")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 10
Transient ischemic attacks: predictability of future ischemic stroke or transient ischemic attack events
Authors Gupta H, Farrell A, Mittal M
Received 22 September 2013
Accepted for publication 30 October 2013
Published 8 January 2014 Volume 2014:10 Pages 27—35
DOI https://doi.org/10.2147/TCRM.S54810
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 8
Video abstract presented by Dr Gupta
Views: 1886
Harsh V Gupta,1 Ann M Farrell,2 Manoj K Mittal3
1Department of Neurology, The University of Arkansas Medical Sciences, Little Rock, AR, 2Department of Knowledge and Evaluation Research, Mayo Clinic, Rochester, MN, 3Department of Neurology, The University of Kansas Medical Center, Kansas City, KS, USA
Abstract: The short-term risk of an ischemic stroke after a transient ischemic attack (TIA) is estimated to be approximately 3%–10% at 2 days, 5% at 7 days, and 9%–17% at 90 days, depending on active or passive ascertainment of ischemic stroke. Various risk prediction scores are available to identify high-risk patients. We present here a pragmatic review of the literature discussing the main scoring systems. We also provide the sensitivity, specificity, positive predictive value, and negative predictive value for each scoring system. Our review shows that scoring systems including brain imaging and vascular imaging are better at risk prediction than scores that do not include this information.
Keywords: ischemic stroke, transient ischemic attack, prediction, systematic review
Introduction
Definition and epidemiology
A transient ischemic attack (TIA) has been traditionally defined as an episode of neurologic dysfunction caused by focal cerebral ischemia with complete recovery within 24 hours.1 Approximately 240,000 TIAs are seen annually in the US, and about one third of TIA patients do not see a physician within 24 hours.2,3 In 2009, the American Heart Association changed the definition of a TIA from a time-based definition to a tissue-based definition, whereby the presence of restricted diffusion on magnetic resonance imaging (MRI) is now classified as ischemic stroke irrespective of duration of symptoms.4 It has been estimated that a tissue-based definition of TIA could reduce the annual incidence of TIA in the US by 33% and increase the annual incidence of stroke by 7%.5
TIA and risk of future TIA/ischemic stroke
Short-term risk of ischemic stroke after a TIA is estimated to be ≈3% to 10% at 2 days, 5% at 7 days, and 9% to 17% at 90 days depending on active or passive ascertainment for ischemic strokes.6,7 Electronic medical records were used for passive ascertainment in the California cohort with a 10% 90-day stroke risk whereas a face-to-face patient encounter was used for active ascertainment in the Oxford cohort with a 14% 90-day stroke risk.8 The fluctuation in short-term risk of stroke can further be explained by a difference in study methods (timing from TIA event to enrolment in the study, inclusion/exclusion criteria, and methods used for stroke ascertainment), clinical setting (outpatient clinic, emergency department, or inpatient stroke service), intensity of secondary stroke prevention, patient characteristics, and underlying stroke etiology.7,8
Early treatment post TIA has been shown to reduce the 90-day risk of ischemic stroke by 80% in a population-based cohort study.9 Interventions to reduce the recurrent stroke risk include antiplatelet therapy (aspirin and/or clopidogrel),10–13 anticoagulation if indicated, statins,14 antihypertensives with a goal systolic blood pressure of <130 mmHg, and endarterectomy for ≥50% symptomatic carotid stenosis.9,15,16 Brain imaging with computed tomography (CT)/MRI should be performed to rule out hemorrhage or tumor before initiation of antiplatelet or anticoagulation therapy. Practice guidelines have advised secondary stroke prevention in the form of lifestyle modification; however, there is no randomized trial proving its efficacy.17 INSPiRE-TMS (intensified secondary prevention intending a reduction of recurrent events in TIA and minor stroke patients) is a prospective, multicenter, randomized, open intervention trial designed to study the role of intensified secondary prevention after a minor stroke or TIA.18
The post TIA stroke risk is different for each individual based on his/her modifiable (high blood pressure, diabetes, abnormal blood lipid profile, smoking status, sedentary lifestyle, and obesity) and nonmodifiable (age, sex) risk factors. Many clinical risk scoring systems, such as the ABCD, ABCD2, ABCD2-I, ABCD3-I, and California rule, have been developed to predict future ischemic stroke events after a TIA. Scoring systems like these not only help in diagnosing TIA but also help to predict future risk of ischemic stroke and in triaging patients in the acute setting for urgent workup during inpatient admission versus outpatient workup. Triage in the emergency room based on prediction scores can help physicians to identify patients who are at high risk of stroke recurrence in the next 48 hours or at high risk for a severe ischemic stroke. This paper aims to review the current literature on predictors of ischemic stroke after a TIA, to determine whether one scoring system is better than another, and to identify the limitations of these clinical scoring systems.
Literature review
We reviewed all published articles via a comprehensive search conducted using Ovid Medline from 1995 to April 18, 2013, irrespective of any language barrier. The search strategy (controlled vocabulary supplemented with keywords) was designed and conducted by an experienced librarian (AMF) with input from the study team. The search terms used were “transient ischemic attack” AND “stroke” AND “prediction OR predictor OR outcome OR future risk”. “Future risk” related to the risk of recurrent TIA or ischemic stroke. All papers of interest were further screened for relevant references.
