")
Back to Journals » Advances in Medical Education and Practice » Volume 6
The educational environment of the undergraduate medical curriculum at Kuwait University
Authors Karim J, Al-Halabi B, Marwan Y, Sadeq H, Dawas A, Al-Abdulrazzaq D
Received 28 January 2015
Accepted for publication 20 February 2015
Published 7 April 2015 Volume 2015:6 Pages 297—303
DOI https://doi.org/10.2147/AMEP.S81729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Jumanah Karim,1 Becher Al-Halabi,2 Yousef Marwan,3 Hussain Sadeq,4 Ahmed Dawas,5 Dalia Al-Abdulrazzaq5
1Department of Pediatrics, Al-Amiri Hospital, Kuwait City, Kuwait; 2Department of Surgery, Mubarak Al-Kabeer Hospital, Kuwait City, Kuwait; 3Department of Orthopaedic Surgery, Al-Razi Orthopaedic Hospital, Kuwait City, Kuwait; 4Department of Pediatrics, Al-Adan Hospital, Kuwait City, Kuwait; 5Department of Pediatrics, Faculty of Medicine, Health Sciences Center, Kuwait University, Kuwait City, Kuwait
Background: Educational environment of an institution affects the quality of learning. We aim to assess the educational environment of the undergraduate curriculum of Faculty of Medicine, Kuwait University (FOMKU).
Methods: A cross-sectional study was carried out during April 2014. The validated Dundee Ready Education Environment Measure (DREEM) questionnaire was e-mailed to 607 students. Mean scores of the main domains of the questionnaire, and for each item, were calculated, and their association with the students’ background information was measured using Student’s t-test (P-value of ≤0.05 was considered as the cut-off level of significance).
Results: Of 607 students, 117 (19.3%) completed the questionnaire. The total mean score for DREEM was 108.7/200 (54.3%). The mean score for students’ perception of teaching, perception of teachers, academic self-perception, perception of atmosphere, and social self-perception were 25.2/48 (52.5%), 24.6/44 (55.9%), 18.4/32 (57.5%), 26.2/48 (54.5%), and 14.3/28 (51.0%), respectively. The highest mean score for an item of DREEM questionnaire was for “my accommodation is pleasant” (3.48±0.75), while the lowest was for “there is a good support system for students who get stressed” (0.88±0.86). The total mean score was not significantly different between the two phases of the curriculum, or among males and females; however, few significant differences among the main domains and items were noted.
Conclusion: Based on the learners’ perspectives, the educational environment of FOMKU, was suboptimal. Medical educators in Kuwait should improve this environment in order to advance the quality of the delivered curriculum.
Keywords: medical education, undergraduate, medical students, environment, learning, teaching
Introduction
The quality of undergraduate medical education is affected by several factors; one of the most important determinants of an effective undergraduate medical curriculum is its educational environment.1–3 The academic quality of any medical school/institution is reflected by its educational environment.1–5 Therefore, several tools were developed to assess the educational environment of learners.6–11 Assessing the medical educational environment provides medical educators with a comprehensive view of the delivered curriculum.4,5
The undergraduate medical curriculum of the Faculty of Medicine, Kuwait University (FOMKU) is currently made up of three phases (I–III). Phase I (1 year) is a preprofessional program consisting of language and sciences courses. Phase II (3 years) consists of system courses that use a variety of methods including a series of problem-based learning cases, self-learning activities, didactic lectures, tutorials, laboratory exercises, and hospital visits aimed at stimulating active learning. The Faculty aims at promoting professional and behavioral development through the early introduction of students to the hospital environment at this phase. Phase III (3 years) is a clinical phase consisting of student clerkships through Medicine, Surgery, Community Medicine, Pediatrics, Obstetrics and Gynecology, and Psychiatry. This phase ends up with a preinternship program that aims at transitioning medical students to being practicing physicians.
During the past decade, the FOMKU had adopted a system based on case-triggered integrated curriculum for student intake. Previous studies revealed that changes in the curriculum are stressful on both the students and teachers, thus affecting the learning environment.6,12 To ensure successful implementation of a new curriculum, evaluation of the change should be done periodically. Medical educators of FOMKU attempted to evaluate and improve the new curriculum; however, a proper assessment of the educational environment of the new curriculum was not done before.13–17 Because the students’ achievements, satisfaction, and success can be affected by a change in the educational environment, an assessment of the curriculum’s environment is a must to ensure the delivery of high-quality teaching.1,4,18,19
By conducting this study, we aim to provide an assessment of the educational environment of the new undergraduate medical curriculum at the FOMKU. We also plan to investigate if this environment varies between the three phases of the curriculum.
