")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 7
Sociodemographic drivers of multiple sexual partnerships among women in three rural districts of Tanzania
Authors Exavery A, Kanté AM, Tani K, Hingora A, Phillips JF
Received 31 October 2014
Accepted for publication 10 December 2014
Published 9 April 2015 Volume 2015:7 Pages 105—113
DOI https://doi.org/10.2147/HIV.S76694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Shenghan Lai
Amon Exavery,1 Almamy Malick Kanté,1–3 Kassimu Tani,1 Ahmed Hingora,1 James F Phillips2
1Ifakara Health Institute, Dar es Salaam, Tanzania; 2Heilbrunn Department of Population and Family Health, Mailman School of Public Health, Columbia University, New York, NY, USA; 3Swiss Tropical and Public Health Institute, University of Basel, Basel, Switzerland
Background: This study examines prevalence and correlates of multiple sexual partnerships (MSP) among women aged 15+ years in Rufiji, Kilombero, and Ulanga districts of Tanzania.
Materials and methods: Data were collected in a cross-sectional household survey in Rufiji, Kilombero, and Ulanga districts in Tanzania in 2011. From the survey, a total of 2,643 sexually active women ages 15+ years were selected for this analysis. While the chi-square test was used for testing association between MSP and each of the independent variables, logistic regression was used for multivariate analysis.
Results: Number of sexual partners reported ranged from 1 to 7, with 7.8% of the women reporting multiple sexual partners (2+) in the past year. MSP was more likely among both ever married women (adjusted odds ratio [AOR] =3.83, 95% confidence interval [CI] 1.40–10.49) and single women (AOR =6.13, 95% CI 2.45–15.34) than currently married women. There was an interaction between marital status and education, whereby MSP was 85% less likely among single women with secondary or higher education compared to married women with no education (AOR =0.15, 95% CI 0.03–0.61). Furthermore, women aged 40+ years were 56% less likely compared to the youngest women (<20 years) to report MSP (AOR =0.44, 95% CI 0.24–0.80). The odds of MSP among Muslim women was 1.56 times as high as that for Christians women (AOR =1.56, 95% CI 1.11–2.21). Ndengereko women were 67% less likely to report MSP compared to Pogoro women (AOR =0.33, 95% CI 0.18–0.59).
Conclusion: Eight percent of the women aged 15+ in Rufiji, Kilombero, and Ulanga districts of Tanzania are engaged in MSP. Encouraging achievement of formal education, especially at secondary level or beyond, may be a viable strategy toward partner reduction among unmarried women. Age, religion, and ethnicity are also important dimensions for partner reduction efforts.
Keywords: HIV/AIDS, transmission, Rufiji, Kilombero, Ulanga
Introduction
While the human immunodeficiency virus (HIV) and acquired immune deficiency syndrome (AIDS) epidemic remains a significant global health concern, sub-Saharan Africa continues to be the most affected region on the globe.1 Behavioral patterns in sexual relationships play a significant role in the spread of HIV/AIDS.2 A recent publication in the Lancet cites extra-couple partnerships as a factor that has, and continues to play, a paramount role in driving new HIV infections among men and women within couples.3 According to the same study, while the transmission within couples occurs mostly from men to women, the study indicates that women experience a very high risk period before couple formation. In sub-Saharan Africa, unsafe sex is accountable for the vast majority of HIV infections.4 In Tanzania, the epidemic is described as generalized since it affects all sectors of the population.5 In 2012, the HIV/AIDS prevalence among Tanzanian adults age 15–49 years was estimated at 5.1% (6.2% women and 3.8% men),6 ranging from as low as <2% in Arusha region to as high as 16% in Iringa region.7 In 2011, Tanzania recorded more than 80,000 deaths due to HIV/AIDS.9 Approximately 1.6 million Tanzanians are living with HIV,8 with over 400 new infections occurring every day, spreading predominantly through heterosexual contact.6,9
Previous studies have identified a number of factors associated with multiple sexual partnerships (MSP). In 2006, a think tank of the Southern Africa Development Community reported high levels of multiple and concurrent sexual partnerships among men and women and identified inconsistent and incorrect condom use and low levels of male circumcision as key drivers of the HIV epidemic in the region.10 Other factors that fuel the epidemic include male attitudes and behaviors, intergenerational sex, gender-based violence, stigma, lack of openness about the epidemic, and untreated sexually transmitted infections (STIs). Underlying these biological and social drivers are the structural factors of high mobility and inequalities of wealth as well as cultural factors, including gender inequality, with young women rendered particularly vulnerable to HIV infection.10
Van den Borne argues that the major motivational driver for MSP among women in Malawi is the struggle for survival in the fight against poverty, which encourages engagement in transactional sex and MSP to make ends meet.11 This was also emphasized by several other studies.12–15 However, these were not the only socioeconomically related drivers of MSP according to several studies conducted by Chirwa16,17 and Msolomba and Chirwa.18 They point out that while men engage in MSP in pursuit of prestige, status, and honor, women are driven by attractiveness, peer pressure, and quest for leisure and entertainment among other motivators. These studies detail further that for both men and women, the pursuit of leisure and entertainment, sexual gratification, experimentation with sexual variety, alcohol abuse, and migrancy result in MSP. History, culture, socialization, and religion are also major determinants of multiple concurrent partners in the country.
