")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 8
The impact of anesthesia providers on major morbidity following screening colonoscopies
Authors Lubarsky D, Guercio J, Hanna J, Abreu M, Ma Q, Uribe C, Birnbach D, Sinclair D, Candiotti K
Received 12 November 2014
Accepted for publication 8 January 2015
Published 28 May 2015 Volume 2015:8 Pages 255—270
DOI https://doi.org/10.2147/JMDH.S77408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
David A Lubarsky,1 Jason R Guercio,2 John W Hanna,3,4 Maria T Abreu,5 Qianli Ma,3 Claudia Uribe,3 David J Birnbach,1,6 David R Sinclair,1 Keith A Candiotti1
1Department of Anesthesiology, Perioperative Medicine and Pain Management, University of Miami – Miller School of Medicine, Miami, FL, USA; 2Department of Anesthesiology, Duke University, Durham, NC, USA; 3Humana, Comprehensive Health Insights, Miami, FL, USA; 4University of Miami – Miller School of Medicine, Miami, FL, USA; 5Department of Medicine, Division of Gastroenterology, University of Miami – Miller School of Medicine, Miami, FL, USA; 6Department of Public Health Sciences, University of Miami – Miller School of Medicine, Miami, FL, USA
Background and aims: Few studies evaluate the impact of anesthesia providers during procedures, such as colonoscopy, on low-risk patients. The objective of this study was to compare the effect of anesthesia providers on several outcome variables, including major morbidity, following screening colonoscopies.
Methods: A propensity-matched cohort study of 14,006 patients who enrolled with a national insurer offering health maintenance organization (HMO), preferred provider organization (PPO), and Medicare Advantage plans for a screening colonoscopy between July 1, 2005 and June 30, 2007 were studied. Records were evaluated for completion of the colonoscopy, new cancer diagnosis (colon, anal, rectal) within 6 months of the colonoscopy, new primary diagnosis of myocardial infarction (MI), new primary diagnosis of stroke, hospital admission within 7 days of the colonoscopy, and adherence to guidelines for use of anesthesia providers.
Results: The presence of an anesthesia provider did not affect major morbidity or the percent of completed exams. Overall morbidity within 7 days was very low. When an anesthesia provider was present, a nonsignificant trend toward greater cancer detection within 6 months of the procedure was observed. Adherence to national guidelines regarding the use of anesthesia providers for low-risk patients was poor.
Conclusion: A difference in outcome associated with the presence or absence of an anesthesia provider during screening colonoscopy in terms of MI, stroke, or hospital admission within 7 days of the procedure was not observed. Adherence to published guidelines for the use of anesthesia providers is low. The incidence of completed exams was unaffected by the presence of an anesthesia provider. However, a nonstatistically significant trend toward increased cancer detection requires further study.
Keywords: safety, complications, myocardial infarction, stroke, endoscopy, anesthesiology
Introduction
Colorectal cancer is the third leading cause of cancer death among men and women in the US. In 2009, an estimated 146,970 cases were diagnosed and an estimated 49,920 deaths occurred.1 Current colon cancer prevention guidelines from the American Cancer Society are for average-risk men and women over 50 years of age to receive a flexible sigmoidoscopy every 5 years, a colonoscopy every 10 years, a double-contrast barium enema every 5 years, or a computed tomography colonography every 5 years to identify the presence of precancerous adenomatous polyps and detect colon cancer.2 Despite these recommendations, screening colonoscopies remain uncommon. An estimate by the Behavioral Risk Factor Surveillance System in 2001 estimated that only 47.3% of adults above the age of 50 years had ever undergone a lower endoscopy.3
Since screening colonoscopies are recommended for a large segment of the American population, the efficient use of resources is essential.4,5 Colonoscopies are rarely performed without sedation.6 Typically, sedative medications are administered to ensure patient comfort and to decrease awareness during the procedure. The overall cost of providing sedation for the colonoscopy increases if an anesthesia provider is present.
