")
Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 5
Targeting CD20 in chronic lymphocytic leukemia
Received 21 November 2014
Accepted for publication 13 January 2015
Published 10 March 2015 Volume 2015:5 Pages 43—53
DOI https://doi.org/10.2147/BLCTT.S55823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor David Dingli
Myrna R Nahas, Jon E Arnason
Beth Israel Deaconess Medical Center, Boston, MA, USA
Abstract: Chronic lymphocytic leukemia (CLL), the most common leukemia in adults, is standardly managed with chemotherapy in combination with the anti-CD20 antibody rituximab. In this review, we discuss the history, use, and evolution of rituximab in the treatment of CLL and explore the next generation CD20 antibodies ofatumumab and obinutuzumab with a focus on recent clinical trials. Increased understanding of the importance of B cell receptor (BCR) signaling in CLL has resulted in the development of several drugs with significant clinical activity that are ideally suited for combination with CD20 therapy as is being currently explored. Moving forward, these developments have the potential to result in treatment regimens that do not include traditional chemotherapeutic agents, which is of particular importance in CLL given the late onset of diagnosis and potential frailty of the patients.
Keywords: CLL, monoclonal antibody, rituximab, ofatumumab, obinutuzumab
Introduction
Chronic lymphocytic leukemia (CLL), the most prevalent adult leukemia, is a complex hematologic condition with great phenotypic heterogeneity, ranging from an indolent to a rapidly progressive disease. The malignant, nonfunctional B cells proliferate not only in the peripheral blood, but also within compartments found in lymph nodes, the bone marrow, liver, and spleen.1 In terms of genetic factors, patients with an unmutated immunoglobulin heavy chain (IGHV), mutations in TP53, mutations in chromosome 11 including the 11q deletion (ATM abnormalities), and the 17p deletion each portend poor prognosis, making effective treatment of these subgroups particularly challenging.2,3 Despite the variance in disease trajectory, there lies no definitive cure for CLL short of an allogeneic bone marrow stem cell transplant, which is only considered for select patients.4
For over four decades, CLL had been managed with chlorambucil, a nitrogen mustard alkylating agent, which did not affect overall survival (OS) and had a modest complete response rate (CRR).5 However, chlorambucil still remains an attractive agent for frail elderly patients given its oral formulation and overall low toxicity profile despite the increased risk of secondary malignancies.6 At the turn of the decade, the concept of immunotherapy to treat CLL was introduced secondary to significant improvements in the understanding of the biology of the disease. The addition of the chimeric monoclonal CD20 antibody, rituximab, to chemotherapeutic agents has revolutionized CLL treatment by improving OS. Since the advent of rituximab, next generation anti-CD20 antibodies remain on the forefront of the pharmaceutical armamentarium (Table 1). This review will focus on the history and present state of utilizing anti-CD20 therapies in the management of CLL as well as future pharmacologic directions.
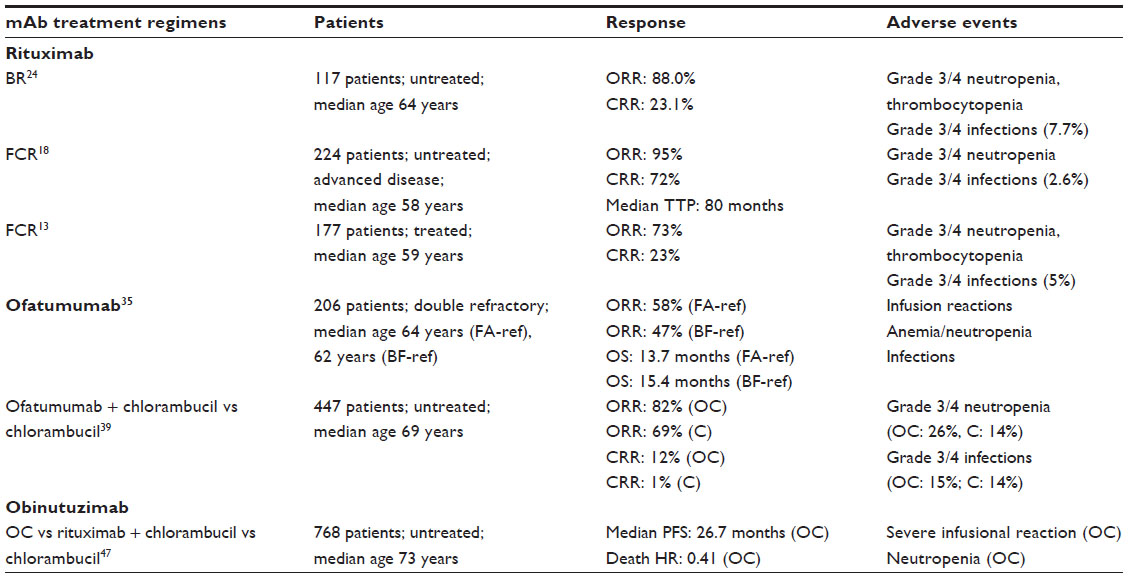 | Table 1 A summary of the key clinical studies describing the effects of targeting CD20 with rituximab, ofatumumab, and obinutuzumab |
Rituximab and targeting of CD20
By the 1990s, it was well-established that the combination of the purine analog, fludarabine, and alkylating agent, cyclophosphamide, was superior to monotherapy alone in the management of CLL.5 However, data on the addition of immunotherapy to a purely chemotherapeutic regimen had not been thoroughly investigated on a clinical basis.
CD20 is a cell surface protein expressed on B cells at most stages of development. However, CD20 is only weakly expressed on the surface of CLL cells.7 CD20, which contains both an N and C terminus within the cell, is a member of the MS4A protein group.8–10 CD20 is comprised of two extracellular loops, of which the larger component is made up of 44 amino acids. Rituximab was the first mouse–human chimeric antibody clinically developed to target CD20 and acts through multiple different mechanisms, including complement-mediated cytotoxicity (CDC), antibody-dependent cytotoxicity (ADCC), and direct toxicity.11,12 Rituximab binds to the larger extracellular loop of CD20. It has been shown that rituximab specifically recognizes epitopes containing the two amino acids alanine and proline, which facilitate its binding.9
From a pathogenic perspective, immunotherapy with rituximab functions synergistically with chemotherapy in targeting CLL malignant cells. One postulated mechanism lies in the fact that CDC by rituximab is facilitated in the presence of fludarabine’s downregulation of the complement-resistance CLL proteins CD46, CD55, and CD59.13 Additionally, it has been shown that CD20 is not internalized, downregulated, or shed after the binding of rituximab.14 However, one resistance mechanism that has been elucidated is that CD20 is ‘shaved’ from the surface of CLL cells following mAb exposure.14 The postulated mechanism appears to involve the removal of the rituximab–CD20 complex by FcR-expressing effectors, including Kupffer cells.9 Notably, rituximab as compared to alemtuzumab, an anti-CD52 mAb, promotes less CDC because B cells express less CD20 than CD52 on their surface; however, alemtuzumab has a worse toxicity profile. Thus, rituximab is in general utilized preferentially over alemtuzumab, which is reserved for select patients.15
In the late 1990s to early 2000s, there were a number of small Phase II trials utilizing weekly low-dose rituximab for refractory small lymphocytic lymphoma (SLL)/CLL.16 Overall, the results of these rituximab-monotherapy studies showed response rates inferior to those seen in other non-Hodgkin lymphoma subtypes possibly due to comparatively lower CD20 expression on CLL.16,17 In fact, follicular lymphoma has a much higher CD20 antigen density of about 90,000 molecules/cell compared to approximately 8,000–15,000 molecules/cell in CLL.14 Due to the poor single-agent activity and strong rationale for combination therapy, rituximab in CLL has been used as an adjuvant to chemotherapeutic agents.