MSP is a risky sexual behavior that substantially contributes to the spread of the HIV/AIDS pandemic.19 Forms of MSP include promiscuity, infidelity, prostitution and commercial sexual activities, and rape.8 MSP along with inconsistent or absent condom use is associated with increased risk of contracting HIV infection. In countries where HIV infection has declined significantly, such as Uganda, Kenya, Zimbabwe, Zambia, and Thailand, partner reduction reportedly played a major role.20 This underscores the need for efforts to promote MSP reduction to combat the HIV pandemic in other countries. Therefore, a strong evidence base concerning both the individual and the sociocultural drivers of MSP is needed to inform the design and scale-up strategies that will effectively promote partner reduction and change the social norms that facilitate MSP.20
Unfortunately, a rigorous assessment of the drivers of MSP among women in rural Tanzania and most developing countries is limited. In response to this gap, this study seeks to establish prevalence of and factors associated with MSP among 15+ year-old women in Rufiji, Kilombero, and Ulanga districts of Tanzania.
Materials and methods
Study area
This analysis is based on data collected in three rural district of Tanzania – Rufiji, Kilombero, and Ulanga – in 2011. Within these districts, there are two ongoing health and demographic surveillance systems (HDSS) of Rufiji and Ifakara, which are longitudinal, health and vital events registration systems that monitor demographic events, including births, deaths, and migrations. The Rufiji HDSS is located in the Rufiji district in the Pwani region, while the Ifakara HDSS occupies parts of Kilombero and Ulanga districts, both of which are located in the Morogoro region. In 2011, these HDSS altogether covered a population of approximately 370,000 people, 24% of which were women of reproductive ages. Details about these HDSS are available in further publications.21,22
Study design, sampling, and participants
This study was cross-sectional in design. The HDSS provided a sampling frame of households from which 2,183 households were randomly selected. The households were sampled using probability proportionate to size to ensure that the final sample is representative of each village in the study area. In these households 3,127 women were interviewed, and 2,643 of them who were aged 15+ years were selected for the current analysis because they had at least one sexual partner in the past 12 months preceding the survey. More details about this survey are available elsewhere.23
Variables and definition
The outcome or dependent variable for the current analysis was MSP in the past 12 months prior to the survey. This was derived from the original question which was “In the last 12 months how many sexual partners have you had (including your husband), if any?” Responses to this question were absolute numbers of the sexual partners reported, with acceptable values being positive integers: 0, 1, 2, 3, etc. Respondents who reported that they did not have any sexual partner (zero partners) (n=477, 15.3%) within the same period and those who did not answer the question (n=7, 0.2%) were excluded from the analysis because they were considered less pertinent to the research question. The resulting outcome variable was dichotomized into two categories – “no” or “yes,” with codes “0” and “1” used to represent the former and latter category respectively, such that,
Independent variables included in the analysis were age in years (<20, 20–29, 30–39, 40+), marital status (married, ever married, single), ethnicity (Pogoro, Ndengereko, Ngindo, Ndamba, Sukuma, Ngoni, Hehe, Bena, other), place of residence (urban, rural), education (no formal education, primary, secondary/higher), religion (Christian, Muslim, traditional/other), household socioeconomic status (poor, middle, rich), and district of residence (Rufiji, Kilombero, Ulanga). Household socioeconomic status was constructed using principal component analysis of household assets owned. This included toilet, type of toilet, and source of drinking water. Unfortunately, information regarding other household assets such as roofing material, wall material, floor material, etc that are conventionally included in determining household wealth status using principal component analysis were not available. Finally, all women were grouped in three categories of household wealth status as poor, middle, or rich according to their household wealth score.
Statistical analysis
Descriptive statistics were calculated using frequencies in one-way tabulations. This indicated distributional features of the data across the variables. Bivariate analysis was then conducted by cross-tabulating the outcome variable against each of the independent variables. Bivariate analysis was used to assess the degree of association between each pair of cross-tabulated variables using the Pearson chi-square test. Logistic regression was used to perform both univariate (regression model with one independent variable) and multivariate (regression model with more than one independent variable) analyses. In both cases, missing observations were excluded from the model. Multivariate logistic regression was performed to determine the independent predictors of MSP. Using the log-likelihood ratio test, a variable was selected for inclusion in the multivariate model if it was statistically significant at 5% that its presence improved the overall model.24 The model was also checked for statistical interactions and adequacy before being declared final. This was achieved using the Hosmer–Lemeshow goodness-of-fit test.24 Crude odds ratios, adjusted odds ratios (AOR), and their corresponding 95% confidence intervals (CIs) and P-values were all presented. The entire process of data analysis was conducted using Stata (version 11) statistical software and a significance level of 5% was used.
