")
Back to Journals » Clinical Epidemiology » Volume 6
The epidemiology of Sjögren’s syndrome
Received 4 February 2014
Accepted for publication 19 March 2014
Published 30 July 2014 Volume 2014:6 Pages 247—255
DOI https://doi.org/10.2147/CLEP.S47399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Ruchika Patel, Anupama Shahane
Division of Rheumatology, University of Pennsylvania, Philadelphia, PA, USA
Abstract: Sjögren’s syndrome is a chronic systemic autoimmune disease characterized by lymphocytic infiltration of exocrine glands. It can present as an entity by itself, primary Sjögren's syndrome (pSS), or in addition to another autoimmune disease, secondary Sjögren's syndrome (sSS). pSS has a strong female propensity and is more prevalent in Caucasian women, with the mean age of onset usually in the 4th to 5th decade. Clinical presentation varies from mild symptoms, such as classic sicca symptoms of dry eyes and dry mouth, keratoconjunctivitis sicca, and xerostomia, to severe systemic symptoms, involving multiple organ systems. Furthermore, a range of autoantibodies can be present in Sjögren's syndrome (anti-SSA/Ro and anti-SSB/La antibodies, rheumatoid factor, cryoglobulins, antinuclear antibodies), complicating the presentation. The heterogeneity of signs and symptoms has led to the development of multiple classification criteria. However, there is no accepted universal classification criterion for the diagnosis of Sjögren's syndrome. There are a limited number of studies that have been published on the epidemiology of Sjögren's syndrome, and the incidence and prevalence of the disease varies according to the classification criteria used. The data is further confounded by selection bias and misclassification bias, making it difficult for interpretation. The aim of this review is to understand the reported incidence and prevalence on pSS and sSS, the frequency of autoantibodies, and the risk of malignancy, which has been associated with pSS, taking into account the different classification criteria used.
Keywords: Sjögren's syndrome, incidence, prevalence, classification criteria, autoantibodies, lymphoma
Introduction
Sjögren’s syndrome (SS) is a chronic systemic autoimmune disease that is best characterized by lymphocytic infiltration of the exocrine glands and epithelia resulting in classic sicca symptoms of dry eyes and dry mouth, and objective evidence of keratoconjunctivitis sicca and xerostomia. SS can present as an entity by itself, without an underlying autoimmune condition – primary SS (pSS) – or may occur in conjunction with an underlying autoimmune condition – secondary SS (sSS). Clinical presentation can vary considerably from relatively mild sicca symptoms, arthralgias, and fatigue to severe systemic symptoms such as vasculitis, glomerulonephritis, and a host of neurological manifestations. The heterogeneity of signs and symptoms often leads to a delay in diagnosis.
The variability of presentation has led to the development of several classification criteria for SS. Due to the lack of universally accepted classification criteria, estimated incidence and prevalence of the disease varies significantly depending on the criteria used.
Objectives
The objectives of this article are to review the frequently used classification criteria for SS and review published data on incidence and prevalence of SS. The article reviews the prevalence of SS in association with other autoimmune conditions and autoantibodies in SS.
Classification criteria
The three most commonly used criteria for the diagnosis of pSS are: 1) the Copenhagen criteria; 2) the European classification criteria; and 3) the International Collaborative Clinical Alliances Cohort (Table 1). The Copenhagen criteria, proposed in 1986, included objective evidence of keratoconjunctivitis sicca, salivary gland involvement, and whole unstimulated salivary flow.1 The European classification criteria was initially proposed in 1996 and was later revised in 2002 by the American–European consensus group (AECG). According to this criteria, the diagnosis of pSS can be met by fulfilling four out of six items. Four of the six items include subjective or objective evidence of keratoconjunctivitis sicca and xerostomia. The two final items include a positive minor salivary gland biopsy with a focus score of ≥1/4 mm2 or the presence of anti-Ro/SSA or anti-La/SSB antibodies.2
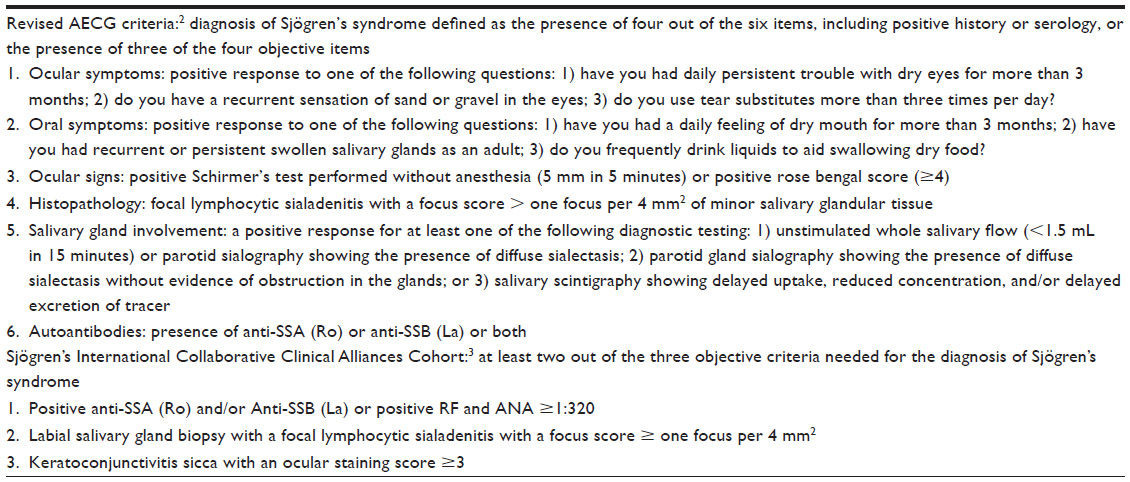 | Table 1 Different criteria used for the diagnosis of primary Sjögren’s syndrome |
The third classification criteria, proposed in 2012 by the Sjögren’s International Collaborative Clinical Alliances Cohort, has since been approved by the American College of Rheumatology. Based on this criteria, the diagnosis of pSS can be established with the presence of two or more of the following objective findings: 1) positive anti-Ro/SSA and/or anti-La/SSB antibodies, or positive rheumatoid factor (RF) and positive antinuclear antibodies (ANA); 2) positive minor salivary gland biopsy with a focus score of ≥1/4 mm2; and 3) keratoconjunctivitis sicca with an ocular staining score of ≥3.3 Both the American–European consensus and the International Collaborative Clinical Alliances Cohort have been validated in further studies with a sensitivity and specificity of greater than 90%.3,4 This paper reviews the incidence and prevalence of SS, as reported in the medical literature. A PubMed search was conducted using the terms “Sjögren’s syndrome”, “incidence”, “prevalence”, and “epidemiology”; reviews, case reports, and case series published between the years of 1970 and 2013 were reviewed.