Subjects and methods
This cross-sectional study was conducted during April 2014, involving medical students at FOMKU. The Arabic version of the 50-item Dundee Ready Education Environment Measure (DREEM) questionnaire was used to assess the education environment in this study. This version was translated by the Centre for Medical Education of the University of Dundee and English Language Centre of Umm Al-Qura University.6,20,21 The DREEM inventory is composed of five subscales. These are perceptions of teaching/learning (12 items), perceptions of teaching (eleven items), academic self-perceptions (eight items), perceptions of atmosphere (12 items), and social self-perceptions (seven items). The items of DREEM were scored from 0 to 4 (0= strongly disagree; 1= disagree; 2= unsure; 3= agree; 4= strongly agree), except for nine negative items (numbers 4, 8, 9, 17, 25, 35, 39, 48, and 50) which were scored in reverse. A maximum possible score of DREEM is 200. Data on the students’ age, sex, year of study, and grade point average were also collected during the study.
The questionnaire was forwarded to the students through their university e-mails, and they were given 2 weeks to complete the questionnaire. Remainder e-mails were sent every third day. Phase II and III medical students were invited to participate in the study (total of 607 students); Phase I students were excluded from the study as they are at the preprofessional program, which included students of all health sciences studies (Medicine, Pharmacy, Dentistry, and Allied health).
This study was ethically approved by the Committee for The Protection of Human Subjects in Research of the Health Sciences Centre. The objectives of the study were explained to the students in the invitation e-mail. Their consents were taken, and it was made clear to them that the participation in the study was optional and there was no harm if they declined to participate. The name or any other information that might identify the participant identity was not obtained, ensuring confidentiality of the data.
The Statistical Package for Social Sciences Version 17.0 (SPSS Inc., Chicago, IL, USA) was used to analyze the collected data. Descriptive data, including frequencies, percentages, means, and standard deviations, of the variables were calculated. The association between qualitative and quantitative variables was assessed using the Student’s t-test. A cut-off level for statistical significance using a P-value level of <0.05 was considered. The internal consistency of the Arabic translation of DREEM was assessed by measuring the Cronbach’s alpha.
Results
Of the 607 students who were invited to participate in the study, 117 (19.3%) completed the questionnaire. Table 1 demonstrates the personal and academic characteristics of the students. The age of most of the participants was between 21 years and 22 years (44, 37.6%), ranging from 18 years to 27 years. Sixty-six (56.4%) students were females. A large number of the participants had a grade point average between 2.50 and 2.99 out of 4.00 (39.3%), while only eight (6.80%) had a grade point average more than 3.49. Sixty-two (53.0%) students were in Phase II of the curriculum.
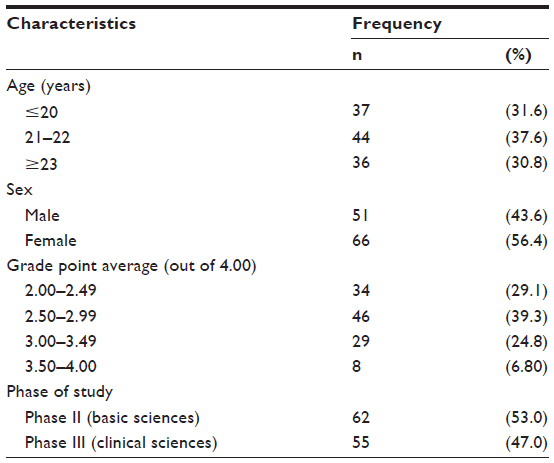 | Table 1 Characteristics of participating students (n=117) |
Tables 2 and 3 show the mean scores of each of the main domains and specific items of the DREEM questionnaire. The tables also demonstrate the association between these domains and items, and the students’ sex and phase of undergraduate medical curriculum. The mean scores for students’ perception of teaching, perception of teachers, academic self-perception, perception of atmosphere, and social self-perception were 25.2/48 (52.5%), 24.6/44 (55.9%), 18.4/32 (57.5%), 26.2/48 (54.5%), and 14.3/28 (51.0%), respectively. The highest mean score for an item of the DREEM questionnaire was for “my accommodation is pleasant” (3.48±0.75), while the lowest score was for “there is a good support system for students who get stressed” (0.88±0.86). The total mean score for DREEM was 108.7/200 (54.3%). Students in their Phase III of the curriculum reported a statistically significant higher mean score for academic self-perception (P=0.047) and social self-perception (P=0.045). Moreover, the mean score for the students’ social self-perception was significantly higher (P=0.026) among male students (15.3±4.00) compared to female students (13.6±3.86). Nevertheless, the total mean score was not significantly different between the two phases of the undergraduate medical curriculum, or male and female students. Significant differences of a few items of the educational environment between students in different phases of the medical curriculum, with sex differences are demonstrated in Tables 2 and 3. Cronbach’s alpha was 0.91 for the entire inventory.
