–10%, usually secondary to thrombotic complication.5,10 Without alternate anticoagulation, the risk of thromboembolic complication can be seen in 30%–75%.18,19
Management of HIT is thus essential for a patient’s life and entails cessation of all forms of heparin and LMWH (including heparin flushes and heparin-coated catheters).2,7,8 It is a general principle that for patients with suspected (non-low pretest probability) or confirmed HIT, heparin should be stopped and full-dose anticoagulation with an alternative nonheparin anticoagulant should be commenced. The direct thrombin inhibitors (DTIs), such as argatroban, bivalirudin, and lepirudin, are a class of potent anticoagulants that are emerging in current anticoagulation therapy and are effective in the treatment of HIT-induced thromboembolism and as alternative anticoagulants for thrombosis prophylaxis in patients diagnosed with HIT. Moreover, other agents such as fondaparinux are increasingly being used on the basis of successful clinical experience.20 However, the choice of alternative anticoagulant is primarily driven by comorbidities and half-life considerations, and by the availability of agents in each country. The use of parenteral DTI is preferred in the case of a critically ill patient, often due to the need for procedural interventions and/or underlying bleeding risk; a shorter half-life is desirable for these patients, given potential hemorrhage and lack of an antidote. The half-lives of lepirudin, danaparoid, and fondaparinux are approximately 80 minutes, 24 hours, and 17–20 hours, respectively.8,10
Argatroban is approved by the US Food and Drug Administration and is licensed in Canada, Japan, and several European countries for prophylaxis and treatment of thrombosis in adult patients with HIT. It is also used as an adjunct therapy for percutaneous coronary intervention (PCI) in patients who have or are at risk of thrombosis due to HIT. However, argatroban is the only nonheparin anticoagulant currently approved in the United States for the treatment of HIT; although lepirudin is approved for use in HIT, production was halted for commercial reasons in Europe in 2011 and in North America in 2012.10,21,22 Danaparoid was withdrawn from the US market by the manufacturer in 2002 because of a short supply, but it is available in Canada, Japan, Europe, and Australia.10 All this makes the knowledge of pharmacological properties of the nonheparin anticoagulant significantly important, as their selection for clinical use is dependent on both their properties and their current availability in each country. The current review examines the pharmacological characteristics and the clinical efficacy and the safety of Argatroban in adults with HIT, including those undergoing PCI.
Argatroban: pharmacology and pharmacokinetics
Argatroban is a synthetic DTI derived from L-arginine that selectively and reversibly binds to the thrombin active site, inhibiting its catalytic activity.10,18,22–26 It is a small molecule (molecular weight approximately 500 Da) that inhibits thrombin, both free and clot-associated, because it acts independently of antithrombin, like the other DTIs. Argatroban exerts its anticoagulant effects by suspending thrombin-catalyzed or thrombin-induced reactions, such as activation of coagulation factors V, VIII, and XIII; fibrin formation; activation of protein C; and platelet aggregation. Argatroban is highly selective for thrombin and has little or no effect on related serine proteases (trypsin, factor Xa, plasmin, and kallikrein).25 These pharmacological properties are distinctly different from those of heparin, which has a reduced capacity for inhibition of clot-bound thrombin.26
Argatroban is hepatically metabolized by hydroxylation and aromatization, mainly by the liver microsomal cytochrome P450 enzymes CYP3A4/5, to four main metabolites, which do not possess relevant pharmacological activity. It is then eliminated in the feces through biliary excretion.22,24,25 Therefore precaution is needed in patients with hepatic impairment due to decreased clearance. In such cases, it is not entirely contraindicated but dose adjustment is recommended. Renal elimination of argatroban is minimal, and the pharmacodynamic and pharmacokinetic parameters of argatroban are comparable between healthy subjects and individuals with renal insufficiency. Therefore, no initial dosage adjustment is required in patients with renal impairment.
