")
Back to Archived Journals » Comparative Effectiveness Research » Volume 5
The role and importance of economic evaluation of traditional herbal medicine use for chronic non-communicable diseases
Authors Hughes G, Aboyade O, Hill J, Rasu R
Received 7 November 2014
Accepted for publication 25 February 2015
Published 16 July 2015 Volume 2015:5 Pages 49—55
DOI https://doi.org/10.2147/CER.S77163
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Corrine I Voils
Gail D Hughes,1 Oluwaseyi M Aboyade,1 John D Hill,2 Rafia S Rasu3
1South African Herbal Science and Medicine Institute, University of the Western Cape, Western Cape, South Africa; 2Department of Pharmacy, Cleveland Clinic, Cleveland, OH, 3School of Pharmacy, University of Kansas, Lawrence, KS, USA
Background: Non-communicable diseases (NCD) constitute major public health problems globally, with an impact on morbidity and mortality ranking high and second to HIV/AIDS. Existing studies conducted in South Africa have demonstrated that people living with NCD rely on traditional herbal medicine (THM) primarily or in combination with conventional drugs. The primary research focus has been on the clinical and experimental aspects of THM use for NCD, with limited data on the economic impact of health care delivery. Therefore, the purpose of this study will be to determine the cost and utilization of resources on THM in South Africa for NCD.
Materials and methods: Study describes the methods toward incorporating cost estimations and economic evaluation illustrated with the Prospective Urban and rural Epidemiological (PURE) study in South Africa. The South African PURE cohort is investigating the geographic and socioeconomic influence of THM spending and utilization, variations in spending based on perceived health status, marital status, and whether spending patterns have any impact on hospitalizations and disability.
Data collection and evaluation plan: Since the individual costs of THM are not regulated nor do they have a standardized price value, information obtained through this study can be utilized to assess differences and determine underlying factors contributing to spending. This insight into THM spending patterns can aid in the development and implementation of guidelines or standardized legislation governing THM use and distribution. An economic evaluation and cost estimation model has been proposed, while the data collection is still ongoing. Particularly, willingness to pay method measures how much participants are willing to pay for THM for perceived improvements in health. Resource-use and expenditures along with annual direct costs for households will be determined.
Conclusion: Economic evaluations can provide insight for health care policy decision makers on the appropriate inclusion of THM to reduce the overall burden of health care costs in South Africa. Because of the increased prevalence of integrative medicine, it is crucial to consider potential implications and their use of comparative effectiveness research to incorporate complementary and alternative medicine in future.
Keywords: complementary medicine, alternative medicine, economics, comparative effectiveness research, CAM
Background
Chronic non-communicable diseases (NCD), consisting of cardiovascular disease, type 2 diabetes, chronic respiratory disease, and certain cancers currently account for 44% of premature deaths and 60% of all deaths worldwide.1 These diseases particularly affect low- and middle-income countries, where they account for 80% of all mortality.1 Several factors have contributed to the increased burden of chronic NCD in these countries, which include lengthened average life span, decreases in physical activity, increases in consumption of unhealthy food, and continued tobacco use.1 The combination of these factors has led to projections that the burden of these diseases will continue to rise by 15% globally between 2010 and 2020.2 Low- and middle-income countries, already facing a greater burden of chronic NCD, are expected to see a 20% increase over the same period.2 All of these factors together have led to chronic NCD becoming a top global health concern.
South Africa has been affected by particularly high rates of communicable diseases, such as the HIV/AIDS epidemic, but is now similarly facing a substantial burden of chronic NCD. In 2004, estimates by the World Health Organization (WHO) suggested that chronic NCD, as measured by disability-adjusted life years, accounted for 28% of the total burden of disease in South Africa.3 These estimates place the burden of NCD in South Africa at two to three times that of most developed countries and similar to other sub-Saharan and central European countries.3 The rise in prevalence of chronic NCD largely can be attributed to demographic transitions and lifestyle changes as a result of urbanization. High levels of modifiable risk factors that contribute to chronic NCD including tobacco use, physical inactivity, and unhealthy diets have all been reported in the South African adult population.4–6 Improved medical care has led to a lengthened life span for the South African population, with projections that the proportion of the population above 60 years old is expected to grow at more than four times the rate of the general population.7 Socioeconomic disparities have resulted in the urban poor facing the largest burden of chronic NDC. In combination, these factors have resulted in a continually evolving and complex burden of disease and an increased prevalence of chronic NCD in South Africa.
