")
Back to Journals » Veterinary Medicine: Research and Reports » Volume 6
The management of equine acute laminitis
Authors Mitchell C, Fugler LA, Eades S
Received 1 September 2014
Accepted for publication 24 October 2014
Published 22 December 2014 Volume 2015:6 Pages 39—47
DOI https://doi.org/10.2147/VMRR.S39967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Takashi Agui
Colin F Mitchell, Lee Ann Fugler, Susan C Eades
Veterinary Clinical Sciences, School of Veterinary Medicine, Louisiana State University, Baton Rouge, LA, USA
Abstract: Laminitis is an extremely painful condition resulting in damage to the soft tissues anchoring the third phalanx to the hoof, which can result in life-threatening debilitation. Specific therapy is not available. The most important principles of therapy include aggressive nutritional and medical management of primary disease processes, cryotherapy, anti-inflammatory therapy, pain management, and biomechanical support. This review focuses on the principles of evidenced-based therapies.
Keywords: laminitis treatment, laminitis biomechanics, laminitis pain
Introduction
Acute laminitis is a severely debilitating, excruciatingly painful, and potentially career-ending and life-threatening disease of the epidermal (insensitive) and dermal (sensitive) laminae of the equine digit affecting adult horses and ponies of any breed or use. The acute phase is identified as the onset of clinical signs of pain, heat, and increased digital pulses. The acute phase continues until the distal phalanx displaces, marking the beginning of the chronic phase of the disease.1 There is a consensus among veterinarians that laminitis is most commonly associated with ingestion of nonstructural carbohydrates (NSCs) in pasture.2 Laminitis also commonly occurs in a wide range of diseases associated with sepsis and/or endoxemia (metritis, anterior uveitis, bronchopneumonia, pleuropneumonia, and numerous causes of gastrointestinal compromise including duodenitis/proximal jejunitis, enterocolitis, surgically managed colic, and grain overload), pituitary pars intermedia dysfunction, equine metabolic syndrome, and support limb overload in horses that have severe non-weight-bearing lameness.3 Studies of the various etiologies of laminitis often group the predispositions listed here into three categories: inflammatory-inducing diseases associated with a systemic inflammatory response (sepsis, endotoxemia, and nonseptic conditions) and ingestion of rapidly hydrolyzable carbohydrates, endocrinopathies (pituitary pars intermedia dysfunction and equine metabolic syndrome), and excess weight bearing.2–4
Laminitis is frustrating for veterinarians because current knowledge and understanding of the pathophysiology of the disease is incomplete, limiting efforts at prevention and treatment. It also causes profound emotional stress and economic loss to horse owners and trainers because of the agonizing pain experienced by affected horses. Therefore, a timely diagnosis, medical management, and biomechanical support of affected feet are of utmost importance in helping to minimize the effects of this devastating disease. Because specific therapies are not available to prevent or repair laminar damage, the objective of this article is to review the principles of therapy and to discuss some of the more commonly employed treatments.
Clinical signs
Laminitis can affect a single foot, all four feet, the forefeet alone, or less commonly, the hind feet alone. The Obel laminitis grading system is useful to describe the severity of lameness.5 In Obel Grade 1 laminitis, horses alternately and incessantly lift their feet. Lameness is not evident at a walk but is evident at a trot as a short, stilted gait. Horses with Obel Grade 1 laminitis may exhibit transient periods of weight shifting, have slight increases in temperature at the coronary band, and have slight increases in digital pulse pressures. Horses that walk with a stilted gait but still allow a foot to be lifted are classified as Obel Grade 2. These horses will often have a head-bobbing lameness when walked in a tight circle in either direction. Horses with Obel Grade 3 laminitis move reluctantly and vigorously resist lifting of their feet. The most severe classification is Obel Grade 4, in which horses refuse to move unless forced.
Many severely affected horses only rise for short periods of time and demonstrate a characteristic “saw horse” stance of rocking or shifting their weight onto their hind feet. This stance is commonly seen in horses with more severe pain in the forefeet than in the hind feet and is often accompanied by anxiety, muscle fasciculations, and reluctance to move. Horses with pain equally severe in all four feet may have a normal stance. Horses with the most severe cases of laminitis often develop poor body condition and pressure sores resulting from prolonged periods of recumbency.
Laminitis can often result in rotational or distal displacement (sinking) of the third phalanx within the hoof capsule.6 Mild cases may resolve without displacement; however, once displacement occurs, significant lameness often persists. This can occur at any time after the onset of lameness, ranging from hours to weeks. In most cases, several days are required for third phalanx displacement to occur. In peracute cases of laminitis, serum leakage and/or bleeding from the coronary band develop within hours to a few days after the onset of lameness, signaling widespread laminar separation. A dropped sole or palpation of a depression located at the level of the coronary band are clinical signs that indicate displacement of the third phalanx may be occurring. Lateromedial radiographs of the digit are used to determine whether rotational or distal displacement has occurred. Once displacement of the third phalanx has occurred, the horse is considered to be in the chronic stage of the disease.