Ethical consideration
The primary survey received ethical approval from the Medical Research Coordinating Committee of the National Institute for Medical Research as well as from the Ifakara Health Institute’s institutional review board in Tanzania and the institutional review board of Columbia University, USA. All respondents participated in the survey voluntarily. Each participant signed an informed consent form prior to being interviewed. Completed questionnaires and consent forms were stored separately to ensure that the data remains anonymous.
Results
Profile of respondents
Data analysis pertained to 2,643 women who were aged 30.5 years on average (standard deviation =9.3), ranging from 15 to 63 years. Almost three-quarters (74.4%) of the women were married and 69.3% had primary education. Half (50.6%) of the respondents were Muslim while Christians amounted to 46.0% of the total participants. In terms of district of residence, Kilombero held the majority of the respondents (62.9%). Furthermore, 80.9% of the respondents resided in rural settings and the rest resided in urban or suburban areas (Table 1).
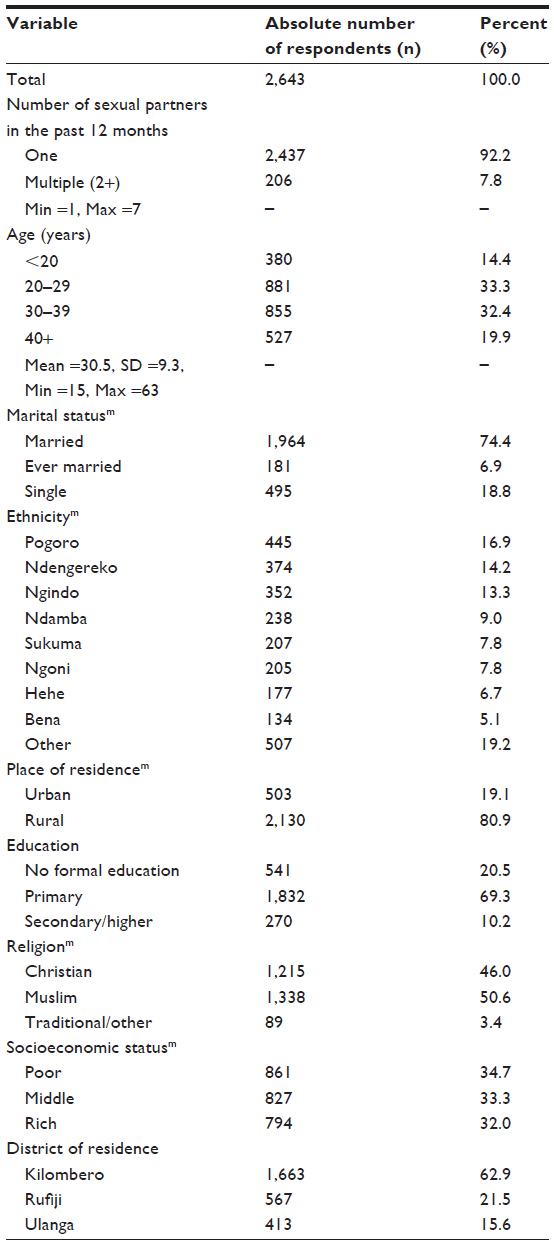 | Table 1 Sample characteristics (n=2,643) |
MSP by background characteristics
Overall, the number of sexual partners reported ranged from 1 to 7, with 7.8% of the women reporting MSP in the past 12 months preceding the survey. This proportion varied significantly by some characteristics of the respondents. The proportion of women reporting MSP was highest at 10.5% among youngest women (<20 years) and declined as age advanced to as low as 4.2% among women who were aged 40+ years (P<0.001). As such, a test for trend of MSP across ordered age groups showed significant findings (P<0.001). While 5.8% of married women reported MSP, 14.4% of women who were ever married (currently divorced or widowed) and 13.5% of women who were single reported MSP (P<0.001). With respect to religion, MSP was 8.8% among Muslims, 7.0% among Christians, and 2.3% among those following traditional or other unspecified beliefs (P=0.03) (Table 2). These observations were also in agreement with those reported in univariate models in Table 3.
