")
Back to Journals » Nursing: Research and Reviews » Volume 4
The mental health benefits of regular physical activity, and its role in preventing future depressive illness
Authors Stanton R, Happell B, Reaburn P
Received 26 February 2014
Accepted for publication 26 March 2014
Published 23 May 2014 Volume 2014:4 Pages 45—53
DOI https://doi.org/10.2147/NRR.S41956
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Robert Stanton,1 Brenda Happell,1 Peter Reaburn2
1Institute for Health and Social Science Research, Centre for Mental Health Nursing Innovation and School of Nursing and Midwifery, Central Queensland University, Rockhampton, QLD, Australia; 2School of Medical and Applied Sciences, Central Queensland University, Rockhampton, QLD, Australia
Abstract: There is a large body of literature which examines the mental health benefits of physical activity. In general, studies report an inverse, dose dependent relationship between leisure-time physical activity participation, and mental health outcomes. Studies also show a positive association between maximal aerobic capacity and general well-being. More recent studies have confirmed the positive effects of physical activity participation on cognition, including the treatment and prevention of dementia. The current exercise prescription suggested for the treatment of depression is similar to that recommended to the general population for the development and maintenance of cardiorespiratory fitness. There is also strong evidence from large population level studies that long term physical activity participation reduces the risk of future depressive illness. From the available evidence, it would appear that physical activity performed at a frequency, intensity, and duration which is substantially less than that required for the development and maintenance of cardiorespiratory and muscular fitness in the general population, may afford significant benefits in reducing the risk of future depressive illness. This may be particularly encouraging for people with prior depressive illness, or at high risk of future depressive illness, since this vulnerable population already faces significant barriers to physical activity participation over and above those encountered by the general population.
Keywords: exercise, major depression, depressive disorder, preventive medicine
Introduction
Physical activity is known to confer significant overall health benefits.1–3 Current recommendations indicate that moderate intensity aerobic activity should be performed at least 5 days per week, for a minimum of 150 minutes per week, or more vigorous aerobic activity performed at least 3 days per week for a minimum of 75 minutes per week. This program of activity should be accompanied by resistance exercise at least 2 days per week.2 People who undertake even modest amounts of regular physical activity have been shown to have lower rates of chronic diseases such as type II diabetes, cardiovascular disease, and some cancers.1 However, it has recently been estimated that almost one third of the world’s population fail to achieve the minimum level of physical activity required to achieve these health benefits.4 In some parts of the world this figure approaches half of the population.4 Compared to moderate intensity physical activity, more vigorous activity is recognized to confer additional health benefits.3 Alarmingly, less than one third of the population report engaging in this form of activity at levels sufficient to experience these additional benefits.4
In addition to the physical health benefits, exercise and physical activity participation is increasingly linked to improved mental health. The present review will draw from, and briefly summarize the research literature on the mental health benefits of physical activity. It will provide evidence for the efficacy of physical activity in the treatment of depression, and then consider the evidence for the role of physical activity in the prevention of future depressive illness. Importantly, this review will provide a framework for the prescription of physical activity interventions likely to afford benefit to those with depression. This is important since, in general, clinical practice guidelines for the inclusion of physical activity in the treatment of mental illnesses are lacking in such detail. Finally, this review will highlight the limitations of the current body of literature and offer suggestions for future research studies.
The mental health benefits of physical activity
Mental illnesses are estimated to contribute to 13% of the total global burden of disease.5 People diagnosed with mental illness experience significant distress and disability, and the financial and personal cost of mental illness, including loss of productivity and work participation, is significant.6 Physical activity is one strategy often recommended for people with mental illness with three recent, large cross-sectional studies showing a strong association between physical activity participation and mental health.7–9
Firstly, Galper et al reported an inverse dose-dependent relationship between maximal aerobic capacity and depression score measured using the Centre for Epidemiologic Studies Depression Scale (CES-D) in a sample of more than 6,000 adult men and women as part of the Aerobic Centre Longitudinal Study in the US.7 Participants were stratified into three groups according to aerobic fitness level measured using a graded treadmill test. Significant differences were observed between low, moderate, and high aerobic fitness groups for mean depression score. In a subsequent analysis, participants were stratified according to physical activity participation. Those categorized as inactive exhibited significantly higher depression scores than those categorized as insufficiently active, sufficiently active, or highly active. Participants in this study also completed the General Well-Being Schedule.7 In a manner similar to that found for depression scores, a positive graded dose-response relationship was observed between both maximal aerobic capacity and physical activity participation, and well-being scores. In summary, those with the highest levels of aerobic fitness and the highest levels of physical activity participation also reported the highest level of general well-being.7
Secondly, Harvey et al collected physical activity data using a questionnaire which separated leisure-time and occupational physical activity; and mental health using the Hospital Anxiety and Depression Scale (HADS)10 from 40,401 Norwegian adults as part of the Health Study of Nord-Trøndelag County (HUNT-2) study.8 The results showed an inverse association between leisure-time physical activity participation, but not occupation physical activity, and depression, with and without comorbid anxiety. There was no difference between light and vigorous physical activity in the association with depression. Light intensity, but neither vigorous intensity leisure-time physical activity nor occupational physical activity, was associated with a lower likelihood of anxiety symptoms. While the strength of this study was its sample size, the interpretation of the findings are limited by the use of a self-report measure of physical activity for which the validity is not reported, as well as the inability of the HADS to provide a clinical diagnosis of either depression or anxiety. Nonetheless, the findings of this study offer support for the positive association between physical activity participation and improved mental health.