When argatroban is administered by continuous intravenous (IV) infusion, it exhibits linear pharmacokinetic behavior, and steady state levels of both drug and anticoagulant effects are attained within 1–3 hours after the start of an infusion and remain stable until infusion discontinuation or dosage adjustment. In healthy volunteers and cardiac patients, the argatroban dose dependently increases the activated partial thromboplastin time (APTT), the activated clotting time (ACT), the prothrombin time, the international normalized ratio (INR), and the thrombin time.22,23,25 However, the ecarin clotting time yields a more linear dose response, but this test is not widely available in hospital laboratories and has not been standardized.24
The elimination half-life of argatroban in healthy subjects is about 45 minutes (range, 30–51 minutes), with a corresponding decline in its anticoagulant effects, which reach their pretreatment level within 2–4 hrs after cessation of an infusion, compared with at least 6 hours (and up to 20 hours) in patients with hepatic impairment.2,8,18,22,27 In a special population study of five patients with moderate hepatic impairment (Child-Pugh score >6), compared with 12 healthy volunteers receiving argatroban at 2.5 μg/kg/minute, hepatic impairment was associated with approximately fourfold decreased systemic clearance and threefold increase in elimination half-life of argatroban.28
Argatroban lacks major drug–drug interactions with CYP3A4/5 inhibitors such as erythromycin, acetaminophen, and digoxin.22 However, there is a very recent case report in which a severe decrease of cyclosporine levels was described in a 60-year-old patient receiving argatroban after a second heart transplant. Possible mechanisms of interaction are considered, such as an analytical interference, an idiopathic hemodilution, an increase of renal and hepatic clearance, and a metabolic drug–drug interaction.29 Furthermore, there have been several studies that characterize the pharmacokinetic and pharmacodynamic properties of argatroban in vulnerable patient groups, ie, elderly patients and patients with renal and/or hepatic dysfunction. The only effect of age or sex was an approximately 20% lower clearance in elderly men versus elderly women, which does not translate into clinically or statistically significant differences in pharmacodynamic response.28
Argatroban dosing and monitoring
In adult patients with HIT or HITTS without liver impairment, argatroban is given as a continuous IV infusion. Usual initial dosing is 2 μg/kg/minute adjusted to steady-state APTT 1.5–3.0 times initial baseline value, which cannot surpass 100 seconds, and no initial bolus is needed. It commences after cessation of heparin therapy and after determining baseline APTT, (Table 1). The APTT should be performed 2 hours after the initiation of infusion and after every dosage adjustment until the steady-state APTT is 1.5–3.0 times the initial baseline value. Nevertheless, the maximum dosage should not exceed 10 μg/kg/minute.2,8,18,22,23,25
 | Table 1 Licensed or suggested dosing schedules for treatment of HIT with argatroban |
In adult patients with HIT or HITTS undergoing PCI, argatroban infusion should be started after determining the baseline ACT. As is proposed from the historical control trials,30 it is given at an IV bolus of 350 μg/kg administered over 3–5 minutes and then at continuous IV infusion 25 μg/kg/minute, to achieve a therapeutic ACT of 300–450 seconds. The ACT test should be performed 5–10 minutes following the bolus dose. If it is necessary to achieve this therapeutic range, the maintenance infusion dose can be titrated (15–40 μg/kg/minute) and/or an additional bolus dose of 150 μg/kg could be given. When a therapeutic ACT (between 300–450 seconds) has been reached, this infusion dose should be pursued during the procedure. In case of impending abrupt closure, thrombus formation during the procedure, or inability to achieve or maintain an ACT >300 seconds, additional bolus doses of 150 μg/kg may be given and the infusion dose could be raised to 40 μg/kg/minute. The ACT should be monitored after each additional bolus or change in the rate of infusion. Additional ACTs should be performed about every 20–30 minutes during a prolonged procedure and at the end of a PCI procedure. If a patient requires anticoagulation after the procedure, argatroban may be continued at lower infusion dosages as those are recommended for patients with HIT or HITTS.8,23,25,30