Pathogenesis
The mechanisms involved in the pathogenesis of laminitis have not been completely elucidated and are most likely numerous and interrelated. Epithelial detachment resulting from inflammation and enzyme activation associated with sepsis and other disease processes, insulin resistance, vascular endothelial dysfunction, and excessive weight bearing are factors at the forefront of current investigations.
Pasture-associated laminitis clearly has a nutritional basis, but the exact mechanism or mechanisms that link the consumption of pasture forage to the development of laminar failure is not known. The ingestion of pasture forage may trigger laminitis by means of induction of digestive or metabolic disturbances. At certain times of the year, pasture forage is rich in NSCs.2 Colonic fermentation of plant NSCs may cause gastrointestinal disturbances that can lead to laminitis.2 In addition, intake of feeds rich in NSCs may lead to hyperinsulinemia and insulin resistance in animals with metabolic syndrome. Experimental models leading to hindgut fermentation of carbohydrates and hyperinsulinemia both reliably induce laminitis.7,8
Laminitis associated with sepsis has been studied using two carbohydrate overload models involving administration of either cornstarch/wood flour or oligofructose.3 Leukocyte infiltration, endothelial activation, and increased messenger RNA concentration of pro-inflammatory cytokines and cyclooxygenase (COX)-2 expression have been documented in experimental models of equine sepsis and gastrointestinal disease.3 Although the exact trigger mechanisms leading to laminitis in these events are unknown, extracellular matrix injury resulting from proteases and dysregulation of epithelial adhesion molecules culminate in laminar failure.3 Alterations in laminar hemodynamics, including alterations in blood flow and increased venous resistance favoring edema formation, have been documented but may not be the primary events leading to laminar failure.9
Medical therapy in acute laminitis
Treatment of acute laminitis remains empiric and is often based on the experience and preference of the clinician. One should always consider acute laminitis a medical emergency and should institute treatment immediately after clinical signs develop or, preferably, before the onset of clinical signs. The goals of treatment are to eliminate or minimize any predisposing factors, reduce pain, reduce or prevent the magnitude of permanent laminar damage, and prevent displacement of the third phalanx within the hoof capsule (Table 1). Although considerable controversy exists regarding the treatment of laminitis resulting from the lack of complete understanding of its pathophysiology, the cornerstones of treatment are still directed at different components of the known pathophysiologic processes.
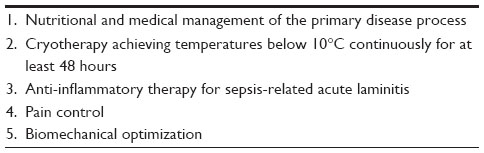 | Table 1 Principles of acute laminitis therapy |
Effective treatment/prevention requires aggressive and appropriate therapeutic measures aimed at resolution of the primary disease process when possible. To institute preventive treatment for laminitis, one must first identify those horses at risk. Many of the primary diseases thought to predispose horses to the development of laminitis are associated with circulating endotoxin. Therefore, a common preventive measure is combating the effects of endotoxemia and sepsis effectively by decreasing the severity of the primary illness.10 Recommended treatments include, but are not limited to, administration of mineral oil (if the horse engorged on grain), intravenous fluids, parenteral antibiotics when bacterial infection is documented, nonsteroidal anti-inflammatory drugs (NSAIDs), polymyxin-B, and hyperimmune serum or plasma. Similarly, effective preventive management of horses with laminitis-associated pituitary pars intermedia dysfunction involves restoration of pars intermedia function with pergolide. Management of laminitis associated with equine metabolic syndrome and pasture-associated laminitis involves weight control by restriction of carbohydrate intake. Variable efficacy has been seen in horses with the use of medications that improve insulin sensitivity in people.
Continuous application of cryotherapy (maintaining hoof wall surface temperature at 5°C–7°C) to the distal aspect of limbs for 48 hours prevents lameness, improves epidermal laminar histologic scores, reduces expression of messenger RNA for matrix metalloproteinase 2 (MMP-2), and reduces lamellar inflammatory signaling in horses with carbohydrate overload-induced laminitis.11–17 In the only clinical study of cryotherapy for laminitis prophylaxis, Kullman et al found that horses with colitis were ten times less likely to develop laminitis when the limbs were cooled continuously for 48 hours or more.18 This treatment is generally well tolerated by horses; however, it requires intensive management, replacing ice every 1–2 hours to have a constant ice slurry capable of keeping the hoof wall surface temperature below 10°C, as recommended.17 Methods that incorporate the hoof, pastern, fetlock, and a portion of the cannon bone while still allowing some freedom of movement are needed for optimal hoof cooling. The most effective cooling methods are either 63 cm tall vinyl boots containing ice and water or a circulating refrigerated bath.12,14 Both of these systems restrict movement and necessitate constant monitoring of horses. As a result, these methods are not usually practical for the treatment of laminitis in clinical practice. Five liter intravenous fluid bags are durable and of sufficient size to hold enough ice slurry to incorporate the hoof and pastern and keep hoof wall surface temperatures near 7°C–10°C.19 Gelpack cooling products do not adequately cool the hoof.19 Even with improved techniques, cryotherapy is a labor-intensive treatment most suited to a hospital setting.