The value of having sedation for screening colonoscopies administered by anesthesia providers (anesthesiologists and/or certified registered nurse anesthetists [CRNAs]) has been debated. Much of the discussion centers around the use of propofol. Gastroenterologists frequently prefer propofol over other sedatives (such as opioids and benzodiazepines) due to propofol’s quick onset and quick offset. The beneficial effect of propofol on throughput is an important consideration for gastroenterologists.7,8 However, due to the US Food and Drug Administration’s (FDA) restrictions for propofol use exclusively among providers who have been trained in the administration of general anesthesia and not involved in the conduct of the surgical/diagnostic procedure, many gastroenterologists will not use propofol without the presence of a licensed anesthesia provider.9 Patients’ satisfaction appears equivocal, when choosing between sedation with propofol versus sedation with an opioid and benzodiazepine combination.10 However, researchers have stated that the presence of an anesthesia provider improves the quality of sedation and is cost-effective, allowing for a more complete and carefully conducted colonoscopy with improved health outcomes.11 Recent studies have challenged these assertions. In a retrospective population-based study of 165,527 procedures in 100,359 Medicare beneficiaries, including 35,128 (21.2%) who received anesthesia services, Cooper et al demonstrated that anesthesia services were associated with an increased risk of aspiration (0.14%) compared to non-anesthesia services (0.10%) (P=0.02).12 The increased risk of aspiration was the main factor accounting for the overall increase in complications (perforation and splenic injury) in patients undergoing colonoscopy with anesthesia services (0.22%) compared to without anesthesia services (0.16%) (P=0.0001).
Mortality following a screening colonoscopy is a rare event.12 The overall 30-day mortality is 0.29% and was similar in the anesthesia (0.32%) and non-anesthesia (0.28%) groups (P=0.29). The overall 1-year mortality was 2.68% and was also similar in the anesthesia (2.82%) and non-anesthesia (2.64%) groups (P=0.06). Although the absolute risk of 30-day and 1-year mortality was low, the frequency of major cardiac or neurologic morbidity is unknown.
This study evaluates the impact of anesthesia services on major morbidity associated with myocardial infarction (MI) or stroke within 7 days following a screening colonoscopy. In addition, the efficacy, completion rate, incidence of a repeat colonoscopy within 6 months, and incidence of hospital admission within 7 days following a screening colonoscopy were also studied. We hypothesize that the presence of an anesthesia provider during colonoscopy would result in a more complete exam and an associated increased incidence of cancer detection. Additionally, we hypothesize that sedation administered by an anesthesia provider would be associated with fewer serious complications during and after a screening colonoscopy, due to better sedation management skills. Diagnostic outcomes and adverse events associated with the presence or absence of an anesthesia provider in a large population undergoing screening colonoscopies are evaluated. In addition, adherence to the 2004 joint national guidelines published by the American College of Gastroenterology (ACG), American Gastroenterological Association (AGA), and American Society of Gastrointestinal Endoscopy (ASGE) on the use of anesthesia providers during screening colonoscopies is studied.
Methods
After institutional review board approval, a cross-sectional and retrospective cohort analysis was conducted, using medical and pharmaceutical claims data for a representative population insured through commercial (HMO or PPO) or Medicare Advantage plans administered by Humana, Inc. Three electronic databases were merged. The member file database contained demographic information for each member per encounter (age, sex, type of insurance, and geographical region). The medical file database stored up to nine recorded International Classification of Diseases Ninth revision (ICD-9) codes per encounter, the primary code/reason for the encounter, the Current Procedural Terminology (CPT) codes, the CPT modifiers, and the G codes for procedures. The pharmacy file contained all Generic Product Identifier (GPI) numbers of pharmacy-dispensed medications per claim.
Study population
Between the identification period of July 1, 2005 and June 30, 2007, patients 50 years of age and older with at least one medical claim containing 45,355, 45,378, or 45,380 CPT codes for colonoscopy and at least one G0121 or G0105 code were identified. To increase the likelihood of capturing only screening colonoscopies, patients with prior history (by ICD-9 code) of colorectal cancer, ulcerative colitis, or Crohn’s disease involving the colon during the 12-month baseline period were excluded. The index date was defined as the date of the first medical claim for screening colonoscopy. Patients were eligible for the study if they had 18 months of continuous insurance enrollment, defined as at least 12 months of baseline coverage prior to the index date and at least 6 months of follow-up coverage. All codes used in the analysis are listed in Table S1.
Baseline characteristics
Baseline characteristics for all patients include the demographics (sex, age, race/ethnicity, and type of health insurance plan), the Deyo–Charlson Modified Comorbidity Index, and the Revised Cardiac Risk Index (RCRI). The American Society of Anesthesiologists’ (ASA) Physical Status Classification was noted whenever it was coded. The Deyo–Charlson modified index is an extensively studied and validated comorbidity index, which has been adapted for use with ICD-9 databases and includes 17 diseases that have been selected and weighted on the basis of the strength of their association with mortality.13
Definition of average-risk and high-risk patients
All patients were defined as either average-risk or high-risk, based upon their baseline characteristics of the RCRI score calculated using baseline period claims data.5 A subset of patients was also risk stratified by ASA status if the physical status CPT modifier was submitted either with the claim for screening colonoscopy or in the year prior to the index date. In the latter case, the most recent ASA status was used.