Prediction scores
An ideal score for stroke prediction after TIA is one that is easily available, easy to calculate manually, cost-effective, practical, includes up to five variables, has high predictive value, can accurately categorize patients into meaningful categories, and is validated in various cohorts and settings. Weighing of variables should ideally be done based on the beta coefficient for each variable calculated during logistic regression.19 Another method is based on the odds ratio (OR) or hazards ratio, which may be less precise than using the beta coefficient, but is simple to use clinically, making it a viable pragmatic option.20 Weighing of scores in the California score was not based on the hazards ratio or the beta coefficient from the logistic regression. The authors simply allocated an integer of 1 to each risk factor irrespective of the OR or beta intercepts.21 For the ABCD score, the authors allocated each bivariate risk factor integer values of 0 and 1, and values of 0, 1, and 2 for each trivariate factor.22 This method of integer allocation is not precise and may not provide the correct prediction due to poor calibration. Subsequent scores followed ABCD scoring and have the same issues with precision and internal validity.
In Table 1, we have compared various prediction scores for post TIA stroke. In Table 2, we have compared data from the derivation cohort of all the above scores in terms of their sensitivity, specificity, positive predictive value, and negative predictive value. When available, follow-up at 3 months was selected for different score comparison. For a stroke prediction model, we want to have the maximum sensitivity and negative predictive value to identify patients who are at a higher risk of stroke after a TIA episode. For the purpose of comparison, we set the cutoff as 90% true positives for dichotomizing the scores when possible.
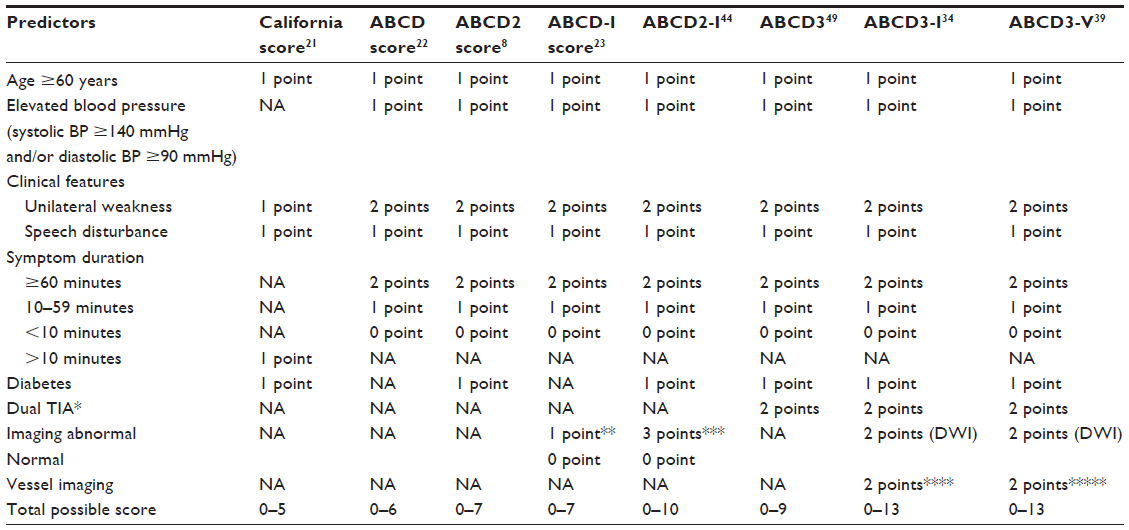 | Table 1 Various post TIA stroke prediction scores |
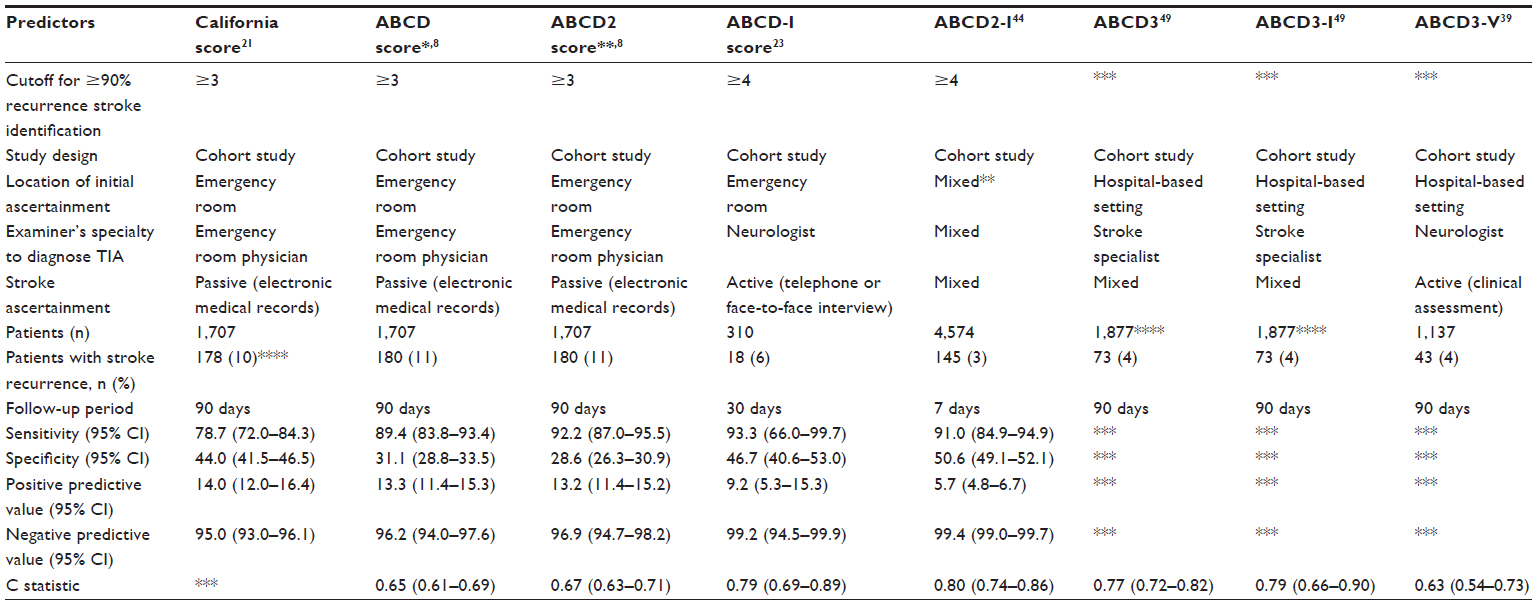 | Table 2 Comparison of various prediction scores according to their derivation cohorts |
California score (2000)
The California score was designed to predict the 90-day stroke risk after an episode of TIA, using stroke risk factors (age, diabetes), clinical features of TIA, and duration of symptoms (Table 1). It was later validated in a study with patients from the UK and the US.8
Limitations: in the absence of vascular imaging or cardiac testing, the California score does not help to differentiate various stroke etiologies (ie, large vessel atherosclerosis, cardioembolic, or small vessel disease).
ABCD score (2005)
The ABCD score was designed to predict post TIA ischemic stroke using stroke risk factors (age, blood pressure), clinical features of TIA, and duration of symptoms (Table 1).22 The ABCD score has been externally validated in various countries, including Italy, Australia, and the US.8,23,24 To increase its ease of use, the ABCD score was dichotomized into <5 or ≥5 (high risk) with a high sensitivity (100%, 86%) and negative predictive value (100%, 98%) but poor specificity (53%, 54%) and a positive predictive value (8%, 12.5%) for 7-day and 90-day stroke prediction, respectively.24 In a study of 274 TIA patients, an ABCD score of 4–6 was associated with a four-fold increase in stroke risk and a score of 5–6 was associated with a six-fold increase in stroke risk at 7 days and 30 days.23