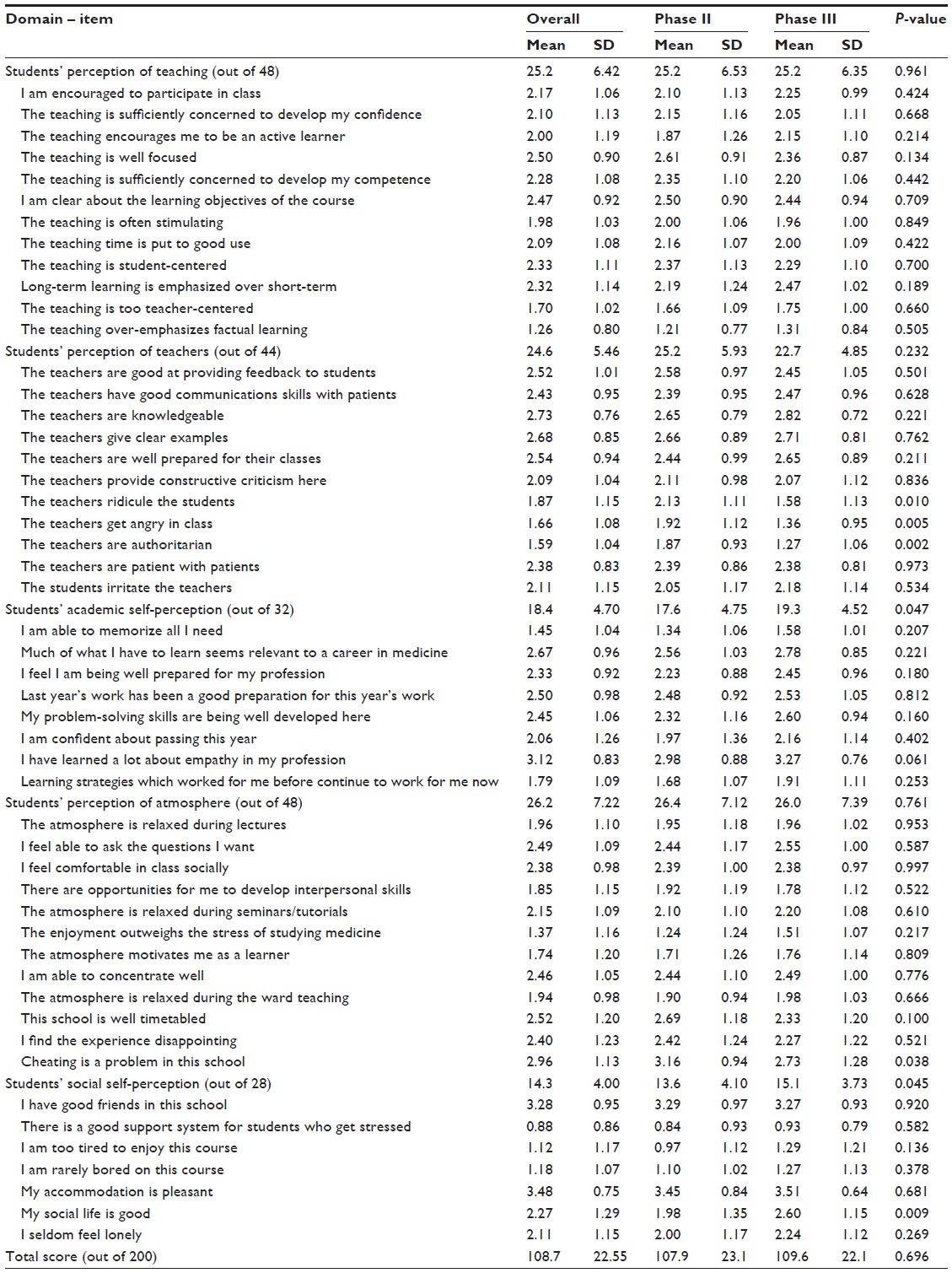 | Table 2 Mean Dundee Ready Education Environment Measure score per domain/item according to the phase of the undergraduate study |
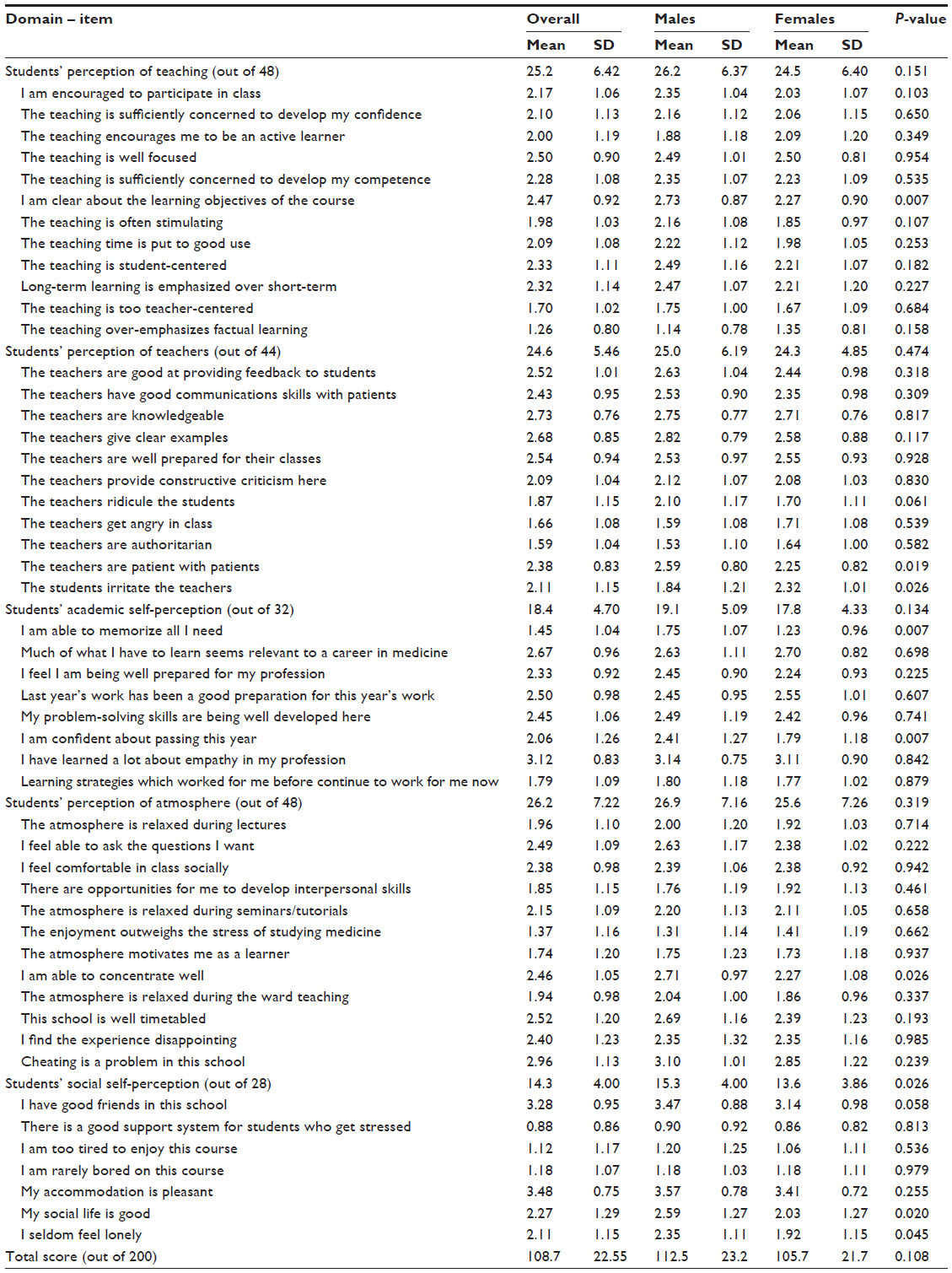 | Table 3 Mean Dundee Ready Education Environment Measure score per domain/item according to sex of the participants |
Discussion
This study provides an analysis of the strengths and weaknesses of the educational environment of the FOMKU using the DREEM questionnaire. Because the quality of the educational environment of an institution affects the effectiveness of the delivered curriculum, the findings of this study are important for the development of medical education curricula in Kuwait.1–3 Moreover, the internal consistency of the Arabic translation of DREEM inventory was excellent, meaning that the items of the questionnaire measure the same concept appropriately.