Investigations have documented a marked inflammatory mediator response during the early stages of acute laminitis that may be at least partially responsible for injury to the laminar basilar epithelial cells. Inflammatory mediator-induced injury leads to detachment of these cells from the underlying basement membrane and causes failure of the laminar attachments, resulting in displacement of the third phalanx.10 Therefore, anti-inflammatory medications are recommended to decrease inflammation and reduce laminar damage.3,10 Phenylbutazone appears to have the best anti-inflammatory and analgesic effects of any of the NSAIDs commonly used in horses. One can administer a dose of 2.2–4.4 mg/kg of phenylbutazone intravenously or by mouth every 12 hours. Alternatively, flunixin meglumine can be administered at 0.5–1.1 mg/kg intravenously or by mouth every 12 hours (Table 2). A dose of 0.25 mg/kg flunixin meglumine administered intravenously every 8 hours interrupts eicosanoid production associated with endotoxemia and minimizes adverse effects. However, this low dosage does not provide analgesia. Firocoxib is available for use in horses but often does not provide sufficient analgesia for laminitis cases. Furthermore, COX-1 inhibition may provide greater efficacy than COX-2 inhibition by reducing platelet-activated release of inflammatory and vasoactive products.10 Dimethyl sulfoxide (DMSO) is an anti-inflammatory drug and weak scavenger of hydroxyl radicals. Because minimal oxygen free radical generation has been documented in either insulin resistance or sepsis, DMSO has a minimal effect on the clinical outcomes of laminitis in these cases. DMSO is sometimes administered for other anti-inflammatory effects at 0.1–1.0 g/kg intravenously, diluted in a polyionic fluid to a concentration of 10% every 8–24 hours (Table 2). Some clinicians prefer to place DMSO topically on the coronary bands.
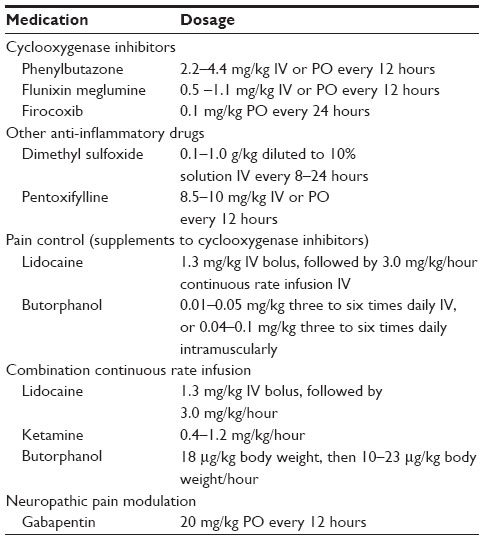 | Table 2 Medications often used in equine acute laminitis |
Phosphodiesterase inhibitors regulate MMP expression by increasing intracellular adenosine 3′,5′-cyclic monophosphate concentrations that disrupt phosphorylation pathways and prevent gene transcription.20 Pentoxifylline is a methylxanthine phosphodiesterase inhibitor with anti-inflammatory effects and immune regulatory properties.21 Pentoxifylline also improves blood flow in people through actions on the red blood cell membrane22 and improves red blood cell deformability in horses, with variable effects on blood flow.23–25 Numerous in vivo and in vitro studies performed in horses document the drug’s anti-inflammatory activities.26,27 As a phosphodiesterase inhibitor, pentoxifylline can affect the systemic inflammatory response through multiple pathways20 and was recently shown to be an effective MMP inhibitor in horses.28 Pentoxifylline (8.5 mg/kg intravenously every 12 hours) had the most potent inhibitory effects on pro-MMP-9 and modest inhibitory effects on pro-MMP-2 production when compared with oxytetracycline, flunixin meglumine, and doxycycline in horses with experimentally induced endotoxemia.28 Pentoxifylline (8.5 mg/kg intravenously every 12 hours) also reduced the severity of lameness in horses with laminitis induced by cornstarch overload.29 However, the mechanism by which pentoxifylline improved lameness in this model is uncertain, as MMPs may not play an active role in developmental laminitis.30 There is also substantial evidence suggesting that pentoxifylline reduces blood glucose concentrations after diabetes induction in rats by improving insulin receptor sensitivity,31 thus making it a potential therapeutic agent for laminitis associated with metabolic disease.