Average-risk patients were defined as those with an RCRI Class score of I or II, which means not having any risk factors or one risk factor of ischemic heart disease, history of congestive heart failure, history of cerebrovascular disease, insulin therapy for diabetes, or renal insufficiency. Patients with the risk factor of “insulin therapy for diabetes” must have had claims with an ICD-9 code for diabetes and a GPI code for insulin. High-risk patients were defined as those with an RCRI Class score of III or IV, which means two or more of the RCRI risk factors.
Presence or absence of anesthesia provider
The presence of an anesthesia provider was identified by the 00810 CPT code (anesthesia for lower intestinal endoscopic procedures, endoscope introduced distal to duodenum) submitted with the screening colonoscopy claim. If no claims for anesthesia services were associated with the submitted screening colonoscopy claim, then no anesthesia provider was presumed to be present.
Outcome and process measurements
Six months of follow-up claims were evaluated to identify whether the diagnosis of new colon cancer was made within 6 months of the colonoscopy; whether the colonoscopy was completed on the index date; whether repeating the colonoscopy was necessary; whether new primary ICD-9 diagnosis codes for MI and stroke were added within 7 days of the procedure; and whether hospital admission was required within 7 days. Each patient was followed for a 6-week period after the colonoscopy (latest follow-up was December 31, 2007). Adherence to ACG/AGA/ASGE guidelines, which support the administration of sedation by non-anesthesia providers to average-risk patients receiving a screening colonoscopy, was measured.14
Statistical analysis