To treat these rapidly emerging chronic NCD, South Africans rely on Western pharmaceutical medicine, but also display widespread dependence on traditional herbal medicines (THM). The WHO defined THM as, “health practices, approaches, knowledge, and beliefs incorporating plant, animal and mineral based medicines, spiritual therapies, manual techniques and exercises, applied singular or in combination, to treat, diagnose and prevent illnesses or maintain well-being.”8 WHO estimates are that 80% of rural populations in developing countries depend on THM for their health care needs.9 Several cultural and socioeconomic factors contribute to the widespread utilization observed throughout these populations. The use of THM in South Africa is an inherent, culturally accepted practice with traditional healers more positively viewed than the public health care system.10 The overall inadequacy of the South African health care system, in combination with the high cost of Western pharmaceutical medicine, serves to drive patients toward THM use.11 The relative ease of access and effectiveness of THM compared to conventional drugs, in terms of side effects, also contributes to patients preferentially selecting THM. Cultural acceptance, accessibility, and affordability all contribute to this observed THM utilization within the South African population. Some of the most commonly used medicinal plants are outlined in Table 1. So far, researchers have focused on the clinical and experimental aspects of THM use; hence, there exists a lack of available literature addressing the cost and utilization of THM for NCD. Therefore, the purpose for this study will be to determine the cost and utilization of resources on THM for NCD in South Africa.
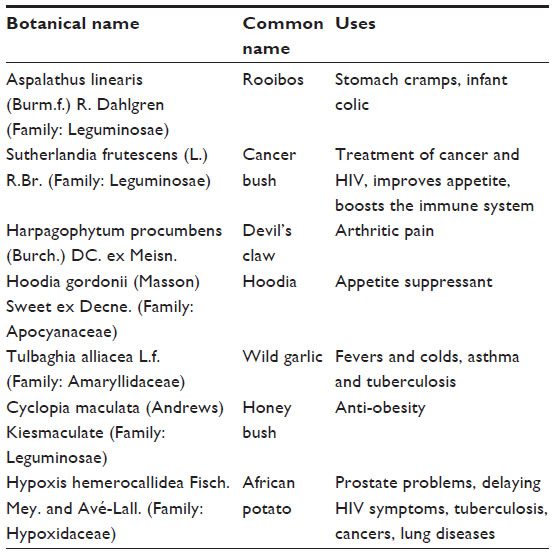 | Table 1 List of commonly used medicinal plants in South Africa |
Methodology
Study design and research plan
Through this cross-sectional descriptive study, we will perform economic analyses on THM use as an extension of the Prospective Urban and Rural Epidemiological (PURE) study in South Africa. The PURE study is a global population-based cohort study in 17 low-, middle-, and high-income countries. The primary aim of the PURE study is to examine societal influences, the prevalence of risk factors, incidence of chronic NCD, and changes in risk factor rates in the population over time. Data on baseline demographic characteristics, clinical-medical history, socioeconomic status, and lifestyle behaviors were collected, and has been described elsewhere.12 The PURE study methodology paper mentions that data were collected by an adult questionnaire; using two measures of resting blood pressure; fasting blood sample for biochemical and genetic testing; the Framingham Risk Score and its components and the prevalence of cardiovascular disease.12 These data and questions on THM use will be used to link NCD and THM.
Utilizing the pre-existing PURE study questionnaire, we will be obtaining additional information at the individual, household, and community level on the expenditure and utilization of THM for chronic NCD. Using this information, an economic evaluation will be conducted to assess how family structure, socioeconomic status, and health care utilization influence, and are influenced by THM use. By using willingness to pay methods, we will be able to measure cost benefit analysis, and answer how much they are willing to pay for THM for perceived improvements in health.