More recent evidence demonstrates the benefits of physical activity participation on cognition. Smith et al reported that even modest engagement in physical activity may be neuroprotective against cognitive decline in later life.9 Their review provided evidence from numerous cross-sectional studies which demonstrate the positive dose-dependent association between overall and leisure-time physical activity, and cognitive function. In support of the findings of cross-sectional studies, this review provided evidence from a number of prospective studies. These studies demonstrate a similar positive dose-dependent relationship between physical activity and the risk of cognitive decline and dementia in later life with risk reductions of up to 50%.9 In the same review, Smith et al presented the outcomes of physical activity interventions which showed improved cognition in both healthy populations, and in those with cognitive impairment, from aerobic such as walking and resistance training. The review offers substantial support for a range of physical activity interventions across a range of populations for the treatment and prevention of cognitive decline. While the exact mechanisms for such effects remain elusive, it is possible that a reduction in vascular risk factors, increased cerebral blood flow, and an increase in neural growth factors may play a role. More studies including measurements of these factors are critical to improve our understanding of the interaction between physical activity participation and cognition.
Previously mentioned studies have informed recent systematic reviews and meta analyses which confirm the positive associations between physical activity and mental health. These associations appear to remain, following adjustment for confounding variables such as age, sex, socioeconomic status and ethnicity.11 What remains to be evaluated are studies based on theoretical models of behavior change to determine their relative efficacy in ensuring successful delivery and uptake of physical activity interventions at population level.
Physical activity and the treatment of mental illness
In addition to the positive associations between physical activity participation and positive mental health outcomes, data from short-term interventions also demonstrate the efficacy of physical activity as a stand-alone, or co-intervention in the treatment of a range of mental illnesses including depression, schizophrenia, and anxiety conditions.12–14 However, the generalizability and usefulness of individual studies is often hampered by poor methodological design, failure to fully report intervention details, and lack of long term follow-up.12,15,16 Nonetheless, the outcomes of numerous trials investigating the effect of physical activity on mental illness have led to the inclusion of physical activity recommendations in the treatment guidelines for a number of mental illnesses including depression and schizophrenia.17–20
Exercise and the treatment of depression
Globally, the prevalence and incidence of major depressive disorder is reported to be 4.7% and 3.0%, respectively.21 Support for physical activity in the treatment of depression is increasing with a number of clinical practice guidelines for the treatment of depression now including recommendations for physical activity, albeit with varying levels of detail.17–19 For example, Clinical Guidelines from the Canadian Society for Mood and Anxiety Treatments (CANMAT) suggest there is “reasonable evidence” for the role of exercise in the treatment of depression in adults.18 CANMAT guidelines indicate there is Level 2 evidence (at least one randomized controlled trial [RCT] with an adequate sample size and/or meta analysis with wide confidence intervals) for the use of physical activity as an adjunct to medication in the treatment of mild to moderate major depressive disorder, however CANMAT guidelines do not support the use of exercise as monotherapy. The format of the CANMAT guidelines is one of question/answer. Therefore, the document fails to provide clinicians with recommendations for the frequency, intensity, type or duration of exercise which may afford clinical benefits. The latter is critical for the delivery of physical activity interventions for clinicians since manipulating these variables has substantial influence on the expression of physiological outcomes and is likely to influence mental health outcomes. More detailed guidelines may be needed to allow clinicians to adequately develop and deliver physical activity interventions which contribute to improved outcomes for people with depression.