Primary Sjögren’s syndrome
In the realm of autoimmune diseases, pSS is a relatively common disease. However, only a limited number of epidemiologic studies estimating the prevalence of this disease have been published. In these studies, the estimated prevalence of pSS varies even within the same geographical area, depending on the type of classification criteria used. This is further confounded by selection bias and misclassification bias making it difficult for interpretation.
As with most autoimmune diseases, pSS has a strong female propensity. Depending on the studies, female to male ratio varies from as high as 20:1 to 9:1.5,6 pSS is more prevalent in Caucasian women and, although it may present at any age, the mean age of onset is usually in the 4th to 5th decade.
Incidence
In our review, we noted three studies estimating the incidence of pSS. The first retrospective study, from Olmstead County, Minnesota, USA, reviewed data between 1976 and 1992. It estimated the annual incidence of pSS at 3.9 per 100,000 (95% confidence interval [CI] 2.8–4.9). A higher prevalence was noted in women compared to men (6.9 [95% CI 5.0–8.8] versus 0.5 [95% CI 0.0–1.2] per 100,000).7 The second, a prospective study from Slovenia between 2000 and 2002, estimated the incidence of pSS also at 3.9 per 100,000 (95% CI 1.1–10.2), in a population of 599,589. The incidence of pSS was noted to be ten times higher in women compared to men from Slovenia.8 The third, a prospective study from Greece, identified 422 new cases of pSS in a population of 488,435 from 1982 to 2003, with reported incidence of 5.3 per 100,000 (95% CI 4.5–6.1). In this population, in northwest Greece, women were 20 times more likely to be affected than men.6
Prevalence
The prevalence rates can vary considerably depending on the classification criteria used (Table 2). This is demonstrated by the following three studies. A large Norwegian population based study, the Hordaland Health Study, estimated the point prevalence percentage of pSS in individuals aged 40–44 years at 0.44 (95% CI 0.34–0.57) using the European criteria, and 0.22 (95% CI 0.15–0.32) using the revised criteria.9 This study also demonstrated that individuals aged 71–74 years compared to those aged 40–44 years had an 8.07 times higher prevalence rate of pSS using the European criteria, and a 6.36 times higher prevalence rate using the revised criteria. In the two other Scandinavian countries, Denmark and Sweden, the prevalence of pSS has been reported as 0.2%–2.1%, and 2.7%, respectively.10,11
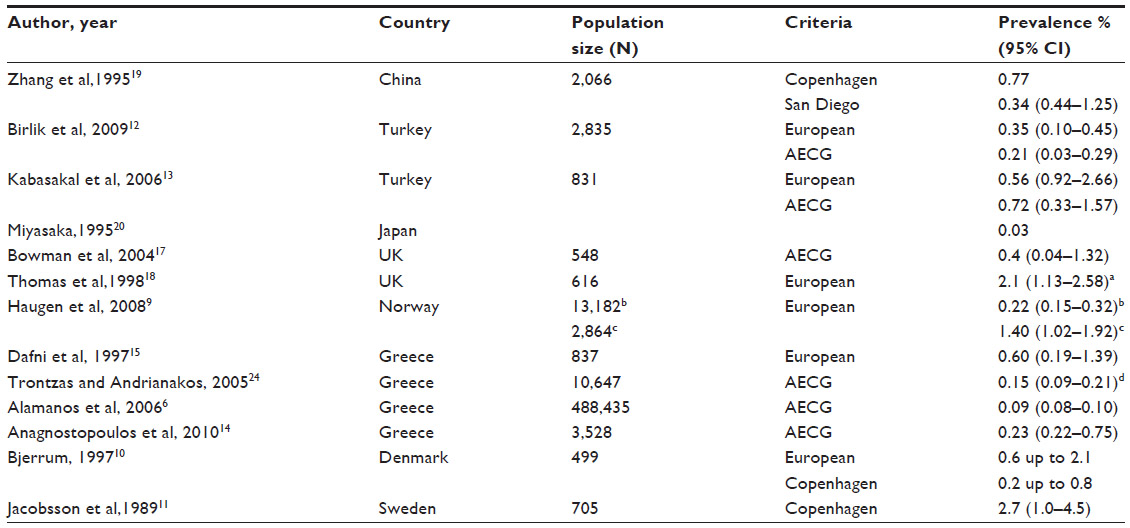 | Table 2 A summary of studies on the prevalence of primary Sjögren’s syndrome according to diagnostic criteria used |
A Turkish study reported by Birlik et al estimated the prevalence of pSS at 0.35 (95% CI 0.10–0.45) using the European criteria and 0.21 (95% CI 0.03–0.29) using the revised AECG criteria.12 The third study, a cross-sectional population based survey in Turkey by Kabasakal et al, estimated the prevalence of pSS in women aged 18–75 years at 1.56 (95% CI 0.92–2.66) using the European Criteria and 0.72 (95% CI 0.33–1.57) using the revised criteria.13
The reported prevalence in Greece ranges from 0.09%–0.23%6,14,15 and prevalence in Slovenia is estimated at 0.60%.16
In the United Kingdom, two large cross-sectional population based surveys, in Manchester and Birmingham, estimated the prevalence of pSS using the revised AECG criteria at 1.6 (95% CI 9–26) and 0.14 (95% CI 0.02–0.51), respectively.17,18 Both studies involved questionnaires that were sent to adults who were followed in their general practice clinic; however, in the study from Birmingham the questionnaires were only sent to Caucasian women, aged 35–74 years, making it difficult to interpret the data due to selection bias. If there was a high suspicion of pSS based on the survey, these patients were invited to the clinic for the diagnosis of pSS based on serological makers and objective evidence of keratoconjunctivitis sicca.
The estimated prevalence of pSS in Beijing, China, is 0.77% using the Copenhagen criteria.19 A low prevalence of 0.03% has been reported in a population-based study in Japan by Miyasaka,20 which increases to 2.3% when evaluated among Nagasaki atomic bomb survivors.21