Descriptive statistics were produced for each set of the study measures. Mean and reported standard deviation for continuous variables, and frequency counts and percentage for categorical variables, were reported. McNemar’s test was used to determine the statistical significance of differences in categorical measures, including comparison of the ratings based on RCRI score and ASA status.
The study cohorts for evaluating the impact of an anesthesia provider were obtained by matching patients who had an anesthesia provider on the index date with those without an anesthesia provider, using the propensity score method on a 1:1 basis.15 The Parsons algorithm selected matched pairs and the final cohorts, using the five digits match.16
Logistic regression using the generalized estimating equations (GEE) method was used to incorporate the matched pairs design and compare the effects of having an anesthesia provider present on the efficacy of colonoscopy in identifying colon cancer; the completion of the colonoscopy on the index date (as defined by coding that the examination was completed distal to the splenic flexure); the requirement for a repeat colonoscopy within 6 months; the development of an MI (a new primary ICD-9 code for the hospital encounter) within 7 days of colonoscopy; the incidence of stroke (a new primary ICD-9 code for the hospital encounter) within 7 days of colonoscopy; and the incidence of a hospital admission within 7 days of the screening colonoscopy in both groups. SAS (v.9.1; SAS Institute Inc., Cary, NC, USA) was used for all statistical analyses.
Results
Baseline characteristics
Table 1 reports the demographics and the frequency of comorbid conditions among the patients who received screening colonoscopies. Inclusion criteria were met by 63,750 Humana members. Only 6.52% of subjects had an ASA score submitted, of which the most commonly reported score was a physician status 3.The majority of patients had 0 or 1 RCRI factors (73% and 19%, respectively). An anesthesia provider was present in 25.48% of screening colonoscopies.
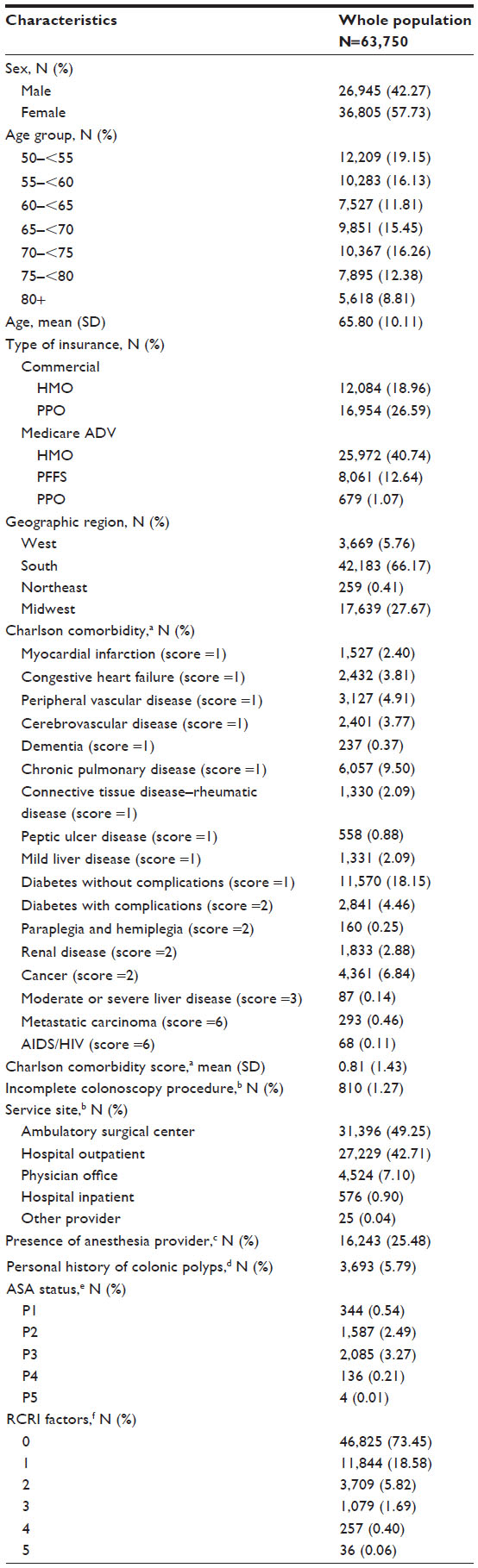 | Table 1 Baseline demographic and clinical characteristics in whole population |
