")
Back to Journals » Patient Preference and Adherence » Volume 8
Single-arm, observational study of the ease of use of a redesigned pen device to deliver recombinant human follicle-stimulating hormone (follitropin alfa) for assisted reproductive technology treatment
Authors Illingworth P, Lahoud R, Quinn F, Chidwick K, Wilkinson C, Sacks G
Received 22 November 2013
Accepted for publication 12 March 2014
Published 5 June 2014 Volume 2014:8 Pages 813—826
DOI https://doi.org/10.2147/PPA.S58046
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Peter J Illingworth,1 Robert Lahoud,1 Frank Quinn,1 Kendal Chidwick,2 Claire Wilkinson,2 Gavin Sacks1
1IVFAustralia, Greenwich, Sydney, NSW, Australia; 2Scientific Affairs, Merck Serono Australia Pty Ltd, Frenchs Forest, Sydney, NSW, Australia
Purpose: Evaluation of patients’ ease of use of the redesigned, disposable, ready-to-use follitropin alfa pen during controlled ovarian stimulation for assisted reproductive technology.
Methods: This single-center, observational, open-label, single-arm study recruited infertile normo-ovulatory women (aged 18–45 years). Nurses trained patients to self-administer recombinant human follicle-stimulating hormone daily using the follitropin alfa pen (300 IU, 450 IU, and 900 IU). Before treatment, patients completed Questionnaire A. Following self-administered treatment, on stimulation days 5–6 and 7–8 (within a day of receiving recombinant human chorionic gonadotropin), patients completed Questionnaire B. Nurses completed an ease-of-learning/teaching questionnaire. The primary endpoint was proportion of patients rating the pen as “easy/very easy” to use (Questionnaire B) on the final visit before recombinant human chorionic gonadotropin. Secondary endpoints included: proportion of patients rating the follitropin alfa pen as easy to learn, use, prepare, deliver, and dispose of (Questionnaires A and B). Proportions (95% confidence intervals [CIs]) were provided for primary and secondary endpoints. Adverse events were reported descriptively.
Results: Eighty-six patients received recombinant human follicle-stimulating hormone.
Of the 72 patients who had completed the overall assessment questions, 66 (91.7%; 95% CI =82.7%–96.9%) found the pen “easy” to use. Also, 70/86 (81.4%) patients “strongly agreed/agreed” that, overall, it was easy to learn how to use the pen; 72/86 (83.7%) “strongly agreed/agreed” that easily understandable, verbal information was provided; and 70/86 (81.4%) were confident about using the pen correctly. In total, 24/26 nurses (92.3%; 95% CI =74.9%–99.1%) rated the pen as easy to use. Clinical pregnancy rate/patient/cycle/embryo transfer was 37%. Twenty-six ovarian hyperstimulation syndrome events were reported (none severe; 16 patients [19%]); of these, 13 occurred at embryo transfer.
Conclusion: In this observational study, patients had a high acceptance of the redesigned follitropin alfa pen, with most finding it very easy/easy to use. Assisted reproductive technology nurses found the pen very easy/easy to teach.
Keywords: controlled ovarian stimulation, ease of learning, ease of teaching, prefilled pen, questionnaire, self-injection
Introduction
Controlled ovarian stimulation (COS) using gonadotropins is a key component of assisted reproductive technology (ART).1 During COS, daily injections of recombinant human follicle-stimulating hormone (r-hFSH) result in exogenous FSH levels being maintained above the threshold for follicle development for several days, and this allows multiple follicles to develop and multiple oocytes to be retrieved.2 Individual responses to COS are highly variable,3,4 and an excessive response is associated with ovarian hyperstimulation syndrome (OHSS), a rare and potentially life-threatening condition.5 As individual patient responses to COS vary, the starting dose of r-hFSH required by patients should be individualized.3,5 There may also be a need to adjust the r-hFSH dose used for a particular patient once treatment has started.
In the past, FSH was available as a lyophilized formulation in glass ampoules or vials and was administered subcutaneously using syringes.6,7 These conventional delivery systems were designed for administration by a health care professional, friend, or family member, or they could be self-administered. The option of self-administration has the key advantages of convenience and self-sufficiency, requiring fewer clinic visits.7
To enable easier and more convenient self-administration, liquid formulations of r-hFSH, such as follitropin alfa and follitropin beta, have been developed for administration using pen devices.6 In a prospective, open-label study, women found that using a prefilled pen for r-hFSH self-administration during ovulation induction was less stressful and easier to use than conventional ampoules plus syringe.8 Furthermore, in a prospective, open-label survey, markedly more women (undergoing ovulation induction or ART) expressed a preference for a pen injection device over a needle-free reconstitution and conventional syringe.9 Also, in a randomized, open-label study, women undergoing COS for ART found that, compared with a conventional syringe, self-injection with a pen device was easier, less painful, and more convenient.7
The follitropin alfa pen (GONAL-f® Prefilled Pen, 300 IU, 450 IU, and 900 IU; Merck Serono SA, Geneva, Switzerland, a subsidiary of Merck KGaA, Darmstadt, Germany) is a redesigned, disposable, ready-to-use pen containing follitropin alfa for injection and is designed for subcutaneous self-administration by women undergoing COS for ART. The redesigned follitropin alfa pen has a number of features that the “original” pen does not: for example, small dose increments of 12.5 IU, graduated markings on the cartridge reservoir showing approximate units remaining, and a dose display that returns to zero when the full dose has been administered;6 consequently, it is important to ensure that patients find the redesigned pen easy to use and are able to accurately self-administer their treatment. The primary objective of the present study was to evaluate Australian patients’ perceptions of the ease of use of the redesigned r-hFSH (follitropin alfa) pen. Other objectives included evaluations of function, reliability, ease of teaching and learning with the follitropin alfa pen, and to assess health care providers’ perceptions of the ease of use of the pen.
Material and methods
Study design
This was a single-center, observational (non-interventional), Phase IV, open-label, single-arm study in ART (Merck Serono identification number: EMR 700623-529; Merck Serono protocol number: RH090). Three clinic sites were involved (Bondi Junction, Greenwich, and Westmead; NSW, Australia); however, as these clinics are part of the same center (IVFAustralia, Sydney, NSW, Australia) and use the same guidelines for protocols and procedures, this was considered to be a single-center study.
The study was conducted in accordance with the ethical principles stated in the Declaration of Helsinki and the National Health and Medical Research Council statement. The study protocol was approved by the independent ethics committee (IVFAustralia Human Research and Ethics Committee). Written, informed consent was obtained from patients prior to study start.
A study monitor visited the study sites regularly as part of the data quality assurance procedures.
Patients
Normo-ovulatory women aged 18–45 years undergoing a first, second, third, or fourth cycle of ART with an indication for in vitro fertilization (IVF) or intracytoplasmic sperm injection were recruited. Patients were required to have a regular, spontaneous menstrual cycle of 21–35 days, both ovaries, a normal uterus, a body mass index (BMI) of <30 kg/m2, and an early follicular phase (cycle days 2–4) serum FSH level of ≤20 IU/L. A further inclusion criterion was availability of normal sperm (or sperm previously obtained through surgical procedures) that was adequate for performing IVF or intracytoplasmic sperm injection according to the center’s standard criteria.