In June 2005, two publications in the Journal of Clinical Oncology (JCO) demonstrated the clear clinical adjunctive benefit of incorporating rituximab into CLL chemotherapeutic regimens in both treatment-naïve and previously treated patients. Keating et al18 conducted a large single-arm study of fludarabine, cyclophosphamide, and rituximab (FCR) in 224 untreated, advanced-stage CLL patients with a median age of 58 years. The overall response rate (ORR) was 95% with a high CRR of 70% in this patient population and a time-to-treatment failure analysis predicted a sustained response at 4 years in 69% of subjects.18 The 6-year results in the final cohort of 300 patients were fairly similar, with an ORR of 95%, a CRR of 72%, and a median time to progression of 80 months.19 A smaller study utilizing FCR in 177 previously treated CLL patients resulted in an ORR of 73%, with a CRR of 23%. The most common toxicity was bone marrow suppression, but the regimen was well-tolerated overall.13
In 2010, FCR became the standard treatment regimen for untreated CLL patients based on the initial results of a multicenter, international randomized Phase III trial of the German CLL Study Group (GCLLSG), the CLL8 Protocol, comparing FC to FCR in 817 physically fit, treatment-naïve patients showing improved OS (83% vs 87%, P=0.01) and progression-free survival (PFS) (45% vs 65%, P<0.0001).20 Indeed, this was the first study to show improved OS in newly diagnosed CLL patients. Extended follow-up results of the CLL8 Protocol at 5.9 years showed statistically significant improved PFS in all Binet stages as well as improved disease-free progression (hazard ratio [HR]: 0.6, P<0.0001) in the FCR arm compared to the FC arm. Notably, the incidence of secondary malignancies was fairly similar in both arms, at 9.9% (FCR arm) and 12.1% (FC arm). The FCR arm, did however, have an increased incidence of prolonged neutropenia, which can last up to 2 years after discontinuing therapy.21 For previously treated patients, the REACH study (Rituximab in the Study of Relapsed Chronic Lymphocytic Leukemia) was a large randomized trial of 552 subjects comparing FCR to FC. This study established precedence in utilizing FCR over FC for previously treated patients given improvements in median PFS (30.6 months vs 20.6 months, P<0.001), event-free survival (EFS), response rate, CRR, duration of response, and time to new CLL treatment or death.22
It is interesting to note that there is evidence that patients with IGHV mutated CLL benefit more from FCR than unmutated patients.23 Given the fact that the FCR trials were conducted in ‘physically fit’ patients and that CLL is primarily a disease of elderly patients, who are often less fit and with multiple comorbidities, the GCLLSG conducted the Phase II CLL2M trial, assessing the efficacy of combining bendamustine with rituximab (BR) in previously untreated CLL patients irrespective of fitness or age.24 More specifically, 117 patients from 40 centers in Germany participated in the study with a median age of 64 years and 35.0% of subjects with a creatinine clearance of <70 mL/minute. The ORR was 88.0%, with a CRR of 23.7%, and a median EFS of 33.9 months; the subgroup with 17p deletion did not respond well. Based on the above, BR is another reasonable therapeutic strategy for treatment-naïve patients not harboring the 17p deletion.4,24 Although promising results have been reaped from FCR, as patients increase in age, especially those >70 years, the tolerability of FCR decreases, making it a less ideal regimen for the elderly.25
For elderly or unfit patients, the combination of chlorambucil and rituximab has been recently investigated given that both agents alone are well-tolerated by these populations. Laurenti et al conducted a small study of 27 elderly or unfit patients published in 2013. The specific regimen administered was chlorambucil in eight 28-day cycles adjunctive with rituximab dosed at 375 mg/m2 for cycle one and 500 mg/m2 for the remaining cycles. The ORR was 74% with grade 3 or 4 neutropenia occurring in 18.5% of subjects.26 In 2014, Foà et al published the results of a Phase II trial comparing chlorambucil and rituximab as first-line induction treatment with or without rituximab as maintenance for elderly CLL patients.27 The regimen in this trial included chlorambucil in eight 28-day cycles and rituximab dosed at 375 mg/m2 on C3 and 500 mg/m2 for cycles four to eight. Subsequently, those who responded to this regimen were then randomized to twelve 8-week doses of rituximab versus observation. Eighty-five patients received at least one dose of rituximab in the induction phase and the ORR was 82.4% (95% confidence interval [CI]: 74.25%–90.46%). From the responders, 34 patients were randomized to rituximab maintenance and 32 patients to observation only. The ORR for the maintenance group was 55.9% (95% CI: 39.19%–72.57%) versus 34.4% (95% CI: 17.92%–50.83%) in the observation-only group, with a P-value of 0.079. Neutropenia occurred in one-third of patients in the induction period and grade 3 or 4 infections occurred in only 1% of patients. In further analysis, it appears that rituximab maintenance may be more effective in patients achieving at least a partial remission (PR) after induction as well as those with unmutated IGHV status.27 Finally, Hillmen et al28 published Phase II trial results of chlorambucil and rituximab in elderly patients in the March 2014 issue of JCO.28 In this study, 100 patients with a median age of 70 years and a median of seven comorbidities were treated with the combination regimen. The ORR was 84% (95% CI: 75.3%–90.6%) with a CR attained in 10% of patients. The median PFS was 23.5 months (95% CI: 16.4–25.8 months) and the median OS was not reached at 30 months of follow-up. Neutropenia/lymphopenia occurred in 41% of the subjects and neutropenic sepsis in 4%. In this study, there was a trend for a better ORR in patients with trisomy 12q, but interestingly, IGHV status did not affect the ORR.28 Based on these investigational studies, the combination of chlorambucil with rituximab may be a reasonable regimen for the elderly or unfit CLL subgroup.
In summary, the use of adjunctive rituximab with chemotherapy as opposed to rituximab monotherapy has been shown to modestly improve both OS and PFS in CLL patients, especially those who are more fit; however, this treatment paradigm is not curative and ultimately, for the majority of patients, the disease will recur.