Limitations: in the absence of vascular imaging or cardiac testing, the ABCD score by itself does not help to understand the stroke etiology (large vessel atherosclerosis, cardioembolic, or small vessel disease). Also, a low ABCD score does not rule out the risk of recurrent stroke, as shown in a prospective study where patients with an ABCD score <4 still had a high risk (14%) of clinical cerebral ischemia during 90 days of follow-up.25
ABCD2 score (2007)
The ABCD2 score was created combining diabetes with the ABCD score to predict the 2-day, 7-day, and 90-day risk of stroke after an episode of TIA. Diabetes was an independent predictor of stroke at 30 days after a TIA in a case series and pooled data from two population-based Oxford groups, justifying its addition to the ABCD score.8 The ABCD2 score was classified as low stroke risk (score <4), moderate stroke risk (score 4–5), and high stroke risk (score >5, Table 1).8 It has been extensively validated in multiple cohorts from Canada, People’s Republic of China, Greece, Italy, Singapore, and the US.26–32 Despite the change in TIA definition from a time-based to a tissue-based one, the ABCD2 score is still a good predictor of stroke after a TIA. In a study of more than 4,500 patients, the 7-day recurrent stroke rate was 7.1% in diffusion-weighted imaging (DWI)-positive patients (defined as complete and rapid symptomatic recovery but presence of infarction on MRI) and 0.4% in tissue-negative events (no infarction on MRI but complete clinical recovery).33 Similar rates in CT-imaged patients were 12.8% and 3.0%, respectively.33 At 90-day follow-up, tissue-positive events with low ABCD2 scores and tissue-negative events with high ABCD2 scores had a similar stroke risk.33
Limitations: for stroke prediction, a study of 2,056 patients from Canada found a low (12.5%) specificity but high sensitivity (94.7%) for the ABCD2 score at 7 days or 90 days with a cutoff score of 2.29 No significant association was seen between a higher ABCD2 score and future stroke risk in a study of 393 TIA patients by Ghandehari et al.34 Another study of 1,679 TIA patients found that those with a ABCD2 score <4 in the presence of internal carotid artery stenosis, intracranial stenosis, or a source of emboli, remained at high risk of stroke.35
Systematic review and meta-analysis showed a better predictive value of ABCD and ABCD2 scores for TIA patients in terms of future stroke prediction at 0–7 days36 (area under the curve [AUC] 0.71) than at 8–90 days (AUC 0.63).37 The ABCD2 score is useful as an initial screening tool for use by non-neurologists, but should be used with caution in young patients and in those with other risk factors for recurrent stroke, including atrial fibrillation, carotid stenosis, intracranial stenosis, and a positive DWI lesion on MRI.35,38
ABCD-I score (2008)
Sciolla et al23 added imaging findings to the ABCD score and formulated a new scoring system, ie, the ABCD-I score (Table 1). The ABCD-I score (OR 2.89, 95% confidence interval [CI] 1.62–5.16) had better predictive power than the ABCD score (OR 2.62, 95% CI 1.44–4.76) for 30-day stroke recurrence.