Key exclusion criteria included: anti-Müllerian hormone (AMH) level >40 pmol/L in the 6 months prior to study treatment; previous severe OHSS; polycystic ovary syndrome (according to the Rotterdam criteria);10 endometriosis and/or uterine myoma requiring treatment; ≥3 miscarriages; clinically significant systemic disease; and clinically significant abnormal hematology, chemistry, or urinalysis results at screening.
Nurses (both study nurses and general clinic nurses) involved in the care of patients participating in the study were recruited to complete the nurse questionnaire towards the end of the patient recruitment period; this ensured that they had trained at least one patient. There were no specific inclusion criteria for nurses.
Training
Nurses were trained by the Merck Serono Key Account Manager, as per normal practice, when the redesigned pen was launched. This training included a formal presentation with a step-by-step guide, diagrams, and information about how the pen had changed from the previous version. If any nurses were unavailable at this time, then the Nurse Unit Manager at IVFAustralia ensured they were trained. During training, nurses could practice with demonstration devices. In addition, nurses who were retained at the clinics could refer to training materials.
Patients were instructed by nurses on how to use the redesigned pen. In addition, patients were provided with written instructions (patient information and an injection mat).
Assessments and interventions
At screening, laboratory samples were obtained for routine hematology, chemistry, urinalysis, and hormone level determinations. Blood samples were analyzed locally to assess AMH and early follicular phase FSH levels. During screening (after enrollment), patients were trained by their nurses on how to use the redesigned follitropin alfa pen.
Following a negative pregnancy test result, patients underwent a single ART treatment cycle, started within 2 months following the screening visit. Follitropin alfa was self-administered subcutaneously daily using the redesigned pen. The investigator decided the starting dose of follitropin alfa, which was dosed according to the standard clinical practice (and within the approved label) from stimulation day 1 until the required criterion for recombinant human chorionic gonadotropin (r-hCG) administration was met (≥3 follicles, ≥17 mm). From stimulation day 5 or 6, the dose could be increased or decreased on the basis of the patient’s ovarian response and according to the center’s standard practice. Follicular development was monitored according to the center’s standard practice by transvaginal ultrasound (US) and/or estradiol levels. Once r-hCG criterion had been met, a single 250 μg r-hCG injection was administered to induce final oocyte maturation. Patients were withdrawn from the study if they experienced a lack of ovarian response (defined as the development of ≤3 follicles of ≥12 mm after at least 7 days of follitropin alfa treatment).
Pituitary downregulation was achieved with either the gonadotropin-releasing hormone (GnRH) agonist long protocol or the GnRH antagonist protocol as per the center’s standard protocol. Oocytes were retrieved vaginally under US monitoring 34–38 hours after r-hCG administration. Oocyte pick-up, IVF, embryo transfer (ET), and luteal support were performed as per the center’s standard practice.
To evaluate compliance with treatment, patients were consulted by the clinic nurse and the daily r-hFSH dose was recorded.
Ease of use
Patients evaluated various aspects relating to the ease of use of the redesigned follitropin alfa injection pen by completing two questionnaires. Following training on how to use the new pen and before the start of treatment (either during the screening period or the day before starting treatment), patients completed Questionnaire A (Figure S1). Questionnaire B (Figure S2) was completed by patients on days 5–6 and 7–8 of r-hFSH stimulation and also at the end of stimulation (within a day of r-hCG administration). Questionnaires were completed independently without clinic personnel involvement; once completed, patients placed them in a dedicated, locked box. The box could only be opened by the study monitor who sent the questionnaires for database entry. Confidentiality was maintained and no responses were known by clinic personnel.
At the end of recruitment, the teaching nurses completed a questionnaire (Questionnaire C; Figure S3) on the ease of learning to use the pen and the ease of teaching how to use it.
Safety
Data on adverse events (AEs) were collected throughout the study. The possible causality, in the investigator’s opinion, of an AE in relation to study treatment was also recorded.
A posttreatment, safety follow-up evaluation was performed at the last study visit for all patients who had received r-hCG; for nonpregnant patients, this evaluation occurred when the pregnancy diagnosis test was conducted (post r-hCG day 15–20), and for pregnant patients this occurred when the US to confirm clinical pregnancy was conducted (post r-hCG day 35–42). Patients who withdrew from the study at any time and received at least one dose of follitropin alfa had their post-treatment safety visit 15–20 days after the last follitropin alfa administration.
Outcomes
Primary endpoint
The primary endpoint was the proportion of patients rating the follitropin alfa injection pen as “easy” or “very easy” to use for self-injection based on a user questionnaire (Questionnaire B), which was completed at the final monitoring visit before r-hCG administration.
Secondary endpoints
Secondary endpoints included the proportion of patients rating the redesigned follitropin alfa injection pen (Questionnaires A and B) as easy to learn, easy to use, easy to prepare for injection, easy to deliver the injection, and easy to dispose of after completing the injection. Other secondary endpoints included the proportion of nurses rating the redesigned follitropin alfa pen in a Nurse Questionnaire (Questionnaire C) as easy to learn, easy to use, and easy to teach.
Other (tertiary) endpoints included total dose of follitropin alfa used, mean daily dose of follitropin alfa used, biochemical pregnancy rate, clinical pregnancy rate, cycle cancelation prior to r-hCG, and the incidence of multiple pregnancies.
Safety endpoints included the incidence and severity of treatment-emergent AEs (TEAEs; according to their relationship to ART treatment in general), including OHSS. The incidences of early onset OHSS (occurring during stimulation and up to 9 days after r-hCG administration and oocyte retrieval) and late-onset OHSS (occurring on or after 10 days after r-hCG administration and oocyte retrieval) were recorded. In addition, injection tolerability was evaluated from the general AE data.
Statistical analysis
The intent-to-treat (ITT) population was used to summarize and analyze the primary, secondary, and other endpoints. The ITT population was defined as all patients who received at least one dose of follitropin alfa and who had at least one postbaseline efficacy measurement (dose of follitropin alfa or completed questionnaire). The safety population (all patients who received at least one dose of follitropin alfa) was used to evaluate safety data, follitropin alfa dose, and the rate of cycle cancellation prior to r-hCG.
All data were made anonymous prior to analysis. Table 1 presents the specific questions used from each of the three questionnaires for the primary and secondary endpoints and the visit at which they were answered. The primary efficacy measure in this study was obtained from Questionnaire B completed at the end of follitropin alfa stimulation. If a patient had not completed Questionnaire B at this visit, the day 7–8 Questionnaire B data were used. At least 50% of questions required for an efficacy measure were needed to provide a valid estimate. A sensitivity analysis including those results based on <50% of questions was also undertaken. For Questionnaire C, if a nurse had >50% unanswered responses for the questions for an endpoint then these data were not included in the analysis for that endpoint.