Guidelines from the Scottish Intercollegiate Guidelines Network (SIGN) for the non-pharmaceutical management of depression in adults draw upon high quality studies with Level 1++ (high quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low risk of bias) and Level 1+ (well conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias).19 They provide Level B recommendations (extrapolated evidence from studies rated as Level 1++ or Level 1+) for structured exercise which meets the public health dose defined as activity performed on 3 or more days per week at an intensity sufficient to provide an energy expenditure of 70%–80% of the heart rate reserve (difference between resting and maximum heart rate). As an example, these guidelines suggest that walking at a moderate intensity, sufficient to be slightly out of breath, on most days of the week, will meet these recommendations. Furthermore, the SIGN guidelines include practice points suggesting the use of a screening questionnaire to determine the need for additional investigation of clinical risk factors, the referral to exercise counselling services for relevant and accessible activities, and the use of goal setting or exercising with a partner, to assist with maintaining motivation and adherence.19 These SIGN guidelines offer greater direction and are more likely to be used by clinicians compared to those cited previously.18
Although developed earlier, the guidelines of the National Institute for Clinical Excellence (NICE)17 in the UK extend on those offered by SIGN, to offer an even more prescriptive approach. Specifically, NICE guidelines suggest that for persistent sub-threshold depressive symptoms, or mild to moderate depression, patients are encouraged to engage in aerobic exercise delivered in a group format by a competent practitioner. Sessions should be 45–60 minutes in duration and be undertaken three times weekly over a period of 10–14 weeks.17 While failing to address the issue of exercise intensity, the NICE guidelines offer additional guidance over those offered elsewhere with respect to session duration and length of intervention.
Individually, these clinical guidelines statements, while acknowledging the benefits of exercise in the treatment of depression, do not address all the specific variables pertaining to the prescription of physical activity for people with depression. This may be due to the application of the guidelines with respect to the clinical diagnosis of depression. It is likely due to one of the significant limitations surrounding studies investigating physical activity interventions for people with depression, that of the reporting of intervention variables. Despite previous reviews calling for the need for better reporting,16,22,23 there remains significant heterogeneity surrounding the program variables employed in studies investigating the effects of exercise in people with depression.12
To address this uncertainty in the previous literature, we recently conducted a systematic review of studies reporting positive outcomes from exercise in people with depression to evaluate the exercise prescription variables most likely to contribute to positive outcomes. Our review concluded that exercise which is likely to confer benefits for people with depression is not dissimilar to that recommended for the general population.24 That is, a program of supervised aerobic exercise such as walking or cycle exercise, undertaken three times per week at moderate or patient-preferred intensity with sessions of 30–40 minutes duration appear beneficial. Both individual and group exercise formats appear to be of value. The recommended intervention duration is at least 9 weeks, and should ideally be ongoing. Our findings are consistent with previous reviews examining the exercise program variables for the treatment of depression25 and, arguably, highlight the utility of the population health recommendations for physical activity participation.2 However, a further significant limitation of many studies investigating the effect of physical activity participation on depression or other mental illness is the lack of long term follow-up.
Despite the inclusion of the physical activity and exercise recommendations in the published clinical practice guidelines for the treatment of depression and other mental illnesses, some reviews have been more guarded in their conclusions. For example, the most recent Cochrane Review reported that, compared to no treatment, or a controlled intervention, exercise provided a moderate clinical effect (effect size −0.62, 95% confidence interval −0.158–0.42).12 However, compared to psychological or pharmacological interventions, exercise offered no significant advantage.12 Moreover, when only high quality trials were included (adequate allocation concealment, intention-to-treat analysis, and blinded outcomes), exercise was found to have only a small clinical effect. Therefore, more robust and larger trails are needed before a conclusive statement can be made regarding the effectiveness of physical activity as a treatment strategy for depression.12
It is also important to appreciate that physical activity interventions which differ from the more commonly performed aerobic or strength training programs, are gathering research support. For example, a recent systematic review and meta-analysis of 12 studies investigating the effect of yoga therapy on depression concluded that, in the short-term, yoga is moderately more effective compared to usual care, however it found limited evidence for effectiveness compared to aerobic exercise or relaxation therapy.26 However, long term follow-up showed no difference between yoga and usual care, group therapy, or social support.26 Analysis of the individual studies suggested that neither complex nor exercise-based yoga therapy offers any advantage over group therapies, social support, massage, or pharmacotherapy. As with other studies investigating the effect of other forms of physical activity on depression, methodological differences and poor reporting of intervention details may contribute to the lack of conclusive evidence.