As is recommended by the manufacturer, for adult patients with HIT or HITTS and hepatic impairment, the initial infusion dosage should be reduced to 0.5 μg/kg/minute and APTT should be checked closely. Similarly, in adult patients with HIT or HITTS and hepatic impairment who are undergoing PCI, argatroban dosages should be titrated carefully to obtain therapeutic ACTs.25 Furthermore, the use of high doses of argatroban should be avoided in PCI patients with clinically significant hepatic disease or alanine aminotransferase/aspartate aminotransferase levels ≥3 times the upper limit of normal. It may also be advisable for a reduced initial dose to be given to patients with conditions associated with hepatic congestion, which may potentially decrease argatroban clearance, as well as to patients with heart failure, multiorgan failure, or severe anasarca, or after cardiac surgery.19,25,27,31,32 Based on these reports, the American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (both eighth and ninth editions) and the British Guidelines suggest initial dosages of argatroban at 0.5–1.2 μg/kg/minute in the clinical settings listed above.2,7,8 Nevertheless, as we shall discuss later, lower dosages may be considered for some patients.33 Moreover, as already mentioned, no initial dosage adjustment is required in patients with renal impairment where there are none of the aforementioned conditions.2,8
Transition from argatroban to warfarin
When switching to vitamin K antagonists (VKAs) therapy after argatroban treatment, the possibility of combined effects of argatroban and warfarin (or other VKA) on INR measurements should be taken into consideration. It is well known that argatroban in therapeutic doses has the greatest effect on the INR among the other DTIs. Therefore it is suggested that when a VKA is introduced, argatroban and VKA therapy should be overlapped to avoid prothrombotic effects and to ensure continuous anticoagulation for the initial period of VKA treatment. Warfarin and argatroban should be overlapped for at least 5 days and an INR of ≥4 should be monitored for 2 consecutive days before argatroban is discontinued. An upper range target for the INR in this situation is not given, but at very high INR levels the patient may be over-anticoagulated. It is recommended that, at an INR >5, the argatroban infusion should be discontinued for 4 hours and the INR should be repeated.7,8,25 Another option is to monitor the VKA with a chromogenic factor X assay. In this setting, factor X levels <45% have been associated with INR values >2 when the effect of argatroban has been eliminated. Monitoring factor X levels may be safer than aiming for an INR ≥4 when VKAs are given in conjunction with argatroban.24
Argatroban: efficacy, tolerability, and side effects
The data describing the role of argatroban in HIT are obtained from two multicenter, prospective, nonrandomized open-label studies (ARG-911 and ARG-915),34,35 where it was compared with historical controls for efficacy of the drug, which is most often treated by cessation of heparin alone or substitution of heparin with oral anticoagulation using VKA. This is due to the fact that when these studies were carried out, no approved alternative agent was available for use as an active comparator. The studies enrolled adult patients with either isolated HIT or HITTS. The quality of these studies has been criticized because of the fact that about one third of the patients included in the analysis were found to be HIT antibody negative upon retrospective testing,36 and some of the patients included had a remote rather than an immediate history of HIT. Afterwards, Lewis et al37 again retrospectively analyzed thrombotic outcomes in 882 HIT patients (697 patients receiving mean argatroban doses of 1.7–2.0 μg/kg/minute for 5–7 days to achieve an APTT of 1.5–3.0, plus 185 historical control subjects) from previously reported prospective studies (Table 2). In this study argatroban treatment resulted in a significant reduction in the primary end point of a composite risk of death due to thrombosis, amputation secondary to HIT-associated thrombosis, or new thrombosis within 37 days of baseline for both patients with HIT without thrombosis at diagnosis (hazard ratio [HR] =0.33; 95% confidence interval [CI] =0.2–0.54; P<0.001) and with thrombosis at diagnosis (HR =0.39; 95% CI =0.25–0.62; P<0.001). More argatroban-treated patients remained thrombosis-free during the 37-day follow-up, again for patients both with and without thrombosis at the time of diagnosis, and fewer died from thrombosis (P<0.001).7,37 However, there were concerns due to the fact that there was no significant effect of argatroban on amputation secondary to HIT-associated thrombosis. A retrospective analysis of 21 of the amputation events in the prospective studies of argatroban in HIT found that severe ischemia or gangrene was present in 98% of the amputated limbs before argatroban was started, and that amputation was already planned for most patients.38 Hence, a reduction in amputation rate could not have been expected. Furthermore thrombotic risks were two times higher in nonwhite than in white patients, 1.7 times higher in female than in male patients with HIT and thrombosis, and were increasing as the body weight or platelet count were decreasing.37
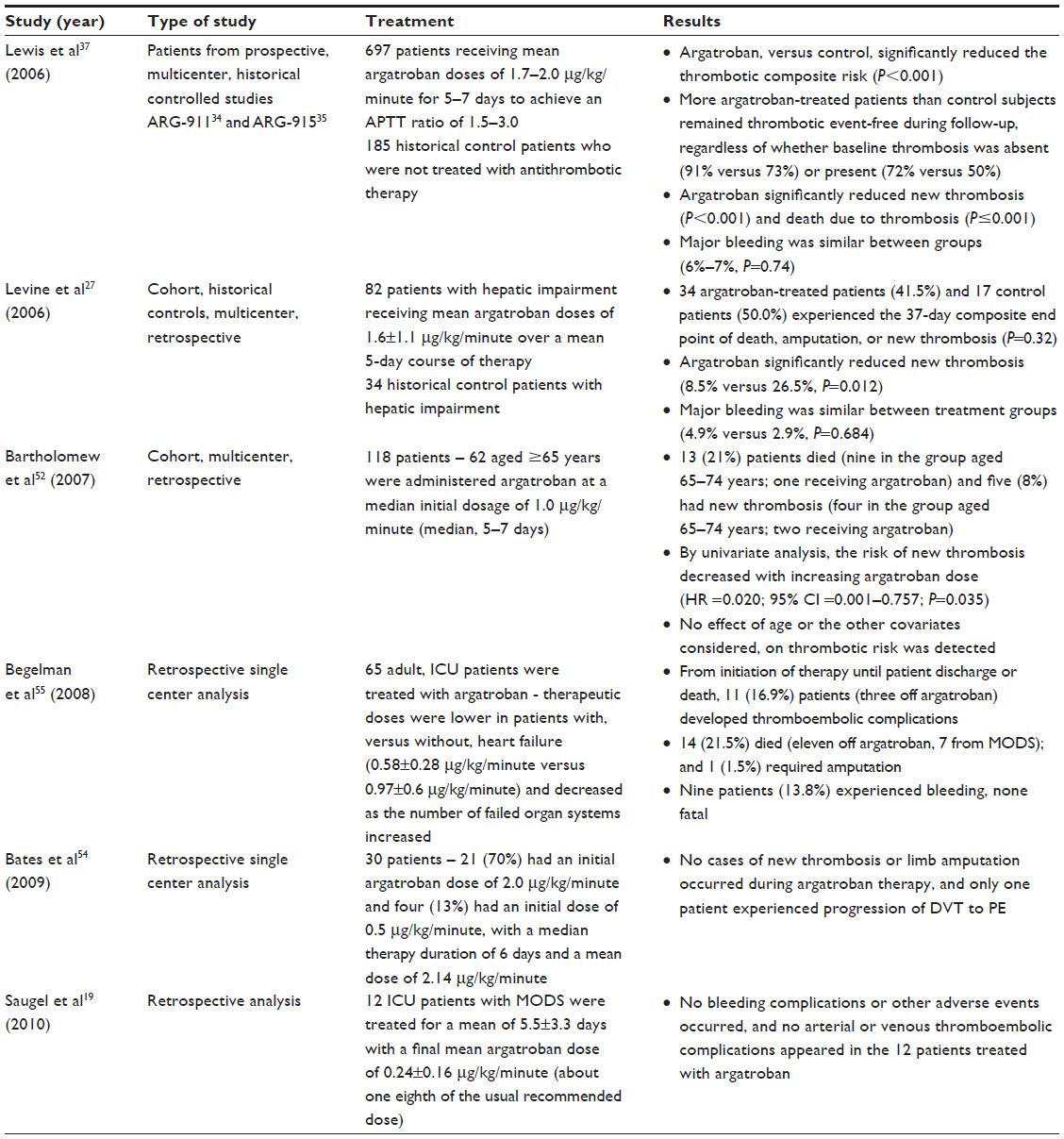 | Table 2 Summary of findings from the most recent studies for argatroban for treatment of HIT/HITT |