Provider type, outcomes, and adverse events
High-risk patients were significantly more prevalent among the group having an anesthesia provider present during the colonoscopy (9.3% vs 7.5%, P<0.0001). Through propensity scoring using the Charlson comorbidity index and RCRI score, 14,006 colonoscopy patients were matched (7,003 patients in the group without an anesthesia provider and 7,003 with an anesthesia provider). The demographics of the two matched groups are shown in Table 2.
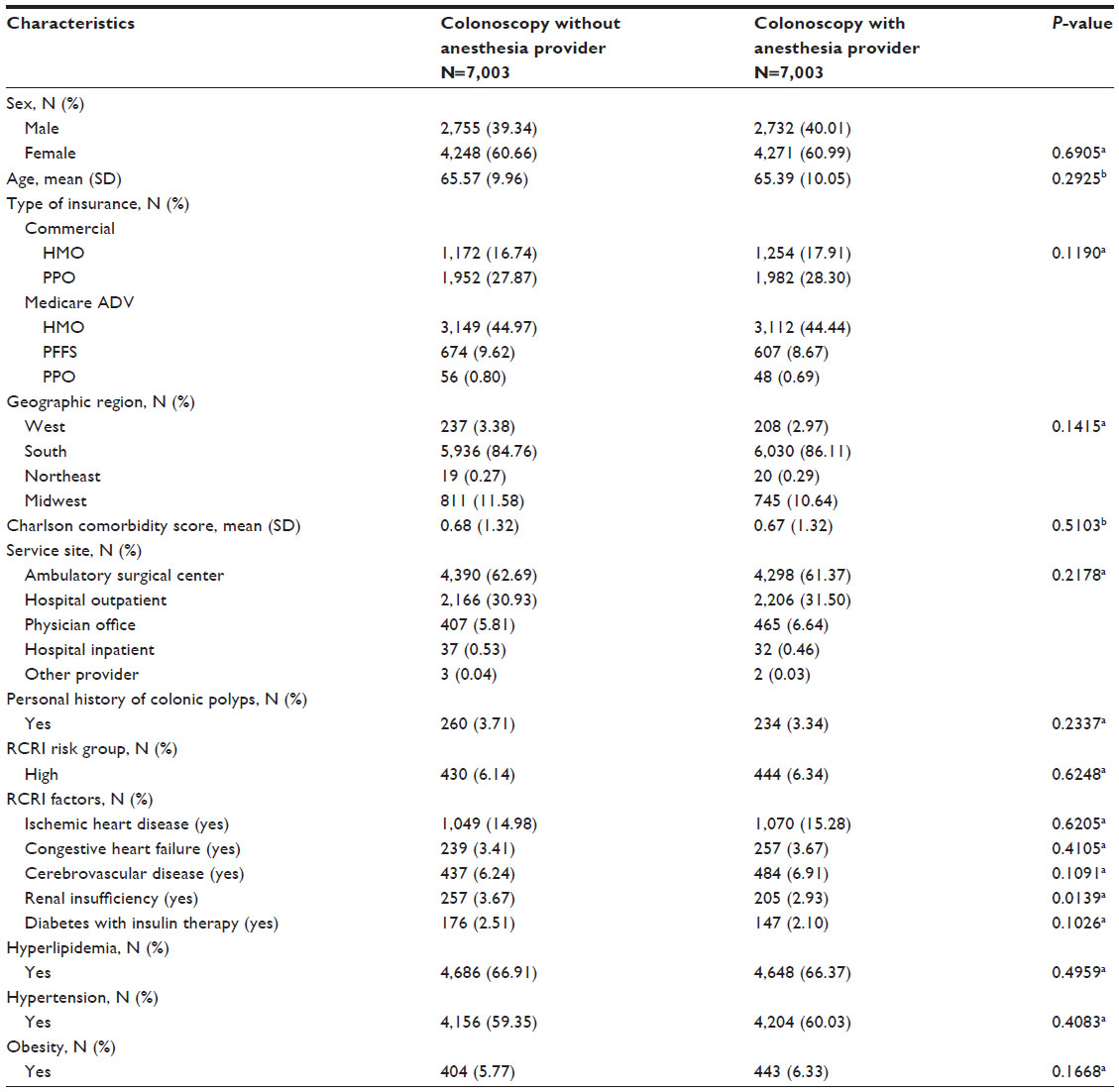 | Table 2 Baseline demographic and clinical characteristics after propensity score matching (N=14,006) |
MIs (0.07%), strokes (0.06%), and hospital admissions (0.76%) within 7 days of the procedure were rare in both groups. A significant difference in the number of these events between the groups did not exist. The incidence of incomplete colonoscopies was not significantly different between those procedures performed with or without an anesthesia provider (1.39% and 1.14%, respectively). However, the incidence of repeat colonoscopies were significantly increased following a colonoscopy without an anesthesia provider as compared to with an anesthesia provider (2.40% vs 1.78%, P<0.02). A nonsignificant trend toward a greater likelihood of a cancer diagnosis was present if an anesthesia provider was involved (2.03% vs 1.7%, P=0.13) (Tables 3 and 4).
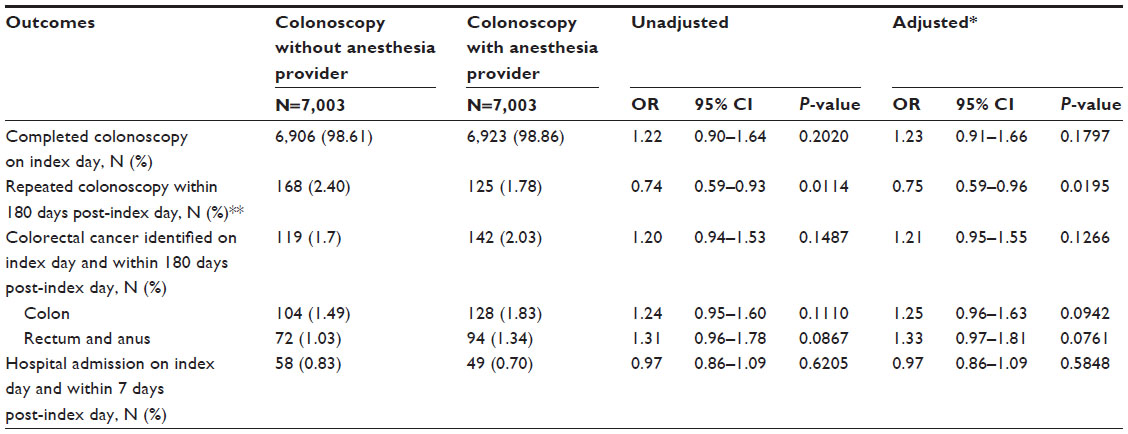 | Table 3 Comparison of colonoscopy outcomes |
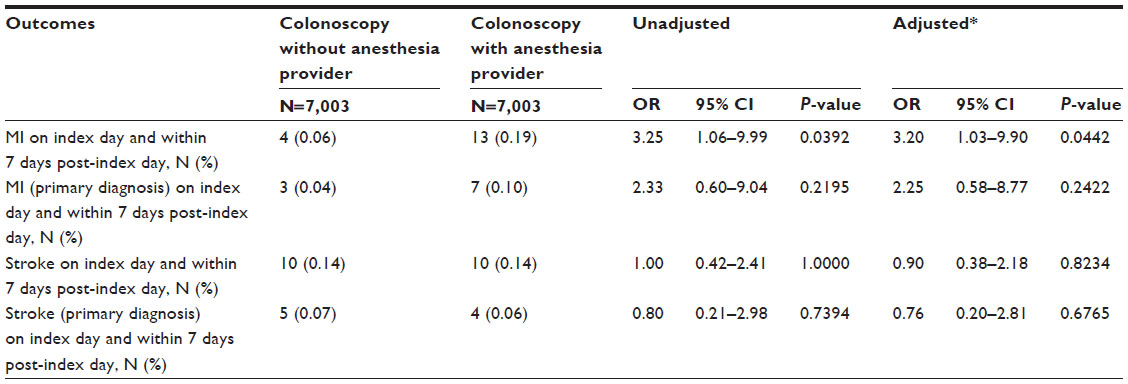 | Table 4 Comparison of cardiovascular outcomes |
Adherence to guidelines
Nine point three one percent of the 16,243 patients who had an anesthesia provider qualified as high-risk by RCRI criteria. The remaining 90.69% of the patients were average-risk. The demographics of those with an anesthesia provider versus those without an anesthesia provider are shown on Table 5.