Study setting
The current investigation will be conducted on the PURE study sample in Langa, an urban township located in Cape Town in the Western Cape Province, and Mount Frere, a small rural town located in the Eastern Cape Province, South Africa (Figure 1).
 | Figure 1 Study Sites: Langa, Western Cape Province, and Mount Frere, Eastern Cape Province, South Africa. |
Sampling for PURE – South Africa
The cohort was drawn to represent the adult population resident in both communities (Langa and Mount Frere) but also with mindfulness to the possibility of follow-up of participants. These communities were purposely selected on the basis of having a relatively stable (less migratory) black population, thus allowing for feasibility of follow-up in a prospective cohort study. For the urban community (Langa), households were grouped into three development areas recognized administratively by the City of Cape Town and which mirror the socioeconomic status of the residents. A street map obtained from the City of Cape Town was used to randomly select streets in each of the three areas. Once a street was selected, a systematic sample of every second house was approached for possible inclusion in the study.
Households’ eligibility was based on the criteria that at least one member should be between ages 30 and 70 years, and that this person intends to live in the current home for the following 4 years. All households with eligible individuals were approached by trained field workers for recruitment. All individuals who were “usual residents” were considered “household members” and eligible to be selected for the study. A “usual resident” was defined as one “who eats and sleeps in the household on most days of the week and in most weeks of the year and considered the household his/her primary place of habitation”.
For the rural community (Mount Frere), the absence of delineated streets precluded the possibility to follow the same sampling approach used for the urban township. Therefore, a cluster sampling approach of houses in the community was undertaken according to the division of areas by the clan heads. All households within the clusters were included provided that there should be a household member aged 30–70 years. The initial recruitment took place between April and August 2009 with close to 1,000 participants recruited in both locations. A second phase recruitment took place between April and August 2010. The response rate was 85%. All the individuals who agreed to participate provided written informed consent.
Sampling for the current study
The sampling frame for the current study includes the 2,000 participants who took part in the original South African PURE study. An administrative spreadsheet used to capture participants’ information throughout the PURE follow-up period will be used to randomly select a sample of 1,000 participants comprising 500 participants from the rural site and 500 participants from the urban site. To facilitate the data collection process, their names, contact details, and residential addresses were noted.
Data collection plan
We will align PURE THM study with the larger PURE study. We will collect data once a year and there is data collection for follow-up and anthropometric measures. Appointments with participants to collect data will be made by means of a telephone call. Using their residential addresses, trained interviewers will visit the households/individuals on the day of the appointment to collect data on the epidemiology of THM use for chronic conditions. All the data will be collected (2013–2014) using structured questionnaires administered by means of face-to-face interviews. The interviews conducted by trained data collectors will be in the preferred language of the respondent (English or Xhosa). Respondents’ demographic characteristics’ (age, sex, education, marital and employment status), clinical-medical history, and THM usage (duration of use, condition for use, dosage, and form) will be recorded. The PURE THM sub-study addressed questions as follows: basic demographics; medical-clinical characteristics – general well-being; visits to clinic and hospital; level of illness/disability; any NCD/conditions; medication use both conventional/prescription; health seeking behavior; question on migration patterns (urban/rural); traditional medicine/complementary and alternative medicine (CAM) use – practice, type of medicines/practice and for what condition; frequency and purpose; length of practice; opinions/belief of practice (Likert scale); and economics of THM use – monthly expenditure. We will be collecting information on: source of THM - whether provided by practitioner or self-administered; location of purchase/acquisition; type of THM - whether plant or herbal; and method of THM administration - whether ingested as tea or tincture, or in another form etc. The quality of data collected is maintained by using standardized protocols and centralized training. The additional economic questions utilized in our study have been developed and validated based on evidence provided through previously conducted research.13–20 These additional cost estimation questions are:
- How much do you spend (South African Rand, ZAR) on herbal remedies monthly/yearly?
- How much did you/your family pay (ZAR) for herbal remedies last year?