Limitations: this study was limited due to its small sample size.23 The ABCD-I score was not found to be useful in a multicenter cohort from Spain, probably due to initiation of early evaluation and preventative treatment by a stroke neurologist, which may have led to a change in the patients’ recurrent stroke risk. Another factor which may have led to a lower AUC for the ABCD-I score is the heterogeneity arising from inclusion of 30 Spanish centers and the difference in training of the study neurologists (ie, neurologists versus stroke neurologists).39
ABCD2-I score (2010)
DWI lesions are seen in 28%–40% of patients with a transient neurologic event and are associated with a higher (10.8%) incidence of stroke recurrence at 90 days when compared with patients without DWI lesions (4.3%).40–44 The incidence of DWI lesions initially increases up to 5 days (lesions occurring after 24 hours may represent silent infarcts) from symptom onset and then decreases (small lesions may resolve by the time of imaging).45 A systematic review revealed a relationship between DWI lesions and symptom duration >60 minutes, dysphasia, and motor weakness, but not with age, hypertension, or diabetes. DWI lesions were seen more often in patients with atrial fibrillation or carotid stenosis (≥50%).46 After this study, infarction on DWI or CT head was added to the ABCD2 score to formulate the ABCD2-I score, which increased the predictive value of the ABCD2 score for stroke at 7 days (AUC 0.66 with the ABCD2 score and 0.78 with the ABCD2-I score, three points for infarction) and 90 days (AUC 0.68 with the ABCD2 score and 0.80 with the ABCD2-I score).44 This score was externally validated in a study of 410 patients with an AUC of 0.77 for one-year risk of stroke.47
Limitations: This score may not be generalizable to all centers across the world due to the need for MRI to calculate an individual’s risk of future stroke. Availability of MRI is restricted to larger centers and developed nations, thereby limiting its use.
ABCD3 and ABCD3-I score (2010)
During hospitalization, patients with recurrent TIA have a higher (7%) risk of ischemic stroke than patients with a single TIA (2%).48 Carotid stenosis was noted to be an independent predictor for 90-day stroke in a population-based study.38 Identification of recurrent TIA, carotid stenosis, and DWI lesions as independent predictors for 90-day stroke led to the inception of the ABCD3 and ABCD3-I scores. A study of 3,886 patients derived the ABCD3 score (range 0–9 points) by assigning two points for dual transient ischemic attack (ie, an earlier transient ischemic attack within 7 days of the index event). Different weightings were assigned for carotid stenosis, DWI lesions, and dual TIA in this study based on the regression beta coefficients. The authors did not change the weights for the ABCD2 score and used the previously reported weights.49 The C statistic was 0.80 at 7 days and 0.77 at 90 days. Merwick et al49 also included stenosis of at least 50% on carotid imaging (two points) and abnormal DWI (two points) in the ABCD3-imaging (ABCD3-I) score. The C statistic for the ABCD3-I score was 0.92 at 7 days and 0.79 at 90 days.49 The ABCD3-I score has been externally validated in the People’s Republic of China and Spain.50–52
Limitations: like the ABCD2-I score, the ABCD3-I score may have limited generalizability due to the need for MRI to calculate an individual’s risk for future stroke. The ABCD3 and ABCD3-I scores may also be limited due to recall bias, given that some patients may not be able to provide an accurate account of TIA in the previous 7 days.
ABCD3-V score (2012)
A proximal lesion in the intracranial arteries has been shown to be an independent predictor of recurrent ischemic lesions (stroke or TIA) at 7 days.53 The ABCD3-V (vasculature) score included all components of the ABCD3-I score with addition of vessel information (two points for at least 50% symptomatic stenosis on carotid or intracranial imaging).39 In the PROMAPA study, a comparison of various TIA prediction scores (ABCD, ABCD2, ABCDI, ABCD2-I, ABCD3, California score, Essen stroke risk score, and Stroke Prognosis Instrument II) showed that scores not including vascular imaging or prior TIA (TIA before the TIA episode when the prediction is being done) failed to predict stroke risk after TIA. The ABCD3-V score has not been validated thus far.