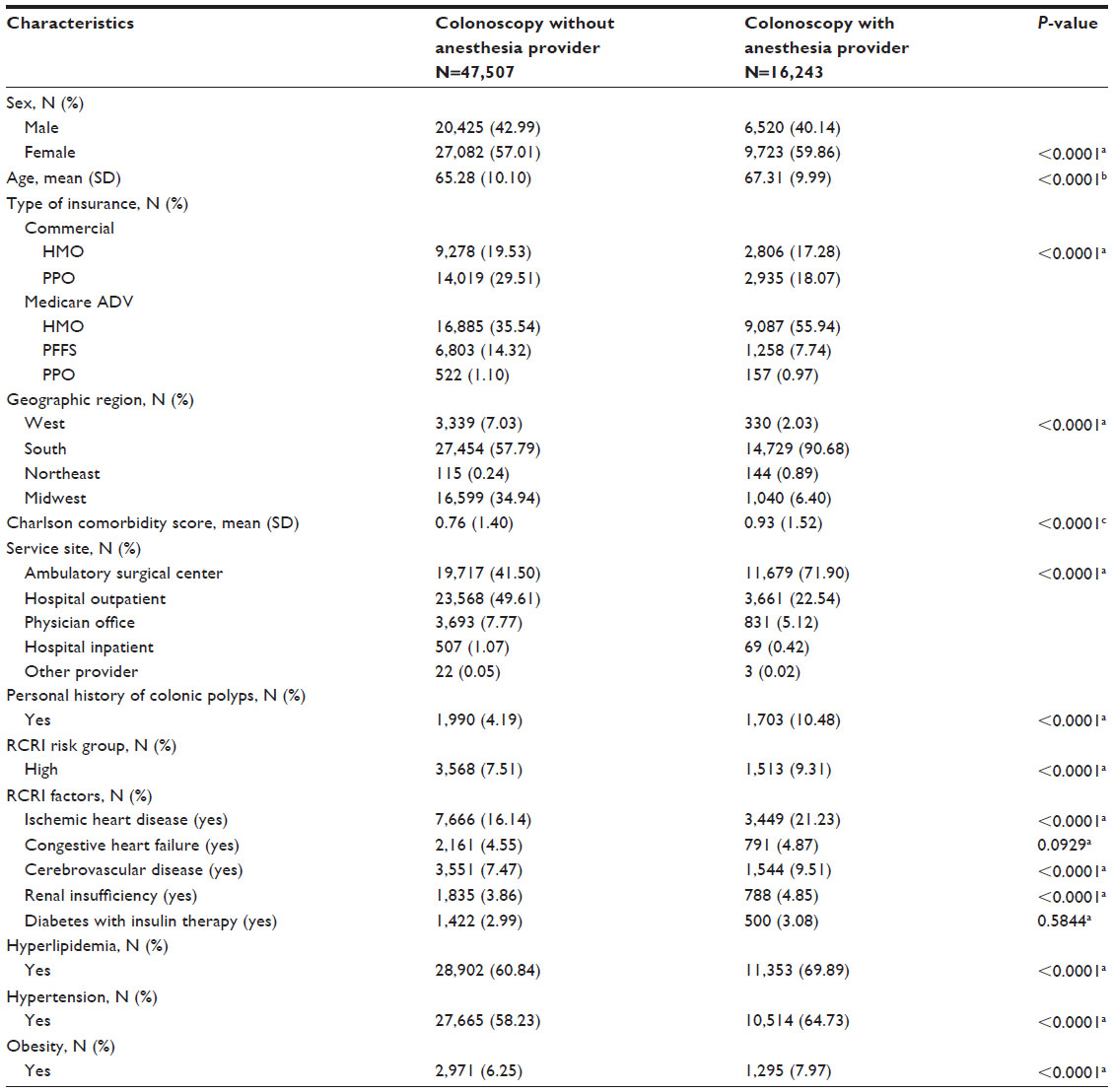 | Table 5 Baseline demographic and clinical characteristics (N=63,750) |
Discussion
This retrospective observational study of a large health benefits claims database evaluated the impact of the presence or absence of an anesthesia provider on major morbidity for a large population of average- and high-risk patients undergoing screening colonoscopies. Anesthesia providers were present 25.48% of the time, which is consistent with previously published US and Canadian rates of 27.8% and 19.1%, respectively.6,17
Our study demonstrates that, in a population of predominantly average-risk patients, the presence of an anesthesia provider during a colonoscopy has no impact on the incidence of MI or stroke. However, a statistically significant decrease in the rate of repeated colonoscopies (0.7%) was associated with the presence of an anesthesia provider. Although further study with sufficient power is needed to confirm the finding of a nonsignificant trend toward increased cancer detection, the decrease in repeat colonoscopies may be consistent with the nonsignificant trend toward greater cancer detection when an anesthesia provider is present. If a gastroenterologist were more inclined to avoid repeating a colonoscopy or aborting a procedure when an anesthesia provider manages the commonly occurring complications of hypoxemia (55.6%), bradycardia (5.6%), and hypotension (8.9%), they may identify more lesions and be more confident that a sufficiently thorough exam was performed.18
Guidelines prepared jointly by the ACG, AGA, and ASGE, addressing the issue of sedation during routine lower endoscopic procedures, do not support the administration of moderate sedation by specially trained anesthesia providers to average-risk patients. However, for high-risk patients, the guidelines suggest that the administration of sedation by an anesthesiologist or other anesthesia provider might be considered.17 Conflicting results regarding outcomes and adverse events exist.19 The ASA has equivocated on whether the immediate availability of a provider with postgraduate training in anesthesiology increases the likelihood of a satisfactory outcome or decreases the associated risks associated with moderate sedation (more commonly performed on average-risk patients). For deep sedation or when procedures are performed on high-risk patients, the ASA agrees that the immediate availability of an anesthesiologist increases the likelihood of satisfactory sedation and decreases the likelihood of adverse outcomes.20 However, recent data suggests that the use of propofol by anesthesiologists has been associated with an increased risk of aspiration pneumonia among Medicare patients undergoing outpatient colonoscopy.12 Agostoni et al found that pulmonary aspiration is the most common significant complication of a colonoscopy.21 Additional evidence attributes the risk of respiratory complications and infections following endoscopies and colonoscopies to the depth of sedation achieved during the procedure.22
National guidelines regarding the use of anesthesia providers are not commonly followed in clinical practice. Currently, an endoscopist’s decision to include an anesthesia provider has largely been dependent upon their level of comfort managing the administration of sedation and their desire to best meet the needs of their patients. The implementation of any guideline requires an understanding of existing trends in clinical practice and a commitment at the national, regional, and local levels to adapt evidence-based recommendations to available resources. In the absence of any outcome study, individual physicians may rationalize more care than less.