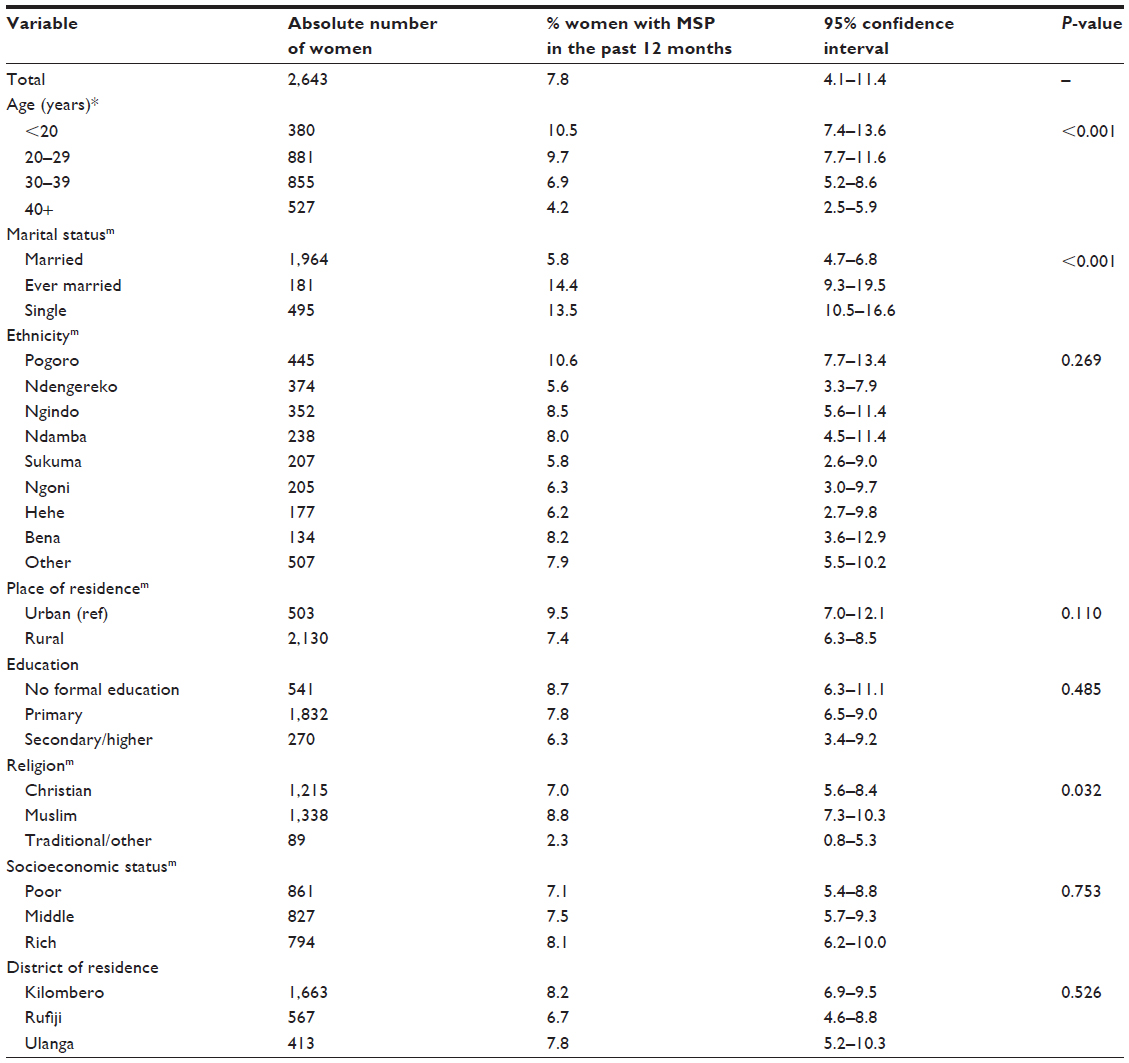 | Table 2 Percent distribution of MSP among women by background characteristics (n=2,643) |
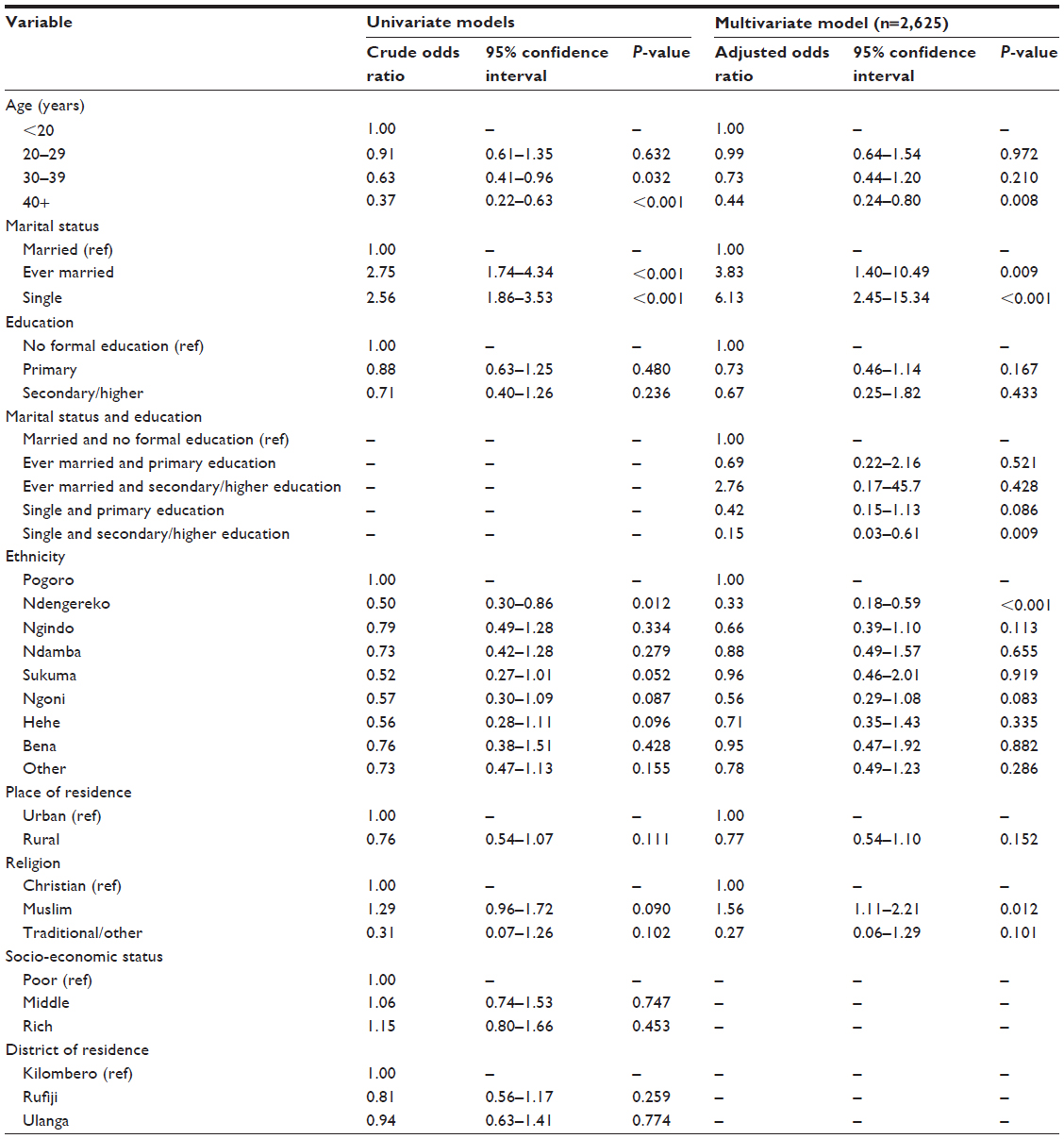 | Table 3 Univariate and multivariate logistic regression analysis of factors associated with multiple sexual partnerships among women in three rural districts of Tanzania, 2011 |
Multivariate analysis
Results of the multivariate logistic regression analysis of factors associated with MSP are presented in Table 3. They show that as age increased, the odds of MSP declined generally, but significant differences were observed for women aged 40+ years. These women (age 40+ years) were 56% less likely compared to the youngest women (<20 years) to report MSP (AOR =0.44, 95% CI 0.24–0.80). MSP was significantly associated with marital status. Ever married women were almost three times more likely to have MSP compared to the married women (AOR =3.83, 95% CI 1.40–10.49). Similarly, women who were single were 6.13 times more likely to have MSP compared to the married women (AOR =6.13, 95% CI 2.45–15.34). The data showed further that there was a significant interaction between marital status and education; whereby single women with secondary or higher education were 85% less likely to have MSP compared to married women with no education (AOR =0.15, 95% CI 0.03–0.61). Ethnicity was also important, where the adjusted odds of MSP was generally lower in all ethnic groups compared to the Pogoro ethnic group, and was significantly lower among Ndengereko women compared to the Pogoro women (AOR =0.33, 95% CI 0.18–0.59). With respect to religion, the results showed that Muslim women were 56% more likely to have MSP compared to Christian women (AOR =1.56, 95% CI 1.11–2.21).