Doxycycline has been approved for use as an MMP inhibitor in human patients. Extrapolation from this has led to the use of doxycycline in the treatment of equine laminitis to inhibit MMP-mediated destruction of laminar connections. In contrast, results of a recent study of horses with experimental endotoxemia revealed that although doxycycline is a potent inhibitor of constitutive MMP-2, it is a weak inhibitor of inflammation-associated MMP-9 in horses.28 As a result of alterations of microbial flora after oral administration, doxycycline may be contraindicated in some cases of alimentary-associated laminitis.
Horses with acute laminitis are predisposed to developing significant laminar edema, which can further compromise endothelial attachments and lead to laminar damage.32 This is a result of both the normal anatomy of the lamina and hoof and the microvascular alterations that develop with the onset of laminitis. Support of plasma oncotic pressure by supplementation with plasma or another colloidal solution, such as hydroxyethyl starch, can improve transcapillary pressures. In addition, one should take care when administering intravenous fluid therapy to horses with acute laminitis or those predisposed to its development, as excessive intravascular volume caused by overzealous fluid administration could perpetuate development of laminar edema in horses with abnormal digital hemodynamics. Limb edema can be treated with hydrotherapy and support wraps. Medications used to improve digital blood flow (acepromazine, glyceryl trinitrate, and isoxsuprine hydrochloride) do not appear to improve the clinical outcomes of horses with laminitis.
Stem cell therapy is being used by some practitioners for the treatment of laminitis.33 It is important to clarify that there have been no studies performed to evaluate the safety or efficacy of stem cells for the treatment of laminitis. Although stem cell administration may decrease the inflammatory response, the potential exists for the opposite effect to occur without tested therapeutic regimes. Despite the lack of published guidelines for its use in clinical cases, an empiric regime currently in use involves regional limb perfusion of stem cells via the lateral digital vein at the level of the sesamoid bones. Stem cells are administered once, early in the acute episode, and again 14 days later. As there are currently no published data to evaluate the effectiveness of stem cells for laminitis, proper administration techniques, cell types, and cell numbers have not yet been evaluated. Another drawback with this treatment is the delay between harvesting the bone marrow or fat and culturing sufficient numbers of stem cells for injection.
Pain control in laminitis
As previously stated, NSAIDs are the most commonly used analgesics in horses with laminitis. Phenylbutazone is the most efficacious drug for controlling orthopedic pain in horses and the most common analgesic therapy for laminitis. Flunixin meglumine is often used in horses with concurrent gastrointestinal disease, septic metritis, and so on, as it is a more potent visceral analgesic and is slightly less toxic than phenylbutazone. Concurrent administration of flunixin meglumine with phenylbutazone may increase the likelihood of toxicity and often does not provide superior analgesia to that of phenylbutazone alone.34 Similarly, increasing dosages do not provide superior analgesia. More selective COX-2 inhibitors, firocoxib and meloxicam, provide good analgesia in lameness models but appear to be less effective in pain control for horses with laminitis. These analgesics may also be less effective in reducing mediator release from activated platelets.10
Additional medications have been sought when the pain management provided by NSAIDs alone is inadequate. An intravenous continuous rate infusion of lidocaine (1.3 mg/kg bolus followed by 3.0 mg/kg/hour) has been used extensively in hospitalized horses undergoing exploratory celiotomy to control pain and ileus in the postoperative period.35,36 Lidocaine has been used less extensively to supplement analgesia provided by NSAIDs in cases of laminitis; therefore, the efficacy is unknown. Butorphanol can also be administered intravenously (0.01–0.05 mg/kg three to six times daily) or intramuscularly (0.04–0.1 mg/kg three to six times daily) to supplement analgesia provided by NSAIDs and/or lidocaine.
Horses in severe pain can exhibit distress that may be perceived as anxiety and hypersensitization. Multimodal analgesic therapy has been advocated in these situations, requiring hospitalization for intravenous continuous rate infusion of analgesics.34 Combination continuous rate infusion of lidocaine (1.3 mg/kg bolus followed by 3.0 mg/kg/hour), ketamine (0.4–1.2 mg/kg/hour), and butorphanol (18 μg/kg body weight, then 10–23 μg/kg body weight/hour) are commonly used in this situation. Ketamine is used in this application in subanesthetic doses to reduce central sensitization in severe states. Morphine can be used in place of butorphanol in the most severe situations but is more commonly associated with excitement, which can be managed with concurrent administration of sedatives. Transdermal fentanyl patches (one or two patches per horse) have been used in a few cases, with variable results and excitation in some cases necessitating further study.37
Gabapentin has been used extensively in human medicine to treat neuropathic pain, which has been suspected in cases of chronic laminitis. Pharmacokinetic properties have been evaluated in horses at 20 mg/kg by mouth and intravenously, demonstrating that the medication is safe, causes mild sedation, and has poor oral bioavailability. It has been difficult to evaluate whether gabapentin provides benefit to patients with laminitis, suggesting the need for further evaluation.38
Biomechanical considerations in acute laminitis
Before investigating treatments aimed at providing mechanical support to the distal phalanx within the hoof capsule, a review of the biomechanical forces to which this region is exposed is important.