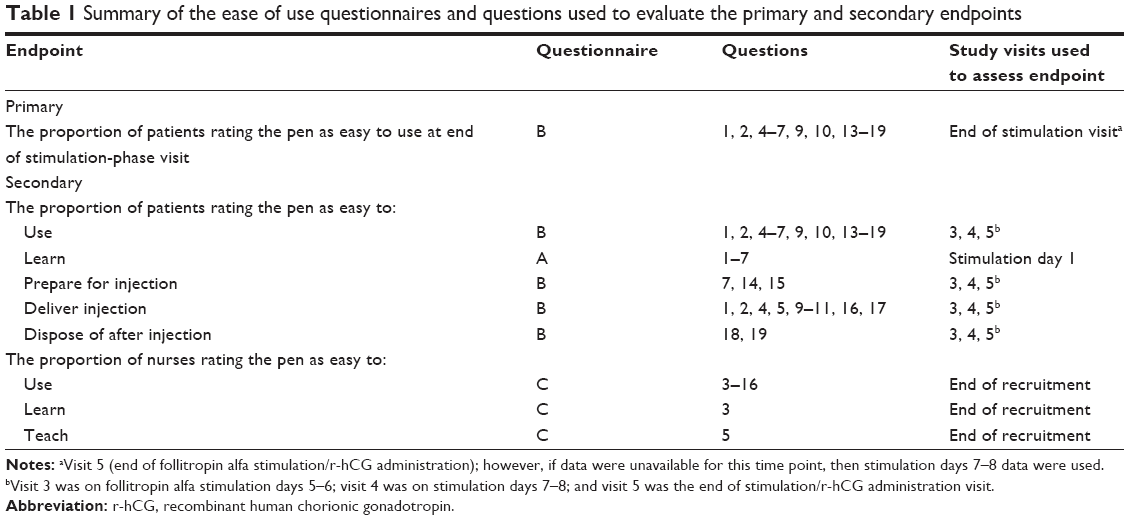 | Table 1 Summary of the ease of use questionnaires and questions used to evaluate the primary and secondary endpoints |
The primary and secondary endpoints were presented as a proportion with 95% confidence intervals (CIs). For other endpoints, quantitative variables were summarized by the number of patients (n), mean, standard deviation (SD) and range; qualitative variables were summarized by frequency and percentage of patients; rates were summarized by the numerator, denominator, rate, and its 95% CI. Descriptive statistics only were provided for AE data.
Sample size
A sample size of 100 patients treated for one ART cycle was determined based on the precision of the 95% CI for the primary endpoint (the proportion of patients rating the pen as “easy” or “very easy” to use) as this was a single-arm study. Under this approach, no statement of power was required and alpha =0.05 was used as the CI specified as 95%.
A sample size of 100 patients produces a two-sided 95% CI with a width that differs depending on the assumed proportion. For example, if the proportion is 0.50 (or 50%) and n=100 patients, the 95% CI will be 0.40 to 0.60, a width of 0.2; whereas if the proportion is as high as 0.85 the confidence interval will be 0.77 to 0.91, a width of 0.14.
Changes to the statistical section of the protocol
Originally, the protocol indicated that the endpoints (eg, ease of use, ease of learning, ease of preparation) for the follitropin alfa pen would be obtained from a response of “easy” or “very easy”; this implied that only one question would be used to assess each endpoint. The questionnaires used contained multiple questions addressing each endpoint; hence, a modification was made to the process used to classify a patient’s response as “easy”.
Results
The study was conducted in Australia between March 31, 2011 and February 9, 2012.
Patients
A total of 100 patients were screened and enrolled in the study. Fourteen patients failed screening (eligibility violation, n=4; withdrew consent, n=9; other, n=1); 86 attended the prescheduled first day of stimulation (Figure 1) and thus received r-hFSH treatment and were included in the safety population. All 86 patients in the safety population were included in the ITT population (n=86). To achieve pituitary downregulation, the GnRH agonist long protocol was used for 20 patients and the GnRH antagonist protocol was used for 66 patients.
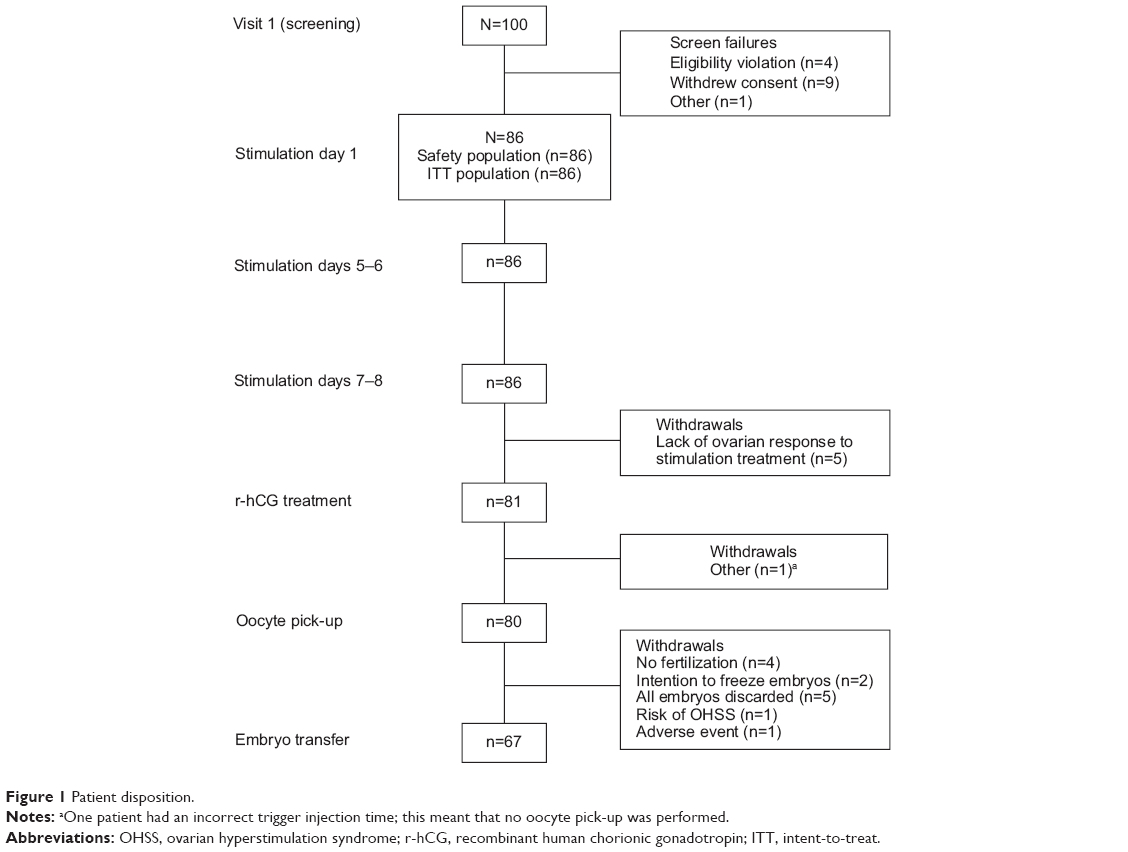 | Figure 1 Patient disposition. |
Patient demographics and other characteristics are given in Table 2. Some patients had protocol deviations relating to the study inclusion/exclusion criteria; for example, three patients were later discovered to have had more previous ART cycles than stipulated in the eligibility criteria. However, as the inclusion/exclusion deviations were considered not to impact the primary or secondary endpoints relating to Questionnaire B, no patients were excluded from the analyses because of such deviations.