It was found that the overall mean score of the educational environment and the individual domains’ scores were around 50% of the possible maximum score, indicating that the current educational environment is suboptimal. Students’ perceptions of their academic achievements (ie, students’ academic self-perception) received the highest score out of the maximum possible score. These perceptions are comparable to other medical students worldwide.6,7,20–30 The total score of DREEM ranged approximately between 45.0% and 69.5% worldwide. The score of the FOMKU is very close to the scores of medical schools of the Middle East;20,21,24,27 whereas, it was lower than medical schools in the other parts of the world such as Dundee, Chile, Malaysia, and Nepal.6,7,23,25,26,28,29 This difference between schools of our region and schools of different regions is most likely because universities of the Middle East are more recently established, with less experience in teaching and other scholarly activities. The main domains of the educational environment varied between schools.6,7,20–30 In our study, students of Phase III of the curriculum reported a slightly better educational environment (not statistically significant) compared to students of Phase II. Such a finding is likely because our students enjoy studying clinical subjects more than basic sciences. This finding is different to what was found in other studies.29–31 Moreover, the number of the items of the DREEM questionnaire that were significantly different between males and females were comparable to Dundee students and less than Saudi students.20 Nevertheless, the mean scores of these items were generally better among male students, similar to Saudi students and in contrast to Dundee students. This indicates that medical schools of Kuwait and Saudi Arabia provide a better educational environment for male students than female students, while the opposite was provided by Dundee University. There is no clear explanation for this finding. Medical educators in our institutions should investigate the reasons for such differences in order to ensure the presence of appropriate learning environments.
Although this study provided important data regarding the educational environment of the FOMKU, it has a few limitations. The response rate was less than 25%, which could have led to results that were not representative of all students. In addition, the reliability of the Arabic translation of the DREEM questionnaire, which was used in this study, has not been assessed before. There are no data about the educational environment of the old curriculum of this school. Therefore, studying the effect of the new curriculum on the educational environment at FOMKU is challenging.
Conclusion
In conclusion, the educational environment of the FOMKU was suboptimal based on the learners’ perspectives. Medical educators in Kuwait should invest on improving this environment in order to improve the quality of the delivered medical education curriculum.
Disclosure
The authors report no conflicts of interest in this work.
References
Genn JM. AMEE Medical Education Guide No 23 (Part 1): curriculum, environment, climate, quality and change in medical education – a unifying perspective. Med Teach. 2001;23(4):337–344. | |
Genn JM. AMEE Medical Education Guide No 23 (Part 2): curriculum, environment, climate, quality and change in medical education – a unifying perspective. Med Teach. 2001;23(5):445–454. | |
Hutchinson L. The ABC of learning and teaching: educational environment. BMJ. 2003;326:810–812. | |
Roff S, McAleer S. What is educational climate? Med Teach. 2001; 23(4):333–334. | |
Genn JM, Harden RM. What is medical education here really like? Suggestions for action research studies of climates of medical education environments. Med Teach. 1986;8(2):111–124. | |
Roff S, McAleer S, Harden RM, et al. Development and validation of the Dundee ready education environment measure (DREEM). Med Teach. 1997;19:295–299. | |
Roff S, McAleer S, Ifere OS, Bhattacharya S. A global diagnostic tool for measuring educational environment: comparing Nigeria and Nepal. Med Teach. 2001;23(4):378–382. | |
Roff S, McAleer S, Skinner A. Development and validation of an instrument to measure the postgraduate clinical learning and teaching educational environment for hospital-based junior doctors in the UK. Med Teach. 2005;27(4):326–331. | |