Limitations: similar to other imaging-based scores, use of the ABCD3-V would be limited due to its higher cost and need for MRI, carotid imaging, and intracranial vessel imaging. Also, this score has not been externally validated.
Other variables
TIA characteristics
TIAs may have different underlying mechanisms (large artery atherosclerosis [LAA] 23%–38%, cardioembolism 22%, or small vessel disease 18%).54,55 Cluster TIAs are more common with LAA (42%) than cardioembolic (17%) or small vessel TIAs (13%). Aphasia or cortical signs are more common in cardioembolic TIA (48%, 56%) than LAA (31%, 36%) or small vessel disease (0%).55 LAA TIAs are short-lasting as compared with small vessel or cardioembolic TIAs.55 Small vessel TIAs mainly present with motor weakness (57%), are stereotypical (90%), and have multiple episodes (48%).54 Small vessel TIAs also have a shorter latency between the last episode or the first episode and the definitive ischemic stroke.54 A study of 388 TIA patients found large artery atherosclerosis to carry the highest risk of recurrent stroke (20%) followed by cardioembolism (11.5%), undetermined (4.7%), and small vessel disease (1.5%).55 Interestingly, a study of 1,753 patients found previous TIA to be an independent predictor of a good outcome for patients with nonlacunar strokes. The authors suggested ischemic tolerance as the possible underlying mechanism for better recovery in these patients.56
Atrial fibrillation
Atrial fibrillation is a well known risk factor for cardio-embolic stroke; however, so far it has not been found to be an independent predictor for future stroke risk after a TIA.24,38,41,57,58
Ankle-brachial pressure index
Although a decreased ankle-brachial pressure index (ABPI) is not a recognized risk factor for stroke or TIA, we found a few studies that correlated the ABPI value with recurrent ischemic strokes. Weimer et al and later Tsivgoulis et al found an ABPI ≤0.9 to be an independent predictor of future stroke or TIA at 30 days (19.2% versus 3.3% for ABPI >0.9; OR 2.67, 95% CI 0.64–11.05) and 17.5 months (6.6% versus 4.6% for ABPI >0.9; OR 1.47, 95% CI 0.76–2.83) in acute ischemic stroke or TIA patients.59,60
C-reactive protein
C-reactive protein is a protein synthesized by the liver, that rises in response to acute inflammation. High-sensitivity C-reactive protein >4.1 mg/L at the time of a TIA has been linked to future stroke events at one year (hazard ratio 2.81, 95% CI 1.12–7.10);61 however, a recent nested case control study did not confirm this finding.62
MicroRNAs
MicroRNAs (miRNAs) are a novel class of endogenous, noncoding small RNAs that bind to complementary sequences, resulting in their silencing.63 miRNAs are involved in different aspects of cardiovascular disease, are mediators of smooth muscle cell phenotypic modulation and vessel remodeling, and can be used to identify the development and progression of atherosclerosis. Animal studies have shown upregulation of miRNAs after ischemic brain injury. It remains to be seen if blood miRNAs may be used as a biomarker in the future for stroke diagnosis in patients with negative neuroimaging, for differentiating stroke subtypes, or for predicting recurrent episodes of TIA or stroke.64
Fluid-attenuated inversion recovery imaging in TIA
In a study of 43 patients with TIA, distal hyperintense vessels on fluid-attenuated inversion recovery MRI sequence were independently associated with large artery severe stenosis or occlusion, seen in 33% patients who had an MRI brain performed within 24 hours of symptom onset.65
Need for carotid imaging
Tholen et al conducted a cost-effectiveness analysis for various noninvasive carotid imaging techniques in patients with a recent TIA or a minor stroke. In low-risk patients, they found duplex ultrasound to be a cost-effective first test, followed by CT angiogram if the patient has symptomatic carotid stenosis on carotid imaging. In a high-risk patient, they found CT angiogram to be the cost-effective initial carotid imaging modality.66 The ABCD2 score may be used to identify high-risk patients (>5) in the emergency room when making a decision about ordering a carotid ultrasound or CT angiogram. Low-moderate risk patients (ABCD2 score ≤5) may be considered for outpatient evaluation, because in a study from Spain, outpatient evaluation for low-moderate risk patients reduced the cost by one fifth without any increase in cerebrovascular recurrence rate.67 Similar findings were also noted in the US and Portugal, with outpatient evaluation being more cost-effective.68,69 In the absence of availability of ultrasound imaging or limited resources, clinical prediction can be used to identify patients with carotid stenosis. A study of 726 patients reported 97% specificity and 17% sensitivity for any three of the four features (ipsilateral bruit, diabetes mellitus, and previous TIA, no lacunar syndrome); and 99% sensitivity and 22% specificity for one or more of the four features.70 The decision for carotid imaging should be tailored according to a patient’s individual risk, local infrastructure (availability of a same-day TIA clinic), insurance coverage, and patient preferences.