Like all other anticoagulant drugs, argatroban is contraindicated in patients with overt major bleeding. Particular vigilance is needed during its use in conditions or circumstances that increase the risk of hemorrhage, such as severe hypertension, immediately following lumbar puncture, spinal anesthesia, and major surgery, especially brain, spinal cord, or eye surgery. Special caution should be exercised in patients with hematological conditions associated with increased bleeding diathesis, such as congenital or acquired bleeding disorders, and gastrointestinal lesions such as ulcerations.23,25 There is no known specific antidote for overdose of argatroban. Therefore if excessive plasma concentrations of argatroban are suspected or life-threatening bleeding occurs, therapy should be stopped immediately, APTT should be performed, and symptomatic treatment should be administered to the patient. In the aforementioned study, major bleeding, defined as a fall in hemoglobin of ≥2 g/dL, or as having led to transfusion of ≥2 units of red blood cells, or that was into the central nervous system, retroperitoneum, or a prosthetic joint, was similar in both groups with no significant excess in the argatroban recipients.7 Furthermore, although recombinant factor VIIa can reverse the anticoagulant effect of DTIs in healthy volunteers, the usefulness of this agent in patients who are bleeding has not been established, while hemodialysis or hemoperfusion can remove argatroban.24
As regards the comparison between argatroban and lepirudin for efficacy and safety, they have been directly compared only in small retrospective cohort studies.39–41 But comparison across these studies is quite problematic because the primary outcome measures differed, and the outcomes that have been identified as important were not consistently reported. Furthermore, the doses of argatroban and lepirudin given in these retrospective studies were lower than the doses given in the historical controlled trials.34,35 The bleeding risk of these agents was reported in two of these studies. In particular, Kiser et al41 reported that significant bleeding occurred in 6% of patients taking argatroban and 5% of patients taking lepirudin. However, in the other study conducted by Smythe et al39 important bleeding has been shown in 11.5% of patients taking lepirudin and 10.3% of patients taking argatroban. However, an additional factor that needs to be considered is that in 30% of patients, antibodies develop against lepirudin after the first exposure and in 70% of patients upon second exposure. Severe and in some cases fatal reactions have been reported following lepirudin sensitization. For this reason, lepirudin should be used only once during a patient’s lifetime.42–44 As a result of antibody formation, renal clearance of lepirudin is delayed, leading to accumulation, which may place the patient at increased risk of bleeding. Lepirudin antibodies also display cross-sensitivity to bivalirudin. Therefore, it is recommended that bivalirudin be avoided in patients who previously received lepirudin.
Argatroban was evaluated as anticoagulant therapy in HIT patients who underwent PCI in three prospective, multicenter, historical controlled trials (ARG-216, ARG-310, and ARG-311). The studies – one studying dose confirmation and two evaluating efficacy and safety – were similarly designed with respect to patient inclusion and exclusion criteria, argatroban dosing regimen, primary efficacy outcomes, and recorded outcomes. In a secondary pooled analysis of these studies, the investigators analyzed the outcomes of 91 HIT patients who underwent 112 separate coronary interventions on a total of 177 treated lesions (149 in the initial group and 28 in the repeat group) while on intravenous argatroban (350 μg/kg initial bolus followed by 25 μg/kg/minute adjusted to reach an ACT of 300–450 seconds, as is described above).30 Eligible patients were males or nonpregnant females >18 years of age with a history of HIT supported by a previous or current positive HIT antibody test or a previous or current clinical diagnosis of HIT. Primary efficacy endpoints were assessments of the satisfactory outcome of the procedure and the achievement of adequate anticoagulation during PCI. Among patients undergoing initial PCIs with argatroban (n=91), 94.5% had a satisfactory outcome of the procedure and 97.8% achieved adequate anticoagulation. Across all trials, seven (7.7%) patients overall experienced myocardial infarction and/or revascularization at 24 hr after PCI (four patients and four patients respectively), while one patient (1.1%) had periprocedural major bleeding. For patients who had subsequent hospitalizations (for a mean time of 150 days) for reoperation using argatroban anticoagulation (n=21), there were no unsatisfactory outcomes.
Thereafter, in patients without HIT (n=152), argatroban alone, or in combination with glycoprotein IIb/IIIa inhibitors during PCI, was evaluated in a prospective cohort study without internal controls.45 The incidence of primary efficacy outcomes (death, Q-wave myocardial infarction, and urgent revascularization) and major bleeding was acceptably low in both groups (0%–3%).