Our study contains a number of limitations related to its retrospective nature and use of insurance claims data. The “presence of anesthesia provider” does not differentiate between the presence of an anesthesiologist (or the subset of board-certified anesthesiologists) or a CRNA. Perhaps measuring outcomes separately would reveal different outcomes between the two provider groups. Similarly, in the “absence of anesthesia provider” group, almost all patients still received some degree of sedation. However, no method existed to determine if the sedation was administered by another physician or registered nurse. Furthermore, the medications used to provide sedation could not be identified. Medications represent a potential confounding variable, as they differ in their safety and pharmacologic profiles. As an example, anesthesia providers are more likely to utilize medications such as propofol, which has more profound pharmacodynamic effects than other sedatives. Data on the type of anesthesia administered (general anesthesia, deep sedation, or moderate sedation) was not available. However, given the extremely low incidence of complications, the likely that further stratification of providers, depth of anesthesia, or type of sedative medications administered would change our conclusions is low. Finally, polyp yield from the colonoscopy procedure and histology and staging for cases of colon cancer identified were not available in the dataset, which might have caused a missed benefit of having an anesthesia provider present, if effectiveness of the screening examination was considered using that data. There were a very small number of cardiovascular events from which to draw conclusions about the choice of professionals providing sedation.
Evaluating the effectiveness of the therapies and the usefulness of anesthesia providers for routine screenings, treatments, or symptom management is a national imperative of medical research. This study helps formulate updated policies related to endoscopic sedation and advances the understanding of health care expenditures about the outcomes related to sedation during colonoscopy. Through additional carefully conducted research and thoughtful analysis, physicians and guideline-setting organizations will be able to make recommendations on the optimal use of health resources, for the benefit of individual patients and the health of our society.
Conclusion
The presence of an anesthesia provider during a screening colonoscopy did not affect the incidence of completed colonoscopies or the incidence of significant morbidity. MI and stroke following screening colonoscopies are very rare. A nonstatistically significant trend toward increased cancer detection was found, when an anesthesia provider was present. Furthermore, repeat colonoscopies were significantly increased following a colonoscopy without an anesthesia provider. Adherence to 2004 published guidelines by several societies representing gastroenterologists regarding the use of anesthesia providers was poor.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
We would like to thank Valerie A Arkoosh, MD, MPH, of the University of Pennsylvania – Department of Anesthesiology for her assistance with this project. We would also like to thank Ms Garla Connor and Miss Krystie Cabrales for their assistance with manuscript preparation.