Ofatumumab
In 2009, the US Food and Drug Administration (FDA) approved the use of the second-generation type I monoclonal CD20 antibody, ofatumumab, in CLL cases refractory to fludarabine and alemtuzumab.14 Ofatumumab differs from rituximab in that it binds to a different CD20 epitope, affording improved CDC.30,31 CDC of B cells occurs via the complement classical pathway (CP). Activation of the CP occurs when C1q binds to IgG bound to the B cell surface. It has been shown in preclinical models that ofatumumab binds more strongly to C1q than does rituximab.32 CDC activity is also enhanced when the distance between the CLL cell’s plasma membrane and the constant region of the mAb is smallest.9,33 Ofatumumab binds to a more proximal epitope than does rituximab, thereby facilitating complement activity and increased cell lysis.14,33 Additionally, ofatumumab has a slower off-rate and binds more stably to CD20; thus, it is efficacious in cells with low CD20 expression relative to rituximab.30 Moreover, ofatumumab has a low rate of human anti-human antibody (HAHA) formation.34
The first infusional dose-escalating Phase I/II trial of ofatumumab, published in 2008, was conducted in 33 patients with relapsed or refractory CLL. The results revealed either a PR or nodular PR in 50% of the Phase II patients. The median duration of response was 3.7 months and the median time to requiring next-line CLL therapy was 12 months. When compared to previously published rituximab trials with a similar patient population, these results were overall more impressive.30
In 2010, Wierda et al led an international, multicenter trial in 206 double-refractory CLL patients, specifically 95 patients with fludarabine/alemtuzumab-refractory (FA-ref) disease and 111 patients with bulky lymphadenopathy >5 cm (BF-ref).35 Patients received eight weekly infusions of ofatumumab followed by four monthly infusions during a 24-week period. The final analysis showed an ORR of 51% with a complete response (CR) in two patients from the BF-ref cohort. The duration of response was 5.7 months in the FA-ref cohort and 6.0 months in the BF-ref cohort. The most prevalent side effects included infusion reactions (ie, rigors, rash, fever, fatigue, increased sweating, urticaria), especially with the first two doses, and infections, both of which were mainly grade 1 or 2 events.14,35 In an ad hoc retrospective analysis of the trial, it was found the patients previously treated with rituximab still gained benefit with ofatumumab, with similar ORRs, PFS, and OS. For rituximab-treated, rituximab-refractory, and rituximab-naïve patients, the respective ORRs were 43%, 44%, 53%, the median PFS were 5.3, 5.5, and 5.6 months, and the median OS were 15.5, 15.5, and 20.2 months.36,37
Similar to rituximab, ofatumumab has also been investigated as an adjunct to chemotherapy. Wierda et al36 conducted the BIFROST study, a Phase II trial studying 61 previously untreated CLL patients divided into two cohorts, each with a different dose of ofatumumab (500 mg or 1,000 mg), combined with fludarabine and cyclophosphamide (O-FC) for six cycles. The CR rate was 32% for the lower dose O-FC arm and 50% for the higher dose arm; the ORR was 77% (low dose) and 73% (high dose). Although these results are not as promising as that seen with FCR, many of the patients were high risk with an elevated B2-microglobulin. In addition, 52% of the patients in the 500 mg ofatumumab arm and 30% in the 1,000 mg ofatumumab arm had unmutated IGHV and 6% of the patients in the 500 mg ofatumumab arm harbored the 17p deletion compared to 20% in the opposing arm.36,38 The preliminary results of the Phase III COMPLEMENT trial investigated ofatumumab–chlorambucil versus chlorambucil monotherapy in previously untreated patients with CLL in patients with comorbidities or advanced age preventing the use of fludarabine. The ofatumumab–chlorambucil arm had greater ORR (82% vs 69%, P=0.001), CR rate (12% vs 1%), and median PFS (22.4 vs 13.1 months, P<0.001); however, there has not been improvement in OS reported to date.39
Moreover, the Phase II, open-label, multicenter GIMEMA (Gruppo Italiano Malattie EMatologiche dell’Adulto) study (CLL0809) was conducted to investigate the addition of ofatumumab to bendamustine in 47 patients with relapsed/refractory CLL, with about one-third of the subjects over the age of 70 years. More specifically, 22% of the patients had TP53 mutations and 65% were of unmutated IGHV status. Additionally, three-quarters of the patients had previously received fludarabine-based chemotherapy and about half had previously received treatment with rituximab. This trial also studied mutations in genes, including NOTCH1, SF3B1, and BIRC3, all implicated in worse CLL outcomes. After six cycles of treatment, the ORR was 72.3% (95% CI: 57%–84%) of which 17% were a CR. Most notably, the response rate was not dependent on the following: IGHV status, 11q deletion, NOTCH1 mutations, BIRC3 mutations, age older than 70 years, prior exposure to fludarabine and/or rituximab, and number of previous therapies. However, those with the 17p deletion or TP53 mutations had a markedly lower ORR of 30%. The multivariate analysis had statistically worse ORR in patients with both the TP53 mutation and lymph nodes >5 cm. The most common side effect of the treatment regimen was bone marrow suppression. Of clinical significance, 61.7% of patients had grade 3 or 4 neutropenia, which is higher than that seen with the BR combination, but similar to that of the FCR regimen. Of the 61.7%, grade 3 infections occurred in only 6% of the patients.29
Recently, the addition of lenalidomide to ofatumumab was studied in a Phase II trial of 21 subjects with advanced, relapsed, and refractory disease. Eighty-six percent of the patients had unmutated IGHV and 29% had the 17p deletion. Mechanistically, lenalidomide, an immunomodulatory chemotherapeutic agent, activates immune effector natural killer (NK) and T cells, thereby promoting both NK and monocyte-mediated ADCC CLL toxicity by ofatumumab.34 Additionally, lenalidomide inhibits T regulatory cells and it has been demonstrated that it improves T-cell synapse formation with CLL.4,40 The study regimen was 2,000 mg ofatumumab intravenously (IV) on day 1, with 10 mg lenalidomide on days 8–28 for six cycles as tolerated. Not surprisingly, the most common dose-limiting side effect was bone marrow suppression manifested as neutropenia and thrombocytopenia. In addition, a tumor flare reaction (TFR) defined as the acute painful enlargement of CLL-involved lymph nodes, increased lactate dehydrogenase, and a lymphocytosis, was experienced by nearly half of the patients in this study. The TFR was treated with steroids and this adverse event did not require any dose reductions in any of the participating subjects. There was a 53% partial response rate, less than what was anticipated at study design (70%) including responses in 50% of the patients with the 17p deletion and in 50% of patients with fludarabine-refractory disease. The median survival was 21.5 months (95% CI: 12.3–30.7 months).34
Another Phase II study of 36 patients was conducted at MD Anderson Cancer Center investigating the combination ofatumumab and lenalidomide in patients with relapsed CLL with prior FCR treatment. The specific regimen was longer than in the Costa et al34 trial and was planned as: ofatumumab IV weekly for 4 weeks (300 mg week 1 followed by 1,000 mg on subsequent weeks), monthly in months 2–6, and every other month in months 7–24 with lenalidomide 10 mg orally per day started on day 9 and continued for 24 months. In terms of patient characteristics, 65% harbored an unmutated IGHV and 26% had the 17p deletion. There was a 68% response rate, with 24% of patients achieving a CR and about half of patients with the 17p deletion achieving a PR. The median duration of response was 22 months, with a median follow-up of 24 months.41 These results are superior to that seen in the Costa trial and this could be due to the longer duration of treatment.