Primary Sjögren’s in the elderly
Although the mean age of onset of pSS is usually in the 4th to 5th decade, onset of the disease in the 6th or 7th decade is not uncommon. An Italian cohort of 322 consecutive patients with pSS between 1990 and 2007 was studied retrospectively, where pSS was noted in 6% of adults over 65 years of age.22 A Spanish cohort of 223 consecutive pSS patients noted the disease in 14% of adults aged 70–87 years.23
The prevalence of pSS in the elderly population is between five to eight times higher, depending on the age used to define the population. In a Norwegian study by Haugen et al,9 the prevalence of pSS is six to eight times higher in adults aged 71–74 years compared to younger adults aged 40–44 years. In Greece, the prevalence of pSS is five times higher in adults over 65 years of age,24 and, in the UK, Thomas et al reported prevalence rates of 4.9% in adults over 55 years of age.18 There are several factors that can contribute to the higher observed prevalence rate of pSS in the elderly population. A multitude of factors, including physiological decrease in saliva production, higher rates of comorbid conditions such as diabetes, as well as polypharmacy, can contribute to decreased saliva production, which can potentially cause more pronounced subjective and objective evidence of sicca symptoms.9 There is also an increased prevalence of autoantibodies in the elderly. The host of factors can confound the true prevalence of pSS in the elderly.
Primary Sjögren’s in children
pSS is rare in children; only 81 cases have been reported in the literature from 2000–2010. The age of diagnosis ranges from 4 to 16 years (mean age of 9.84 years). Female to male ratio of 5:1 is observed in children.25
Secondary Sjögren’s syndrome
Secondary SS is associated with a number of autoimmune diseases (Table 3). This has been reviewed extensively by two papers: Theander and Jacobsson,26 and Ramos-Casals et al.27
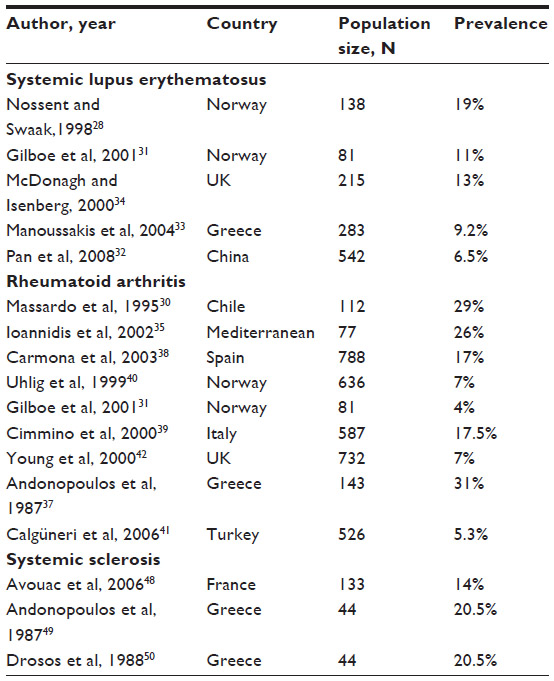 | Table 3 Prevalence of secondary Sjögren’s syndrome in SLE, RA, and systemic sclerosis |
Secondary Sjögren’s syndrome and systemic lupus erythematosus
The prevalence of sSS in Secondary Sjögren’s syndrome and systemic lupus erythematosus (SLE) is wide-ranging, varying from 6.5%–19%, which can be partly attributed to the application of different criteria.28–33 The age of onset of sSS in SLE is higher than the onset of SLE itself: 48.3±2.5 years versus 36.1±1.6 years.31 SLE patients with sSS have an increased expression of anti-SSA, anti-SSB, anti-ribonucleoprotein antibodies, and RF. These patients are more likely to have Raynaud’s phenomenon but have lower rates of thrombocytopenia, renal involvement, and lymphadenopathy as compared to patients with SLE alone.27,28,32,34 Similar findings were observed in a Chinese prospective study, where 542 consecutive patients with SLE were enrolled from 1999–2005.32 An estimated prevalence of sSS in SLE was noted at 6.5%, based on a thorough objective assessment of lacrimal and salivary glands, including a slit lamp examination with rose bengal staining and unstimulated whole salivary flow. Patients with subjective symptoms but no objective symptoms were excluded from the study. Patients with subjective and objective evidence of sicca symptoms then underwent a minor salivary glands biopsy; if positive, they met the AECG criteria for the diagnosis of SS.32
Patients over 50 years of age may have an atypical presentation of SLE, and a higher occurrence of autoantibodies (ANA, anti-SSA/SSB, and RF) is noted. Since, the overall prevalence of pSS is more frequent in this age group, differentiating between pSS and SLE in this population can be challenging.27
Secondary Sjögren’s syndrome and rheumatoid arthritis (RA)