Tai Chi has also been demonstrated to have beneficial health effects. A recent systematic review reported that 16 of the included 42 studies showed that Tai Chi produced significant improvements in depression scores compared to other treatments such as medication, non-exercise, or sham exercise controls.27 A subsequent meta-analysis included only three studies for final analysis and reported a significant treatment effect of Tai Chi on depression symptoms as assessed using the CES-D, compared to waitlist or education controls, or other forms of exercise including martial arts training and sham exercise. While encouraging, studies on the effect of Tai Chi, similar to other physical activity interventions, are plagued by inconsistencies in intervention design, outcome measures, and populations under investigation.
In summary, there appears to be sufficient evidence for a range of physical activity interventions in the treatment of depressive illness. Trials are often limited by heterogeneous design, poor reporting, lack of long term follow-up, and inconsistent use of outcome measures. More robust, well designed studies are needed to confirm these findings. However, in light of these limitations, clinicians should be confident that, at worse, physical activity will not offer any disadvantage over other treatments.
Does physical activity prevent future depressive illness?
If physical activity is valuable in the treatment of depression, there may also be a number of advantages in its use as a means of providing a protective effect in reducing the risk of future depressive episodes. Firstly, physical activity is a low cost intervention which is easily accessible by a large proportion of the population. Secondly, physical activity is a safe intervention with few reported adverse events. Thirdly, physical activity interventions may be easily tailored to suit individuals with chronic disease or musculoskeletal conditions which may otherwise limit participation. Fourthly, physical activity interventions may be delivered using technology-based formats such as the Internet, which significantly reduces the geographic and time barriers. Finally, physical activity interventions offer additional health benefits, not only with regard to depressive illness, which may improve overall quality of life and reduce early mortality.
Recent studies have shown that physical activity undertaken during childhood is associated with a reduced likelihood of the development of depression during the adult years.28,29 These findings are consistent with the view that physical inactivity is an independent risk factor for the development of depression during adulthood.30,31 Indeed, a large number of previous studies demonstrate an inverse relationship between physical activity levels reported at baseline, and follow-up depression scores (for a comprehensive review see Mammen and Faulkner32). Moreover, from the available evidence, the review of Mammen and Faulkner concluded that the promotion of physical activity may alleviate the future burden associated with mental and physical illness.32 Despite this promising conclusion, from both a population health and clinician advice perspective, there remains a need to deliver useful and useable physical activity prescriptions to patients at risk of, or already diagnosed, with depression. In the following sections we provide a synthesis of this information using the frequency, intensity, time, and type principles of physical activity prescription.
Frequency: how often should one engage in physical activity?
The accepted frequency of physical activity participation for general health includes performing moderate intensity physical activity more than 5 days per week for a minimum weekly duration of 150 minutes, or vigorous physical activity at least 3 days per week for a minimum of 75 minutes per week, in addition to resistance exercise at least twice weekly.2 However, studies investigating the protective effect of physical activity on future depressive illness report that substantially less frequent participation may be beneficial.33–35 Hamer et al studied 4,323 men and women over a 4 year period, recording baseline and follow-up data using physical activity questions extracted from a validated population survey on health, and depressive symptoms using the CES-D.34 They concluded that either moderate or vigorous activity, undertaken at least once per week resulted in a significant reduction in the likelihood of developing future depressive illness compared to no activity.
The potential benefit associated with less frequent physical activity participation is supported in other studies. Bernaards et al assessed depression via CES-D and physical activity participation using a single item asking about strenuous leisure-time physical activity or sport participation in the past 4 months in 1,747 Dutch adults categorized by occupation to sedentary or non-sedentary.33 Those with a sedentary occupation who engaged in strenuous leisure-time physical activity at least once to twice a week were at a significantly lower risk of depression at 3 year follow-up compared to those who engaged in strenuous leisure-time physical activity less than once a month. More frequent (≥3 times weekly), or less frequent (1–3 times per month) participation in strenuous leisure-time physical activity was not associated with a reduced risk of depression at 3 year follow-up. For those with a non-sedentary occupation, no associations between leisure-time participation in strenuous physical activity were present.
As part of a longitudinal investigation into aging, Ku et al reported on a 7 year follow-up of 2,831 Taiwanese adults.35 Depressive symptoms were assessed using the abbreviated Chinese version of the CES-D, while physical activity was assessed using a single item with four response categories. Compared with those who were more active, those who participated in physical activity less than three times a week were significantly more likely to develop depressive illness at 7 year follow-up.35
Methodological disparities in the manner in which physical activity participation and depression symptoms are categorized make it difficult to draw firm conclusions. However, it would appear that physical activity participation less frequent than that recommended for the development and maintenance of cardiorespiratory and musculoskeletal fitness in apparently healthy adults, may be sufficient as a preventative measure against future depressive illness.