Although many studies have shown promising results with ofatumumab, CLL ultimately becomes resistant to treatment. In a recent publication by Baig et al, it was shown that following CDC of circulating cells by ofatumumab, there is a rebound increased lymphocytosis due to CLL cell mobilization from a noncirculating compartment. In addition, the circulating cells that are not lysed via CDC undergo a process called trogocytosis.15 Trogocytosis is the unidirectional transfer of plasma membrane material (ie, CD20) from target cells to effector cells of the immune system.42 Thus, as a consequence of trogocytosis, C20 expression is markedly decreased leading to a lack of response to ofatumumab. Thus, it is suggested that alternate dosing regimens, perhaps smaller doses more frequently, could prevent this resistance phenomenon.15 Moreover, it does not appear that ofatumumab alone has great clinical activity in patients previously treated with rituximab.38 Finally, it is important to point out that there has not been a randomized study comparing rituximab and ofatumumab to demonstrate differences in efficacy.
Obinutuzumab
More recently, there has been excitement over a next gene-ration anti-CD20 humanized, glycoengineered type 2 mAb, obinutuzumab (GA101) which was FDA approved in November 2013 based on the results of the Phase III CLL 11 trial.43 Obinutuzumab binds to the CD20 type II epitope as opposed to rituximab, which binds to the type I epitope.44–46 Type II mAbs differ from type I mAbs in that they do not utilize complement (less CDC) and thus, instead promote increased ADCC as well as far greater direct cell death (DCD).14,47,48 The proposed mechanism of DCD is that binding of the drug to CD20 leads to a series of events, including actin reorganization, homotypic adhesion, lysosomal permeabilization, and finally, ROS-dependent cell death.43 In particular, obinutuzumab has a 50-fold higher affinity for the FcgRIIIa region and 100-fold greater ADCC than rituximab.43,49 It also has no CD20 antigen internalization with binding, and thus no shaving/trogocytosis in contrast to rituximab.43
The CLL 11 study conducted by the GCLLSG was recently published in the New England Journal of Medicine (NEJM). In this study, 768 untreated CLL patients (median age of 73 years) with a ‘clinically meaningful burden of coexisting conditions’ defined as a score >6 on the Cumulative Illness Rating Scale (CIRS) or a creatinine clearance (CrCl) of 30–69 mL/minute were randomized into one of three arms in a 1:2:2 fashion. Regarding comorbidities, 82% of the subjects had at least three and 27% of subjects suffered from at least one uncontrolled medical condition. The three arms included: chlorambucil alone, chlorambucil–rituximab, and chlorambucil–obinutuzumab for six 28-day cycles, as tolerated.47 The choice of chlorambucil as a comparator was made because at the time of the CLL 11 study, there were no other proven effective regimens aside from chlorambucil monotherapy for elderly patients and/or those with significant comorbidities.43 Of note, crossover was allowed from the chlorambucil-alone arm to the obinutuzumab–chlorambucil group for disease progression. The chlorambucil–obinutuzumab arm had the greatest PFS interval, with a median PFS of 11.1 months in the chlorambucil-alone arm compared to 26.7 months in the obinutuzumab-containing arm (HR: 0.18, 95% CI: 0.13–0.24, P<0.001) and a PFS of 16.3 months in the rituximab–chlorambucil arm compared to the monotherapy arm (HR: 0.44, 95% CI: 0.34–0.57, P<0.001). Of note, these improvements were not seen in patients with deletion 17p. Additionally, the obinutuzumab–chlorambucil arm had improved overall, complete, and molecular responses when compared to the rituximab–chlorambucil arm. There was not a significant improvement in OS in the obinutuzumab–chlorambucil arm versus the rituximab–chlorambucil arm (HR: 0.66, 95% CI: 0.41–1.06, P=0.08). The rate of induction of negative status in the blood for minimal residual disease was greater than ten-fold higher in the obinutuzumab–chlorambucil arm over the rituximab–chlorambucil arm (87/231 vs 8/243). Finally, in terms of toxicity, the two arms with mAbs had greater neutropenia, but without increased infections. However, the obinutuzumab arm had a greater incidence in severe infusion reactions (primarily with the first infusion), with some requiring termination of treatment. It is postulated that this may be due to the rapid B cell depletion by obinutuzumab.47
At the American Society of Hematology (ASH) Annual Meeting of 2013, the results of the Phase Ib GALTON study were presented. This was a nonrandomized, parallel group study of 41 patients investigating obinutuzumab plus FC (fludarabine + cyclophosphamide) or B (bendamustine) as initial therapy for CLL. The ORR was 62% (two CR, three CR with incomplete recovery of blood count [CRi], eight PR) in the G-FC arm and 90% (four CR, five CRi, nine PR) in the G-B arm. Importantly, the adverse events were similar between groups.50 Preliminary results of the GAGE trial were presented in an abstract at the American Society of Clinical Oncology (ASCO) Annual Meeting in 2014.51 This was a Phase II trial of 80 patients comparing two doses of obinutuzumab, 1,000 and 2,000 mg, in untreated CLL patients. The results were not statistically significant with an ORR P-value of 0.08. Ongoing studies investigating obinutuzumab including combinations with ABT-199, a BCL2 inhibitor, and lenalidomide are currently recruiting patients.4
BCR pathway inhibitors
The BCR pathway is central to the survival and proliferation of CLL.52 The malignant CLL cells accumulate in lymphatic tissue pseudofollicles. Both chemokine signals from the microenvironment as well as aberrantly constitutively active BCR-signaling pathways result in proliferation of the disease.53 Many novel BCR pathway inhibitors have recently demonstrated efficacy in CLL.
In its normal state, the BCR is composed of pairs of immunoglobulin heavy and light chains, each with its own variable region. BCR signaling is promoted by one of two ways: an active versus a tonic process. The active mechanism drives signaling after an extracellular antigen binds to a variable region on the BCR. The tonic mechanism does not depend on antigenic contact to induce signaling. CLL has hijacked the BCR cascade for its own survival.54 In CLL, there is aberrant regulation of the BCR pathway, resulting in constitutive activation of downstream kinase signaling.55
In the process of BCR pathway signaling, CD19, a B cell transmembrane protein becomes phosphorylated by Src kinase, which in turn causes phosphoinositide 3-kinase (PI3K) to interact with the BCR. This interaction recruits Bruton’s tyrosine kinase (BTK) and AKT (a cytosolic protein kinase) to the plasma B cell membrane, ultimately activating nuclear factor κB (NF-κB), PI3K, mitogen-activated protein kinase (MAPK), nuclear factor of activated T cells (NFAT), and RAS pathways, resulting in cell proliferation and survival.54,56–58 In fact, in CLL, there is massive amplification of these constitutively active survival pathways (PI3K, NF-κB, and MAPK/ERK).4 Not surprisingly, drug development targeting players in the BCR pathway has been a focused topic in CLL translational research endeavors.