Overall, sSS is a common extra-articular manifestation of RA. Within Mediterranean countries, the highest prevalence of sSS in RA is reported in Greece, ranging from 26%–31%.33,35–37 A large cross-sectional study in Spain estimated the prevalence of sSS at 17% in 788 RA patients over a 10 year period.38 A similar prevalence rate of 17.5% was noted in a prospective study of 587 consecutive RA patients in Italy.39 In Chile, sSS in RA patients is reported at 29%.30 On the other hand, lower rates of sSS in RA have been reported; 4%–7% in Norway,29,40 5.3% in Turkey,41 and 7% in the UK.42
Secondary Sjögren’s syndrome and mixed connective tissue disease (MCTD)
Two studies have evaluated sicca symptoms in patients with MCTD. In the first study by Alarcon-Segovia, 12 of the 25 patients reported sicca symptoms. These patients subsequently underwent objective testing for involvement of salivary and lacrimal glands and were all found to have ss based on the presence of three of the following objective findings: Schirmer’s tests; rose bengal staining tests, salivary gland scintiscans, radionuclide excretion studies in saliva, parotid sialographies, and lip biopsies.43 In the second study, Setty et al followed 55 patients with MCTD longitudinally from 1969–2000. The presence of anti-SSA and anti-SSB antibodies was detected in 32.7% and 3.6% of patients, respectively. Interestingly, the presence of antibodies did not correlate to the presence of sicca symptoms, which were noted in 42% of the patients.44 Overall, there are only a handful of case reports in the literature of pSS and MCTD.29,45
Secondary Sjögren’s syndrome and systemic sclerosis
Sicca symptoms in systemic sclerosis are common, and objective evidence of keratoconjunctivitis sicca is found in 55.5%–88% of patients. Minor salivary gland biopsies in these patients have a high rate of fibrosis (80%),46 whereas lymphocytic infiltration of the glands, which is pathogenically characteristic of pSS, is reported in only 4.4% of the biopsies.47 sSS is reported in 14%–20.5% of patients with underlying systemic sclerosis.48–50
Sjögren’s syndrome and other autoimmune diseases
Autoimmune chronic active hepatitis and primary biliary cirrhosis (PBC) have been reported in 2.6%–9% and 1.8%–4%, respectively, of patients with SS.47,51 A retrospective study in Mexico reported rates of SS in 4.8% and 11.9% of patients with autoimmune hepatitis and PBC, respectively.52 A higher prevalence of 35% PBC has been reported in Japan, although this study was limited by a small sample size of 17 patients.53
Hypothyroidism and Grave’s disease is reported in 7%–14% and 1.8%–3%, respectively, of patients with SS.47,54 Patients with one autoimmune disease are generally at a higher risk for developing a second autoimmune disease. This is shown by a retrospective study by Scofield et al in which patients with SLE and a concomitant diagnosis of sSS were noted to have a higher risk of developing autoimmune thyroid disease then SLE patients alone (odds ratio 2.3 [95% CI 1.59–3.36] P<0.001).55
Although antiphospholipid antibodies can be found in up to 13% of patients with pSS, only 1.4% of them fulfill the criteria for antiphospholipid syndrome.27
The prevalence of SS and sarcoidosis ranges from 1%–2%, which is higher than the estimated prevalence of sarcoidosis in the general population. The coexistence of SS and sarcoidosis has been reported in 28/53 patients (53%) whereas, in the remaining 25 (47%) patients, sarcoidosis was found to mimic SS.27 This, however, was reported in a crude analysis of all the published cases of SS and sarcoidosis.56
There is very limited data on the incidence and prevalence of SS with inflammatory muscle disease. The incidence of sSS and polymyositis ranges from 1.8%–14%.47,57 There are case reports of patients with SS and inclusion body myositis who seem to have a better prognosis than patients with inclusion body myositis alone.58,59
The association of SS and anti-neutrophilic cytoplasmic antibodies-associated vasculitides is rare, described in only three cases.27
Immunity
The serological profile of patients with pSS has been reviewed extensively by Bournia VK et al.60 A variety of autoantibodies may be seen in patients with pSS, as summarized below. In general, the presence of autoantibodies correlates with a younger age of onset, female predominance, increased risk of organ involvement, and the presence of other antibodies.
