")
Back to Journals » Patient Preference and Adherence » Volume 8
Shared decision-making: the perspectives of young adults with type 1 diabetes mellitus
Authors Wiley J, Westbrook M, Greenfield J, Day R , Braithwaite J
Received 16 November 2013
Accepted for publication 13 December 2013
Published 2 April 2014 Volume 2014:8 Pages 423—435
DOI https://doi.org/10.2147/PPA.S57707
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Janice Wiley,1 Mary Westbrook,1 Jerry R Greenfield,2,3 Richard O Day,4 Jeffrey Braithwaite1
1Centre for Clinical Governance Research in Health, Australian Institute of Health Innovation, University of New South Wales, 2Diabetes and Obesity Program, Garvan Institute of Medical Research, 3Department of Endocrinology, St Vincent's Hospital, University of New South Wales, Sydney, NSW, Australia; 4Department of Clinical Pharmacology, St Vincent's Hospital, University of New South Wales, Sydney, NSW, Australia
Background: Shared decision-making (SDM) is at the core of patient-centered care. We examined whether young adults with type 1 diabetes perceived the clinician groups they consulted as practicing SDM.
Methods: In a web-based survey, 150 Australians aged 18–35 years and with type 1 diabetes rated seven aspects of SDM in their interactions with endocrinologists, diabetes educators, dieticians, and general practitioners. Additionally, 33 participants in seven focus groups discussed these aspects of SDM.
Results: Of the 150 respondents, 90% consulted endocrinologists, 60% diabetes educators, 33% dieticians, and 37% general practitioners. The majority of participants rated all professions as oriented toward all aspects of SDM, but there were professional differences. These ranged from 94.4% to 82.2% for "My clinician enquires about how I manage my diabetes"; 93.4% to 82.2% for "My clinician listens to my opinion about my diabetes management"; 89.9% to 74.1% for "My clinician is supportive of my diabetes management"; 93.2% to 66.1% for "My clinician suggests ways in which I can improve my self-management”; 96.6% to 85.7% for “The advice of my clinician can be understood”; 98.9% to 82.2% for “The advice of my clinician can be trusted”; and 86.5% to 67.9% for “The advice of my clinician is consistent with other members of the diabetes team". Diabetes educators received the highest ratings on all aspects of SDM. The mean weighted average of agreement to SDM for all consultations was 84.3%. Focus group participants reported actively seeking clinicians who practiced SDM. A lack of SDM was frequently cited as a reason for discontinuing consultation. The dominant three themes in focus group discussions were whether clinicians acknowledged patients' expertise, encouraged patients' autonomy, and provided advice that patients could utilize to improve self-management.
Conclusion: The majority of clinicians engaged in SDM. Young adults with type 1 diabetes prefer such clinicians. They may fail to take up recommended health services when clinicians do not practice this component of patient-centered care. Such findings have implications for patient safety, improved health outcomes, and enhanced health service delivery.
Keywords: shared decision-making, patient perspective, patient-centered care, patient autonomy, type 1 diabetes, young adults, health service delivery, glycemic control
Background
Shared decision-making (SDM) is a practice whose time has come. SDM is a consultation style that involves both the patient and the clinician sharing information and management options to reach agreement on treatment implementation.1–3 It is a core component of patient-centered care.4 Whilst patient-centered care has had various definitions,5 other elements considered essential include clinician consideration of patient needs and preferences,6–8 health literacy skills,6–8 and accessibility to health services.7,8
Across the USA, the UK, Europe, Canada, and Australia, there is an impetus to move to more patient-centered systems of care.2,3,5,9–14 Efforts to improve health service quality and safety, changing social attitudes, and an ethical imperative have been amongst the driving forces.2,3,5,9,15 In respect of diabetes health service provision, patient-centered systems of care have been associated with improved glycemic control,16,17 greater patient satisfaction,17,18 higher levels of patient well-being,18,19 increased patient engagement,17–19 and more provider satisfaction.19
SDM acknowledges patient expertise and preferences by incorporating the patient as an active partner alongside the clinician in defining appropriate medical management.2,3 This emerging ideology has particular relevance in chronic disease management where the need for collaborative, integrated, and accessible care aligns with patient engagement in forms of self-management.20 In keeping with societal shifts in consumer sovereignty and greater levels of individualization, the role of SDM might be better understood by a consideration of self-determination theory, which suggests that clinician consultation attitudes that inhibit patient autonomy may lead to poorer health outcomes.21 Self-determination theory has been shown to be applicable to an understanding of improved glycemic control in diabetes management.22 SDM might acknowledge the practical reality of equalizing rights and power in the health provider–patient relationship as well as empowerment of the patient in taking increasing responsibility for his or her own care.