Argatroban is a suitable regimen for use in renal replacement therapy (RRT), due to the fact that it is mainly eliminated via the liver, and moreover dialytic clearance by high-flux membranes is considered clinically insignificant.46 It can be used in both continuous and intermittent RRT (bolus 100 μg/kg and infusion 0.5 μg/kg/minute adjusted to achieve an APTT 1.5–3.0 times baseline, and bolus 250 μg/kg and infusion 2.0 μg/kg/minute adjusted to achieve an ACT 170–230 seconds, respectively).7 The use of argatroban during RRT in patients with HIT is evidence-based on a secondary analysis of prospective, historical, controlled treatment studies (47 patients with HIT and renal failure requiring RRT who underwent 50 treatments with argatroban)47 and from a second small prospective, dose-finding study in patients undergoing continuous RRT (n=30).48 The incidence of new thrombosis (0%–4%) and major bleeding (0%–6%) in patients who received argatroban in these studies was low. Furthermore, another randomized control trial evaluating three different doses of argatroban during intermittent RRT in patients without HIT (n=13) showed similar results.46
Argatroban: recent updates from clinical trials
Argatroban has been effectively utilized in critically ill intensive care unit (ICU) patients with multiple organ dysfunction (MODS) and diagnosed with HIT.19 In a retrospective analysis, 12 ICU patients with MODS were treated with argatroban for suspected or diagnosed HIT. The patients had a mean platelet count of 46.000±30.310/μL, a mean APACHE (Acute Physiology and Chronic Health Evaluation) II score of 26.7±7.8 on ICU admission, and a mean SAPS (Simplified Acute Physiology) II score of 61.5±16.3 on the first day of argatroban treatment. The results of this study suggest that patients with MODS and HIT can be effectively treated by using argatroban anticoagulation, although the clinician should be alert for diagnosing HIT in these complex patients. However, in critically ill patients with MODS, the dosing of argatroban has to be adjusted. To avoid excessive anticoagulation and bleeding complications, argatroban should be initiated at a markedly reduced dose of about one tenth to one eighth of the 2 μg/kg/minute recommended for ICU patients with MODS. Because achievement of steady-state anticoagulation will be delayed in this special patient population, APTT must be monitored at close intervals after drug commencement or dose change to ensure that the desired level of anticoagulation is achieved.
A retrospective study was recently done comparing the three DTIs (lepirudin, argatroban, or bivalirudin) approved for HIT management, in patients receiving RRT with a presumable diagnosis of HIT at the University of Pittsburgh Medical Center from January 1, 1995, through March 1, 2008.49 The primary outcome assessed was a triple composite end point of thrombosis, bleeding, and inhospital mortality. A secondary assessment compared the pharmacodynamic correlation between APTT and the triple composite end point. For the primary end point, there was no statistically significant difference observed among DTIs. In patients receiving RRT, lack of a previous heparin allergy, the degree of INR, and lower serum albumin were significantly correlated with increased morbidity and the occurrence of the composite end point. No differences in adverse events or other clinical outcomes were observed in this retrospective evaluation of DTI use in patients receiving RRT and with presumed HIT.
Another more recently published study evaluated the use of argatroban as an anticoagulant during continuous RRT in the early period after cardiac surgery.50 Argatroban was compared to UFH with respect to bleeding complications and the effectiveness of anticoagulation. Ninety-four patients requiring RRT after cardiac surgery from March 2007 to June 2009 were identified. The effectiveness of anticoagulation was measured indirectly by the duration of dialysis filter use. Bleeding was defined as clinical signs of blood loss or the need for transfusion. Of these patients, 41 received argatroban, 27 UFH, and 26 required conversion from UFH to argatroban. In all three subgroups, RRT initiated within a median postoperative period of 2.0 days. Similar levels of anticoagulation were achieved with the duration of the circuit, and filters were changed an average of 1.1 times daily during RRT. Liver function was similar in all patients. Neither clinically relevant signs of bleeding nor significant differences in the hemoglobin levels or a requirement for transfusion were noted. However, the SAPS II values during dialysis and mortality were significantly greater in the patients initially receiving argatroban compared with those who received UFH alone (54±2 versus 43±3; P<0.001; 71% versus 44%, P=0.04). Argatroban can moreover provide effective anticoagulation in postoperative cardiac patients receiving continuous RRT.50 Close monitoring and dose titration resulted in a comparable risk of bleeding for anticoagulation with both argatroban and heparin, regardless of the disease severity or impaired hepatic function.
Regarding the dosage of argatroban, it has been reported that the maximum dose is 10 μg/kg/minute. A case report has described using high-dose argatroban for treatment of HIT with thrombosis, with initial dose starting at 2 μg/kg/minute and the target desirable APTT value between 40–80 seconds.51 This patient had continued worsening of swelling at the site of thrombosis while developing a new venous thrombosis, and therefore the target APTT was increased eventually to >75 seconds and the infusion rate reached 15.5 μg/kg/minute. Higher doses of argatroban can be considered in patients with HIT plus thrombosis that is not responding to initial doses of infusion and may need the goal APTT increased. This patient did not have significant side effects but this is hard to predict with such high doses. Ideally, it would be beneficial if laboratories were able to measure actual argatroban concentration in patient’s serum, but this is not yet available. High doses of argatroban are an option, if needed, with close APTT monitoring.18,51
Age is not a contraindication for the use of argatroban. In fact, in a retrospective multicenter database analysis of 118 inpatients (including 62 adults aged ≥65 years) treated with argatroban for HIT, age was not a significant determinant for argatroban dosage or the thrombotic risk.52 No patient experienced major bleeding or required amputation, and no patients in the elder group (≥65 years old) died or developed new thrombosis. Furthermore, in a case report published just recently, a 95-year-old woman with severe HIT was treated with argatroban, and she had a positive clinical evolution with recovery of thrombocytopenia.53 The low-dose protocol was used (0.5 μg/kg/minute). The biological monitoring of argatroban was performed daily with both APTT (1.5–3.0 times patient baseline) and a specific coagulation test derived from the thrombin time (Hemoclot) leading to an estimation of the argatroban concentration.