Anti-SSA and anti-SSB antibodies are found in 33%–74% and 23%–52%, respectively, of patients with pSS. Presence of anti-SSA and anti-SSB antibodies is associated with a younger age of onset of pSS and longer disease duration. It also correlates to objective evidence of sicca symptoms and parotid gland damage, ie, decreased salivary flow, worse Schirmer’s test, higher rose bengal staining scores, and higher focus scores on lip biopsy. Patients with anti-SSA and anti-SSB antibodies also have a higher prevalence of extraglandular manifestations of SS such as subcutaneous vasculitis, Raynaud’s phenomenon, peripheral neuropathy, cytopenias, arthritis, renal involvement, and interstitial lung disease.60 In addition to the increased extraglandular manifestations of SS, the presence of anti-SSA antibodies in the mother increases the risk of neonatal lupus and complete heart block in the fetus. The risk is 1%–2% in the first pregnancy and increases significantly to 17% in the subsequent pregnancy if a previous child has been affected.61 Transient manifestations of neonatal lupus syndromes include photosensitivity, subacute cutaneous lupus, cytopenias, hepatosplenomegaly, myocarditis, and pneumonitis.
Up to 59%–85% of patients with pSS are noted to have an elevated ANA titer.60 ANA positivity is associated with a higher prevalence of anti-SSA and anti-SSB antibodies, antiphospholipid antibodies, RF, and hypergammaglobulinemia. The presence of ANA in pSS is associated with a higher risk of cutaneous vasculitis, articular and renal involvement, and higher utilization of corticosteroids.
RF positivity is fairly common, reported in 36%–74% of patients with pSS.60 Anti-cyclic citrullinated peptide antibodies have been reported in 3%–10% of patients with pSS. A prospective Italian study of 141 consecutive patients with pSS patients described positive anti-cyclic citrullinated peptide antibodies in 9.9% (14/141) of patients, and their presence was associated with higher rates of synovitis.62
The prevalence of cryoglobulins in pSS is 9%–15%, the most common type being type III mixed cryoglobulinemia followed by type II mixed cryoglobulinemia.60 pSS patients with cryoglobulinemia are younger and have a higher incidence of parotid gland enlargement, vasculitis, renal involvement, peripheral neuropathy, and lymphoma. The presence of cryoglobulins correlates more specifically with RF positivity, anti-SSA/anti-SSB antibodies, hypocomplementemia, and monoclonal gammopathy.
Antibodies to carbonic anhydrase II are seen in several autoimmune diseases, with prevalence in pSS ranging from 12%–28%.60 Although antibodies to carbonic anhydrase II are not readily available for serological testing, there is indirect evidence to show association with increased risk of distal renal tubular acidosis (RTA), a known complication of pSS. A genetic defect of carbonic anhydrase II can lead to RTA and in vivo studies have shown that induction of antibodies to carbonic anhydrase II causes RTA in mice.60
In their study of 16 patients with pSS compared to age and sex matched controls, Bacman et al demonstrated that immunoglobulin G antibodies present in human sera could bind to and activate muscarinic acetylcholine receptors of the rat parotid gland, confirming that autoantibodies to muscarinic acetylcholine receptors played a pathologic role in the development of pSS.63 The muscarinic acetylcholine receptor is a target for drug development; cevimeline is a specific MR3 agonist used in the treatment of sicca symptoms.
Several novel autoantibodies have been found in patients with SS, including alpha and beta fodrin, islet cell autoantigen, actin, and nuclear mitotic apparatus. Clinical significance of these antibodies is not yet understood and novel antibodies are not available through commercial testing at this time.64 There is increasing interest in identifying markers to help classification of SS. B-cell subset profiling and immune system activation marker assays have been developed and evaluated. Studies so far have not shown that the use of these markers can lead to improvement of the current classification criteria. Further investigation in this area is warranted.65
Lymphoma
An increased risk of non-Hodgkin B-cell lymphoma (NHL) in patients with pSS was first observed in 1978. The significantly elevated risk of developing NHL was estimated at 44 times higher compared to age, race, and sex-matched controls.66 Since then, several studies have published the relative risk (RR) of NHL, with differing results. To answer the question of increased lymphoma risk in patients with pSS, a large meta-analysis of 14 cohort studies investigated the RR of malignancies in 14,524 patients with pSS. This meta-analysis concluded that the overall risk of malignancy is increased with a RR of 1.54 (95% CI 1.17–1.88). pSS was associated with a significantly elevated risk of NHL (RR 13.76; 95% CI 8.53–18.99) and, notably, an increased risk for thyroid cancer (RR 2.58; 95% CI 1.14–4.03). The risk of NHL was notably higher in all geographic areas after adjusting for age and sex. It remains unclear whether the overall risk of malignancy is a direct reflection of the significantly elevated risk of NHL.67
Significant predictors for the development of NHL lymphoma include low complements (C3 and C4), presence of cryoglobulins, low CD4:CD8 ratio, persistence of unilateral or bilateral parotid gland enlargement, splenomegaly, lymphadenopathy, and skin vasculitis.68
Conclusion
SS is one of the more prevalent autoimmune disorders, which can be seen as pSS or sSS in association with an underlying autoimmune disorder. Clinical presentation of SS can vary considerably, ranging from classic sicca symptoms, to mild constitutional symptoms (such as fatigue, malaise, arthralgias), to systemic symptoms (such as neuropathy or vasculitis). Sicca symptoms are nonspecific and may be seen in several medical conditions or as the result of medications or aging, and SS can often present with relatively nonspecific symptoms, thus requiring a high level of suspicion for detection.