However, MSP was not significantly associated with the socioeconomic status of the household, the place of residence (rural/urban), and district of residence.
Discussion
Given the enormous impact of the HIV/AIDS pandemic in Tanzania and the notable role of sexual behaviors in its spread,2 this analysis assesses the extent and drivers of MSP among women in Rufiji, Kilombero, and Ulanga districts of Tanzania. It should be borne in mind that sexual relationships with multiple partners are associated with an increased risk of transmission and acquisition of STIs including HIV/AIDS infection among others.25,26 This study shows that overall 8% of the women in the study area have had MSP in the past 12 months. This proportion is twice as high as that reported in the 2011 Tanzania Demographic and Health Survey report.27 This might have been due to the fact that even within Tanzania, this proportion varies by location, as it was as low as 2.0% in the northern zone and as high as 8.6% in the southern zone of the country.2 This observation is fairly similar to the prevalence observed in Lesotho, where MSP among women in the last 12 months is 6% according to the Lesotho Demographic and Health Survey.28 However, our observation was very high relative to statistics from other African countries such as Uganda,29 Kenya,30 Malawi,31 Zambia,32 and Nigeria.33 A study in Mpumalanga, South Africa among pregnant women found that the prevalence of MSP was 20%.34 These variations suggest that the magnitude of MSP depends on the context at hand because populations differ in several aspects including locations, cultures, values, beliefs, norms, and practices.