Argatroban can also be considered in patients with hepatic dysfunction even though it is cleared by the hepatobiliary system.33 In these instances, APTT needs to be monitored closely and frequently, and dose reduction is required. Thus, although argatroban undergoes hepatic metabolism, with a fourfold decrease in clearance and a threefold increase in elimination half-life (eg, from approximately 51 to 181 minutes), package insert recommendations provide guidance on dose reductions (eg, reducing the starting dose from 2 μg/kg/minute to 0.5 μg/kg/minute for patients with moderate hepatic impairment).25,33 In a retrospective analysis, Levine et al27 studied 82 hospitalized patients treated with argatroban for HIT, many of whom also had hepatic dysfunction (average estimated MELD [Model For End-Stage Liver Disease] =21). It is noted that more than 50% of these patients had combined hepatic and renal dysfunction. Patients with elevated total bilirubin levels required 50% lower argatroban doses compared with patients with normal bilirubin levels (0.8 μg/kg/minute versus 1.6 μg/kg/minute), regardless of renal function. Furthermore, argatroban dose requirements correlated inversely with total bilirubin levels up to 5 mg/dL, which is a better indicator than alanine aminotransferase or aspartate aminotransferase, but were unaffected by the presence or absence of renal dysfunction. As the authors suggest, argatroban should be initiated at a dose of 0.5 μg/kg/minute, if a patient’s serum total bilirubin level is 1.5 mg/dL, if combined hepatic/renal dysfunction is present, or if conservative initial dosing is desired. In those cases, the best-fit equation may be that, for every 1 mg/dL increase in total bilirubin, argatroban dose requirements decrease by 0.38 μg/kg/minute.33 Because achievement of steady-state anticoagulation will be delayed in many patients with hepatic dysfunction, it would be wise to check the APTT at least 4–5 hours after drug initiation or dose change to ensure the desired level of anticoagulation is present.
Finally, because coagulation parameters will take longer to normalize on infusion withdrawal in patients with hepatic dysfunction (>5 hours in many patients in this study and up to 20 hours in a previous study), argatroban should be discontinued for a more extended period and anticoagulant effects should be monitored carefully before an invasive procedure, to ensure adequate hemostasis.27,28 However, other published retrospective studies and observational reports support the need for further reduced doses of argatroban in patients with hepatic impairment.19,33,54,55 When these authors reduced the starting dose to 0.2 μg/kg/minute, therapeutic levels of anticoagulation were achieved without bleeding complications. Moreover, in the retrospective analysis of 65 critically ill patients, Begelman et al55 found that argatroban dosing requirements decreased as the number of failing organs increased.
Conclusion
Argatroban is generally well tolerated and improves clinical outcomes in adults with HIT. The data of the ARG-911 and ARG-915 investigations provide convincing evidence that argatroban enables rapid and effective anticoagulation in this condition and is an effective therapy for HIT-associated complications. On the basis of this evidence, for patients with confirmed or strongly suspected HIT, with or without thrombosis, the American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (ninth edition) recommend the use of argatroban (grade of recommendation 1C), as well as other nonheparin anticoagulants (danaparoid [grade of recommendation 1C], lepirudin [grade of recommendation 1C], or fondaparinux [grade of recommendation 2C]) over the further use of UFH or LMWH or introduction or continuation of VKA.8 Moreover, data from the pooled analysis of three small, uncontrolled trials showed that argatroban can be an effective anticoagulant in patients with HIT undergoing PCI.22
The approved initial dosage of argatroban for adults with HIT or HITTS is 2 μg/kg/minute for patients with normal hepatic function and 0.5 μg/kg/minute for patients with hepatic dysfunction. However, other published retrospective studies support the need to further reduce starting doses of argatroban to 0.2 μg/kg/minute in patients with more severe hepatic impairment.19,33 Furthermore, there is evidence that a reduced initial dose may also be advisable for patients with heart failure, MODS, severe anasarca, or after cardiac surgery. Given this information, argatroban can be effectively utilized in treating HIT with monitoring of APTT.
Argatroban is a small molecule with a shorter half-life than lepirudin, fondaparinux, or danaparoid, and its use is preferred in patients who may need procedural interventions or have high bleeding risk. Finally, argatroban is a suitable regimen for use in RRT, due to the fact that it is eliminated via the liver, and its use is suggested over other nonheparin anticoagulants in patients with HIT and renal insufficiency.8
Disclosure
The author reports no conflicts of interest in this work.