- What percentage of your income/family income have you spent on herbal remedies last year/last month?
- How much are you willing to pay (ZAR) for herbal remedies to feel better?
- How much are you/your family members willing to pay (ZAR) for herbal remedies per year?
Studies conducted in the future could modify these questions to best reflect specific demographic and cultural aspects of the population being evaluated. The large size and extended duration of this study, in combination with the resultant familiarity of the South African population with the research team will all likely serve to strengthen the results obtained and increase the robustness and reliability of our findings.
The Senate Research Committee of the University of the Western Cape, South Africa, approved the study protocol.
Economic evaluation procedure
To assess the role and importance of economic evaluation of THM use for chronic NCD, cost-analysis, cost-comparison, cost-benefit, and multiple sensitivity analyses will be conducted. These economic evaluations will be performed to determine a variety of factors regarding patients’ THM use and overall health care expenditure from their viewpoint. All results will be reported in ZAR utilizing the 2013 value. This information can be analyzed to determine THM spending patterns at the individual, household, and community levels. The study will assess the geographic and socioeconomic influence of THM spending and utilization, variations in spending based on perceived health status, marital status, and whether spending patterns have any impact on hospitalizations and disability. Several regression models will be developed to assess spending determinants. Patient willingness to pay methods and economic data will be utilized to perform cost-benefit analyses regarding THM use. Costs will be calculated on a weekly, monthly, or annual basis to determine temporal relationships associated with THM spending and utilization. Data will be further extrapolated to determine direct health care costs, and the impact of THM utilization on health outcomes and expenditure. The methodology of our study design is shown in Figure 2. As the figure displays, the PURE study serves to provide the background demographic information at the community and household levels. Using this information, an economic evaluation will be conducted to assess how family structure, socioeconomic status, and health care utilization impact on, or are impacted by THM use.
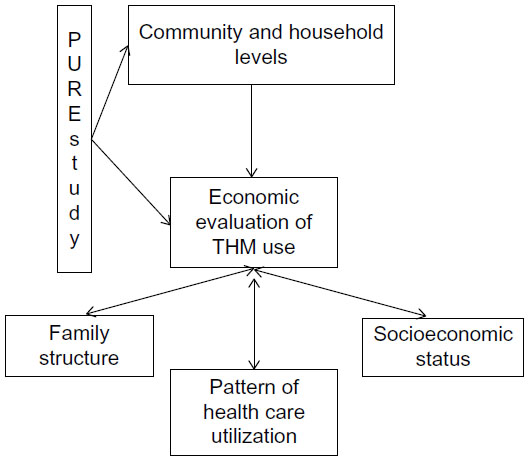 | Figure 2 Study design and conceptual framework. |
We will be collecting household and community level estimates on the expenditure and utilization of THM for chronic NCD from this population. Individually, we will ask them, “How much do you spend (ZAR) on herbal remedies monthly?”, and “How much did you/your family pay (ZAR) for herbal remedies?” We will also ask them how much they spent in the previous year. Based on these individual- and family-level data we will be able to calculate community-level and eventually population-level spending, as this is a population-based epidemiological cohort study. We will be able to extrapolate these numbers to provide a yearly spending pattern.
Sensitivity analysis
One-way sensitivity analyses will be conducted to determine independent associations between geographic location, employment status, educational level, marital status, and perceived health status on the prevalence of THM expenditure. Several hypothetical scenarios will also be analyzed to gather maximum and minimum cost ranges using the baseline demographic and economic data obtained from the survey. These parameters will include the effect of change in currency value both geographically and temporally throughout the study period, as well as comparisons to other study outcomes estimating the THM prevalence in South Africa.