A number of determinants of MSP among women in the three districts of Tanzania were identified. Marital status was the most pervasive driver of MSP, with ever married and single women showing much higher risk for MSP than those currently married. It may be that currently unmarried women (either single or ever married) feel insecure without a husband or at least a permanent sexual partner or simply a potential husband. Therefore, apart from commercial sex workers, there is an obvious chance that before a woman finds her most preferred partner, she will be particularly susceptible to MSP on the course of finding one. One study confirms that outside marital union, women have a very high-risk period to contract HIV infection,3 which could be due to MSP. In marriage, women likely become secure and settled, thus they are better able to avert risky sexual behaviors including MSP. However, further studies are still needed to clearly reveal underlying mechanisms of the observed relationship. Therefore, social and behavioral interventions should particularly target unmarried women with partner reduction strategies. Outside marital union, abstinence remains the most reliable method against transmission or acquisition of STIs including HIV.35
This study found further that the chances of MSP declined as age advanced, particularly 40 years or above. This observation is in agreement with other studies, which have also observed that younger age is a risk factor for multiple partnerships,36–38 and has therefore been associated with an inclination toward longer-term, monogamous relationships at older ages.38 Additionally, it has been pointed out that adolescents typically engage in fleeting sexual relationships, which consequently make them more likely than their adult counterparts to have sex with multiple partners, thus placing them at a greater risk of contracting HIV/AIDS and other STIs.39
Interestingly, as higher levels of education were achieved, the odds of MSP declined generally, but significant only among single women with secondary or higher education. This suggests the need to promote and support women’s formal education – preferably at secondary level or beyond – to enhance their self-esteem, confidence, capability to make decisions, and freedom of expression40 regarding their choices in sexual relationships.23 In addition, a recent study in this population reveals that education beyond primary school improves condom use.23 Therefore, unmarried women in the study area are likely to change their risky sexual behaviors in favor of protective behaviors such as limiting the number of sexual partners and using condoms if their formal education is enhanced. Education is known to be a catalyst for change in gender relations as well as safer sex options.40,41 However, in other places such as Uganda,29 it has been noted that MSP among women increases as education enhances.
Ethnic differences in the odds of MSP were observed, with the Ndengereko ethnic group exhibiting lower risk than Porogo. The risk in other ethnic groups was also lower compared to the one observed among the Pogoro women, but the differences were not statistically significant. Also Muslim women had an elevated risk of MSP over Christian women. Although this points to the possibility of cultural or attitudinal differences in perceptions, beliefs, and practices in sexually-related matters, underlying mechanisms for these observations are less clear. Therefore further investigations, particularly qualitative studies, may be needed to understand contexts fostering this observation. Such research would also reveal knowledge, attitudes, values, beliefs, and practices concerning sexual relationships and partnerships in the study area.
Limitations
Some variables which have been shown in similar studies to be determinants of MSP such as the extent of sexual satisfaction between partners, sexual networks, substance abuse, and alcohol abuse were not available for inclusion. Also it should be noted that questions related to sexual behavior are sensitive. Therefore reporting bias may have occurred as some respondents might have underreported their actual number of sexual partners in the past 12 months. However, possible biases were minimized by recruiting experienced young (mostly aged 18 to 30 years) male and female enumerators who had at least secondary education and underwent rigorous 2-week training on the questionnaire and later on by conducting a pilot survey among respondents who were similar to those who participated in the main survey. The pilot findings helped refinement of the tool and selection of the best enumerators after which field data collection commenced and lasted for 2 months.
Causal inferences may not be drawn from these findings due to the “snapshot” nature of cross-sectional studies. In addition, these results are not generalizable nationally or beyond since only three districts within Tanzania were included.
Conclusion
Eight percent of women aged at least 15 years in Rufiji, Kilombero, and Ulanga districts of Tanzania are engaged in MSP. While both single and ever married women are more likely than their married counterparts to report MSP, only single women with at least secondary education have significant less chance for MSP compared to married women with no education. This suggests that promoting formal education at secondary level or beyond could be a sound strategy for sexual partner reduction among single women. Furthermore, although the odds of MSP generally decline as age advances, women aged 20 to 39 years are not significantly different from women <20 years of age. Muslim women as well as women belonging to the Pogoro ethnic group are more likely to engage in MSP in the study area. These groups should be targeted by interventions focused on partner reduction.
Acknowledgments
Connect Project which collected these data is funded by the Doris Duke Charitable Foundation (DDCF) and Comic Relief. A version of the abstract of this manuscript was accepted for presentation as a poster at the STI and AIDS World Congress, July 14–17, 2013 in Vienna, Austria. However, for some reasons the abstract was not presented at the congress. The abstract was later published in the journal Sexually Transmitted Infections.42 It was a requirement that all accepted abstracts for that Congress – even if not presented – would be published in this journal.
We are greatly thankful to the District councils of Rufiji, Kilombero, and Ulanga and the communities from which the data were collected. Field data collectors, field supervisors, and all the participants are especially acknowledged for the role each one played to make the survey a success. Special appreciations are extended to Anna Larsen of Columbia University for proofreading the manuscript.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interests in this work.