The specific PI3-kinase isoforms found in hematopoietic cells are delta (δ) and gamma (γ) subtypes.55,59 Activation of PI3Kd results in CLL proliferation, survival, and motility, as noted earlier. Idelalisib, an oral selective inhibitor of PI3Kd, was developed to treat CLL.59 Recently published in May 2014, Brown et al conducted a Phase I trial in 54 patients with unfavorable relapsed and refractory CLL, utilizing six differing doses of oral idelalisib, as tolerated. In terms of unfavorable patient factors, 80% had bulky lymphadenopathy, 91% had unmutated IGHV, 24% harbored the 17p deletion and/or TP53 mutations, and the patients had a median number of five previous CLL-directed therapies. The ORR was 72% and 81% of patients exhibited a nodal response. The median PFS was 15.8 months.60 A key observation from this trial was the development of significant lymphocytosis that corresponded with a decrease in lymphadenopathy. It is thought that idelalisib and other inhibitors of the BCR-signaling pathway cause a migration of CLL from the protective lymph node niche into the periphery where survival is shortened. Because of this dramatic lymphocytosis, response guidelines have been modified for patients receiving these agents.61 Idelalisib was ultimately FDA approved in July 2014 for relapsed CLL/SLL and follicular lymphoma.59
There have also been a number of studies investigating combination regimens with mAb-directed drugs adjunctive with idelalisib in order to target CLL from multiple pathogenic angles. The rationale for the combined modality is that inhibitors of the BCR pathway redistribute the malignant CLL cells from tissue compartments (lymph node and spleen) to the periphery, allowing for these now peripheral blood CLL cells to be attacked by mAb therapy.62 Recently, Furman et al63 published the results of a multicenter, randomized Phase III study of 220 relapsed CLL patients unable to undergo cytotoxic chemotherapy investigating idelalisib 150 mg and rituximab versus placebo and rituximab. Given the marked efficacy of combination therapy with an ORR of 81% versus 13% (P<0.001) in the placebo arm (including those with the 17p deletion, TP53 mutations, and unmutated IGHV), the study was discontinued at the interim analysis under the auspice of the data and safety monitoring board.63 At ASCO 2014, two ongoing combination studies were presented without results reported at this time. First, Eradat et al is conducting a Phase III, randomized study comparing idelalisib in combination with BR in previously treated patients.64 Second, Salles et al presented a similar trial but with previously untreated CLL patients, which opened for enrollment in January 2014.65
Ibrutinib, an orally available, BTK-specific inhibitor, has demonstrated significant single-agent activity and is now FDA approved for use in CLL. A Phase Ib–II multicenter study of 85 relapsed or refractory CLL/SLL high-risk patients was conducted with ibrutinib. The ORR was 71% in both the 420 mg and 840 mg arms. At 26 months, the PFS rate was 75% and the OS rate was 83%.66 In the NEJM in May 2014, a randomized Phase III clinical trial was published comparing single-agent daily ofatumumab versus ibrutinib in 391 poor-risk CLL patients with relapsed or refractory disease. Ibrutinib was clearly superior in terms of both improved OS at 12 months (90% in ibrutinib arm versus 81% in ofatumumab arm, P=0.005) as well as PFS. Most notably, these improvements were also achieved in patients with the 17p deletion as well as those with resistance to purine analogs.67
Although these results are exciting, resistance to ibrutinib has been demonstrated in select patients. CLL can develop a mutation at C481S of the BTK gene, which prevents binding of ibrutinib and confers resistance to the drug.68,69 Dong et al recently showed that IPI-145, a dual PI3kδ and -γ inhibitor, overcomes C481S ibrutinib resistance.55 Preliminary results of a Phase I study of 55 patients evaluating the efficacy of IPI-145 were presented at ASCO 2013.70 Eleven of the 55 patients had CLL and 82% (n=9) had a PR or nodal response after two cycles.70 There are currently ongoing trials assessing IPI-145 in CLL.
Chimeric antigen receptor T cells
Another tool employed by investigators in an attempt to utilize the host immune system to tackle malignancies is the concept of chimeric antigen receptor (CAR) T cells. CAR T cells are genetically engineered T cells designed to recognize specific antigens found on tumor cells. The T cells are collected from patients and genetically modified, usually through viral transduction, expanded ex vivo, and then reinfused into the patient.71
In 2011, Porter et al published a case report utilizing a CD19 CAR T cell in one patient with refractory CLL who achieved a sustained remission of at least 10 months.72 CD19 is an attractive target in CLL as it is expressed on malignant B cells.73 Cytokine release syndrome (CRS) is a serious adverse event that can follow CAR T cell treatment. At ASH 2012, Grupp et al presented an abstract discussing an adverse event of CAR treatment manifested as CRS and showed that this can be ameliorated with the use of tocilizumab, an antibody to IL-6.74 Aside from CRS, B cell aplasia with persistent hypogammaglobulinemia with increased infection risk remains an additional concern.75
More recently, CAR CD19 T cells have been utilized experimentally in patients with refractory acute lymphoblastic leukemia with promising results giving hope for similar results in CLL. Maude et al published data on 30 patients infused with autologous T cells transduced with a CD19 CAR lentiviral vector. The 6-month EFS rate was 67% (95% CI: 51%–88%) and the OS rate was 78% (95% CI: 65%–95%).76 A Phase I/II trial at Memorial Sloan Kettering Cancer Center investigating CAR CD19 T cells for CLL is currently accruing patients. The results from this study are greatly anticipated.
Conclusion
With standard chemoimmunotherapy, the majority of CLL patients will have a significant and clinically meaningful response. However, this benefit is tempered by inevitable relapse and complications related to therapy. The beginning of this millennium brought targeted therapy, in the form of the CD20-specific antibody rituximab, and with it, further improvements in our ability to treat CLL. Next generation CD20 therapy has demonstrated the ability to regain responses when rituximab is no longer efficacious in the case of ofatumumab, and the potential for improved responses relative to rituximab, as demonstrated in the CLL11 study (Figure 1).