Economic and policy implications
The results obtained can provide an abundance of information to guide economic and governmental policy decision-making. These data will enable appropriate health policy decision-making, by informing policymakers on the prevalence and the geographic and socioeconomic determinants of THM expenditure within the population. Geographic variation in spending and THM costs will be determined and used to assess factors that correlate with THM use. Only two other studies using atopic dermatitis patients and pediatric patients characterized the utilization patterns of traditional Chinese medicine in Taiwan.21,22 Programs and initiatives can then be targeted toward identified areas of interest to provide education and interventions in those sections of the population with the greatest need. Since the individual costs of THM are not regulated or have a standardized value, information obtained through this study can be utilized to assess these differences and determine underlying factors contributing to these disparities. This insight into spending patterns as well as the individual and population level factors that contribute toward THM spending can aid in the development and implementation of guidelines or standardized legislation governing THM use and distribution.
Comparative effectiveness research issues
The results of this study can be used to perform further studies assessing the comparative effectiveness of THM use within the South African population. Comparative effectiveness research (CER) is defined as a measure of the extent to which an intervention, when deployed in the field in routine circumstances, does what it is intended to do for a specific population.23 Thus, effectiveness has become more of a measure of the real impact which a therapeutic option will have when used by a given population that is actually using that treatment in practice. Due to the increased prevalence of integrative medicine in this population, it is crucial to consider potential implications and their use on CER, as patients’ CAM use can influence clinical trial efficacy outcomes.
On the other hand, “efficacy”, as it is often used, has come to be defined as the extent to which a specific intervention is beneficial under ideal conditions.23 The common use of this term then refers more specifically to benefit derived from clinical trials, which provide the basis for most of the efficacy claims of medications. Globally, in locations where THM use is already standard practice in the population, assessing the comparative effectiveness of these treatments and evaluating their effects could prove more beneficial than attempting to alter people’s way of life by imposing westernized medicinal practices.
Currently, most trials that are conducted attempt to determine efficacy of treatment options; however, reverse research and CER are emerging as a pragmatic approach to optimizing global treatment options, especially considering costs. The best treatment option for a given patient or population is not necessarily the most efficacious, but the most effective. Utilizing information obtained through the current study can aid the overall economic impact on health care delivery in South Africa. It is important that decision-makers develop guidelines to address a standardized approach of incorporating CAM into CER.
As opposed to traditional clinical trials, CER also relies on input not only from the researchers, but also from all involved parties, including patients, physicians, and payers in the identification of research questions.24 These same groups are also included in the evaluation of the results and the dissemination of the findings.24 This allows the research to be meaningful to the patient population studied and the results to be shared with them, particularly utilization and costs. The South African population’s unique mixture of reliance on pharmaceutical medicine and THM ensures that this patient population can prove to be an ideal arena to conduct CER. Once available, we plan to share the results of this research with the population who participated in the data collection.
Education of health care professionals and special considerations
With current data largely unknown on the spending, utilization, and reliance on THM for chronic NCD in the South African population, the results of this study will provide new pharmacoeconomic information. These data can be utilized to further investigate their comparative effectiveness. Economic data can provide an additional facet of analysis when conducting CER by enabling the evaluation of the distribution and allocation of resources in patient populations of various levels of economic prosperity. The prevalence and economic implications of THM use on chronic NCD can highlight the importance to the health care community of inquiring about spending patterns and determining populations more likely to be reliant on THM. The unknown prevalence of THM expenditure and lack of personal, family, and societal level data could lead to detrimental and deleterious health effects for this population and the global population. This information can then be used to guide patient therapy, which impacts clinical decision-making at the patient and community level, eventually resulting in an improved quality of care at a lower cost. Through utilization of prevalence data in combination with economic analyses, the provision of the most effective therapeutic options for patients from varying degrees of socioeconomic prosperity can be implemented.