References
Joint United Nations Programme on HIV/AIDS, World Health Organization. AIDS Epidemic Update. Geneva: World Health Organization; 2007. Available from: http://data.unaids.org/pub/EPISlides/2007/2007_epiupdate_en.pdf. | |
Lema LA, Katapa RS, Musa AS. Knowledge on HIV/AIDS and sexual behaviour among youths in Kibaha District, Tanzania. Tanzan J Health Res. 2008;10(2):79–83. | |
Bellan SE, Fiorella KJ, Melesse DY, Getz WM, Williams BG, Dushoff J. Extra-couple HIV transmission in sub-Saharan Africa: a mathematical modelling study of survey data. Lancet. 2013;381(9877):1561–1569. | |
World Health Organization. The World Health Report 2002. Reducing Risks, Promoting Healthy Life. Geneva: World Health Organization; 2002. Available from: http://wwwlive.who.int/entity/whr/2002/en/whr02_en.pdf. Accessed September 8, 2014. | |
HIV and AIDS in Tanzania [webpage on the Internet]. West Sussex, UK: AVERT. Available from: http://www.avert.org/hiv-aids-tanzania.htm. Accessed September 8, 2014. | |
Tanzania Commission for AIDS (TACAIDS), Zanzibar AIDS Commission (ZAC), National Bureau of, Statistics (NBS), Office of the Chief Government Statistician (OCGS), ICF International. Tanzania HIV/AIDS and Malaria Indicator Survey 2011–2012. Dar es Salaam, Tanzania: TACAIDS, ZAC, NBS, OCGS, and ICF International; 2013. Available from: http://dhsprogram.com/pubs/pdf/AIS11/AIS11.pdf. Accessed September 8, 2014. | |
Tanzania Commission for AIDS (TACAIDS), Zanzibar AIDS Commission (ZAC, National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), Macro International Inc. Tanzania HIV/AIDS and Malaria Indicator Survey 2007–2008. Dar es Salaam, Tanzania: TACAIDS, ZAC, NBS, OCGS, and ICF International Inc.; 2008. Available from: http://dhsprogram.com/pubs/pdf/AIS6/AIS6_05_14_09.pdf. Accessed September 8, 2014. | |
UNAIDS. AIDSinfo [webpage on the Internet]. Geneva: UNAIDS. Available from: http://www.unaids.org/en/dataanalysis/datatools/aidsinfo/. Accessed September 8, 2014. | |
UNAIDS. UNAIDS World AIDS Day Report|2012. Geneva: UNAIDS; 2013. Available from: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2012/gr2012/JC2434_World AIDSday_results_en.pdf. Accessed September 8, 2014. | |
Shipena J, Khuruses F. Multiple and Concurrent Sexual Partnerships in Namibia: A Target Audience Research Report. Desert Soul; 2008. Available from: http://desertsoul.org/wp-content/uploads/2011/10/Multiple-Concurrent-Partnerships-in-Nambia-2008-final.pdf. Accessed September 8, 2014. | |
Van den Borne F. Trying to Survive in Times of Poverty and AIDS: Women and Multiple Partner Sex in Malawi. Amsterdam: Het Spinhuis; 2005. | |
Chiwaya W. Bar Girls study in Mangochi District: NACP/District AIDS Coordination; In: Bar Girls Study in Mangochi District: NACP/District AIDS Coordination. Lilongwe: International Eye Foundation; 1995. | |
Chaima M. Knowledge, Attitudes, Beliefs and Behaviour Regarding the Sexual Activities of Girls in T/A Kalolo, Lilongwe District, Malawi. Lilongwe: AIDS Secretariat; 1994. | |
Forster PG. Prostitution in Malawi and the HIV/AIDS Risk. Nord J Afr Stud. 2000;9(1):1–19. | |
Forster PG. AIDS in Malawi: contemporary discourse and cultural continuities. Afr Stud. 2001;60(2):245–261. | |
Chirwa WC. Migrant labour, sexual networking and multi-partnered sex in Malawi. Health Transit Rev. 1997;7(Suppl 3):5–15. | |
Chirwa WC. Sexually transmitted diseases in colonial Malawi [webpage on the Internet]. Popline. Available from: http://www.popline.org/node/531147. Accessed September 8, 2014. | |
Msolomba T, Chirwa WC. The Changing Faces of Prostitution and Transactional Sex in Malawi: Bangwe Township, Blantyre. Chancellor College; 2009. | |
Multiple Sexual Partner and HIV [webpage on the Internet]. HIV Symptoms. Available from: http://hivsymptomsonline.com/multiple-sexual-partner-and-hiv.html. Accessed September 8, 2014. | |
Chirwa WC, Chizimbi S. Multiple and Concurrent Sexual Partnerships in Malawi: A Formative Qualitative Study. Brighton, UK: Eldis; 2009. Available from:http://www.eldis.org/vfile/upload/1/document/1106/Multiple%20and%20concurrent%20sexual%20partnerships%20in%20Malawi.pdf. Accessed September 8, 2014. | |
Ifakara Health Research and Development Centre. Ifakara HDSS, Tanzania. Tanzania: Ifakara Health Research and Development Centre. Available from: http://www.indepth-network.org/leadership/IFAKARA%20HDSS.pdf. Accessed September 8, 2014. | |