Intensity: is vigorous physical activity more effective compared to moderate levels?
Compared to moderate intensity physical activity, vigorous physical activity is known to offer additional general health benefits.3 In a study of more than 4,323 men and women, those individuals undertaking either moderate or vigorous physical activity were significantly less likely to develop depressive symptoms, compared to those undertaking light physical activity or sedentary behavior.34 However, while the odds ratio associated with moderate exercise was greater than that observed for vigorous exercise, the difference between those intensity groups was not statistically significant.34 In a large cohort of women, “brisk” or “very brisk” walking was associated with a reduced risk of depression, but “slow” walking was not.34 In contrast to the previously mentioned findings, Wise et al reported that, in a study of more than 35,000 black women in America, vigorous leisure-time physical activity, but not walking, was associated with a reduced likelihood of depression.36 However, when stratified by body mass index, a weak association was observed between walking and reduced risk of depression in obese women (body mass index >30 kg/m2). This finding suggests that, in obese women, the perceived exertion associated with brisk walking may be interpreted as vigorous.
In summary, vigorous physical activity may offer additional health benefits over and above that of moderate intensity physical activity. However, for the prevention of future depressive illness, moderate intensity exercise may convey mental health benefits in individuals with depression. While there may be a threshold below which there is little or no benefit, more moderate intensity physical activity may be preferred by a greater proportion of the population and may result in a more favorable effect response leading to greater adherence in the longer term. One substantial challenge with interpreting the findings of studies reporting the intensity of exercise is quantifying “light”, “moderate”, and “vigorous” physical activity where no objective measures of intensity are reported. With the development of wearable sensors to allow the upload, remote storage, and access to physical activity data, future studies may include objective measures of intensity and other physical activity parameters to elucidate those most strongly associated with the prevention of future depressive illness.
Time: is there an optimal duration of physical activity?
Public health recommendations suggest that 30 minutes of physical activity undertaken on all or most days of the week, even if undertaken in brief repeated episodes, is beneficial for health.2 Regarding the prevention of future depressive illness, studies show that as little as 10 minutes of physical activity per day may be beneficial.30 For example, in a 10 year prospective study of almost 50,000 women, the relative risk of depression associated with 10–29 minutes of physical activity per day, compared to <10 minutes per day was 0.82 (95% confidence interval, 0.76–0.87). Increasing amounts of physical activity up to more than 90 minutes per day were associated with further significant reductions in the risk of depression. In the study of black women in the US, the odds ratio of depression decreased when up to 3–4 hours per week (~30 minutes per day) of vigorous leisure time physical activity was undertaken, but did not increase beyond this duration.36
Taken together, these findings suggest that a moderate duration of physical activity may be equally as beneficial as longer bouts. This is important to acknowledge as a common barrier to engagement in physical activity is lack of time.37 Therefore, the health message should continue to reinforce the benefits of repeated brief bouts of activity for both physical and mental health.
Type: what type of physical activity is most effective?
Guidelines regarding the type of exercise beneficial for general health suggest a combination of both aerobic and strength exercise.2 Studies investigating the protective effect of physical activity on future depressive illness typically report the volume and intensity of physical activity. However, they rarely report the type of activity. Selected studies which have focused on walking as the principle physical activity behavior report that this activity is associated with a protective benefit from future depressive illness in both adult,38 and elderly39 populations. Data from the study by Smith et al demonstrates a significant inverse dose-dependent relationship between the volume of walking performed and the likelihood of developing depression at 8 year follow-up.39 Since walking is the most commonly performed physical activity, it seems logical this form of activity will be most commonly studied. However, as with physical activity interventions for the treatment of depression, the use of other modes of activity such as resistance exercise remains sparse. Until this type of exercise is more accurately measured in physical activity surveillance, a recommendation for resistance exercise in the prevention of future depressive illness cannot currently be made. However, at present, the inclusion of resistance exercise in physical activity programs is considered best practice and likely to offer additional benefits for general health such as improved body composition, management of blood pressure, and increased insulin sensitivity.2
Do changes in physical activity patterns make a difference?