Conclusion
Multiple studies have investigated prediction scores and their validation. Different scores may produce different results depending on the examiner’s specialty (emergency room physician versus neurologist), patient setting (emergency room versus outpatient clinic), and duration of follow-up (7 days versus 90 days). So far, the ABCD2-I and ABCD3-I seem to be the best scoring systems because they have the maximum AUC, include patient imaging and vasculature data, and have been externally validated. The ABCD3-V score further includes intracranial imaging data and its external validation is needed. These prediction scores are clinically useful because they can help to identify at-risk patients who need to be admitted to the hospital versus patients who can be worked up in an outpatient setting to offset the huge costs of inpatient admissions. Future studies are needed to validate the ABCD3-V score and also to understand how these scores will change TIA patient triage in the emergency room.
Disclosure
None of the authors has any disclosure to make or any conflicts of interest in this work.
References
[No authors listed]. Special report from the National Institute of Neurological Disorders and Stroke. Classification of cerebrovascular diseases III. Stroke. 1990;21:637–676. | |
Kleindorfer D, Panagos P, Pancioli A, et al. Incidence and short-term prognosis of transient ischemic attack in a population-based study. Stroke. 2005;36:720–723. | |
Johnston SC, Fayad PB, Gorelick PB, et al. Prevalence and knowledge of transient ischemic attack among US adults. Neurology. 2003;60:1429–1434. | |
Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. Stroke. 2009;40:2276–2293. | |
Ovbiagele B, Kidwell CS, Saver JL. Epidemiological impact in the United States of a tissue-based definition of transient ischemic attack. Stroke. 2003;34:919–924. | |
Wu CM, McLaughlin K, Lorenzetti DL, Hill MD, Manns BJ, Ghali WA. Early risk of stroke after transient ischemic attack: a systematic review and meta-analysis. Arch Intern Med. 2007;167:2417–2422. | |
Giles MF, Rothwell PM. Risk of stroke early after transient ischaemic attack: a systematic review and meta-analysis. Lancet Neurol. 2007;6:1063–1072. | |
Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369:283–292. | |
Rothwell PM, Giles MF, Chandratheva A, et al. Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet. 2007;370:1432–1442. | |
Lau AY, Zhao Y, Chen C, et al. Dual antiplatelets reduce microembolic signals in patients with transient ischemic attack and minor stroke: subgroup analysis of CLAIR study. Int J Stroke. March 12, 2013. [Epub ahead of print.] | |
Hankey GJ, Johnston SC, Easton JD, et al. Effect of clopidogrel plus ASA vs ASA early after TIA and ischaemic stroke: a substudy of the CHARISMA trial. Int J Stroke. 2011;6:3–9. | |
Wong KS, Wang Y, Leng X, et al. Early dual versus mono antiplatelet therapy for acute non-cardioembolic ischemic stroke or transient ischemic attack: an updated systematic review and meta-analysis. Circulation. 2013;128:1656–1666. | |
Lee M, Saver JL, Hong K-S, Rao NM, Wu Y-L, Ovbiagele B. Risk-benefit profile of long-term dual- versus single-antiplatelet therapy among patients with ischemic stroke: a systematic review and meta-analysis. Ann Intern Med. 2013;159:463–470. | |
Merwick A, Albers GW, Arsava EM, et al. Reduction in early stroke risk in carotid stenosis with transient ischemic attack associated with statin treatment. Stroke. 2013;44:2814–2820. | |
Kirshner HS. Therapeutic interventions for prevention of recurrent ischemic stroke. Am J Manag Care. 2008;14:S212–S226. | |
Alhusban A, Fagan SC. Secondary prevention of stroke in the elderly: a review of the evidence. Am J Geriatr Pharmacother. 2011;9:143–152. | |
Fuentes B, Gallego J, Gil-Nunez A, et al. Guidelines for the preventive treatment of ischaemic stroke and TIA (I). Update on risk factors and life style. Neurologia. 2012;27:560–574. | |
Leistner S, Michelson G, Laumeier I, et al. Intensified secondary prevention intending a reduction of recurrent events in TIA and minor stroke patients (INSPiRE-TMS): a protocol for a randomised controlled trial. BMC Neurol. 2013;13:11. | |
Harrell F. Regression coefficients and scoring rules. J Clin Epidemiol. 1996;49:819. | |
Tu JV, Naylor CD. Clinical prediction rules. J Clin Epidemiol. 1997;50:743–744. | |
Johnston S, Gress DR, Browner WS, Sidney S. Short-term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901–2906. | |
Rothwell PM, Giles MF, Flossmann E, et al. A simple score (ABCD) to identify individuals at high early risk of stroke after transient ischaemic attack. Lancet. 2005;366:29–36. | |