Holt MC, Roff S. Development and validation of the anesthetic theatre educational environment measure (ATEEM). Med Teach. 2004;26(6):553–558. | |
Cassar K. Development of an instrument to measure the surgical operating theatre learning environment as perceived by basic surgical trainees. Med Teach. 2004;26(3):260–264. | |
Mulrooney A. Development of an instrument to measure the practice vocational training environment in Ireland. Med Teach. 2005;27(4):338–342. | |
McAleer S, Roff S, Harden RM, McAleer S, Roff S, Harden RM. The medical education environment measure: a diagnostic tool. Med Educ. 1997;32:209–221. | |
Karim J, Al-Saraji M, Al-Mousawi F, et al. Knowledge and self-reported practice of universal precautions among Kuwait University medical students in their clinical years. Med Princ Pract. 2012;21:328–333. | |
Marwan Y, Al-Saddique M, Hassan A, Karim J, Al-Saleh M. Are medical students accepted by patients in teaching hospitals? Med Educ Online. 2012;17:17172. | |
Karim JA, Marwan YA, Dawas AM, Akhtar S. Self-confidence of medical students in performing clinical skills acquired during their surgical rotation: assessing clinical skills education in Kuwait. Saudi Med J. 2012;33:1310–1316. | |
Almutar S, Altourah L, Sadeq H, Karim J, Marwan Y. Medical and surgical ward rounds in teaching hospitals of Kuwait University: students’ perceptions. Adv Med Educ Pract. 2013;4:189–193. | |
Qadan L, Al-Ozairi E, Ayed A, Huang G. Avoiding honest feedback: discordance between formal evaluations and candid assessments of Kuwaiti PBL students. Med Teach. 2013;35(6):459–464. | |
Cavanaugh S, Simmons P. Evaluation of a school climate instrument for assessing affective objectives in health professional education. Eval Health Prof. 1997;20(4):455–478. | |
Primparyon P, Roff S, McAleer S, Pemba S. Educational environment, student approaches to learning and academic achievement in a Thai nursing school. Med Teach. 2000;22:359–364. | |
Al-Hazimi A, Zaini R, Al-Hyiani A, et al. Educational environment in traditional and innovative medical schools: a study in four undergraduate medical schools. Educ Health (Abingdon). 2004;17(2):192–203. | |
Al-Hazimi A, Al-Hyiani A, Roff S. Perceptions of the educational environment of the medical school in King Abdul Aziz University, Saudi Arabia. Med Teach. 2004;26(6):570–573. | |
Till H. Identifying the perceived weaknesses of a new curriculum by means of the Dundee ready education environment measure (DREEM) inventory. Med Teach. 2004;26(1):39–45. | |
Bassaw B, Roff S, McAleer S, et al. Students’ perspectives on the educational environment, Faculty of Medical Sciences, Trinidad. Med Teach. 2003;25(5):522–526. | |
Al-Ayed IH, Sheik SA. Assessment of the educational environment at the College of Medicine of King Saud University, Riyadh. East Mediterr Health J. 2008;14(4):953–959. | |
Riquelme A, Oporto M, Oporto J, et al. Measuring students’ perceptions of the educational climate of the new curriculum at the Pontificia Universidad Católica de Chile: performance of the Spanish translation of the Dundee ready education environment measure (DREEM). Educ Health (Abingdon). 2009;22(1):112. | |
Pierre RB, Branday JM, Pottinger A, Wierenga A. Students’ perception of the ‘educational climate’ at the Faculty of Medical Sciences, The University of the West Indies, Jamaica. West Indian Med J. 2010;59(1):45–49. | |
Aghamolaei T, Fazel I. Medical students’ perceptions of the educational environment at an Iranian Medical Sciences University. BMC Med Educ. 2010;10:87. | |
Arzuman H, Yusoff MS, Chit SP. Big Sib students’ perceptions of the educational environment at the school of medical sciences, Universiti Sains Malaysia, using Dundee ready educational environment measure (DREEM) inventory. Malays J Med Sci. 2010;17(3):40–47. | |
Jiffry MT, McAleer S, Fernando S, Marasinghe RB. Using the DREEM questionnaire to gather baseline information on an evolving medical school in Sri Lanka. Med Teach. 2005;27(4):348–352. | |
Demirören M, Palaoglu O, Kemahli S, Ozyurda F, Ayhan IH. Perceptions of students in different phases of medical education of educational environment: Ankara University Faculty of Medicine. Med Educ Online. 2008;13:8. | |
Abraham R, Ramnarayan K, Vinod P, Torke S. Students’ perceptions of learning environment in an Indian medical school. BMC Med Educ. 2008;8:20. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.