Yet it appears that SDM may be an academic fiction rather than common practice. Active engagement of the patient in decision-making regarding management is often neglected2,3,23,24 despite evidence that the majority of patients want greater involvement in determining their own care.24–28 Such studies emphasize a growing disjunction between policy requirements signaling a more collaborative orientation to care decisions and traditional practice.
As the quintessential self-managed disease, type 1 diabetes mellitus is at the cutting edge of this ideological evolution. Type 1 diabetes is an autoimmune disease that necessitates lifelong insulin replacement therapy. Effective self-management of type 1 diabetes requires an ability to formulate algorithms for insulin replacement dependent upon a complex array of interactive physiological parameters.29–35 In circumstances where the patient must rely to some extent on the expertise of their own daily therapeutic decision-making, adherence to a didactically prescribed clinician management plan may leave the patient in an untenable position. Incorporation of SDM into a consultation results in a two-way flow of experiential knowledge between the clinician and the patient, and allows for identification of the barriers that may impede achievable treatment goals. SDM can be an effective method for both the patient and the health care provider to reach consensus on implementation of an effective treatment regimen.36
Young adults with type 1 diabetes are of particular interest because they have high attrition rates from health services37,38 and suffer worse health outcomes.37 Yet the use of patients’ perspectives as a driver for quality and safety improvements in health services is underdeveloped.39 This study seeks to address the research gap. We set out to explore the experience of SDM from the perspective of young adults with type 1 diabetes. We wanted to assess whether and to what extent factors fundamental to the process of SDM in multidisciplinary clinician care of type 1 diabetes are becoming manifest.
Materials and methods
Participants
The study population was a sample of Australian adults aged 18–35 years with type 1 diabetes. Participants were recruited from Australian diabetes consumer support organizations via advertisements on websites, e-newsletters, Facebook, and print journals in 2011. To obtain qualitative data, focus groups were conducted in all state capital cities except Hobart, with some participants travelling from regional areas. The University of New South Wales granted ethics approval (HREC 10395). All participants provided their individual informed consent. Age-limited inclusion criteria for the study were established because of the high attrition rates and poor health outcomes known to occur in this age group.37,38 Exclusion criteria were people with type 1 diabetes outside of the set age limits, those with type 1 diabetes not living in Australia, and carers of those with type 1 diabetes.