A similar study could be conducted in the United States, where an estimated 20% of the population relies on THM, commonly referred to as CAM, which accounts for annual expenditures in excess of US$27 billion.25,26 Integration of CAM within the health care system could be facilitated through CER to establish viable alternative treatment options for patients. Pharmacists could be uniquely qualified to aid in this integration; however, curricula are currently insufficient and would need to be altered to improve knowledge of these treatments. Perhaps third-party payers can utilize this guidance to make informed, evidence-based decisions in their drug formulary processes. Expansion of the curriculum and an increased interest in CER can serve to aid in the education of providers and ultimately the integration of THM therapies. This information on utilization and cost, in conjunction with evidence on safety and efficacy of CAM could then be used by third-party payer organizations to possibly reduce health care costs while improving the overall quality of health care delivery.27
Limitations and strengths
Data collection is currently in progress, thus no outcome data are available at this point in time. Reproduction of a similar economic analysis might be difficult because of an inability to locate a large epidemiological study similar to the PURE study with which to partner. The current study primarily focuses on expenditures on THM; however, no efficacy data have been obtained. Therefore, we will be able to analyze the costs and spending patterns of the South African population, but cost-efficacy analyses will not be conducted as there are no outcome data. Willingness-to-pay methods are being utilized in this study to evaluate how much additional money a person with NCD is willing to pay to feel better, and will give us insight about a patient’s perception of THM use. Cost of each herbal medicine is not provided in this study, as the individual costs of THM are not regulated nor do they have a standardized price value in South Africa. Future studies conducted in this area could seek to pair cost information with patient outcomes and efficacy to perform cost-efficacy analyses and CER on THM. Similar research could also focus on adverse event monitoring, drug–herb interactions, and other clinical events associated with herbal medicine safety. A similar study could be conducted to determine the economic implications of herbal medication use in the United States, where an estimated 20% of the population is actively using herbal medications.25
Conclusion
Understanding the economic implications associated with the prevalent use of THM in South Africa can provide a foundation for health policy decision-making. These results can be used to highlight issues associated with chronic NCD as well as the use of THM in the South African population. The awareness that is generated can be used as leverage to garner long-term commitment and involvement from interested parties to provide aid and promote disease prevention.
Information obtained can help to direct future studies in this area, improve future public health initiatives within South Africa, and serve to optimize the integration of THM use with traditional pharmaceutical medicine to ultimately improve patient outcomes and reduce the burden of health care cost.
Acknowledgments
Part of this concept paper was presented at 141st Annual Meeting and Expo, American Public Health Association, held at Boston, MA, USA, on November 2–6, 2013. This study was partially funded by The University of Missouri South African Education Program (UMSAEP).
Disclosure
The authors report no conflicts of interest in this work.
References
Daar AS, Singer PA, Persad DL, et al. Grand challenges in chronic non-communicable disease. Nature. 2007;450(7169):494–496. | |
Global Status Report on Non-Communicable Diseases 2010. World Health Organization. Available from: http://www.who.int/nmh/publications/ncd_report_full_en.pdf. Accessed May 18, 2015. | |
World Health Organization [homepage on the Internet]. The global burden of disease: 2004 update. Geneva: World Health Organization; 2008. Available from: http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/. Accessed May 18, 2015. | |
Department of Health, Medical Research Council, OrcMacro. South Africa Demographic and Health Survey 2003. Pretoria: Department of Health; 2007. | |
South Africa Demographic and Health Survey, 1998. Department of Health, Medical Research Council, Demographic and Health Surveys Macro International Inc. Available from: http://www.mrc.ac.za/bod/dhsfin1.pdf. Accessed September 13, 2013. | |