Disclosure
Qianli Ma and Claudia Uribe are employed by Humana. John Hanna was employed by Humana at the time the project was conducted. The other authors report no conflicts of interest in this work.
References
Jemal A, Siegel R, Ward E, et al. Cancer Statistics, 2009. CA Cancer J Clin. 2009;59(4):225–249. | |
Levin B, Lieberman DA, McFarland B, et al; American Cancer Society Colorectal Cancer Advisory Group; US Multi-Society Task Force; American College of Radiology Colon Cancer Committee. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58(3):130–160. | |
Centers for Disease Control and Prevention (CDC). Colorectal cancer test use among persons aged > or =50 years – United States, 2001. MMWR Morb Mortal Wkly Rep. 2003;52(10):193–196. | |
Walsh JM, Terdiman JP. Colorectal cancer screening: scientific review. JAMA. 2003;289(10):1288–1296. | |
Lee TH, Mercantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043–1049. | |
Cohen LB, Wecsler JS, Gaetano JN, et al. Endoscopic sedation in the United States: results from a nationwide survey. Am J Gastroenterol. 2006;101(5):967–974. | |
Atkinson M, Schmulewitz N. Downstream hospital charges generated from endoscopic ultrasound procedures are greater than those from colonoscopies. Clin Gastroenterol Hepatol. 2009;7(8):862–867. | |
Cohen LB. Production pressure in endoscopy: balancing quantity and quality. Gastroenterology. 2008;135(6):1842–1844. | |
Official Propofol FDA Monograph [webpage on the Internet]. Drugs.com. Available from: http://www.drugs.com/pro/propofol.html. Accessed January 16, 2015. | |
Cohen LB, Delegge MH, Aisenberg J, et al; AGA Institute. AGA Institute review of endoscopic sedation. Gastroenterology. 2007;133(2):675–701. | |
Aetna Retreats on Anesthesia Limits During Colonoscopy [webpage on the Internet]. Wall Street Journal Online. Available from: http://blogs.wsj.com/health/2008/02/27/aetna-retreats-on-anesthesia-limits-during-colonoscopy/. Accessed January 16, 2015. Digestive Disease Week (DDW) 2009: Abstract 722. Presented June 1, 2009. Available from: http://www.medscape.com/viewarticle/703648?src=mpnews&spon=7&uac=36797CY. Accessed January 16, 2015. | |
Cooper GS, Kou TD, Rex DK. Complications following colonoscopy with anesthesia assistance: a population-based analysis. JAMA Intern Med. 2013;173(7):551-556. | |
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619. | |
Gastroenterology Societies Reach Consensus on Recommendations for Sedation During Endoscopic Procedures [webpage on the Internet]. Bethesda, MD: American Gastroenterological Association. Available from: http://www.gastro.org. Accessed January 16, 2015. | |
D’Agostino RB Jr. Propensity score methods for bias reduction in the comparison of a treatment to a nonrandomized control group. Stat Med. 1998;17(19):2265–2281. | |
Parsons LS. Performing a 1:N case-control match on propensity score: Proceedings of the Twenty-Ninth Annual SAS® Users Group International Conference, Montréal, Canada, 9–12 May 2004. Cary, NC: SAS Institute Inc.; 2004. | |
Alharbi O, Rabeneck L, Paszat LF, et al. A population-based analysis of outpatient colonoscopy in adults assisted by an anesthesiologist. Anesthesiology. 2009;111(4):734–740. | |
Khalid-de Bakker CA, Jonkers DM, Hameeteman W, de Ridder RJ, Masclee AA, Stockbrügger RW. Cardiopulmonary events during primary colonoscopy screening in an average risk population. Neth J Med. 2011;69(4):186–191. | |
Vargo JJ, Holub JL, Faigel DO, Lieberman DA, Eisen GM. Risk factors for cardiopulmonary events during propofol-mediated upper endoscopy and colonoscopy. Aliment Pharmacol Ther. 2006;24(6):955–963. | |
American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96(4):1004–1017. | |
Agostoni M, Fanti L, Gemma M, Pasculli N, Beretta L, Testoni PA. Adverse events during monitored anesthesia care for GI endoscopy: an 8-year experience. Gastrointest Endosc. 2011;74(2):266–275. | |
Friedrich K, Scholl SG, Beck S, et al; bng-Study-Group. Respiratory complications in outpatient endoscopy with endoscopist-directed sedation. J Gastrointestin Liver Dis. 2014;23(3):255–259. |
Supplementary table
 | Table S1 |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.