Survey
The quantitative component of the study consisted of a web-based, self-reported, cross-sectional survey of methods of diabetes self-management. The survey was available online from February to May 2011. A paper version of the survey was available but was not utilized by any respondent. The survey consisted of 96 questions that covered a comprehensive assessment of factors relevant to type 1 diabetes self-management although not all questions were relevant to every respondent. (For example, questions related to use of continuous insulin infusion devices were not relevant to respondents who used multiple daily injections.) The survey was developed in 2010 by the authors following a systematic literature review on type 1 diabetes self-management, because no available type 1 diabetes self-management assessment tools gave consideration to the role of new technologies. Following assessment of respondent demographic characteristics, the survey addressed questions related to modes, frequency, and evaluation of insulin delivery systems and blood glucose monitoring systems. The survey also explored respondents’ record-keeping, dietary management, insulin adjustment, and blood glucose target levels (including in the event of exercise, sick days, alcohol consumption), and identification and evaluation of health services and diabetes education accessed. The survey was piloted on a sample of four young adults with type 1 diabetes and ten health services workers and researchers. Recommended improvements were incorporated into the final version. A set of seven questions fundamental to SDM was included. These questions were modified from results of studies of SDM by the Commonwealth Fund, a private US foundation that aims to promote high-performing health care systems.40
Participants were asked to rate their interactions with each of the four types of clinicians in the multidisciplinary diabetes team that they consulted. The clinicians included were an endocrinologist, a diabetes educator (a specialist nurse with an accredited post-graduate certificate or diploma in diabetes education), a dietitian, and a general practitioner. Seven-point Likert scales with endpoints “agree” and “disagree” (mid-point “neutral”) were used for each of seven questions related to SDM. The questions rated were: my (clinician type specified) enquires about how I manage my diabetes; my (clinician) listens to my opinion about my diabetes management; my (clinician) is supportive of my diabetes management; my (clinician) suggests ways in which I can improve my self-management; the advice of my (clinician) can be understood; the advice of my (clinician) can be trusted; and the advice of my (clinician) is consistent with other members of the diabetes team.
Such questions sought participants’ perceptions of the two-way flow of information required for SDM to occur. For example, the question regarding the clinician’s enquiry about self-management examined whether the clinician had requested information regarding self-management skills from the patient. The question regarding the clinician listening to the patient asked whether from the patient’s perspective the clinician had taken account of that information. These facets of SDM stand in contrast to the questions regarding the provision of advice by the clinician. These questions sought to ascertain not only whether the clinician provided information but also whether it was in a format that could be utilized by the patient. The provision of inconsistent information or information that the patient did not trust might impact on patients’ perceptions of the two-way flow of information.
No specific time frame to limit when the consultation experience occurred was allocated in the survey. Although it is recommended care, questions related to consultation with a psychologist or social worker were not included due to the complexities of a therapeutic alliance.
Focus groups
To expand on the results of the survey, participants were invited by email to attend focus groups. Focus groups were conducted from May to August 2011. The focus group method was chosen because focus groups can stimulate participants to explore their own perceptions in ways that may not come to light in personal interviews.41 The focus groups had a semistructured format. Each facet of SDM, as detailed in the survey, was raised by way of an open-ended question asking the group to tell of their experiences in relation to that issue. The focus group discussion continued until content saturation was achieved. Interviews were electronically recorded and transcribed verbatim. The interviewer (JW) wrote notes after each meeting, reflecting on the principal matters discussed and recording the perceived feelings, emotions, and personal interactions of the participants.
Data processing and analysis
Only completed responses were incorporated into the data analysis. Quantitative analysis was undertaken using Statistical Package for the Social Sciences version 20 software (IBM Corporation, Armonk, NY USA). In reporting the survey results for the SDM questions, the three levels of agreement and disagreement were respectively combined whilst the neutral responses remained constant. A mean weighted average agreement for SDM across all clinicians was calculated. Sections of the survey also provided for free text responses. These responses were incorporated into the qualitative data generated by the focus groups.
The qualitative data were analyzed with the aid of the QRS NVivo 9 (QSR International, Doncaster, VIC, Australia) data analysis program for thematic content using a constant comparative method for emerging themes.42 Two health services researchers, a registered nurse (JL) and a registered medical practitioner (JW) with clinical experience in diabetes care, independently analyzed these results. Data were coded using stepwise thematic analysis. Recurring themes and subthemes were clustered and then condensed into overarching themes. Emerging qualitative themes and subthemes were compared with quantitative results for consistency. A third health services researcher (MW) analyzed the quantitative and qualitative data to check for thematic consistency and interpretative analysis. Exemplar quotes are presented using participants’ identifier codes, sex, age, and duration of diabetes.
Results
Survey
Of 167 commenced survey responses, 150 respondents completed all survey questions. This represented a survey response rate of 89.8%.