Norman R, Bradshaw D, Schneider M, et al. A comparative risk assessment for South Africa in 2000: towards promoting health and preventing disease. S Afr Med J. 2007;97(8 Pt 2):637–641. | |
Joubert J, Bradshaw D. Population ageing and its health challenges in South Africa. In: Steyn K, Fourie J, Temple N, editors. Chronic Disease of Lifestyle in South Africa: 1995–2005. MRC Technical Report. Cape Town: South African Medical Research Council; 2006:204. | |
World Health Organization [homepage on the Internet]. Factsheet 134: Traditional Medicine. Geneva: World Health Organization; 2003. Available from: http://www.who.int/mediacentre/factsheets/2003/fs134/en/. Accessed May 18, 2015. | |
Regional Committee for Africa, World Health Organization. Promoting the role of traditional medicine in health systems: a strategy for the African region. Report of the Regional Director presented at: Fiftieth session of the Reginal Committee for Africa, Ouagadougoi, Burkina Faso; August 28–September 2, 2000. | |
Lokita A. Reasons Given by Hypertensive Patients Seen at Natalspruit Hospital, Gauteng, for Consulting Traditional Healers [dissertation]. Medunsa: University of Limpopo; 2009. | |
Osamor PE, Owumi BE. Complementary and alternative medicine in the management of hypertension in an urban Nigerian community. BMC Complement Altern Med. 2010;10:36. | |
Teo K, Chow CK, Vaz M, Rangarajan S, Yusuf S; PURE Investigators-Writing Group. The prospective urban rural epidemiology (PURE) study: Examining the impact of societal influences on chronic non-communicable diseases in low-, middle-, and high-income countries. Am Heart J. 2009;158(1):1–7. e1. | |
Aday LA, Cornelius L. Designing and conducting health Surveys: A comprehensive Guide. 3rd ed. San Francisco, CA: Jossey-Bass; 2006. | |
National Institute for Health and Clinical Excellence (NICE). Developing Costing Tools Methods Guide. Available from: http://www.nice.org.uk/media/F3E/57/DevelopingCostingToolsMethodsGuide.pdf. Accessed October 16, 2014. | |
International Center for Diarrheal Disease Research, Bangladesh [homepage on the Internet]. Cost of utilizing healthcare services in Chakaria, a rural area in Bangladesh. Available from: http://www.icddrb.org/publications/cat_view/10043-icddrb-documents/10058-icddrb-reports-and-working-papers/10060-research-briefs/10253-fhs-research-brief. Accessed May 18, 2015. | |
Rasu R, Rianon N, Shahidullah S, Faisel A, Selwyn B. Effect of educational level on breast cancer knowledge and screening practices in Bangladesh women. Health Care Women Int. 2011;32(3):177–189. | |
Drummond MF, O’Brien B, Stoddart G, Torrance G. Methods for the Economic Evaluation of Health Programmes. 2nd ed. New York: Oxford University Press; 1997. | |
Fox M, Voordouw J, Mugford M, Cornelisse J, Antonides G, Frewer L. Social and economical costs of food allergies in Europe: development of a questionnaire to measure costs and health utility. Health Serv Res. 2009;44(5 Pt 1):1662–1678. | |
Cooper NJ, Mugford M, Symmons DP, Barrett EM, Scott DG. Development of resource-use and expenditure questionnaires for use in rheumatology research. J Rheumatol. 2003;30(11):2485–2491. | |
Neumann PJ, Palmer JA, Nadler E, Fang C, Ubel P. Cancer therapy costs influence treatment: a national survey of oncologists. Health Aff (Millwood). 2010;29(1):196–202. | |
Lin JF, Liu PH, Huang TP, et al. Characteristics and prescription patterns of traditional Chinese medicine in atopic dermatitis patients: ten-year experiences at a medical center in Taiwan. Complement Ther Med. 2014;22(1):141–147. | |
Huang TP, Liu PH, Lien AS, Yang SL, Chang HH, Yen HR. A nationwide population-based study of traditional Chinese medicine usage in children in Taiwan. Complement Ther Med. 2014;22(3):500–510. | |
Last J, Spasoff RA, Harris S. A Dictionary of Epidemiology. 4th ed. Oxford: Oxford University Press; 2001. | |
VanLare JM, Conway PH, Sox HC. Five next steps for a new national program for comparative-effectiveness research. N Engl J Med. 2010; 362(11):970–973. | |
Bent S. Herbal Medicine in the United States: Review of Efficacy, Safety, and Regulation. J Gen Intern Med. 2008;23(6):854–859. | |
National Academy of Sciences. Complementary and Alternative Medicine in the United States. Washington, DC: National Academy of Sciences; 2005. | |
Hill JD, Goolsby KL, Rasu R. Complementary and Alternative Medicine Use in Comparative Effectiveness Research and Implications to Third Party Payers. Poster presentation at: Academy of Managed Care Pharmacy (AMCP) Annual Meeting; April 2014; Tampa, FL. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.