Tanzania Ministry of Health, Tanzania Essential Health Interventions Project, Adult Morbidity and Mortality Project. Rufiji DSS Tanzania. Available from: http://www.indepth-network.org/dss_site_profiles/rufiji.pdf. Accessed September 8, 2014. | |
Exavery A, Kanté AM, Jackson E, et al. Role of condom negotiation on condom use among women of reproductive age in three districts in Tanzania. BMC Public Health. 2012;12:1097. | |
Vittinghoff E, Glidden DV, Shiboski SC, McCulloch CE. Regression methods in biostatistics: linear, logistic, survival, and repeated measures models. In: Gail M, Krickeberg K, Samet J, Tsiatis A, Wong W, editors. Statistics for Biology and Health. New York, USA: Springer Science + Business Media, Inc.; 2005. | |
Sundas B. HIV and AIDS in Darjeeling: Emerging Socio-Political Challenge. New Delhi: Concept Publishing Company; 2011. | |
Rector RE, Johnson KA, Noyes LR, Martin S. The Harmful Effects of Early Sexual Activity and Multiple Sexual Partners Among Women: A Book of Charts. Washington, DC: The Heritage Foundation; 2003. | |
National Bureau of StatisticsTanzania, ICF Macro. Tanzania Demographic and Health Survey 2010. Dar es Salaam, Tanzania: NBS and ICF Macro; 2011. Available from: http://dhsprogram.com/pubs/pdf/FR243/FR243%5B24June2011%5D.pdf. Accessed September 9, 2014. | |
Ministry of Health and Social Welfare (MOHSW) [Lesotho], ICF Macro. Lesotho Demographic and Health Survey 2009. Maseru, Lesotho: MOHSW and ICF Macro; 2010. Available from: http://dhsprogram.com/pubs/pdf/FR241/FR241[NEW_completeHHQst_3March2012].pdf. | |
Uganda Bureau of Statistics (UBOS), ICF International Inc. Uganda Demographic and Health Survey 2011. Kampala, Uganda: UBOS and Calverton, Maryland: ICF International Inc.; 2012. Available from: http://dhsprogram.com/pubs/pdf/FR264/FR264.pdf. | |
Kenya National Bureau of Statistics (KNBS), ICF Macro. Kenya Demographic and Health Survey 2008–2009. Calverton, Maryland: KNBS and ICF Macro; 2010. Available at: http://dhsprogram.com/pubs/pdf/FR229/FR229.pdf. Accessed September 9, 2014. | |
National Statistical Office (NSO), ICF Macro. Malawi Demographic and Health Survey 2010. Zomba, Malawi, and Calverton, Maryland, USA: NSO and ICF Macro; 2011. Available from: http://dhsprogram.com/pubs/pdf/FR247/FR247.pdf. | |
Central Statistical Office (CSO), Ministry of Health (MOH), Tropical Diseases Research Centre (TDRC), University of Zambia, Macro International Inc. Zambia Demographic and Health Survey 2007. Calverton, Maryland, USA: CSO and Macro International Inc.; 2009. Available from: http://dhsprogram.com/pubs/pdf/FR211/FR211[revised-05-12-2009].pdf. | |
National Population Commission (NPC) [Nigeria], ICF Macro. Nigeria Demographic and Health Survey 2008. Abuja, Nigeria: National Population Commission and ICF Macro; 2009. Available from: http://dhsprogram.com/pubs/pdf/fr222/fr222.pdf. | |
Peltzer K, Mlambo G. Sexual HIV risk behaviour and associated factors among pregnant women in Mpumalanga, South Africa. BMC Pregnancy Childbirth. 2013;13:57. | |
Exavery A, Lutambi AM, Mubyazi GM, Kweka K, Mbaruku G, Masanja H. Multiple sexual partners and condom use among 10–19 year-olds in four districts in Tanzania: what do we learn? BMC Public Health. 2011;11:490. | |
Yan H, Chen W, Wu H, et al. Multiple sex partner behavior in female undergraduate students in China: a multi-campus survey. BMC Public Health. 2009;9:305. | |
Santelli JS, Brener ND, Lowry R, Bhatt A, Zabin LS. Multiple sexual partners among US adolescents and young adults. Fam Plann Perspect. 1998;30(6):271–275. | |
Rotermann M. Sex condoms and STDs among young people. Health Rep. 2005;16(3):39–45. | |
Seidman SN, Mosher WD, Aral SO. Women with multiple sexual partners: United States, 1988. Am J Public Health. 1992;82(10):1388–1394. | |
Dominic B. “Women”s education a tool of social transformation’-a historical study based on Kerala society. Int J Sci Eng Res. 2011;2:1–7. | |
World Economic Forum. Women’s Empowerment: Measuring the Global Gender Gap. Geneva: World Economic Forum; 2005. Available at: http://www.weforum.org/pdf/Global_Competitiveness_Reports/Reports/gender_gap.pdf. Accessed September 9, 2014. | |
Exavery A, Kanté AM. Women’s socio-demographic drivers to sexual multi-partnerships in rural Tanzania [webpage on the Internet]. Abstract prepared for STI and AIDS World Congress, July 14–17, 2013, Vienna, Austria. Sex Transm Infect. 2013:89:A330. Available from: http://sti.bmj.com/content/89/Suppl_1/A330.1.full.pdf+html?sid=1787166a-10e8-4163-9e3e-2fe0c182e047. Accessed September 9, 2014. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.