Demographic and clinical characteristics of survey participants
As shown in Table 1, 80% of the survey participants were female, 80% came from the eastern states (reflecting Australian population demographics), 68% were living in major cities, 79% had attained a tertiary education level, 64% were working full time, and 84% had private health insurance.
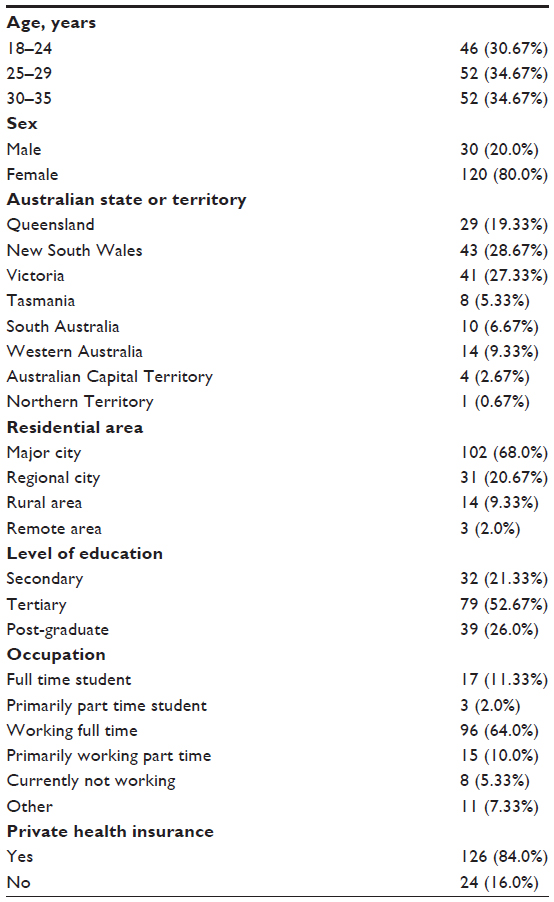 | Table 1 Demographic characteristics of 150 survey participants |
The clinical diabetes characteristics were self-reported. As shown in Table 2, 34% reported that their last hemoglobin A1c (HbA1c) was less than 7.0% (53 mmol/mol), 45% reported that their body mass index was in the normal range, 25.3% had a duration of diabetes of less than 5 years, and 39.3% had a duration of diabetes of greater than 15 years.
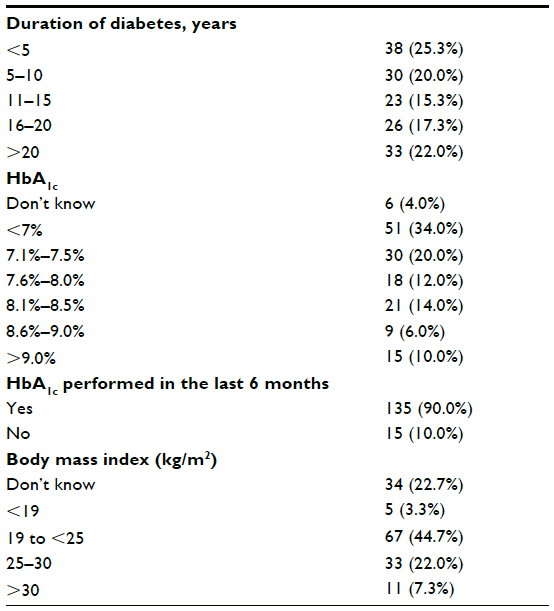 | Table 2 Clinical characteristics of 150 survey participants |
Consultation characteristics of survey participants
Of the 150 respondents, the numbers of participants who currently consulted with each type of clinician on the recommended diabetes care team were as follows: endocrinologists, 135 (90%); diabetes educators, 89 (60%); dieticians, 50 (33%); and general practitioners, 56 (37%). Two percent of our respondents did not currently consult with any clinician. On average, respondents consulted 2.3 types of clinicians.