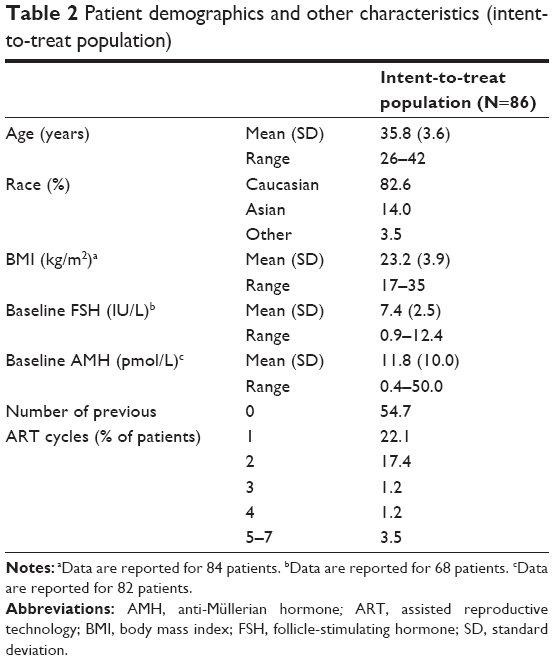 | Table 2 Patient demographics and other characteristics (intent-to-treat population) |
Questionnaire completion
Questionnaire A was completed by 77/86 patients in the ITT population. Questionnaire B was completed by 55 patients on the last day of follitropin alfa stimulation and by 18 patients on day 7–8 of stimulation. Therefore, responses from 73 patients were used for the overall “ease of use” assessment. However, not every patient responded to every question. A total of 26 nurses completed Questionnaire C.
Ease of use
Primary endpoint
Of the 72 patients who had completed the overall assessment questions, 66 (91.7%; 95% CI =82.7%–96.9%) found the pen easy to use overall (Figure 2).
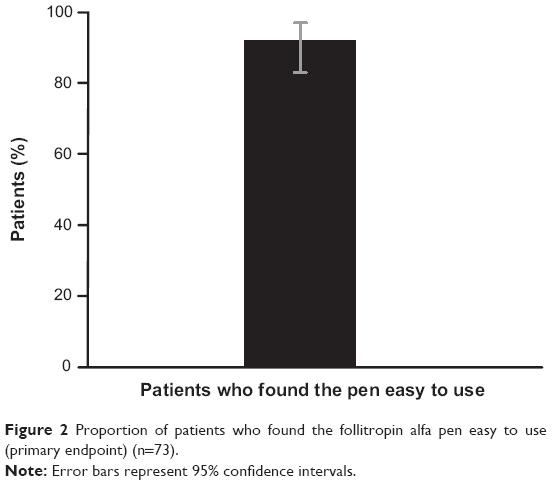 | Figure 2 Proportion of patients who found the follitropin alfa pen easy to use (primary endpoint) (n=73). |
Responses to key questions from Questionnaire B that were used in the primary endpoint are shown in Figure 3.
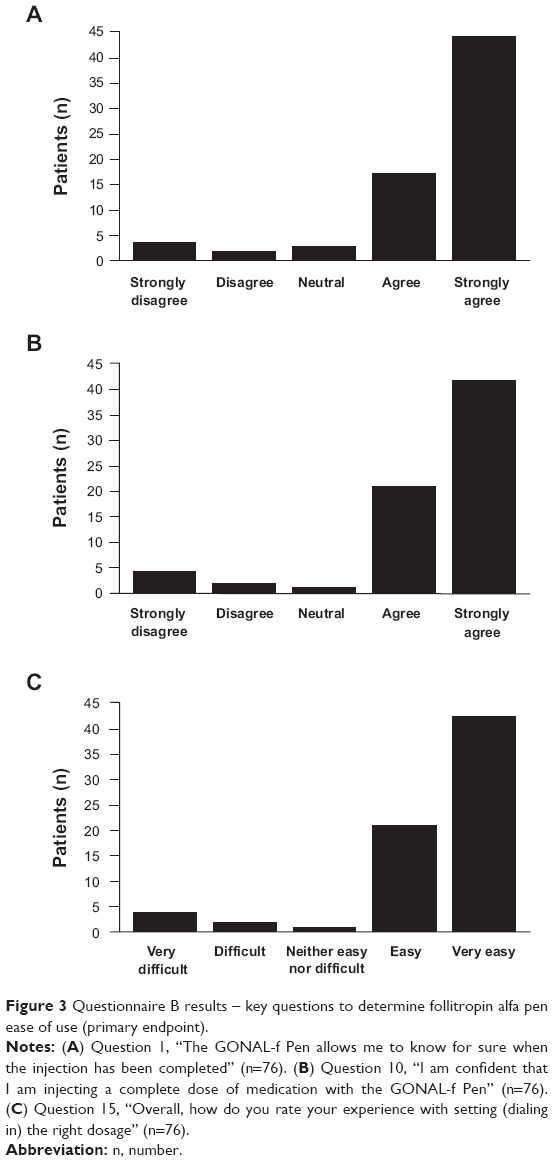 | Figure 3 Questionnaire B results – key questions to determine follitropin alfa pen ease of use (primary endpoint). |
Secondary endpoints
Easy to learn – Questionnaire A
Responses regarding previous experience showed that the majority of patients (50/86, 65.8%) had never used injections/injectable medications prior to the study. There were 17/86 patients (22.4%) who had used >10 injections/injectable medications within the last 12 months.
Most patients (70/76, 92.1%) strongly agreed or agreed that, overall, it was easy to learn how to use the pen. In addition, 72/76 patients (93.5%) strongly agreed or agreed that easily understandable verbal information was provided, and 70/76 patients (92.1%) were confident about using the pen correctly after training.
Easy to use (by visit)
Figure 4 shows the percentage of patients by visit who classified the pen as easy to use.