The horse’s weight is distributed unevenly between the front and hind limbs, with the front limbs carrying approximately 60% of the body weight. This most likely explains why the majority of cases of clinical laminitis affect the forelimbs primarily. It is commonly assumed that the forelimb load is equally shared between the front limbs, although any cause of lameness may alter this balance and expose the overloaded limb to excessive stress.
The third phalanx is supported or slung inside the hoof capsule by interlocking dermal and epidermal lamellae (within the stratum internum). In an adult horse, there are between 550 and 600 primary dermal and epidermal lamellae,39 each with between 100 and 200 secondary lamellae.40 These lamellae form a tight connection between the internal portion of the hoof wall and the third phalanx. This connection is capable of withstanding loads considerably greater than those imposed during weight bearing or normal locomotion, yet still remains flexible enough to allow hoof expansion. The deep digital flexor tendon inserts on the palmar aspect of the third phalanx and exerts tension on the bone caudally. When the hoof is loaded, the lamellae are exposed to either compression or tension, depending on their location. As the dorsal hoof wall compresses during weight bearing, the third phalanx moves caudally and distally, and the heels move abaxially.41 Because of the differences in loading, the lamellae in the toe, quarters, and heel region all develop different architecture to allow them to resist this stress appropriately.40,41
In a horse suffering a laminitic episode, the clinically relevant injury appears to occur within the laminar region. Injury to this region can compromise the ability of the lamellae to maintain the tight connection between the third phalanx and the hoof capsule. It is unclear whether the stress from weight bearing, the tension on the deep digital flexor tendon, or a combination of these forces leads to failure of the lamellar attachments in horses that subsequently develop displacement of the third phalanx. The injury to the lamina is usually more severe in the toe region; therefore, this regional focus of breakdown is thought to explain the higher frequency of horses with rotational displacement of the third phalanx, as opposed to distal displacement.
The goal of initial therapy when treating the biomechanical effects of acute laminitis is to minimize the laminar injury and prevent any displacement of the third phalanx. When signs of third phalanx displacement occur (either clinically or radiographically), the horse is considered to have entered the chronic phase of this process. Medical therapy has been discussed previously and needs to be initiated rapidly after the onset of clinical signs. In horses considered to be at risk for developing laminitis (endotoxemic, pleuropneumonia, enterocolitis patients, etc), preventative therapy is preferably started before the onset of clinical signs, whenever possible, until the primary systemic disturbance has been resolved, because of the unpredictability of the onset of laminitis in these horses.
Mechanical support to the hoof should always be attempted with two goals in mind: limiting displacement of the third phalanx and increasing patient comfort. This can be provided in many different ways, with the caveat that one therapy will not increase comfort for all horses, or may even make some horses less comfortable. Each case should be evaluated carefully, with the foot examined either digitally or using hoof testers to identify areas of pain or sensitivity on the sole or hoof capsule. Observation of the horse in motion may also illustrate painful areas of the hoof that the horse is attempting to keep unloaded; however, these horses should never be forced to move.
The weight of the horse applies the most stress to the lamina and hoof. Providing axial support to unload damaged lamina can help increase the horse’s comfort level. Although the horse can reduce the amount of weight carried on an individual limb, some loading and unloading of the hoof is unavoidable. The easiest way to minimize additional stress is to immediately confine the horse or limit its ability to move. Confining the horse to a well-bedded stall will help reduce the stress on the laminae created by locomotion. Some horses will lie down, helping to further alleviate laminar stress. Sedation with anxiolytic drugs, such as acepromazine, can facilitate this, but the effects of this drug are variable between horses. Despite multiple doses of sedatives or marked pain, some horses are unwilling to lie down in a stall. The bedding type may be a factor. Sand is often recommended as bedding material because it will conform to the solar surface of the hoof and distribute the weight over the solar surface, frog, and hoof wall; however, some horses will not lie down in sand. Providing a top layer of straw or deep shavings may help increase time spent in recumbency. As long as the horse is able to roll over to switch dependent sides and is continuing to defecate and urinate, being recumbent is the simplest way to limit any further damage to the inflamed laminae. There is no ideal bedding material, as hygiene, comfort, and abrasiveness are all variables that have to be taken into consideration from a case management aspect.
Supporting the horse’s weight by intermittent slinging has also been suggested as a supportive treatment. This can be effective but has numerous drawbacks. It is expensive and labor-intensive because of the specific equipment, facilities, and continuous supervision needed. Many horses will not tolerate this type of support, and there is a risk for potential injury to both the horse and personnel. However, if tolerated, horses can be supported by slings to facilitate trimming or shoeing, or simply to help protect their laminae and prevent prolonged periods of lateral recumbency.