Sciolla R, Melis F. Rapid identification of high-risk transient ischemic attacks: prospective validation of the ABCD score. Stroke. 2008;39:297–302. | |
Bray JE, Coughlan K, Bladin C. Can the ABCD score be dichotomised to identify high-risk patients with transient ischaemic attack in the emergency department? Emerg Med J. 2007;24:92–95. | |
Cucchiara BL, Messe SR, Taylor RA, et al. Is the ABCD score useful for risk stratification of patients with acute transient ischemic attack? Stroke. 2006;37:1710–1714. | |
Asimos AW, Johnson AM, Rosamond WD, et al. A multicenter evaluation of the ABCD2 score’s accuracy for predicting early ischemic stroke in admitted patients with transient ischemic attack. Ann Emerg Med. 2010;55:201–210. e5. | |
Cancelli I, Janes F, Gigli GL, et al. Incidence of transient ischemic attack and early stroke risk: validation of the ABCD2 score in an Italian population-based study. Stroke. 2011;42:2751–2757. | |
Fothergill A, Christianson TJ, Brown RD Jr, Rabinstein AA. Validation and refinement of the ABCD2 score: a population-based analysis. Stroke. 2009;40:2669–2673. | |
Perry JJ, Sharma M, Sivilotti ML, et al. Prospective validation of the ABCD2 score for patients in the emergency department with transient ischemic attack. CMAJ. 2011;183:1137–1145. | |
Tsivgoulis G, Stamboulis E, Sharma VK, et al. Multicenter external validation of the ABCD2 score in triaging TIA patients. Neurology. 2010;74:1351–1357. | |
Yang J, Fu JH, Chen XY, et al. Validation of the ABCD2 score to identify the patients with high risk of late stroke after a transient ischemic attack or minor ischemic stroke. Stroke. 2010;41:1298–1300. | |
Ong ME, Chan YH, Lin WP, Chung WL. Validating the ABCD(2) score for predicting stroke risk after transient ischemic attack in the ED. Am J Emerg Med. 2010;28:44–48. | |
Giles MF, Albers GW, Amarenco P, et al. Early stroke risk and ABCD2 score performance in tissue- vs time-defined TIA: a multicenter study. Neurology. 2011;77:1222–1228. | |
Ghandehari K, Ahmadi F, Ebrahimzadeh S, Shariatinezhad K, Ghandehari K. Assessment of ABCD(2) scale in patients with transient ischaemic attack or stroke. Neurol Neurochir Pol. 2012;46:421–427. | |
Amarenco P, Labreuche J, Lavallee PC. Patients with transient ischemic attack with ABCD2 <4 can have similar 90-day stroke risk as patients with transient ischemic attack with ABCD2 ≥4. Stroke. 2012;43:863–865. | |
Galvin R, Geraghty C, Motterlini N, Dimitrov BD, Fahey T. Prognostic value of the ABCD(2) clinical prediction rule: a systematic review and meta-analysis. Fam Pract. 2011;28:366–376. | |
Giles MF, Rothwell PM. Systematic review and pooled analysis of published and unpublished validations of the ABCD and ABCD2 transient ischemic attack risk scores. Stroke. 2010;41:667–673. | |
Sheehan OC, Kyne L, Kelly LA, et al. Population-based study of ABCD2 score, carotid stenosis, and atrial fibrillation for early stroke prediction after transient ischemic attack: the North Dublin TIA study. Stroke. 2010;41:844–850. | |
Purroy F, Jimenez Caballero PE, Gorospe A, et al. Prediction of early stroke recurrence in transient ischemic attack patients from the PROMAPA study: a comparison of prognostic risk scores. Cerebrovasc Dis. 2012;33:182–189. | |
Calvet D, Lamy C, Touze E, Oppenheim C, Meder J-F, Mas J-L. Management and outcome of patients with transient ischemic attack admitted to a stroke unit. Cerebrovasc Dis. 2007;24:80–85. | |
Calvet D, Touze E, Oppenheim C, Turc G, Meder J-F, Mas J-L. DWI lesions and TIA etiology improve the prediction of stroke after TIA. Stroke. 2009;40:187–192. | |
Coutts SB, Simon JE, Eliasziw M, et al. Triaging transient ischemic attack and minor stroke patients using acute magnetic resonance imaging. Ann Neurol. 2005;57:848–854. | |
Purroy F, Montaner J, Rovira A, Delgado P, Quintana M, Alvarez-Sabin J. Higher risk of further vascular events among transient ischemic attack patients with diffusion-weighted imaging acute ischemic lesions. Stroke. 2004;35:2313–2319. | |
Giles MF, Albers GW, Amarenco P, et al. Addition of brain infarction to the ABCD2 score (ABCD2I): a collaborative analysis of unpublished data on 4574 patients. Stroke. 2010;41:1907–1913. | |
Pavlovic AM, Barras CD, Hand PJ, Tress BM, Desmond PM, Davis SM. Brain imaging in transient ischemic attack – redefining TIA. J Clin Neurosci. 2010;17:1105–1110. | |
Redgrave JN, Coutts SB, Schulz UG, Briley D, Rothwell PM. Systematic review of associations between the presence of acute ischemic lesions on diffusion-weighted imaging and clinical predictors of early stroke risk after transient ischemic attack. Stroke. 2007;38:1482–1488. | |
Meng X, Wang Y, Liu L, et al. Validation of the ABCD2-I score to predict stroke risk after transient ischemic attack. Neurol Res. 2011;33:482–486. | |