References
Chong BH. Heparin-induced thrombocytopenia. J Thromb Haemost. 2003;1(7):1471–1478. | |
Warkentin TE, Greinacher A, Koster A, Lincoff AM; American College of Chest Physicians. Treatment and Prevention of Heparin-Induced Thrombocytopenia: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. 8th ed. Chest. 2008;133(Suppl 6):340S–380S. | |
Warkentin TE. Heparin-induced thrombocytopenia: pathogenesis and management. Br J Haematol. 2003;121(4):535–555. | |
Kelton JG, Warkentin TE. Heparin-induced thrombocytopenia: a historical perspective. Blood. 2008;112(7):2607–2616. | |
Arepally GM, Ortel TL. Clinical practice. Heparin-induced thrombocytopenia. N Engl J Med. 2006;355(8):809–817. | |
Amiral J, Bridey F, Dreyfus M, et al. Platelet factor 4 complexed to heparin is the target for antibodies generated in heparin-induced thrombocytopenia. Thromb Haemost. 1992;68(1):95–96. | |
Watson H, Davidson S, Keeling D; Haemostasis and Thrombosis Task Force of the British Committee for Standards in Haematology. Guidelines on the diagnosis and management of heparin-induced thrombocytopenia: second edition. Br J Haematol. 2012;159(5):528–540. | |
Linkins LA, Dans AL, Moores LK, et al; American College of Chest Physicians. Treatment and Prevention of Heparin-Induced Thrombocytopenia: Antithrombotic Therapy and Prevention of Thrombosis. 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(Suppl 2):e495S–e530S. | |
Jang IK, Hursting MJ. When heparins promote thrombosis: review of heparin-induced thrombocytopenia. Circulation. 2005;111(20):2671–2683. | |
Kelton JG, Arnold DM, Bates SM. Nonheparin anticoagulants for heparin-induced thrombocytopenia. N Engl J Med. 2013;368(8):737–744. | |
Kelton JG, Warkentin TE, Moore JC, et al. A prospective study measuring the development of antibodies against platelet factor 4-heparin in healthy males after exposure to heparins. J Thromb Haemost. 2012;10(7):1446–1449. | |
Zheng Y, Wang AW, Yu M, et al. B-cell tolerance regulates production of antibodies causing heparin-induced thrombocytopenia. Blood. 2014;123(6):931–934. | |
Warkentin TE, Sheppard JA, Moore JC, Cook RJ, Kelton JG. Studies of the immune response in heparin-induced thrombocytopenia. Blood. 2009;113(20):4963–4969. | |
Warkentin TE, Sheppard JA, Heels-Ansdell D, et al; Canadian Critical Care Trials Group; Australian and New Zealand Intensive Care Society Clinical Trials Group. Heparin-induced thrombocytopenia in medical surgical critical illness. Chest. 2013;144(3):848–858. | |
Cuker A. Clinical and laboratory diagnosis of heparin-induced thrombocytopenia: an integrated approach. Semin Thromb Hemost. 2014;40(1):106–114. | |
Lo GK, Juhl D, Warkentin TE, Sigouin CS, Eichler P, Greinacher A. Evaluation of pretest clinical score (4 T’s) for the diagnosis of heparin-induced thrombocytopenia in two clinical settings. J Thromb Haemost. 2006;4(4):759–765. | |
Cuker A, Arepally G, Crowther MA, et al. The HIT Expert Probability (HEP) Score: a novel pre-test probability model for heparin-induced thrombocytopenia based on broad expert opinion. J Thromb Haemost. 2010;8(12):2642–2650. | |
Bambrah RK, Pham DC, Rana F. Argatroban in heparin-induced thrombocytopenia: rationale for use and place in therapy. Ther Adv Chronic Dis. 2013;4(6):302–304. | |
Saugel B, Phillip V, Moessmer G, Schmid RM, Huber W. Argatroban therapy for heparin-induced thrombocytopenia in ICU patients with multiple organ dysfunction syndrome: a retrospective study. Crit Care. 2010;14(3):R90. | |
Grouzi E, Kyriakou E, Panagou I, Spiliotopoulou I. Fondaparinux for the treatment of acute heparin-induced thrombocytopenia: a single-center experience. Clin Appl Thromb Hemost. 2010;16(6):663–667. | |
Lee GM, Arepally GM. Heparin-induced thrombocytopenia. Hematology Am Soc Hematol Educ Program. 2013;2013:668–674. | |
Koster A, Fischer KG, Harder S, Mertzlufft F. The direct thrombin inhibitor argatroban: a review of its use in patients with and without HIT. Biologics. 2007;1(2):105–112. | |
Babuin L, Pengo V. Argatroban in the management of heparin-induced thrombocytopenia. Vasc Health Risk Manag. 2010;6:813–819. | |
Garcia DA, Baglin TP, Weitz JI, Samama MM; American College of Chest Physicians. Parenteral Anticoagulants: Antithrombotic Therapy and Prevention of Thrombosis. 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(Suppl 2):e24S–e43S. | |
Argatroban [package insert]. Research Triangle Park, NC: GlaxoSmithKline LLC; 2012. | |
Di Nisio M, Middeldorp S, Büller HR. Direct thrombin inhibitors.N Engl J Med. 2005;353(10):1028–1040. | |
Levine RL, Hursting MJ, McCollum D. Argatroban therapy in heparin-induced thrombocytopenia with hepatic dysfunction. Chest. 2006;129(5):1167–1175. | |
Swan SK, Hursting MJ. The pharmacokinetics and pharmacodynamics of argatroban: effects of age, gender, and hepatic or renal dysfunction. Pharmacotherapy. 2000;20(3):318–329. | |
Sanchez R, Picard N, Mouly-Bandini A, Chalvignac V, Lacarelle B, Sampol-Manos E. Severe decrease of cyclosporine levels in a heart transplant recipient receiving the direct thrombin inhibitor argatroban. Ther Drug Monit. 2014;36(3):273–277. | |