Changes in habitual physical activity patterns are a natural phenomena and can occur in response to a variety of life events such as a change in occupation, place of residence or chronic illness. In general, studies show that a reduction in physical activity over time is associated with an increased likelihood for the development of future depressive illness, with studies reporting up to a 10-fold increase in the likelihood of developing future depressive illness.34,36 Studies also report that increasing physical activity participation leads to a reduction in the risk of future depressive illness.30 These findings suggest that the effect of physical activity on the risk of future depressive illness may be a transient feature, and that, as with other physical and health improvements associated with physical activity participation, one must maintain participation in order to maintain the benefits.2
Are there risks associated with physical activity participation?
In general, physical activity participation is associated with low risk. However, the risk of adverse cardiometabolic and musculoskeletal events may be increased during more vigorous intensity of physical activity.40 Moreover, unaccustomed activity is more likely to result in post-exercise muscle soreness, injury, and tiredness which may be minimized by commencing with very moderate amounts of exercise and progressing in a very gradual manner.41
In an effort to minimize any potential risk, the use of a pre-exercise questionnaire administered by an appropriately qualified person such as a medical practitioner or exercise physiologist may be valuable, but the need for extensive diagnostic screening is usually unnecessary.2 The need for supervision during physical activity participation may not be associated with a reduced risk of adverse events. However, a review of the exercise prescription variables associated with positive outcomes for people with depression recommends some degree of supervision.24 This may be of greater benefit during the commencement of a physical activity program, or when motivation and subsequent engagement subsides.
Summary
Table 1 summarizes the physical activity parameters likely to contribute to the prevention of future depressive illness, compared to recommendations for the general population. From the limited evidence available, it would appear that physical activity performed at a frequency, intensity, and duration which is substantially less than that required for the development and maintenance of cardiorespiratory and muscular fitness in the general population, may afford significant benefits in reducing the risk of future depressive illness. This may be particularly encouraging for those with prior depressive illness, or at high risk of developing depressive illness, since this vulnerable population already faces significant barriers to physical activity participation over and above those encountered by the general population. It should be recognized, however, that this level of physical activity highlights the lowest level of each parameter shown to result in positive outcomes and further studies are needed to confirm the combination of parameters best suited to reducing the risk of future depressive illness.
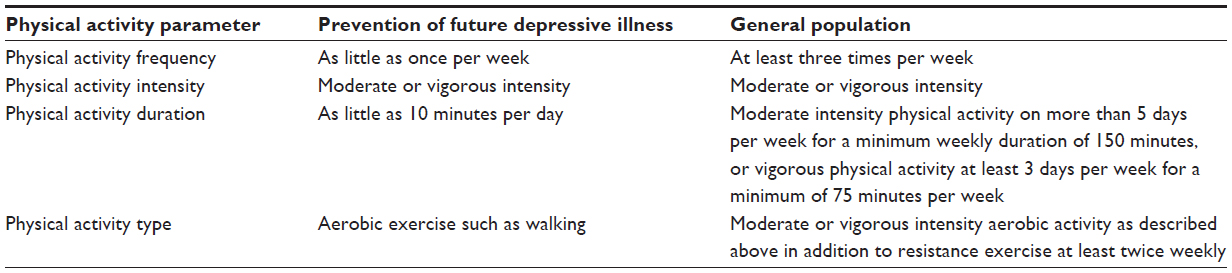 | Table 1 Summary of the physical activity parameters likely to contribute to the prevention of future depressive illness, compared to those recommended for cardiorespiratory and muscular fitness in the general population |
As with pharmaceutical interventions, physical activity is only effective if one engages in it. Therefore, even though position statements, clinical guidelines, and best practice models may indicate a unique physical activity prescription model, individual circumstances, activity preferences, level of enjoyment, prior injury, and physical health must be considered when promoting physical activity. Up skilling clinicians in the importance and effectiveness of physical activity for the prevention of future depressive illness, and maintaining a simple approach to physical activity promotion may contribute to the initial uptake and long term adherence to physical activity.
Implications for practice
Clinicians must be cognizant of the physical and mental health benefits of physical activity and its value in reducing the risk of future depressive episodes. Clinicians must also be mindful of the challenges of initiating and maintaining physical activity behavior and offer support systems to patients with depression and other mental illnesses. These may include referrals to exercise professionals, the use of print and electronic resources from representative and advocacy groups, and role modeling using their own physical activity behaviors. The parameters suggested in Table 1 for the prevention of future depressive illness may be useful when making initial recommendations to individuals regarding the commencement of a physical activity program.
Limitations associated with current studies and implications for future research
The current evidence for the mental health benefits of physical activity and the prevention of future depressive episodes is promising. However, the findings of studies investigating the association between physical activity participation and mental illness are subject to limitations. For example, determination of mental illness either via self-report or through the use of a multitude of diagnostic instruments, or differing diagnostic cut points in the same instrument, makes interpretation and comparison between studies difficult. A differentiation between clinical depression and other forms, and between clinically significant and statistically significant findings will also aid in the translation of research to practice.