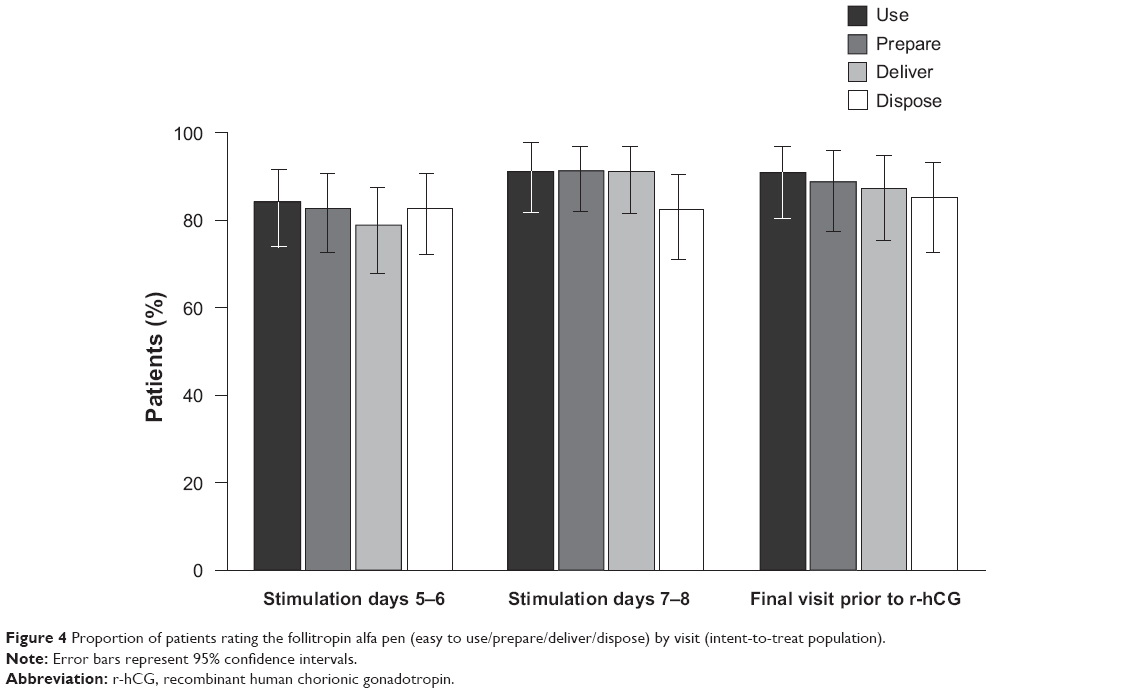 | Figure 4 Proportion of patients rating the follitropin alfa pen (easy to use/prepare/deliver/dispose) by visit (intent-to-treat population). |
At days 5–6 of follitropin alfa stimulation, the pen was classified as easy to use by 64/76 patients (84.2%). At days 7–8 and at the last day of follitropin alfa stimulation (or within a day of r-hCG stimulation) the pen was classified as easy to use by 62/68 (91.2%) and 50/55 (90.9%) of patients, respectively.
Easy to prepare for injection
At the three visits, the pen was classified as easy to prepare for injection by 83%–91% of patients (Figure 4).
Easy to deliver the injection
The proportion of patients who considered that it was easy to deliver an injection using the pen was slightly lower at days 5–6 of follitropin alfa stimulation (78.9%) than at the two later visits (91.2% and 87.3%; Figure 4).
Easy to dispose of after completing the injection
The proportion of patients who considered that it was easy to dispose of the pen was similar at all three visits (82%–85%; Figure 4).
Sensitivity analysis
The sensitivity analysis (based on results where <50% of Questionnaire B questions were answered) found only minor differences in percentages compared with the main analysis, where at least 50% of questions required for an efficacy measure were needed to provide a valid estimate.
Nurses’ experience and perceptions
The nurses had previous ART experience ranging from 4 months to 30 years (mean [SD] =6.1 [6.4] years). Furthermore, 18 nurses (69.2%) were familiar with vials and syringes, 19 (73.1%) with ampoules and syringes, 25 (96.2%) with nonreturnable pens, and 18 (69.2%) with returnable pens. The mean (SD; range) number of patients trained by a nurse was 5.9 (6.6; 1–25).
Overall, the pen was rated as easy to use by 24/26 nurses (92.3%; 95% CI =74.9%–99.1%). All 26 nurses (100%) rated the pen as easy to learn and easy to teach. In addition, all 26 nurses (100%) thought the follitropin alfa pen was: “very easy” or “easy” to learn; “very simple” or “simple” to prepare for first use; and “very easy” or “easy” to teach to patients. Furthermore, 25/26 nurses (96.2%) found it “very simple” or “simple” to dial the correct dose. However, only 5/26 (19.2%) found it easy to read the dosing scale.
All 26 nurses (100%) experienced “no” or “very little” confusion while using the pen, were “very satisfied” or “satisfied” with the time to administer and the time to teach, were “confident” that the dose had been injected, found the patient information and patient support material “very useful” or “useful”, and found the patient information and patient support material “not confusing at all” or had “no opinion”.
In addition, compared with other injection procedures, 22/26 nurses (84.6%) found “much less” or “less” potential for errors during setting the dose, and 19/25 (76.0%) found “much less” or “less” potential for errors during preparation for the injection.
Other endpoints
The mean (SD) of follitropin alfa used was 2,593 IU (1,540.8 IU) for the total dose and 233 IU (99.1 IU) for the daily dose (safety population).
In total, 25/86 patients (29%; 95% CI =20%–40%) had a biochemical pregnancy confirmed by serum β-hCG pregnancy test (safety population). In those patients who underwent ET (n=67), this equated to a 37% (95% CI =26%–50%) biochemical pregnancy rate. All biochemical pregnancies were confirmed as clinical pregnancies by US (ie, clinical pregnancy and biochemical pregnancy rates were the same). Therefore, the clinical pregnancy rate per patient and per ET was 37% (95% CI =26%–50%).
Two women had preclinical miscarriages (defined as a spontaneous cessation of a biochemical pregnancy; no fetal sac/heart detected by US on post r-hCG day 35–42). The treatment cycle was cancelled prior to r-hCG administration in three patients (safety population). In addition, four women had multiple pregnancies.
Compliance
No doses of follitropin alfa were reportedly missed by any patient.
Safety
A total of 30 patients reported at least one TEAE. There were two patients who reported a serious TEAE: one ectopic pregnancy requiring hospitalization, dilation, and curettage, and one case of urinary retention requiring hospitalization. There were no deaths during the study.
Sixteen patients (19%) had at least one event of OHSS. In total there were 26 OHSS events reported: none were severe, six events were moderate (reported by 5 patients [6%]) and 20 events were mild (reported by 13 patients [15%]). Of the 26 OHSS events reported, one occurred at stimulation day 5–6, three at stimulation day 7–8, four at oocyte pick up, 13 at embryo transfer, and five at study end. Ten patients experienced one OHSS event, three patients experienced two OHSS events, two patients experienced three OHSS events, and one patient experienced four OHSS events. At least one OHSS event classified as early onset was reported by 14 patients and five patients had at least one OHSS event classified as late onset.
There were no recorded incidents of injection intolerability (as assessed from the general AE summaries).
Discussion
Pen devices for the self-injection of medicines aim to provide patients with a convenient and easy-to-use option for self-medication. The design of any new pen device should facilitate accurate self-administration of medication, while also providing ease of use benefits. This single-arm, observational study demonstrated that, overall, the majority (92%) of patients found a redesigned follitropin alfa pen easy to use. Furthermore, although a large proportion of patients had never used an injection or injectable device previously, most (81%) found that it was easy to learn how to use the pen. Importantly, a high proportion of patients found that the verbal information provided was easy to understand and were confident about using the pen following training. Therefore, clinicians can be reassured that their patients should be able to use the pen easily and confidently.
In the present study, over time, slightly more patients rated the pen as easy to use (90.9% at the end of follitropin alfa stimulation [within a day of r-hCG administration] compared with 84.2% at days 5–6). This finding suggests that increased familiarity with the pen may make it easier to use. However, as this was observed for only a small number of patients, it does not suggest a need for extended or increased training of patients prior to their first use of the pen.