Survey results
Overall, the participants affirmed that the majority of clinicians in the four professions demonstrated SDM on all seven aspects of decision-making that were investigated. Totaled participant affirmative, negative, and neutral responses respectively to questions related to SDM are shown in Table 3. Comparing the ratings given to individual facets of SDM, the highest average agreement was that the advice of clinicians could be trusted at 89.5%; the advice could be understood at 89.4% and that clinicians enquired about how patients manage their diabetes at 87.0%. The lowest agreement (77.0%) was with the proposition that advice from multidisciplinary team clinicians was consistent.
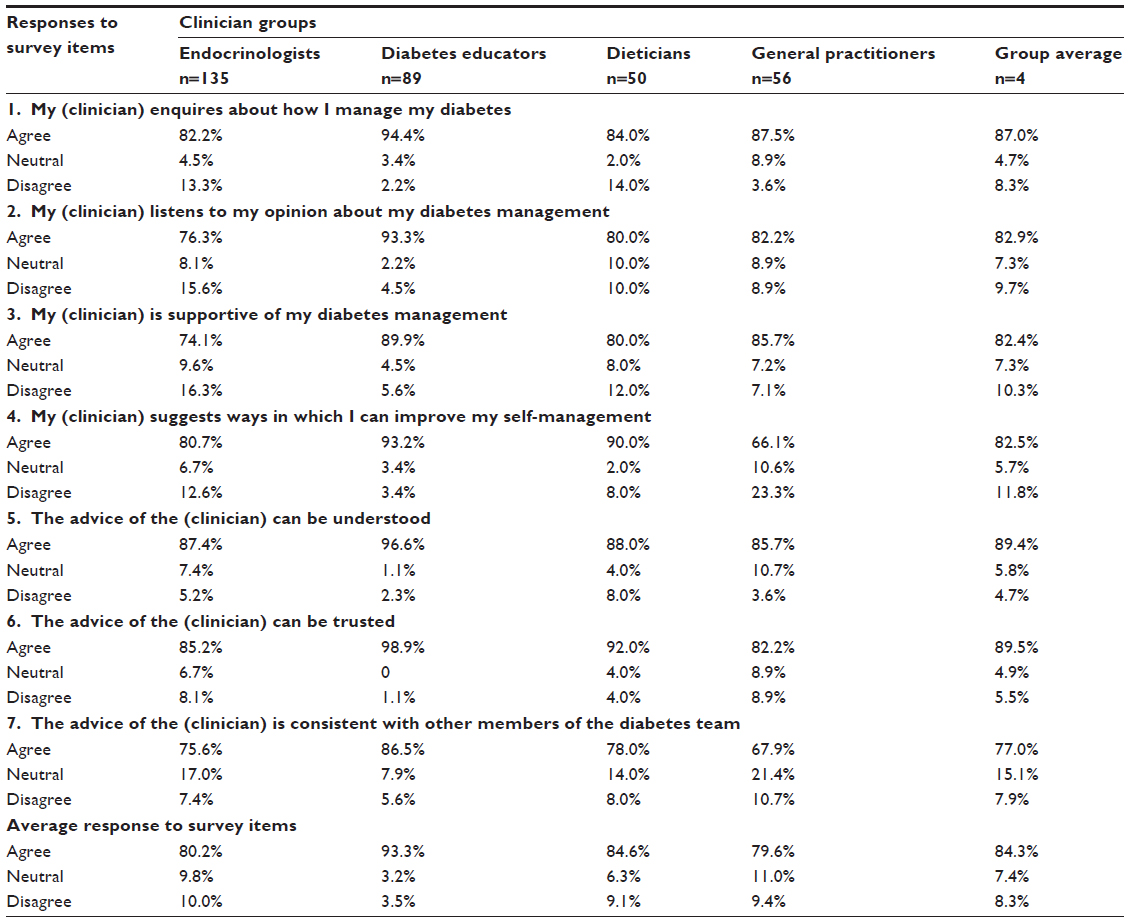 | Table 3 Evaluation of clinician engagement in shared decision-making by participants currently consulting clinician groups |
An SDM estimate was calculated for each clinician group by averaging the percentages of participants who agreed with each of the seven questions regarding that group. For example, as shown in Table 3, an average of 80.2% agreed that their endocrinologists demonstrated the qualities the questions asked about, ranging from 74.1% who agreed that their endocrinologists were supportive of their diabetes management to 85.2% who thought their advice could be trusted. Comparing the proportions of patients reporting SDM across clinician groups, the group rated as demonstrating the most SDM was diabetes educators (93.3%). Dieticians attracted the second highest average score at 84.6%, followed by endocrinologists at 80.2% and general practitioners at 79.6%. The mean weighted average of agreement to SDM for all consultations was 84.3%.