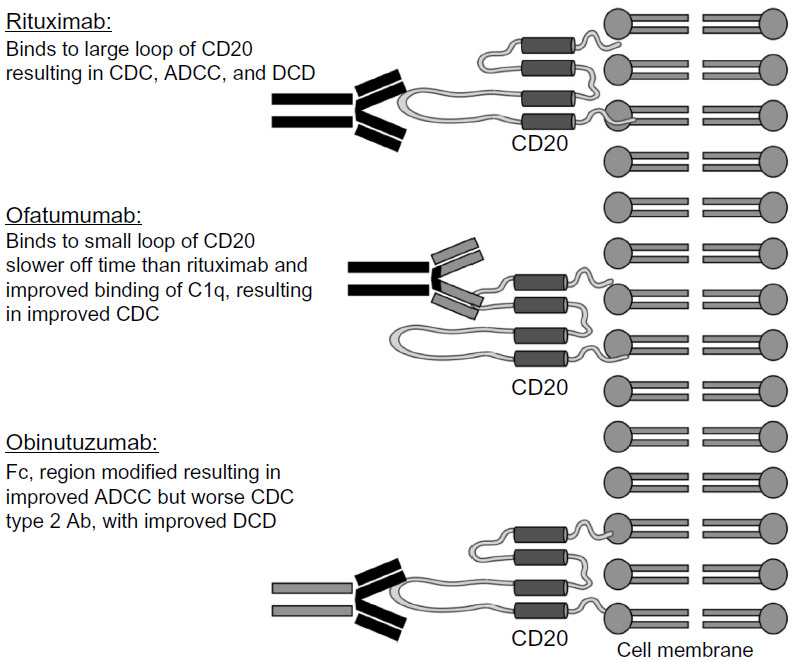 | Figure 1 Rituximab binds to the large loop of CD20 resulting in CDC, ADCC, and DCD. |
A discussion of the importance of CD20 therapy cannot ignore the remarkable developments seen with the targeting of the BCR-signaling pathway. As single agents, idelalisib and ibrutinib have demonstrated significant activity in CLL patients thought to be traditionally poorly responsive to chemotherapy. In addition, a class effect common to these drugs is the migration of CLL from the protected lymph node and bone marrow niches. Future trials seek to take advantage of this migration by combining CD20 targeting and chemotherapy to eliminate CLL in the periphery.
Perhaps most significantly, the combination of CD20 blockade with BCR inhibition suggests the possibility that we may be entering a future where standard treatment options for CLL do not include chemotherapy and that patients have the potential to avoid these toxic and damaging medications. In an effort to explore this possibility, on October 15, 2014, Pharmacyclics and Roche announced a clinical drug supply agreement to evaluate ibrutinib in conjunction with obinutuzumab in patients with CLL.77 Taken together, these findings demonstrate the clear relationship between an understanding of the biology of a disease, the rationale development of targeted therapies, and improved outcomes for patients.
Disclosure
The authors report no conflicts of interest in this work.
References
Hallek M. Chronic lymphocytic leukemia: 2013 update on diagnosis, risk stratification and treatment. Am J Hematol. 2013;88(9):803–816. | |
Sebejova L, Borsky M, Jaskova Z, et al. Distinct in vitro sensitivity of p53-mutated and ATM-mutated chronic lymphocytic leukemia cells to ofatumumab and rituximab. Exp Hematol. 2014;42(10):867–874. e1. | |
Dohner H, Stilgenbauer S, Benner A, et al. Genomic aberrations and survival in chronic lymphocytic leukemia. N Engl J Med. 2000;343(26):1910–1916. | |
Byrd JC, Jones JJ, Woyach JA, Johnson AJ, Flynn JM. Entering the era of targeted therapy for chronic lymphocytic leukemia: impact on the practicing clinician. J Clin Oncol. 2014;32(27):3039–3047. | |
Jaglowski SM, Byrd JC. Rituximab in chronic lymphocytic leukemia. Semin Hematol. 2010;47(2):156–169. | |
Ghia P, Hallek M. Management of chronic lymphocytic leukemia. Haematologica. 2014;99(6):965–972. | |
Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Lyon, France: IARC; 2008. | |
Liang Y, Buckley TR, Tu L, Langdon SD, Tedder TF. Structural organization of the human MS4A gene cluster on Chromosome 11q12. Immunogenetics. 2001;53(5):357–368. | |
Teeling JL, Mackus WJ, Wiegman LJ, et al. The biological activity of human CD20 monoclonal antibodies is linked to unique epitopes on CD20. J Immunol. 2006;177(1):362–371. | |
Cragg MS, Walshe CA, Ivanov AO, Glennie MJ. The biology of CD20 and its potential as a target for mAb therapy. Curr Dir Autoimmun. 2005;8:140–174. | |
Manches O, Lui G, Chaperot L, et al. In vitro mechanisms of action of rituximab on primary non-Hodgkin lymphomas. Blood. 2003;101(3):949–954. | |
Harjunpaa A, Junnikkala S, Meri S. Rituximab (anti-CD20) therapy of B-cell lymphomas: direct complement killing is superior to cellular effector mechanisms. Scand J Immunol. 2000;51(6):634–641. | |
Wierda W, O’Brien S, Wen S, et al. Chemoimmunotherapy with fludarabine, cyclophosphamide, and rituximab for relapsed and refractory chronic lymphocytic leukemia. J Clin Oncol. 2005;23(18):4070–4078. | |
Osterborg A. Ofatumumab, a human anti-CD20 monoclonal antibody. Expert Opin Biol Ther. 2010;10(3):439–449. | |
Baig NA, Taylor RP, Lindorfer MA, et al. Induced resistance to ofatumumab-mediated cell clearance mechanisms, including complement-dependent cytotoxicity, in chronic lymphocytic leukemia. J Immunol. 2014;192(4):1620–1629. | |
Jaglowski SM, Alinari L, Lapalombella R, Muthusamy N, Byrd JC. The clinical application of monoclonal antibodies in chronic lymphocytic leukemia. Blood. 2010;116(19):3705–3714. | |
Almasri NM, Duque RE, Iturraspe J, Everett E, Braylan RC. Reduced expression of CD20 antigen as a characteristic marker for chronic lymphocytic leukemia. Am J Hematol. 1992;40(4):259–263. | |
Keating MJ, O’Brien S, Albitar M, et al. Early results of a chemoimmunotherapy regimen of fludarabine, cyclophosphamide, and rituximab as initial therapy for chronic lymphocytic leukemia. J Clin Oncol. 2005;23(18):4079–4088. | |
Tam CS, O’Brien S, Wierda W, et al. Long-term results of the fludarabine, cyclophosphamide, and rituximab regimen as initial therapy of chronic lymphocytic leukemia. Blood. 2008;112(4):975–980. | |
Hallek M, Fischer K, Fingerle-Rowson G, et al; International Group of Investigators; German Chronic Lymphocytic Leukaemia Study Group. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet. 2010;376(9747):1164–1174. | |
Fischer K, Bahlo J, Fink AM, et al. Extended follow up of the CLL8 Protocol, a randomized phase-iii trial of the German CLL Study Group (GCLLSG) comparing fludarabine and cyclophosphamide (FC) to FC plus rituximab (FCR) for previously untreated patients with chronic lymphocytic leukemia (CLL): results on survival, progression-free survival, delayed neutropenias and secondary malignancies confirm superiority of the FCR regimen. Presented at: ASH Annual Meeting and Exposition; December 8–11, 2010; Georgia, GA. Abstract 435. | |
Robak T, Dmoszynska A, Solal-Céligny P, et al. Rituximab plus fludarabine and cyclophosphamide prolongs progression-free survival compared with fludarabine and cyclophosphamide alone in previously treated chronic lymphocytic leukemia. J Clin Oncol. 2010;28(10):1756–1765. | |