Applying support directly to the frog and heel region of the hoof is always appropriate. When standing on a firm surface, the sole is not usually involved in weight bearing; however, on softer surfaces, this region becomes loaded. It is necessary to carefully examine the sole before applying materials to the ground surface of the hoof, as excessive pressure or loading of painful areas (usually the sole directly under the apex of the third phalanx and the dorsal hoof wall at the toe) will increase discomfort. This form of support can be used to either decrease the lever arm effect of the toe on the damaged lamina and/or to reduce the discomfort associated with tension on the insertion of the deep digital flexor tendon. If the horse is currently shod, it must be decided whether to leave the shoes on and incorporate them into the new form of support or to remove them. If the decision is made to remove them, this must be performed as atraumatically as possible, preferably by rasping off the clinches and pulling out the nails individually. Traction on the shoe and/or hammering to cut the clinches will not be well tolerated. Rasping of the dorsal hoof wall at the toe is often performed in these cases to try and prevent the dorsal laminae in this region from being stressed by contact with the ground.
In its simplest form, increasing the contact or weight-bearing surface of unaffected parts of the foot can help redistribute the load incurred during weight bearing. A bandage frog support can be provided using simple items such as a rolled up piece of brown gauze, placed slightly behind the apex of the frog and running caudally. This should be thick enough to provide firm contact between the ground and the frog when compressed. Excessive pressure in this region is often uncomfortable, but it is relatively easy to adjust. The gauze can be secured in place with adhesive tape to the foot. This will need to be reset if the gauze moves off of the frog or if it becomes too compressed and no longer provides appropriate contact between the frog and ground. Lily pads are a commercially available, urethane frog support that can be trimmed and applied to the sole of the foot. However, they are rigid and may not easily fit to all sizes and shapes of feet.
Foam pads of crushable material, such as polystyrene insulation foam, can be applied to the sole of the hoof for support. These are fixed in place using duct tape. On weight bearing, these pads readily deform and spread the load over the entire solar surface of the hoof. If areas of sole sensitivity are present, these supports may need to be trimmed to leave sections of the sole unloaded before additional pads are placed. Foam pads are rapidly compressed and may need to be changed frequently to provide prolonged relief. The foam must be trimmed to fit the hoof and monitored for compression or slippage. If the horse is maintained in deep bedding, these pads do not conform as well to the sole, are harder to maintain in place, and are more likely to place pressure on sensitive sole areas. The main advantages of foam pads are that they are cheap and easy to use, and the material is widely available.
The authors prefer to use impression material for frog support. Multiple brands with varying levels of firmness are available. Impression material usually comes as two different-colored putties that become soft and pliable when mixed together in similar volumes. Once pliable, the putty is applied to the frog and taped into place until the material cures and becomes firm (Figure 1). Excessive material may migrate over the sole or cranial portion of the frog but can be easily trimmed. Impression material can be expensive, but it forms perfectly to the frog/heel, even after trimming of excessive material (Figure 2). Enough material can be applied to elevate the heels slightly or to fit between the web of a shoe. This material is adaptable, easy to keep in place because of its conforming ability, and easy to adjust or trim once it has cured.
 | Figure 1 Material on the hoof. |
 | Figure 2 Material on ground. |
Shoes that can be adhered or held to the foot by adhesive tape can also be used and have several benefits. They can be applied painlessly, some of them can be adjusted without the aid of a farrier, and they can be applied by owners before a veterinary examination. Modified Ultimate Cuffs (Nanric, Lexington, KY, USA) are a commercially available shoe with a 20° built-in wedge. The shoe is designed to elevate the heel, to unload the deep digital flexor tendon, and to improve blood flow to the dorsal laminae. The shoe contacts the foot around the periphery of the hoof wall, allowing impression material to be used in combination with this shoe and include the frog in the weight-bearing surface. Other boots, such as Easy Boots, can be quickly applied. Their solid base will prevent excessive sole pressure, but they may not unload the dorsal laminae effectively.
Placement of a hoof cast, using either plaster or fiberglass material, has also been described. The application is similar for both materials. The first roll of cast material is placed over the frog and heels to provide elevation and increase the weight-bearing surface. Additional rolls are then used to secure the cast support to the hoof. Care should be taken to prevent the material from contacting the skin above the coronary band, as skin sores can develop if there is excessive motion in these regions.
Changes to the horse’s diet (feed a diet low in NSCs, such as grass or alfalfa hay; avoid pellet/concentrates unless they are specifically low-carbohydrate rations; and prevent access to pasture), activity level, and mechanical support should be instituted in all cases of acute laminitis, along with medical therapy. Horses should be frequently monitored after application of any of the aforementioned forms of mechanical support, as most horses will display almost immediate improvements (often subtle) in comfort after redistribution of their weight-bearing surface. Decreases in weight shifting, respiratory rate, heart rate, or changes in the horse’s demeanor may be the only observed improvements. Therefore, even small changes should not be overlooked. Evaluation may be difficult if the horse is being maintained in a deeply bedded stall, but these horses should not be forced to move, especially not in tight circles. If no improvement is seen, the support can be adjusted on the basis of the findings of the initial hoof examination, or if necessary, a different technique can be used. Effective management is vital to minimizing the chances of the horse entering the chronic phase of laminitis, which requires more extensive veterinary and farrier care.