Evaluation of patients’ use of a newly designed injection pen is important as an assessment of safety. Ease of preparation for injection and ease of delivery of an injection assess how well patients can self-administer the r-hFSH dose. Furthermore, evaluation of the ART nurses’ perceptions of the pen – in terms of dialing the correct dose, confusion while using the pen, potential for errors when setting the dose, and potential for errors during preparation for the injection – also provides valuable insights into aspects of safety.
The findings from the present study indicate that there are no major concerns with the redesigned pen in terms of the above issues relating to safety. However, only 19.2% of nurses found it easy to read the dosing scale on the pen, an issue that may merit further review.
The redesigned follitropin alfa pen is part of a family of pens with a common design concept and similar operating system.11 These pens were developed to simplify the process of gonadotropin self-administration,11 for both the patient and those who teach patients this method. The redesigned pen has enhanced features, such as graduated markings on the cartridge reservoir showing approximate units remaining and that the dose can be dialed up and down.6 In addition, the dosing accuracy of the pen has been confirmed.6
Two initial studies exploring the use of the follitropin alfa pen by patients and nurses were conducted using simulated injections (and so were not evaluating injections during an actual ART cycle). In the first, a market research study in infertile patients and infertility nurses, the authors reported that the redesigned follitropin alfa pen was easy to learn, easy to teach how to use, and well accepted.12 The second, a noninterventional usability study, found no major concerns regarding the risk of misuse or dosing errors, and no unexpected operational risks,13 suggesting that correct dosage and proper use of the follitropin alfa pen device by the patient will be likely in practice.
The rate of clinical pregnancies per ET (37%) reported here was as expected and is consistent with previously published data. For example, clinical pregnancy rates of 36%–41% were reported in an Australian study of women receiving r-hFSH for COS.14
In this study, r-hFSH injections were generally well tolerated; there were no reports of injection intolerability. The majority of OHSS events reported in this study were mild; no severe OHSS events were reported and no patients were hospitalized due to OHSS. The incidence of mild or moderate OHSS events reported here was higher than would normally be expected with r-hFSH treatment for COS.15 It is difficult to establish why this occurred. One possible explanation is that relatively high r-hFSH doses were utilized: the mean daily dose was 233 IU (all r-hFSH doses were determined by the investigator and daily doses could have been higher than the recommended initial 150–225 IU dose) and the mean total dose of r-hFSH was 2,593 IU, which is higher than that observed in a previous study of r-hFSH for COS.16 Polycystic ovary syndrome, prior OHSS, high baseline AMH, and young age (<33 years) are recognized as risk factors for OHSS;5 of these, only young age could have been a possible contributory element in this study.
The strengths of the study include the population size, which allowed the detailed perceptions of a relatively large group of patients to be evaluated, and the use of the center’s standard guidelines for protocols and procedures, thereby reflecting real-life clinical practice. Furthermore, the study evaluated both nurse and patient perceptions; it is important to investigate the opinions of both the user (patients) and those teaching the user (ART nurses) so that a holistic view of the redesigned pen device may be obtained.
The limitations of the study include that it was an open-label, observational study and that the findings are limited to the population studied. The lack of a comparator arm is an additional limitation; however, the aim of the study was to evaluate Australian patients’ perceptions of the ease of use of the redesigned pen and not to compare injection devices. Another possible limitation is that data were obtained from women undergoing their first ART cycle (57% of enrolled patients had not had a previous ART cycle) as well as women who had experienced previous ART cycles. Although this may have introduced bias, as some patients had experience of gonadotropin injections used for ART, it also reflects the real-life clinical situation where patients present with different infertility histories. In addition, another potential limitation is that the three questionnaires used in this study have not been previously validated.
Conclusion
Overall, this single-arm, observational study found that COS with the redesigned pen (follitropin alfa, GONAL-f® Prefilled Pen) was effective and well tolerated. Furthermore, patients had a high level of acceptance for the redesigned pen, with most patients finding it “easy” or “very easy” to use during COS for ART. In addition, most ART nurses found the pen “easy” or “very easy” to teach. An injection device that is both easy to use and easy to teach provides a useful treatment option for both patients and health care professionals.
Acknowledgments
The authors thank Jane Early, Georgina Worthington, and Joanne Phillips of IVFAustralia for their contribution to the study as study nurses. The authors thank Jocelyn Woodcock and Lindsay Judge of Caudex Medical, Oxford, UK (supported by Merck Serono SA, Geneva, Switzerland, a subsidiary of Merck KGaA, Darmstadt, Germany) for their assistance in the preparation of this manuscript.
This study was sponsored by Merck Serono SA Geneva, Switzerland, a subsidiary of Merck KGaA, Darmstadt, Germany.
Author contributions
PJI, RL, FQ, and GS were study investigators and contributed to the study design, data analysis, manuscript drafting, and critical discussion. KC contributed to the study design, data analysis, manuscript drafting, and critical discussion. CW contributed to the study design, study monitoring, data analysis, manuscript drafting, and critical discussion. All authors have read and approved the final manuscript.
Disclosure
PJI has previously received travel grants from Merck Serono Australia Pty Ltd, Sydney, NSW, Australia. RL has had some conference sponsorship from Merck Serono Australia Pty Ltd. FQ has previously received travel grants from Merck Serono Australia Pty Ltd. KC was an employee of Merck Serono Australia Pty Ltd at the time of the study. CW was an employee of Merck Serono Australia Pty Ltd at the time of the study. GS has received travel grants for educational purposes from Merck Serono Australia Pty Ltd. The authors report no other conflicts of interest in this work.