Many studies rely on self-report instruments of physical activity participation, some of which may require further validation. Objective measurement such as accelerometry may represent best practice but their use may be limited by factors such as participant inconvenience and cost, particularly with large, multi-site studies. Analysis of accelerometer data can be time consuming and confounded by the use of varying data processing strategies, cut-points and algorithms. Accelerometers are not able to differentiate between various physical activity types such as walking or resistance training, and where these data need to be captured, self-report instruments may offer advantages. Emerging technologies such as wearable sensors may help overcome these limitations. Self-report instruments rarely capture data pertaining to differing modes of exercise such as the use of resistance training, relaxation exercise or stretching, and this may have implications regarding misclassification of physical activity bouts. Studies should carefully consider the type of data needed for analysis and select physical activity surveillance tools which are cost effective and offer participant convenience, while ensuring all data pertaining to the aims of the research are captured.
Given these limitations, future studies investigating the impact of physical activity participation should seek to quantify the core characteristics of reported physical activity including the frequency, intensity, time (duration), and type of physical activity. In order to investigate the characteristics of physical activity which may influence its relationship with the development of future depressive illness more thoroughly, the delivery (group or individual), level and type of supervision (by whom and how it is supervised), and differentiation between physical activity and exercise, should be examined. This is likely to require the development, validation and implementation of new instruments for self-reported activity behaviors.
Author contributions
RS was invited to prepare the manuscript and wrote the first draft of the manuscript. BH and PR provided content and editorial comments, and contributed to the preparation of the final manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors of this manuscript report no conflicts of interest in this work.
References
Coombes JS, Law J, Lancashire B, Fassett RG. “Exercise is medicine”: curbing the burden of chronic disease and physical inactivity. Asia Pac J Public Health. Epub April 9, 2013. | |
Garber CE, Blissmer B, Deschenes MR, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334–1359. | |
World Health Organisation. Global Recommendations on Physical Activity for Health. Geneva: World Health Organisation; 2010. | |
Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U; Lancet Physical Activity Series Working Group. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247–257. | |
World Health Organisation. The Global Burden of Disease: 2004 Update. Geneva, Switzerland: World Health Organisation; 2008. | |
Lim D, Sanderson K, Andrews G. Lost productivity among full-time workers with mental disorders. J Ment Health Policy Econ. 2000;3(3):139–146. | |
Galper DI, Trivedi MH, Barlow CE, Dunn AL, Kampert JB. Inverse association between physical inactivity and mental health in men and women. Med Sci Sports Exerc. 2006;38(1):173–178. | |
Harvey SB, Hotopf M, Overland S, Mykletun A. Physical activity and common mental disorders. Br J Psychiatry. 2010;197(5):357–364. | |
Smith PJ, Potter GG, McLaren MM, Blumenthal JA. Impact of aerobic exercise on neurobehavioral outcomes. Ment Health Phys Act. 2013:139–153. | |
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica. 1983;67(6)361–370. | |
Saxena S, Van Ommeren M, Tang K, Armstrong T. Mental health benefits of physical activity. J Ment Health. 2005;14(5):445–451. | |
Cooney GM, Dwan K, Greig CA, et al. Exercise for depression. Cochrane Database Syst Rev. 2013;9:CD004366. | |
Gorczynski P, Faulkner G. Exercise therapy for schizophrenia. Cochrane Database Syst Rev. 2010;5:CD004412. | |
Asmundson GJ, Fetzner MG, Deboer LB, Powers MB, Otto MW, Smits JA. Let’s get physical: a contemporary review of the anxiolytic effects of exercise for anxiety and its disorders. Depress Anxiety. 2013;30(4):362–373. | |
Lawlor DA, Hopker SW. The effectiveness of exercise as an intervention in the management of depression: systematic review and meta-regression analysis of randomised controlled trials. BMJ. 2001;322(7289):763–770. | |
Daley A. Exercise and depression: a review of reviews. J Clin Psychol Med Settings. 2008;15(2):140–147. | |