Conclusion
The goal of medical and biomechanical therapies in acute laminitis is to minimize damage to the laminar attachments. Therapeutic measures aimed at resolution of the primary disease process should be instituted immediately. Cryotherapy, if clinically practical, should be applied to the hoof wall and pastern and maintained in a manner that keeps the hoof wall surface temperature at 7°C–10°C for 48 hours. Anti-inflammatory drug therapy is indicated to reduce inflammation associated with acute septic diseases. Analgesic therapy is most often achieved by use of NSAIDs; however, alternative analgesic therapies may be needed when NSAID therapy is not sufficient or not tolerated. Mechanical support should be instituted to limit displacement of the third phalanx and increase patient comfort. There are multiple ways to provide mechanical support, with no single therapy being appropriate for all horses. It is necessary to examine the response of each horse individually and alter the therapy, based on pain. Applying support directly to the frog and heel region of the hoof and increasing the contact or weight-bearing surface of unaffected parts of the foot are among the most effective methods of biomechanical support during the acute stage of laminitis. Horses should be monitored frequently, and the response to all aspects of the treatment regime should be assessed and adjustments made on the basis of this response.
Disclosure
Dr Eades and Fugler report receiving grants from the Grayson Jockey Club Research Foundation. The authors report no other conflicts of interest in this work.
References
Reilly PT, Dean EK, Orsini JA. First aid for the laminitic foot: therapeutic and mechanical support. Vet Clin North Am Equine Pract. 2010;26(2):451–458. | |
Geor RJ. Pasture-associated laminitis. Vet Clin North Am Equine Pract. 2009;25(1):39–50, v–vi. | |
Belknap JK, Black SJ. Sepsis-related laminitis. Equine Vet J. 2012;44(6):738–740. | |
Virgin JE, Goodrich LR, Baxter GM, Rao S. Incidence of support limb laminitis in horses treated with half limb, full limb or transfixation pin casts: a retrospective study of 113 horses (2000–2009). Equine Vet J Suppl. 2011;40(40):7–11. | |
Obel N. Studies on the Histopathology of Acute Laminitis. Uppsala, Sweden: Almquisst and Wiksells Boktryckeri; 1948. | |
Baxter GM. Equine laminitis caused by distal displacement of the distal phalanx: 12 cases (1976–1985). J Am Vet Med Assoc. 1986;189(3):326–329. | |
de Laat MA, McGowan CM, Sillence MN, Pollitt CC. Equine laminitis: induced by 48 h hyperinsulinaemia in Standardbred horses. Equine Vet J. 2010;42(2):129–135. | |
Pollitt CC, Visser MB, Visser MB. Carbohydrate alimentary overload laminitis. Vet Clin North Am Equine Pract. 2010;26(1):65–78. | |
Robertson TP, Bailey SR, Peroni JF. Equine laminitis: a journey to the dark side of venous. Vet Immunol Immunopathol. 2009;129(3–4):164–166. | |
Belknap JK. The pharmacologic basis for the treatment of developmental and acute laminitis. Vet Clin North Am Equine Pract. 2010;26(1):115–124. | |
Pollitt CC, van Eps AW. Prolonged, continuous distal limb cryotherapy in the horse. Equine Vet J. 2004;36(3):216–220. | |
van Eps AW, Pollitt CC. Equine laminitis: cryotherapy reduces the severity of the acute lesion. Equine Vet J. 2004;36(3):255–260. | |
Van Eps AW, Pollitt CC. Equine laminitis model: cryotherapy reduces the severity of lesions evaluated seven days after induction with oligofructose. Equine Vet J. 2009;41(8):741–746. | |
van Eps AW, Leise BS, Watts M, Pollitt CC, Belknap JK. Digital hypothermia inhibits early lamellar inflammatory signalling in the oligofructose laminitis model. Equine Vet J. 2012;44(2):230–237. | |
van Eps AW, Pollitt CC, Underwood C, Medina-Torres CE, Goodwin WA, Belknap JK. Continuous digital hypothermia initiated after the onset of lameness prevents lamellar failure in the oligofructose laminitis model. Equine Vet J. 2014;46(5):625–630. | |
van Eps AW. Therapeutic hypothermia (cryotherapy) to prevent and treat acute laminitis. Vet Clin North Am Equine Pract. 2010;26(1):125–133. | |
van Eps AW, Walter LJ, Baldwin GI, et al. Distal limb cryotherapy for the prevention of acute laminitis. Clin Tech Equine Pract. 2004;3(1):64–70. | |
Kullmann A, Holcombe SJ, Hurcombe SD, et al. Prophylactic digital cryotherapy is associated with decreased incidence of laminitis in horses diagnosed with colitis. Equine Vet J. 2014;46(5):554–559. | |