Unlike other autoimmune disorders, SS lacks universally accepted classification criteria. Multiple criteria used for diagnosis as well as classification of the disease along with nonspecific symptoms at presentation may lead to under-diagnosis. The lack of standardized criteria also leads to difficulty interpreting epidemiologic studies with a wide range in prevalence, making it challenging to estimate the true incidence and prevalence. Development of universally accepted classification criteria, along with high suspicion of the disease, is essential for appropriate diagnosis and reporting of Sjögren’s syndrome.
Disclosure
The authors report no conflicts of interest in this work.
References
Manthorpe R, Oxholm P, Prause JU, Schiødt M. The Copenhagen criteria for Sjögren’s syndrome. Scand J Rheumatol Suppl. 1986;61:19–21. | |
Vitali C, Bombardieri S, Jonsson R, et al. Classification criteria for Sjögren’s syndrome: a revised version of the European criteria proposed by the American-European Consensus Group. Ann Rheum Dis. 2002;61:554–558. | |
Shiboski SC, Shiboski CH, Criswell L, et al. American College of Rheumatology classification criteria for Sjögren’s syndrome: a data-driven, expert consensus approach in the Sjögren’s International Collaborative Clinical Alliance cohort. Arthritis Care Res (Hoboken). 2012;64:475–487. | |
Baldini C, Talarico R, Tzioufas AG, Bombardieri S. Classification criteria for Sjogren’s syndrome: a critical review. J Autoimmun. 2012;39: 9–14. | |
García-Carrasco M, Ramos-Casals M, Rosas J, et al. Primary Sjögren syndrome: clinical and immunologic disease patterns in a cohort of 400 patients. Medicine (Baltimore). 2002;81:270–280. | |
Alamanos Y, Tsifetaki N, Voulgari PV, Venetsanopoulou AI, Siozos C, Drosos AA. Epidemiology of primary Sjögren’s syndrome in north-west Greece, 1982–2003. Rheumatol Oxf Engl. 2006;45:187–191. | |
Pillemer SR, Matteson EL, Jacobsson LT, et al. Incidence of physician-diagnosed primary Sjögren syndrome in residents of Olmsted County, Minnesota. Mayo Clin Proc. 2001;76:593–599. | |
Plesivcnik Novljan M, Rozman B, Hocevar A, Grmek M, Kveder T, Tomsic M. Incidence of primary Sjogren’s syndrome in Slovenia. Ann Rheum Dis. 2004;63:874–876. | |
Haugen AJ, Peen E, Hultén B, et al. Estimation of the prevalence of primary Sjögren’s syndrome in two age-different community-based populations using two sets of classification criteria: the Hordaland Health Study. Scand J Rheumatol. 2008;37:30–34. | |
Bjerrum KB. Keratoconjunctivitis sicca and primary Sjögren’s syndrome in a Danish population aged 30–60 years. Acta Ophthalmol Scand. 1997;75:281–286. | |
Jacobsson LT, Axell TE, Hansen BU, et al. Dry eyes or mouth – an epidemiological study in Swedish adults, with special reference to primary Sjögren’s syndrome. J Autoimmun. 1989;2:521–527. | |
Birlik M, Akar S, Gurler O, et al. Prevalence of primary Sjogren’s syndrome in Turkey: a population-based epidemiological study. Int J Clin Pract. 2009;63:954–961. | |
Kabasakal Y, Kitapcioglu G, Turk T, et al. The prevalence of Sjögren’s syndrome in adult women. Scand J Rheumatol. 2006;35:379–383. | |
Anagnostopoulos I, Zinzaras E, Alexiou I, et al. The prevalence of rheumatic diseases in central Greece: a population survey. BMC Musculoskelet Disord. 2010;11:98. | |
Dafni UG, Tzioufas AG, Staikos P, Skopouli FN, Moutsopoulos HM. Prevalence of Sjögren’s syndrome in a closed rural community. Ann Rheum Dis. 1997;56:521–525. | |
Tomsic M, Logar D, Grmek M, Perkovic T, Kveder T. Prevalence of Sjögren’s syndrome in Slovenia. Rheumatology (Oxford). 1999;38: 164–170. | |
Bowman SJ, Ibrahim GH, Holmes G, Hamburger J, Ainsworth JR. Estimating the prevalence among Caucasian women of primary Sjögren’s syndrome in two general practices in Birmingham, UK. Scand J Rheumatol. 2004;33:39–43. | |
Thomas E, Hay EM, Hajeer A, Silman AJ. Sjögren’s syndrome: a community-based study of prevalence and impact. Br J Rheumatol. 1998;37:1069–1076. | |
Zhang NZ, Shi CS, Yao QP, et al. Prevalence of primary Sjögren’s syndrome in China. J Rheumatol. 1995;22:659–661. | |
Miyasaka N. [Epidemiology and pathogenesis of Sjögren’s syndrome]. Nihon Rinsho Jpn J Clin Med. 1995;53:2367–2370. Japanese. | |
Hida A, Akahoshi M, Takagi Y, et al. Prevalence of Sjogren syndrome among Nagasaki atomic bomb survivors. Ann Rheum Dis. 2008;67:689–695. | |