Lin KI, Tam CS, Keating MJ, et al. Relevance of the immunoglobulin VH somatic mutation status in patients with chronic lymphocytic leukemia treated with fludarabine, cyclophosphamide, and rituximab (FCR) or related chemoimmunotherapy regimens. Blood. 2009;113(14):3168–3171. | |
Fischer K, Cramer P, Busch R, et al. Bendamustine in combination with rituximab for previously untreated patients with chronic lymphocytic leukemia: a multicenter phase II trial of the German Chronic Lymphocytic Leukemia Study Group. J Clin Oncol. 2012;30(26):3209–3216. | |
Badoux XC, Keating MJ, Wang X, et al. Fludarabine, cyclophosphamide, and rituximab chemoimmunotherapy is highly effective treatment for relapsed patients with CLL. Blood. 2011;117(11):3016–3024. | |
Laurenti L, Vannata B, Innocenti I, et al. Chlorambucil plus rituximab as front-line therapy in elderly/unfit patients affected by B-cell chronic lymphocytic leukemia: results of a single-centre experience. Mediterr J Hematol Infect Dis. 2013;5(1):e2013031. | |
Foà R, Del Giudice I, Cuneo A, et al. Chlorambucil plus rituximab with or without maintenance rituximab as first-line treatment for elderly chronic lymphocytic leukemia patients. Am J Hematol. 2014;89(5):480–486. | |
Hillmen P, Gribben JG, Follows GA, et al. Rituximab plus chlorambucil as first-line treatment for chronic lymphocytic leukemia: final analysis of an open-label phase II study. J Clin Oncol. 2014;32(12):1236–1241. | |
Cortelezzi A, Sciumè M, Liberati AM, et al. Bendamustine in combination with ofatumumab in relapsed or refractory chronic lymphocytic leukemia: a GIMEMA Multicenter Phase II Trial. Leukemia. 2014; 28(3):642–648. | |
Coiffier B, Lepretre S, Pedersen LM, et al. Safety and efficacy of ofatumumab, a fully human monoclonal anti-CD20 antibody, in patients with relapsed or refractory B-cell chronic lymphocytic leukemia: a phase 1–2 study. Blood. 2008;111(3):1094–1100. | |
Beum PV, Lindorfer MA, Beurskens F, et al. Complement activation on B lymphocytes opsonized with rituximab or ofatumumab produces substantial changes in membrane structure preceding cell lysis. J Immunol. 2008;181(1):822–832. | |
Pawluczkowycz AW, Beurskens FJ, Beum PV, et al. Binding of submaximal C1q promotes complement-dependent cytotoxicity (CDC) of B cells opsonized with anti-CD20 mAbs ofatumumab (OFA) or rituximab (RTX): considerably higher levels of CDC are induced by OFA than by RTX. J Immunol. 2009;183(1):749–758. | |
Teeling JL, French RR, Cragg MS, et al. Characterization of new human CD20 monoclonal antibodies with potent cytolytic activity against non-Hodgkin lymphomas. Blood. 2004;104(6):1793–1800. | |
Costa LJ, Fanning SR, Stephenson J, et al. Sequential ofatumumab and lenalidomide for the treatment of relapsed and refractory chronic lymphocytic leukemia and small lymphocytic lymphoma. Leuk Lymphoma. Epub August 17, 2014. | |
Wierda WG, Kipps TJ, Mayer J, et al; Hx-CD20-406 Study Investigators. Ofatumumab as single-agent CD20 immunotherapy in fludarabine-refractory chronic lymphocytic leukemia. J Clin Oncol. 2010;28(10):1749–1755. | |
Wierda WG, Kipps TJ, Dürig J, et al; 407 Study Investigators. Chemoimmunotherapy with O-FC in previously untreated patients with chronic lymphocytic leukemia. Blood. 2011;117(24):6450–6458. | |
Wierda WG, Padmanabhan S, Chan GW, et al; Hx-CD20-406 Study Investigators. Ofatumumab is active in patients with fludarabine-refractory CLL irrespective of prior rituximab: results from the phase 2 international study. Blood. 2011;118(19):5126–5129. | |
Cheson BD. Ofatumumab, a novel anti-CD20 monoclonal antibody for the treatment of B-cell malignancies. J Clin Oncol. 2010;28(21):3525–3530. | |
Hillmen P, Robak T, Janssens A, et al. Ofatumumab + chlorambucil versus chlorambucil alone in patients with untreated chronic lymphocytic leukemia (CLL): results of the phase III study complement 1 (OMB110911). Presented at: American Society of Hematology Annual Meeting and Exposition; December 7–10, 2013; New Orleans, LA. Abstract 528. | |
Ramsay AG, Johnson AJ, Lee AM, et al. Chronic lymphocytic leukemia T cells show impaired immunological synapse formation that can be reversed with an immunomodulating drug. J Clin Invest. 2008;118(7):2427–2437. | |
Ferrajoli AF, Falchi L, O’Brien S, et al. Combination of ofatumumab and lenalidomide in patients with relapsed chronic lymphocytic leukemia (CLL): results of a phase II trial. Presented at: American Society of Hematology Annual Meeting and Exposition; December 8–11, 2012; Atlanta, GA. Abstract 720. | |
Aucher A, Magdeleine E, Joly E, Hudrisier D. Capture of plasma membrane fragments from target cells by trogocytosis requires signaling in T cells but not in B cells. Blood. 2008;111(12):5621–5628. | |
Illidge T, Cheadle EJ, Donaghy C, Honeychurch J. Update on obinutuzumab in the treatment of B-cell malignancies. Expert Opin Biol Ther. 2014;14(10):1507–1517. | |
Lee HZ, Miller BW, Kwitkowski VE, et al. US Food and drug administration approval: obinutuzumab in combination with chlorambucil for the treatment of previously untreated chronic lymphocytic leukemia. Clin Cancer Res. 2014;20(15):3902–3907. | |
Salles G, Morschhauser F, Lamy T, et al. Phase 1 study results of the type II glycoengineered humanized anti-CD20 monoclonal antibody obinutuzumab (GA101) in B-cell lymphoma patients. Blood. 2012;119(22):5126–5132. | |
Cartron G, de Guibert S, Dilhuydy MS, et al. Obinutuzumab (GA101) in relapsed/refractory chronic lymphocytic leukemia: final data from the phase 1/2 GAUGUIN study. Blood. 2014;124(14):2196–2202. | |
Goede V, Fischer K, Busch R, et al. Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N Engl J Med. 2014;370(12):1101–1110. | |
Rogers KA, Jones JA. Obinutuzumab for the treatment of chronic lymphocytic leukemia. Drugs Today (Barc). 2014;50(6):407–419. | |