References
Macklon NS, Stouffer RL, Giudice LC, Fauser BC. The science behind 25 years of ovarian stimulation for in vitro fertilization. Endocr Rev. 2006;27:170–207. | ||
Baird DT. A model for follicular selection and ovulation: lessons from superovulation. J Steroid Biochem. 1987;27(1–3):15–23. | ||
Bosch E, Ezcurra D. Individualised controlled ovarian stimulation (iCOS): maximising success rates for assisted reproductive technology patients. Reprod Biol Endocrinol. 2011;9:82. | ||
Yates AP, Rustamov O, Roberts SA, et al. Anti-Mullerian hormone-tailored stimulation protocols improve outcomes whilst reducing adverse effects and costs of IVF. Hum Reprod. 2011;26(9):2353–2362. | ||
Fiedler K, Ezcurra D. Predicting and preventing ovarian hyperstimulation syndrome (OHSS): the need for individualized not standardized treatment. Reprod Biol Endocrinol. 2012;10:32. | ||
Christen M, Schertz JC, Arriagada P, Keitel J, Müller H. The redesigned follitropin α pen injector for infertility treatment. Expert Opin Drug Deliv. 2011;8(6):833–839. | ||
Platteau P, Laurent E, Albano C, et al. An open, randomized single-centre study to compare the efficacy and convenience of follitropin beta administered by a pen device with follitropin alpha administered by a conventional syringe in women undergoing ovarian stimulation for IVF/ICSI. Hum Reprod. 2003;18(6):1200–1204. | ||
Somkuti SG, Schertz JC, Moore M, Ferrande L, Kelly E; Gonal-F Prefilled Pen in OI Study 24785 Group. Patient experience with follitropin alfa prefilled pen versus previously used injectable gonadotropins for ovulation induction in oligoanovulatory women. Curr Med Res Opin. 2006;22(10):1981–1996. | ||
Weiss N. Gonadotrophin products: empowering patients to choose the product that meets their needs. Reprod Biomed Online. 2007;15(1):31–37. | ||
Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004;19(1):41–47. | ||
Saunders H, Schertz JC, Hecker C, Lang B, Arriagada P. The recombinant human chorionic gonadotropin prefilled pen: results of patient and nurse human factors usability testing. Expert Opin Drug Deliv. 2012;9(8):893–900. | ||
Abbotts C, Salgado-Braga C, Audibert-Gros C. A redesigned follitropin alfa pen injector for infertility: results of a market research study. Patient Prefer Adherence. 2011;5:315–331. | ||
Schertz JC, Saunders H, Hecker C, Lang B, Arriagada P. The redesigned follitropin alfa pen injector: results of the patient and nurse human factors usability testing. Expert Opin Drug Deliv. 2011;8(9):1111–1120. | ||
Porter R, Kissel C, Saunders H, Keck C. Patient and nurse evaluation of recombinant human follicle-stimulating hormone administration methods: comparison of two follitropin injection pens. Curr Med Res Opin. 2008;24(3):727–735. | ||
Merck Serono Australia Pty Ltd. Product Information: GONAL-f® Pen. Frenchs Forest NSW, Australia: Merck Serono Australia Pty Ltd; 2014. Available from: https://www.ebs.tga.gov.au/ebs/picmi/picmirepository.nsf/pdf?OpenAgent&id=CP-2010-PI-03557-3. Accessed February 25, 2014. | ||
Popovic-Todorovic B, Loft A, Bredkjaeer HE, Bangsbøll S, Nielsen IK, Andersen AN. A prospective randomized clinical trial comparing an individual dose of recombinant FSH based on predictive factors versus a ‘standard’ dose of 150 IU/day in ‘standard’ patients undergoing IVF/ICSI treatment. Hum Reprod. 2003;18(11):2275–2282. |
Supplementary materials
The following questions ask about the GONAL-f® Prefilled Pen injection device you will be using as part of the research study.Please choose the most appropriate response.
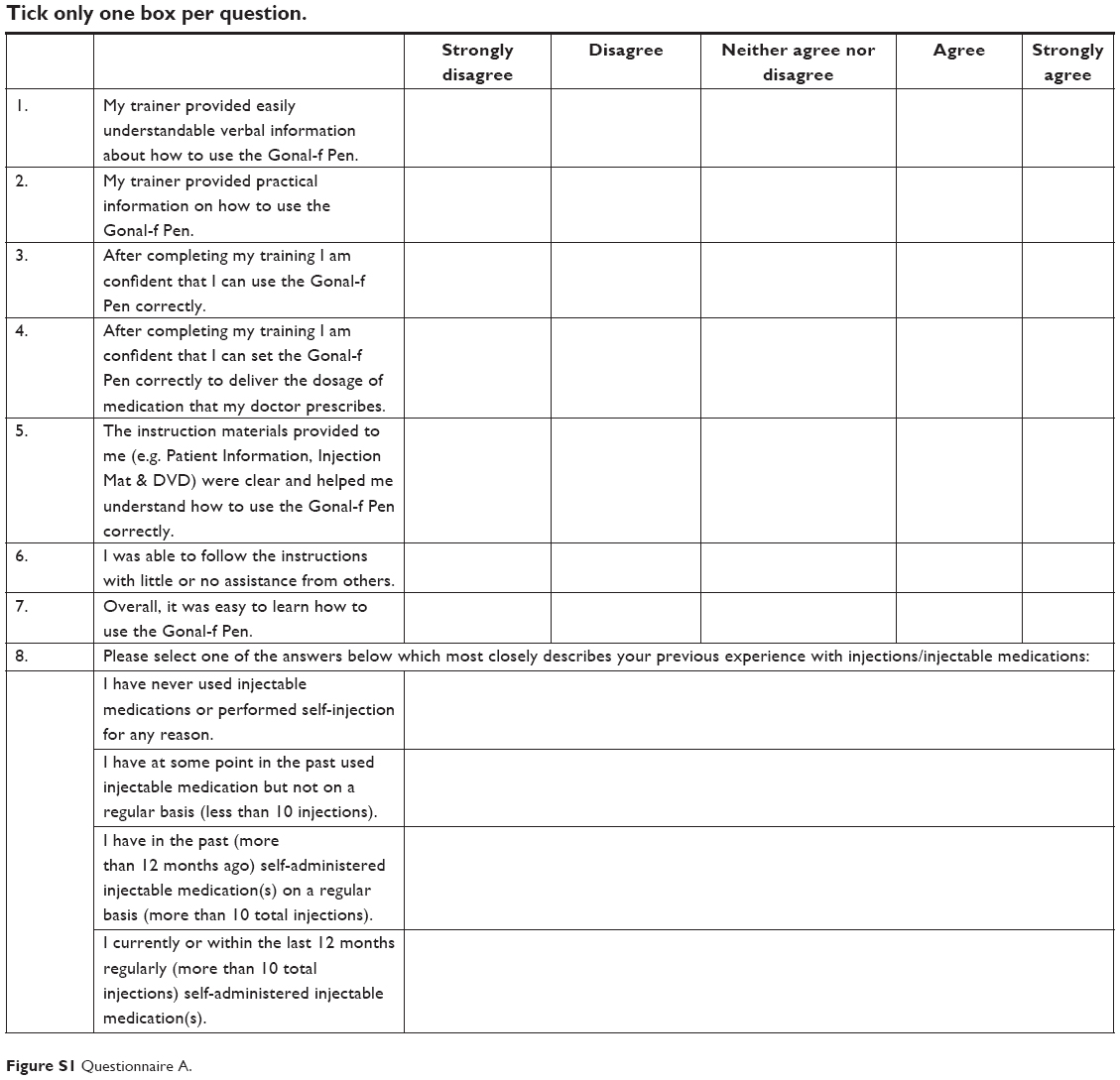 | Figure S1 Questionnaire A. |
The following questions ask about the GONAL-f® Prefilled Pen injection device you have been using as part of the research study. You should answer these questions based on your experience with the injection device you have been using. Thank you for your time in completing this questionnaire.