Chatzikonstantinou A, Willmann O, Jager T, Szabo K, Hennerici MG. Transient ischemic attack patients with fluctuations are at highest risk for early stroke. Cerebrovasc Dis. 2009;27:594–598. | |
Merwick A, Albers GW, Amarenco P, et al. Addition of brain and carotid imaging to the ABCD(2) score to identify patients at early risk of stroke after transient ischaemic attack: a multicentre observational study. Lancet Neurol. 2010;9:1060–1069. | |
Purroy F, Jimenez-Caballero PE, Mauri-Capdevila G, et al. Predictive value of brain and vascular imaging including intracranial vessels in transient ischaemic attack patients: external validation of the ABCD3-I score. Eur J Neurol. 2013;20:1088–1093. | |
Song B, Fang H, Zhao L, et al. Validation of the ABCD3-I score to predict stroke risk after transient ischemic attack. Stroke. 2013;44:1244–1248. | |
Song XK, Wang WJ, Li HY, Ren MS, Wu L, Ma JF. [The value of ABCD3-I score in prediction of cerebral infarction after transient ischaemic attack]. Zhonghua Nei Ke Za Zhi. 2012;51:445–448. Chinese. | |
Ssi-Yan-Kai G, Nasr N, Faury A, et al. Intracranial artery stenosis or occlusion predicts ischemic recurrence after transient ischemic attack. AJNR Am J Neuroradiol. 2013;34:185–190. | |
Arboix A, Martí-Vilalta JL. Transient ischemic attacks in lacunar infarcts. Cerebrovasc Dis. 1991;1:20–24. | |
Purroy F, Montaner J, Molina CA, Delgado P, Ribo M, Alvarez-Sabin J. Patterns and predictors of early risk of recurrence after transient ischemic attack with respect to etiologic subtypes. Stroke. 2007;38:3225–3229. | |
Arboix A, Cabeza N, Garcia-Eroles L, et al. Relevance of transient ischemic attack to early neurological recovery after nonlacunar ischemic stroke. Cerebrovasc Dis. 2004;18:304–311. | |
Quinn TJ, Cameron AC, Dawson J, Lees KR, Walters MR. ABCD2 scores and prediction of noncerebrovascular diagnoses in an outpatient population: a case-control study. Stroke. 2009;40:749–753. | |
Coutts SB, Sylaja PN, Choi YB, et al. The ASPIRE approach for TIA risk stratification. Can J Neurol Sci. 2011;38:78–81. | |
Tsivgoulis G, Bogiatzi C, Heliopoulos I, et al. Low ankle-brachial index predicts early risk of recurrent stroke in patients with acute cerebral ischemia. Atherosclerosis. 2012;220:407–412. | |
Weimar C, Goertler M, Rother J, et al. Predictive value of the Essen stroke risk score and ankle brachial index in acute ischaemic stroke patients from 85 German stroke units. J Neurol Neurosurg Psychiatry. 2008;79:1339–1343. | |
Purroy F, Montaner J, Molina CA, et al. C-reactive protein predicts further ischemic events in transient ischemic attack patients. Acta Neurol Scand. 2007;115:60–66. | |
Selvarajah JR, Smith CJ, Hulme S, et al. Does inflammation predispose to recurrent vascular events after recent transient ischaemic attack and minor stroke? The North West of England transient ischaemic attack and minor stroke (NORTHSTAR) study. Int J Stroke. 2011;6:187–194. | |
Small EM, Olson EN. Pervasive roles of microRNAs in cardiovascular biology. Nature. 2011;469:336–342. | |
Li WY, Jin J, Chen J, Guo Y, Tang J, Tan S. Circulating microRNAs as potential non-invasive biomarkers for the early detection of hypertension-related stroke. J Hum Hypertens. October 17, 2013. [Epub ahead of print.] | |
Yoshioka K, Ishibashi S, Shiraishi A, Yokota T, Mizusawa H. Distal hyperintense vessels on FLAIR images predict large-artery stenosis in patients with transient ischemic attack. Neuroradiology. 2013;55:165–169. | |
Tholen AT, de Monyé C, Genders TS, et al. Suspected carotid artery stenosis: cost-effectiveness of CT angiography in work-up of patients with recent TIA or minor ischemic stroke. Radiology. 2010;256:585–597. | |
Martinez-Martinez MM, Martinez-Sanchez P, Fuentes B, et al. Transient ischaemic attacks clinics provide equivalent and more efficient care than early in-hospital assessment. Eur J Neurol. 2013;20:338–343. | |
Teles de Araujo M, Canhao P. Cost study of transient ischemic attack patients in a transient ischemic attack clinic. Acta Med Port. 2011;24:681–686. | |
Joshi JK, Ouyang B, Prabhakaran S. Should TIA patients be hospitalized or referred to a same-day clinic? A decision analysis. Neurology. 2011;77:2082–2088. | |
Mead GE, Wardlaw JM, Lewis SC, McDowall M, Dennis MS. Can simple clinical features be used to identify patients with severe carotid stenosis on Doppler ultrasound? J Neurol Neurosurg Psychiatry. 1999;66:16–19. | |
[No authors listed]. North American Symptomatic Carotid Endarterectomy Trial. Methods, patient characteristics, and progress. Stroke. 1991;22:711–720. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.