Lewis BE, Matthai WH Jr, Cohen M, Moses JW, Jursting MJ, Leya F; ARG-216/310/311 Study Investigators. Argatroban anticoagulation during percutaneous coronary intervention in patients with heparin-induced thrombocytopenia. Catheter Cardiovasc Interv. 2002;57(2):177–184. | |
Beiderlinden M, Treschan TA, Görlinger K, Peters J. Argatroban anticoagulation in critically ill patients. Ann Pharmacother. 2007;41(5):749–754. | |
Williamson DR, Boulanger I, Tardif M, Albert M, Grégoire G. Argatroban dosing in intensive care patients with acute renal failure and liver dysfunction. Pharmacotherapy. 2004;24(3):409–414. | |
Yarbrough PM, Varedi A, Walker A, Rondina MT. Argatroban dose reductions for suspected heparin-induced thrombocytopenia complicated by child-pugh class C liver disease. Ann Pharmacother. 2012;46(11):e30. | |
Lewis BE, Wallis DE, Berkowitz SD, et al. Argatroban anticoagulant therapy in patients with heparin-induced thrombocytopenia (ARG-911 study). Circulation. 2001;103(14):1838–1843. | |
Lewis BE, Wallis DE, Leya F, Hursting MJ, Kelton JG; Argatroban-915 Investigators. Argatroban anticoagulation in patients with heparin-induced thrombocytopenia. Arch Intern Med. 2003;163(15):1849–1856. | |
Walenga JM, Jeske WP, Wood JJ, Ahmad S, Lewis BE, Bakhos M. Laboratory tests for heparin-induced thrombocytopenia: a multicenter study. Semin Hematol. 1999;36(1 Suppl 1):22–28. | |
Lewis BE, Wallis DE, Hursting MJ, Levine RL, Leya F. Effects of argatroban therapy, demographic variables, and platelet count on thrombotic risks in heparin-induced thrombocytopenia. Chest. 2006;129(6):1407–1416. | |
Haas S. Heparin-induced thrombocytopenia (HIT) type II: a clinically heterogeneous hypercoagulable state requiring prompt intervention. Thromb Haemost. 2004;Suppl S:42–45. | |
Smythe MA, Stephens JL, Koerber JM, Mattson JC. A comparison of lepirudin and argatroban outcomes. Clin Appl Thromb Hemost. 2005;11(4):371–374. | |
Curzio KM, Cheng-Lai A, Kheyfets V, Sinnet M, Billett HH. A comparison of direct thrombin inhibitors in the treatment of Heparin-Induced Thrombocytopenia: a single institution experience. J Thromb Thrombolysis. 2009;28(2):117–123. | |
Kiser TH, Jung R, MacLaren R, Fish DN. Evaluation of diagnostic tests and argatroban or lepirudin therapy in patients with suspected heparin-induced thrombocytopenia. Pharmacotherapy. 2005;25(12):1736–1745. | |
Warkentin TE, Greinacher A. Heparin-induced thrombocytopenia: recognition, treatment, and prevention: the seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;1263(Suppl 3):S311–S337. | |
Refludan® (lepirudin [rDNA] for injection) [package insert]. Wayne, NJ: Bayer Healthcare Pharmaceuticals, Inc.; 2006. | |
Vakil NH, Kanaan AO, Donovan JL. Heparin-induced thrombocytopenia in the pediatric population: a review of current literature. J Pediatr Pharmacol Ther. 2012;17(1):12–30. | |
Jang IK, Lewis BE, Matthai WH, Kleiman NS. Argatroban anticoagulation in conjunction with glycoprotein IIb/IIIa inhibition in patients undergoing percutaneous coronary intervention: an open-label, nonrandomized pilot study. J Thromb Thrombolysis. 2004;18(1):31–37. | |
Murray PT, Reddy BV, Grossman EJ, et al. A prospective comparison of three argatroban treatment regimens during hemodialysis in end-stage renal disease. Kidney Int. 2004;66(6):2446–2453. | |
Reddy BV, Grossman EJ, Trevino SA, Hursting MJ, Murray PT. Argatroban anticoagulation in patients with heparin-induced thrombocytopenia requiring renal replacement therapy. Ann Pharmacother. 2005;39(10):1601–1605. | |
Link A, Girndt M, Selejan S, Mathes A, Böhm M, Rensing H. Argatroban for anticoagulation in continuous renal replacement therapy. Crit Care Med. 2009;37(1):105–110. | |
Abel EE, Kane-Gill SL, Seybert AL, Kellum JA. Direct thrombin inhibitors for management of heparin-induced thrombocytopenia in patients receiving renal replacement therapy: comparison of clinical outcomes. Am J Health Syst Pharm. 2012;69(18):1559–1567. | |
Klingele M, Bomberg H, Lerner-Gräber A, et al. Use of argatroban: experiences in continuous renal replacement therapy in critically ill patients after cardiac surgery. J Thorac Cardiovasc Surg. 2014;147(6):1918–1924. | |
Hellwig TR, Peitz GJ, Gulseth MP. High-dose argatroban for treatment of heparin-induced thrombocytopenia with thrombosis: a case report and review of laboratory considerations. Am J Health Syst Pharm. 2012;69(6):490–495. | |
Bartholomew JR, Pietrangeli CE, Hursting MJ. Argatroban anticoagulation for heparin-induced thrombocytopenia in elderly patients. Drugs Aging. 2007;24(6):489–499. | |
Putot A, Perrin S, Sordet-Guépet H, de Maistre E, Manckoundia P. Successful management of heparin-induced thrombocytopenia using argatroban in a very old woman: a case report. Case Rep Med. 2013;2013:586989. | |
Bates D, Griffin S, Angel B. Clinical experience with argatroban for heparin-induced thrombocytopenia in a large teaching hospital. Can J Hosp Pharm. 2009;62(4):290–297. | |
Begelman SM, Baghdasarian SB, Singh IM, Militello MA, Hursting MJ, Bartholomew JR. Argatroban anticoagulation in intensive care patients: effects of heart failure and multiple organ system failure. J Intensive Care Med. 2008;23(5):313–320. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.