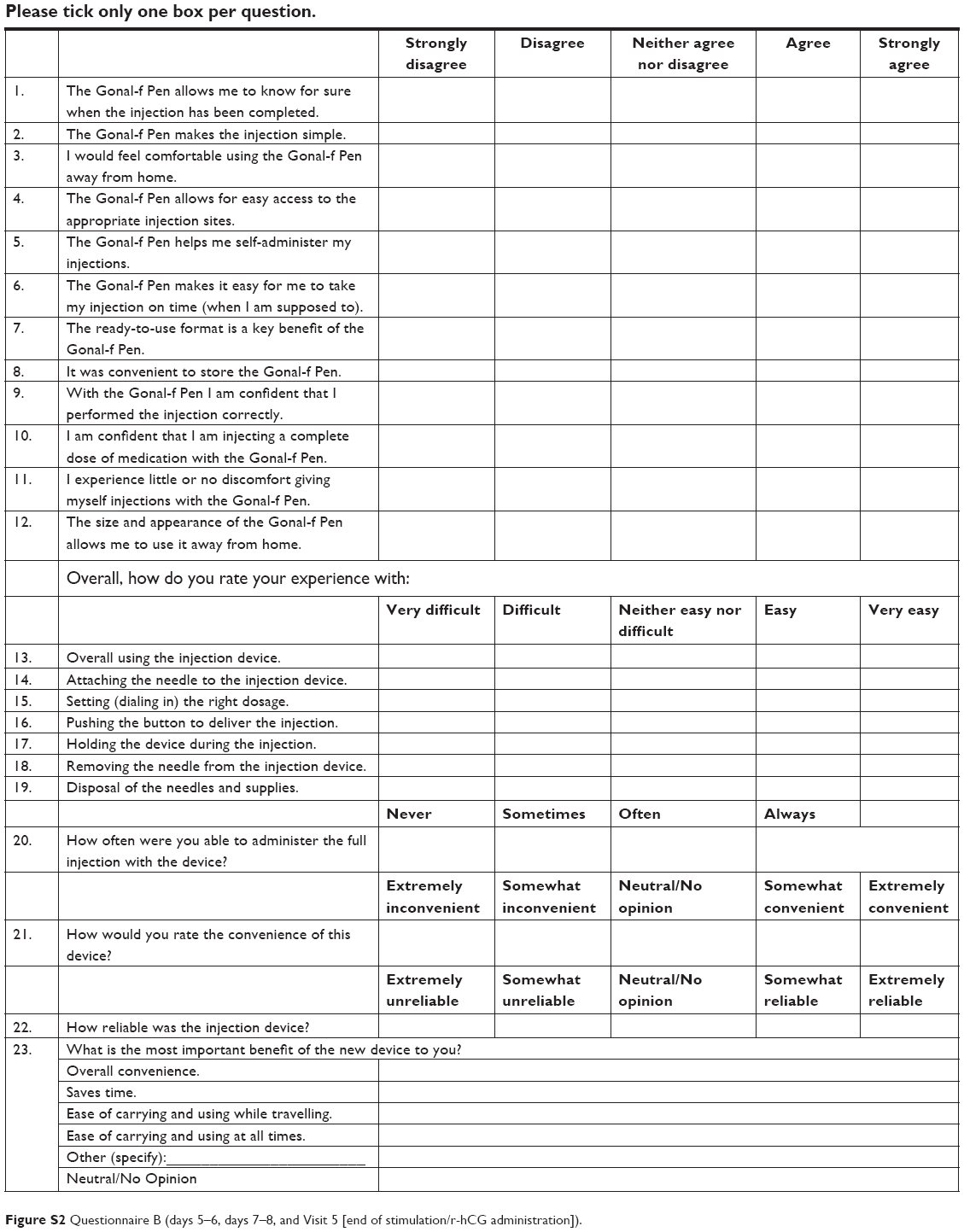 | Figure S2 Questionnaire B (days 5–6, days 7–8, and Visit 5 [end of stimulation/r-hCG administration]). |
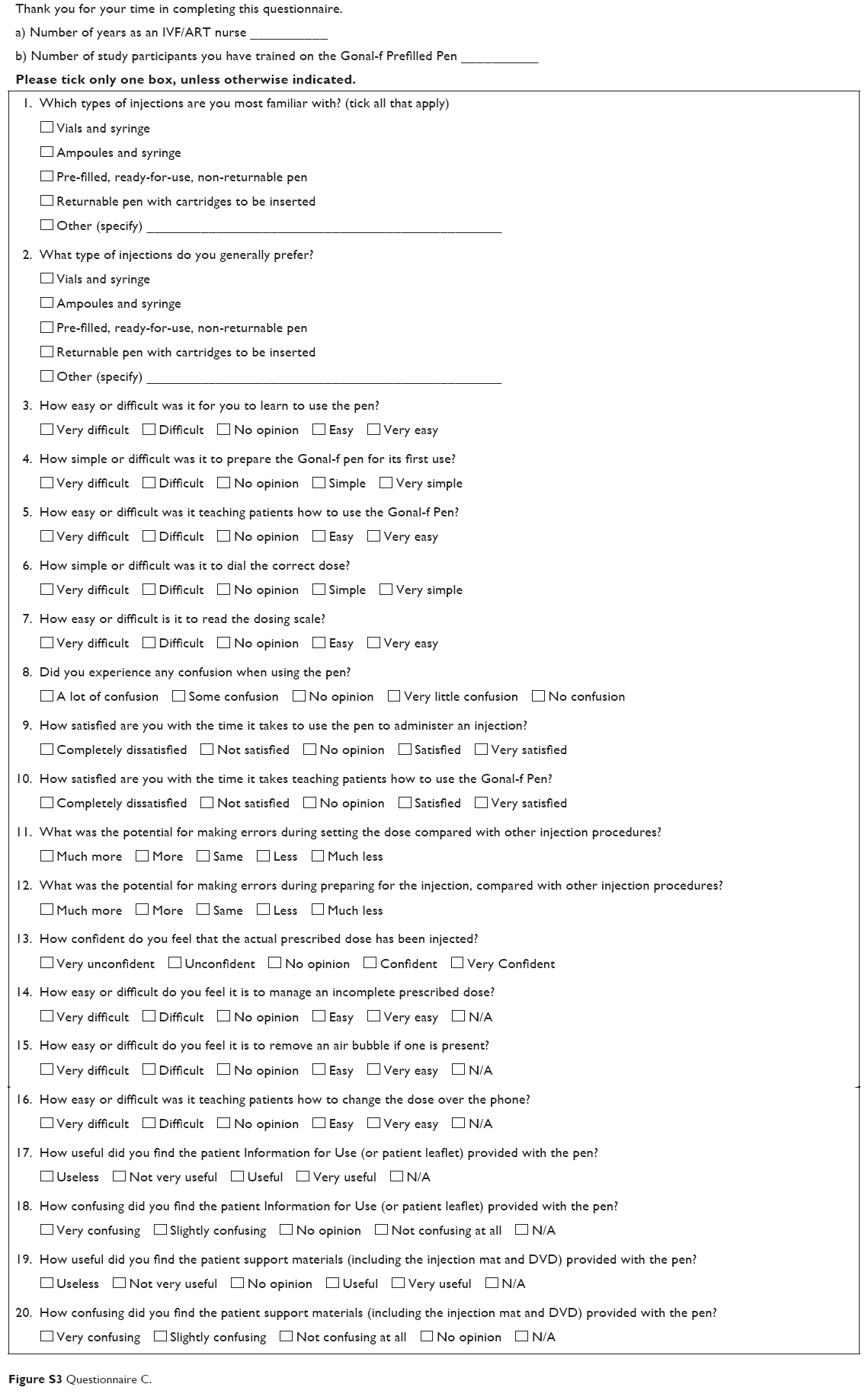 | Figure S3 Questionnaire C. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.