NICE. Depression: The Treatment and Management of Depression In Adults (Update). NICE clinical guideline 90; 2009. Available from: http://www.nice.org.uk/CG90. Accessed November 2, 2012. | |
Ravindran AV, Lam RW, Filteau MJ, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) Clinical guidelines for the management of major depressive disorder in adults. V. Complementary and alternative medicine treatments. J Affect Disord. 2009;117(Suppl 1):S54–S64. | |
Scottish Intercollegiate Guidelines Network. Non-Pharmaceutical Management of Depression in Adults. Edinborough: Scottish Intercollegiate Guidelines Network; 2010. | |
NICE. Psychosis and Schizophrenia in Adults: Treatment and Management. London, UK. National Institute for Health and Care Excellence; 2014. | |
Ferrari AJ, Somerville AJ, Baxter AJ, et al. Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychol Med. 2013;43(3):471–481. | |
Rimer J, Dwan K, Lawlor DA, et al. Exercise for depression. Cochrane Database Syst Rev. 2012;7:CD004366. | |
Mead GE, Morley W, Campbell P, Greig CA, McMurdo M, Lawlor DA. Exercise for depression. Cochrane Database Syst Rev. 2009;3:CD004366. | |
Stanton R, Reaburn P. Exercise and the treatment of depression: a review of the exercise program variables. J Sci Med Sport. 2013;17(2):177–182. | |
Perraton LG, Kumar S, Machotka Z. Exercise parameters in the treatment of clinical depression: a systematic review of randomized controlled trials. J Eval Clin Pract. 2010;16(3):597–604. | |
Cramer H, Lauche R, Langhorst J, Dobos G. Yoga for depression: a systematic review and meta-analysis. Depress Anxiety. 2013;30(11):1068–1083. | |
Wang F, Lee EK, Wu T, et al. The effects of Tai Chi on depression, anxiety, and psychological well-being: a systematic review and meta-analysis. Int J Behav Med. Epub September 28, 2013. | |
Jacka FN, Pasco JA, Williams LJ, et al. Lower levels of physical activity in childhood associated with adult depression. J Sci Med Sport. 2011;14(3):222–226. | |
Pasco JA, Williams LJ, Jacka FN, et al. Habitual physical activity and the risk for depressive and anxiety disorders among older men and women. Int Psychogeriatr. 2011;23(2):292–298. | |
Lucas M, Mekary R, Pan A, et al. Relation between clinical depression risk and physical activity and time spent watching television in older women: a 10-year prospective follow-up study. Am J Epidemiol. 2011;174(9):1017–1027. | |
Brown WJ, Ford JH, Burton NW, Marshall AL, Dobson AJ. Prospective study of physical activity and depressive symptoms in middle-aged women. Am J Prev Med. 2005;29(4):265–272. | |
Mammen G, Faulkner G. Physical activity and the prevention of depression: a systematic review of prospective studies. Am J Prev Med. 2013;45(5):649–657. | |
Bernaards CM, Jans MP, van den Heuvel SG, Hendriksen IJ, Houtman IL, Bongers PM. Can strenuous leisure time physical activity prevent psychological complaints in a working population? Occup Environ Med. 2006;63(1):10–16. | |
Hamer M, Molloy GJ, de Oliveira C, Demakakos P. Leisure time physical activity, risk of depressive symptoms, and inflammatory mediators: The English Longitudinal Study of Ageing. Psychoneuroendocrinology. 2009;34(7):1050–1055. | |
Ku PW, Fox KR, Chen LJ. Physical activity and depressive symptoms in Taiwanese older adults: A seven-year follow-up study. Prev Med. 2009;48(3):250–255. | |
Wise L, Adams-Campbell L, Palmer J, Rosenberg L. Leisure time physical activity in relation to depressive symptoms in the black women’s health study. Ann Behav Med. 2006;32(1):68–76. | |
Carpiniello B, Primavera D, Pilu A, Vaccargiu N, Pinna F. Physical activity and mental disorders: A case-control study on attitudes, preferences and perceived barriers in Italy. J Ment Health. 2013;22(6):492–500. | |
Jonsdottir IH, Rödjer L, Hadzibajramovic E, Börjesson M, Ahlborg G Jr. A prospective study of leisure-time physical activity and mental health in Swedish health care workers and social insurance officers. Prev Med. 2010;51(5):373–377. | |
Smith TL, Masaki KH, Fong K, et al. Effect of walking distance on 8-year incident depressive symptoms in elderly men with and without chronic disease: the Honolulu-Asia Aging Study. J Am Geriatr Soc. 2010;58(8):1447–1452. | |
Thompson PD, Franklin BA, Balady GJ, et al. Exercise and acute cardiovascular events: placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation. 2007;115(17):2358–2368. | |
Franklin BA, Billecke S. Putting the benefits and risks of aerobic exercise in perspective. Curr Sports Med Rep. 2012;11(4):201–208. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.