Botsios C, Furlan A, Ostuni P, et al. Elderly onset of primary Sjögren’s syndrome: clinical manifestations, serological features and oral/ocular diagnostic tests. Comparison with adult and young onset of the disease in a cohort of 336 Italian patients. Joint Bone Spine. 2011;78:171–174. | |
García-Carrasco M, Cervera R, Rosas J, et al. Primary Sjögren’s syndrome in the elderly: clinical and immunological characteristics. Lupus. 1999;8:20–23. | |
Trontzas PI, Andrianakos AA. Sjogren’s syndrome: a population based study of prevalence in Greece. The ESORDIG study. Ann Rheum Dis. 2005;64:1240–1241. | |
de Souza TR, Silva IH, Carvalho AT, et al. Juvenile Sjögren syndrome: distinctive age, unique findings. Pediatr Dent. 2012;34:427–430. | |
Theander E, Jacobsson LT. Relationship of Sjögren’s syndrome to other connective tissue and autoimmune disorders. Rheum Dis Clin North Am. 2008;34(4):935–947, viii–ix. | |
Ramos-Casals M, Brito-Zerón P, Font J. The overlap of Sjögren’s syndrome with other systemic autoimmune diseases. Semin Arthritis Rheum. 2007;36:246–255. | |
Nossent JC, Swaak AJ. Systemic lupus erythematosus VII: frequency and impact of secondary Sjøgren’s syndrome. Lupus. 1998;7:231–234. | |
Andonopoulos AP, Skopouli FN, Dimou GS, Drosos AA, Moutsopoulos HM. Sjögren’s syndrome in systemic lupus erythematosus. J Rheumatol. 1990;17:201–204. | |
Massardo L, Aguirre V, García ME, et al. Clinical expression of rheumatoid arthritis in Chilean patients. Semin Arthritis Rheum. 1995;25:203–213. | |
Gilboe IM, Kvien TK, Uhlig T, Husby G. Sicca symptoms and secondary Sjögren’s syndrome in systemic lupus erythematosus: comparison with rheumatoid arthritis and correlation with disease variables. Ann Rheum Dis. 2001;60:1103–1109. | |
Pan HF, Ye DQ, Wang Q, et al. Clinical and laboratory profiles of systemic lupus erythematosus associated with Sjögren syndrome in China: a study of 542 patients. Clin Rheumatol. 2008;27:339–343. | |
Manoussakis MN, Georgopoulou C, Zintzaras E, et al. Sjögren’s syndrome associated with systemic lupus erythematosus: clinical and laboratory profiles and comparison with primary Sjögren’s syndrome. Arthritis Rheum. 2004;50:882–891. | |
McDonagh JE, Isenberg DA. Development of additional autoimmune diseases in a population of patients with systemic lupus erythematosus. Ann Rheum Dis. 2000;59:230–232. | |
Ioannidis JP, Tarassi K, Papadopoulos IA, et al. Shared epitopes and rheumatoid arthritis: disease associations in Greece and meta-analysis of Mediterranean European populations. Semin Arthritis Rheum. 2002;31: 361–370. | |
Drosos AA, Lanchbury JS, Panayi GS, Moutsopoulos HM. Rheumatoid arthritis in Greek and British patients. A comparative clinical, radiologic, and serologic study. Arthritis Rheum. 1992;35:745–748. | |
Andonopoulos AP, Drosos AA, Skopouli FN, Acritidis NC, Moutsopoulos HM. Secondary Sjögren’s syndrome in rheumatoid arthritis. J Rheumatol. 1987;14:1098–1103. | |
Carmona L, González-Alvaro I, Balsa A, Angel Belmonte M, Tena X, Sanmartí R. Rheumatoid arthritis in Spain: occurrence of extra-articular manifestations and estimates of disease severity. Ann Rheum Dis. 2003;62:897–900. | |
Cimmino MA, Salvarani C, Macchioni P, et al. Extra-articular manifestations in 587 Italian patients with rheumatoid arthritis. Rheumatol Int. 2000;19:213–217. | |
Uhlig T, Kvien TK, Jensen JL, Axéll T. Sicca symptoms, saliva and tear production, and disease variables in 636 patients with rheumatoid arthritis. Ann Rheum Dis. 1999;58:415–422. | |
Calgüneri M, Ureten K, Akif Oztürk M, et al. Extra-articular manifestations of rheumatoid arthritis: results of a university hospital of 526 patients in Turkey. Clin Exp Rheumatol. 2006;24:305–308. | |
Young A, Dixey J, Cox N, et al. How does functional disability in early rheumatoid arthritis (RA) affect patients and their lives? Results of 5 years of follow-up in 732 patients from the Early RA Study (ERAS). Rheumatology (Oxford). 2000;39:603–611. | |
Alarcon-Segovia D. Symptomatic Sjögren’s syndrome in mixed connective tissue disease. J Rheumatol. 1976;3:191–195. | |
Setty YN, Pittman CB, Mahale AS, Greidinger EL, Hoffman RW. Sicca symptoms and anti-SSA/Ro antibodies are common in mixed connective tissue disease. J Rheumatol. 2002;29:487–489. | |