Reesink HL, Divers TJ, Bookbinder LC, et al. Measurement of digital laminar and venous temperatures as a means of comparing three methods of topically applied cold treatment for digits of horses. Am J Vet Res. 2012;73(6):860–866. | |
Coimbra R, Melbostad H, Loomis W, et al. LPS-induced acute lung injury is attenuated by phosphodiesterase inhibition: effects on proinflammatory mediators, metalloproteinases, NF-kappaB, and ICAM-1 expression. J Trauma. 2006;60(1):115–125. | |
Shan D, Wu HM, Yuan QY, Li J, Zhou RL, Liu GJ. Pentoxifylline for diabetic kidney disease. Cochrane Database Syst Rev. 2012;2:CD006800. | |
Poggesi L, Scarti L, Boddi M, Masotti G, Serneri GG. Pentoxifylline treatment in patients with occlusive peripheral arterial disease. Circulatory changes and effects on prostaglandin synthesis. Angiology. 1985;36(9):628–637. | |
Weiss DJ, Geor RJ, Burger K. Effects of pentoxifylline on hemorheologic alterations induced by incremental treadmill exercise in thoroughbreds. Am J Vet Res. 1996;57(9):1364–1368. | |
Ingle-Fehr JE, Baxter GM. The effect of oral isoxsuprine and pentoxifylline on digital and laminar blood flow in healthy horses. Vet Surg. 1999;28(3):154–160. | |
Geor RJ, Weiss DJ, Burris SM, Smith CM II. Effects of furosemide and pentoxifylline on blood flow properties in horses. Am J Vet Res. 1992;53(11):2043–2049. | |
Barton MH, Moore JN, Norton N. Effects of pentoxifylline infusion on response of horses to in vivo challenge exposure with endotoxin. Am J Vet Res. 1997;58(11):1300–1307. | |
Baskett A, Barton MH, Norton N, Anders B, Moore JN. Effect of pentoxifylline, flunixin meglumine, and their combination on a model of endotoxemia in horses. Am J Vet Res. 1997;58(11):1291–1299. | |
Fugler LA, Eades SC, Moore RM, Koch CE, Keowen ML. Plasma matrix metalloproteinase activity in horses after intravenous infusion of lipopolysaccharide and treatment with matrix metalloproteinase inhibitors. Am J Vet Res. 2013;74(3):473–480. | |
Fugler LA, Eades SC, Koch CE, Keowen ML. Clinical and matrix metalloproteinase inhibitory effects of pentoxifylline on carbohydrate overload laminitis: preliminary results. [Abstract]. J Equine Vet Sci. 2010;30(2):106–107. | |
Visser MB, Pollitt CC. The timeline of metalloprotease events during oligofructose induced equine laminitis development. Equine Vet J. 2012;44(1):88–93. | |
Garcia FA, Pinto SF, Cavalcante AF, et al. Pentoxifylline decreases glycemia levels and TNF-alpha, iNOS and COX-2 expressions in diabetic rat pancreas. Springerplus. 2014;3(1):283–294. | |
Allen D Jr, Clark ES, Moore JN, Prasse KW. Evaluation of equine digital Starling forces and hemodynamics during early laminitis. Am J Vet Res. 1990;51(12):1930–1934. | |
Schnabel LV, Fortier LA, McIlwraith CW, Nobert KM. Therapeutic use of stem cells in horses: which type, how, and when? Vet J. 2013;197(3):570–577. | |
Sanchez LC, Robertson SA. Pain control in horses: what do we really know? Equine Vet J. 2014;46(4):517–523. | |
Robertson SA, Sanchez LC, Merritt AM, Doherty TJ. Effect of systemic lidocaine on visceral and somatic nociception in conscious horses. Equine Vet J. 2005;37(2):122–127. | |
Malone E, Ensink J, Turner T, et al. Intravenous continuous infusion of lidocaine for treatment of equine ileus. Vet Surg. 2006;35(1):60–66. | |
Thomasy SM, Slovis N, Maxwell LK, Kollias-Baker C. Transdermal fentanyl combined with nonsteroidal anti-inflammatory drugs for analgesia in horses. J Vet Intern Med. 2004;18(4):550–554. | |
Terry RL, McDonnell SM, Van Eps AW, et al. Pharmacokinetic profile and behavioral effects of gabapentin in the horse. J Vet Pharmacol Ther. 2010;33(5):485–494. | |
Kochová P, Witter K, Cimrman R, Mezerová J, Tonar Z. A preliminary study into the correlation of stiffness of the laminar junction of the equine hoof with the length density of its secondary lamellae. Equine Vet J. 2013;45(2):170–175. | |
Faramarzi B. Morphological and biomechanical properties of equine laminar junction. J Equine Vet Sci. 2014;34(5):589–592. | |
Thomason JJ, McClinchey HL, Faramarzi B, Jofriet JC. Mechanical behavior and quantitative morphology of the equine laminar junction. Anat Rec A Discov Mol Cell Evol Biol. 2005;283(2):366–379. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.