Terszowski G, Klein C, Stern M. KIR/HLA interactions negatively affect rituximab- but not GA101 (obinutuzumab)-induced antibody-dependent cellular cytotoxicity. J Immunol. 2014;192(12):5618–5624. | |
Brown JR, O’Brien S, Kingsley D, et al. Safety and efficacy of obinutuzumab (GA101) with fludarabine/cyclophosphamide (G-FC) or bendamustine (G-B) in the initial therapy of patients with chronic lymphocytic leukemia (CLL): results from the phase 1b Galton trial (GAO4779g). Presented at: American Society of Hematology Annual Meeting and Exposition; December 7–10, 2013; New Orleans, LA. Abstract 523. | |
Flynn JM, Byrd JC, Kipps TJ, et al. Obinutuzumab (GA101) 1,000 mg versus 2,000 mg in patients with chronic lymphocytic leukemia (CLL): results of the phase II GAGE (GAO4768g) trial. J Clin Oncol. 2014;32(5 Suppl): abstract 7083. | |
Bernal A, Pastore RD, Asgary Z, et al. Survival of leukemic B cells promoted by engagement of the antigen receptor. Blood. 2001;98(10): 3050–3057. | |
Burger JA, Gribben JG. The microenvironment in chronic lymphocytic leukemia (CLL) and other B cell malignancies: insight into disease biology and new targeted therapies. Semin Cancer Biol. 2014;24:71–81. | |
Young RM, Staudt LM. Targeting pathological B cell receptor signalling in lymphoid malignancies. Nat Rev Drug Discov. 2013;12(3):229–243. | |
Dong S, Guinn D, Dubovsky JA, et al. IPI-145 antagonizes intrinsic and extrinsic survival signals in chronic lymphocytic leukemia cells. Blood. 2014;124(24):3583–3586. | |
Yamamoto T, Yamanashi Y, Toyoshima K. Association of Src-family kinase Lyn with B-cell antigen receptor. Immunol Rev. 1993;132:187–206. | |
Rolli V, Gallwitz M, Wossning T, et al. Amplification of B cell antigen receptor signaling by a Syk/ITAM positive feedback loop. Mol Cell. 2002;10(5):1057–1069. | |
Mohamed AJ, Yu L, Backesjo CM, et al. Bruton’s tyrosine kinase (Btk): function, regulation, and transformation with special emphasis on the PH domain. Immunol Rev. 2009;228(1):58–73. | |
Markham A. Idelalisib: first global approval. Drugs. 2014;74(14):1701–1707. | |
Brown JR, Byrd JC, Coutre SE, et al. Idelalisib, an inhibitor of phosphatidylinositol 3-kinase p110δ, for relapsed/refractory chronic lymphocytic leukemia. Blood. 2014;123(22):3390–3397. | |
Hallek M, Cheson BD, Catovsky D, et al. Response assessment in chronic lymphocytic leukemia treated with novel agents causing an increase of peripheral blood lymphocytes. Blood. Epub June 4, 2012. | |
Burger JA, Montserrat E. Coming full circle: 70 years of chronic lymphocytic leukemia cell redistribution, from glucocorticoids to inhibitors of B-cell receptor signaling. Blood. 2013;121(9):1501–1509. | |
Furman RR, Sharman JP, Coutre SE, et al. Idelalisib and rituximab in relapsed chronic lymphocytic leukemia. N Engl J Med. 2014;370(11):997–1007. | |
Eradat HA, Robak T, Delgado J, et al. A phase 3, randomized, double-blind, placebo-controlled study evaluating the efficacy and safety of idelalisib (GS-1101) in combination with bendamustine and rituximab for previously treated chronic lymphocytic leukemia (CLL). J Clin Oncol. 2013;31 Suppl: abstract TPS7133. | |
Salles GA, Lamanna N, Amin BR, et al. A phase 3, randomized, double-blind, placebo-controlled study evaluating the efficacy and safety of idelalisib in combination with bendamustine and rituximab for previously untreated chronic lymphocytic leukemia. J Clin Oncol. 2014;32 Suppl 5: abstract TPS7123. | |
Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med. 2013;369(1):32–42. | |
Byrd JC, Brown JR, O’Brien S, et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N Engl J Med. 2014;371(3):213–223. | |
Woyach JA, Furman RR, Liu TM, et al. Resistance mechanisms for the Bruton’s tyrosine kinase inhibitor ibrutinib. N Engl J Med. 2014;370(24):2286–2294. | |
Furman RR, Cheng S, Lu P, et al. Ibrutinib resistance in chronic lymphocytic leukemia. N Engl J Med. 2014;370(24):2352–2354. | |
Horwitz SM, Flinn I, Patel MR, et al. Preliminary safety and efficacy of IPI-145, a potent inhibitor of phosphoinositide-3-kinase-δ,γ, in patients with relapsed/refractory lymphoma. J Clin Oncol. 2013;31 Suppl: abstract 8518. | |
Gill S, June CH. Going viral: chimeric antigen receptor T-cell therapy for hematological malignancies. Immunol Rev. 2015;263(1):68–89. | |
Porter DL, Levine BL, Kalos M, Bagg A, June CH. Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia. N Engl J Med. 2011;365(8):725–733. | |
Uckun FM, Jaszcz W, Ambrus JL, et al. Detailed studies on expression and function of CD19 surface determinant by using B43 monoclonal antibody and the clinical potential of anti-CD19 immunotoxins. Blood. 1988;71(1):13–29. | |
Grupp S PD, Teachey D, et al. CD19-redirected chimeric antigen receptor T (CART19) cells induce a cytokine release syndrome (CRS) and induction of treatable macrophage activation syndrome (MAS) that can be managed by the IL-6 antagonist tocilizumab (toc). American Society of Hematology Annual Meeting and Exposition; December 8–11, 2012; Atlanta, GA. Abstract 2604. | |
Awan FT, Byrd JC. New strategies in chronic lymphocytic leukemia: shifting treatment paradigms. Clin Cancer Res. 2014;20(23):5869–5874. | |
Maude SL, Frey N, Shaw PA, et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N Engl J Med. 2014;371(16):1507–1517. | |
Pharmacyclics and Roche Agree to Jointly Evaluate Ibrutinib and Obinutuzumab in Lymphoma and Leukemia [webpage on the Internet]. Onco’Zine; October 16, 2014. Available from: http://oncozine.com/profiles/blogs/pharmacyclics-and-roche-agree-to-jointly-evaluate-ibrutinib-and-o. Accessed January 15, 2015. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.