Wielosz E, Majdan M, Zychowska I, Jeleniewicz R. Coexistence of five autoimmune diseases: diagnostic and therapeutic difficulties. Rheumatol Int. 2008;28:919–923. | |
Alarcón-Segovia D, Ibánez G, Hernández-Ortíz J, Velázquez-Forero F, González-Jiménez Y. Sjögren’s syndrome in progressive systemic sclerosis (scleroderma). Am J Med. 1974;57:78–85. | |
Lazarus MN, Isenberg DA. Development of additional autoimmune diseases in a population of patients with primary Sjögren’s syndrome. Ann Rheum Dis. 2005;64:1062–1064. | |
Avouac J, Sordet C, Depinay C, et al. Systemic sclerosis-associated Sjögren’s syndrome and relationship to the limited cutaneous subtype: results of a prospective study of sicca syndrome in 133 consecutive patients. Arthritis Rheum. 2006;54:2243–2249. | |
Andonopoulos AP, Drosos AA, Skopouli FN, Moutsopoulos HM. Sjögren’s syndrome in rheumatoid arthritis and progressive systemic sclerosis. A comparative study. Clin Exp Rheumatol. 1989;7: 203–205. | |
Drosos AA, Andonopoulos AP, Costopoulos JS, Stavropoulos ED, Papadimitriou CS, Moutsopoulos HM. Sjögren’s syndrome in progressive systemic sclerosis. J Rheumatol. 1988;15:965–968. | |
Lindgren S, Manthorpe R, Eriksson S. Autoimmune liver disease in patients with primary Sjögren’s syndrome. J Hepatol. 1994;20: 354–358. | |
Montaño-Loza AJ, Crispín-Acuña JC, Remes-Troche JM, Uribe M. Abnormal hepatic biochemistries and clinical liver disease in patients with primary Sjögren’s syndrome. Ann Hepatol. 2007;6:150–155. | |
Matsumoto T, Morizane T, Aoki Y, et al. Autoimmune hepatitis in primary Sjogren’s syndrome: pathological study of the livers and labial salivary glands in 17 patients with primary Sjogren’s syndrome. Pathol Int. 2005;55:70–76. | |
Biró E, Szekanecz Z, Czirják L, et al. Association of systemic and thyroid autoimmune diseases. Clin Rheumatol. 2006;25:240–245. | |
Scofield RH, Bruner GR, Harley JB, Namjou B. Autoimmune thyroid disease is associated with a diagnosis of secondary Sjögren’s syndrome in familial systemic lupus. Ann Rheum Dis. 2007;66:410–413. | |
Ramos-Casals M, Brito-Zerón P, García-Carrasco M, Font J. Sarcoidosis or Sjögren syndrome? Clues to defining mimicry or coexistence in 59 cases. Medicine (Baltimore). 2004;83:85–95. | |
Lindvall B, Bengtsson A, Ernerudh J, Eriksson P. Subclinical myositis is common in primary Sjögren’s syndrome and is not related to muscle pain. J Rheumatol. 2002;29:717–725. | |
Derk CT, Vivino FB, Kenyon L, Mandel S. Inclusion body myositis in connective tissue disorders: case report and review of the literature. Clin Rheumatol. 2003;22:324–328. | |
Kanellopoulos P, Baltoyiannis C, Tzioufas AG. Primary Sjögren’s syndrome associated with inclusion body myositis. Rheumatology (Oxford). 2002;41:440–444. | |
Bournia VK, Vlachoyiannopoulos PG. Subgroups of Sjögren syndrome patients according to serological profiles. J Autoimmun. 2012;39: 15–26. | |
Friedman DM, Rupel A, Buyon JP. Epidemiology, etiology, detection, and treatment of autoantibody-associated congenital heart block in neonatal lupus. Curr Rheumatol Rep. 2007;9:101–108. | |
Atzeni F, Sarzi-Puttini P, Lama N, et al. Anti-cyclic citrullinated peptide antibodies in primary Sjögren syndrome may be associated with non-erosive synovitis. Arthritis Res Ther. 2008;10:R51. | |
Bacman S, Sterin-Borda L, Camusso JJ, Arana R, Hubscher O, Borda E. Circulating antibodies against rat parotid gland M3 muscarinic receptors in primary Sjögren’s syndrome. Clin Exp Immunol. 1996;104: 454–459. | |
Routsias JG, Tzioufas AG. Sjögren’s syndrome – study of autoantigens and autoantibodies. Clin Rev Allergy Immunol. 2007;32:238–251. | |
Cornec D, Saraux A, Pers JO, et al. Diagnostic accuracy of blood B-cell subset profiling and autoimmunity markers in Sjögren’s syndrome. Arthritis Res Ther. 2014;16:R15. | |
Kassan SS, Thomas TL, Moutsopoulos HM, et al. Increased risk of lymphoma in sicca syndrome. Ann Intern Med. 1978;89:888–892. | |
Liang Y, Yang Z, Qin B, Zhong R. Primary Sjogren’s syndrome and malignancy risk: a systematic review and meta-analysis. Ann Rheum Dis. Epub May 17, 2013. | |
Theander E, Henriksson G, Ljungberg O, Mandl T, Manthorpe R, Jacobsson LT. Lymphoma and other malignancies in primary Sjögren’s syndrome: a cohort study on cancer incidence and lymphoma predictors. Ann Rheum Dis. 2006;65:796–803. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.