Focus groups
Characteristics of focus group participants
These were a subset of the survey participants. Sixty-eight respondents expressed interest in attending the focus groups, but only 33 participants (27 females [81.8%] and six males [18.1%]) were available for the organized dates and venues. All participants came from major or regional cities. Their mean age was 25.1 (range 20–33) years. The mean duration of type 1 diabetes was 10.5 (range 0.5–25) years.
Focus group results
Focus group results expanded on the survey findings. They acted to both reinforce the positive responses of those who continued to consult various clinician groups but also to give insights into the experiences of participants where there was a failure by clinicians to engage in SDM. Participants who had type 1 diabetes of longstanding duration reported that over the period of their illness there had been a notable change in clinicians’ consultation style from a model representative of an attitude of “here is your regimen, you stick to it”, to one that embraced such SDM attitudes:
It was a brutal experience. … He (the endocrinologist) always made me feel like I was doing the wrong thing. … It was a very intensive experience where it was; ‘this is the way you do it!’ … Diabetes management at the time was not flexible because insulins weren’t at that level but that meant that the way they treated it was here is your regimen, you stick to it. Any deviation from that was seen as something that needed to be corrected. … But something has happened in diabetes care that has changed over the last ten years. … I don’t handle very well being told what to do. … But now I am presented with options and when I say that bad things have happened she just basically takes it and goes OK so what is going to happen next time so that there is no disappointment. When I do things, which she thinks are a positive step, I get lots of affirmations. So it’s amazing! (woman aged 32 years, with a type 1 diabetes mellitus duration of 25 years).
Three major themes emerged from the focus group data. These related to: whether clinicians engaged in behavior that acknowledged patients’ expertise; whether clinicians engaged in behavior that was supportive and encouraged patients’ autonomy; and whether clinicians provided advice that patients could utilize to improve their self-management skills. Table 4 shows the hierarchy of the themes and subthemes identified in thematic analysis.
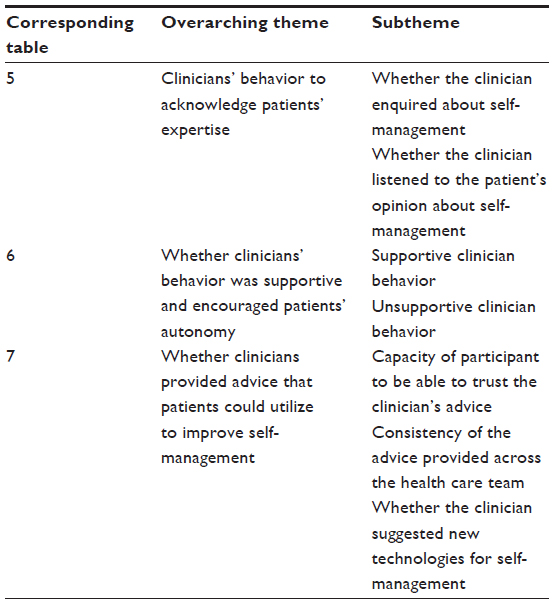 | Table 4 Thematic analysis of focus group results |
Clinicians’ behavior when acknowledging patients’ expertise
Thematic analysis revealed two categories of factors impacting on clinician behavior to indicate that they acknowledged their patients’ expertise (Table 5). These two factors related to the capacity of clinicians to enquire about their patients’ self-management practices and to listen to their patients’ opinion regarding their experience of self-management implementation.
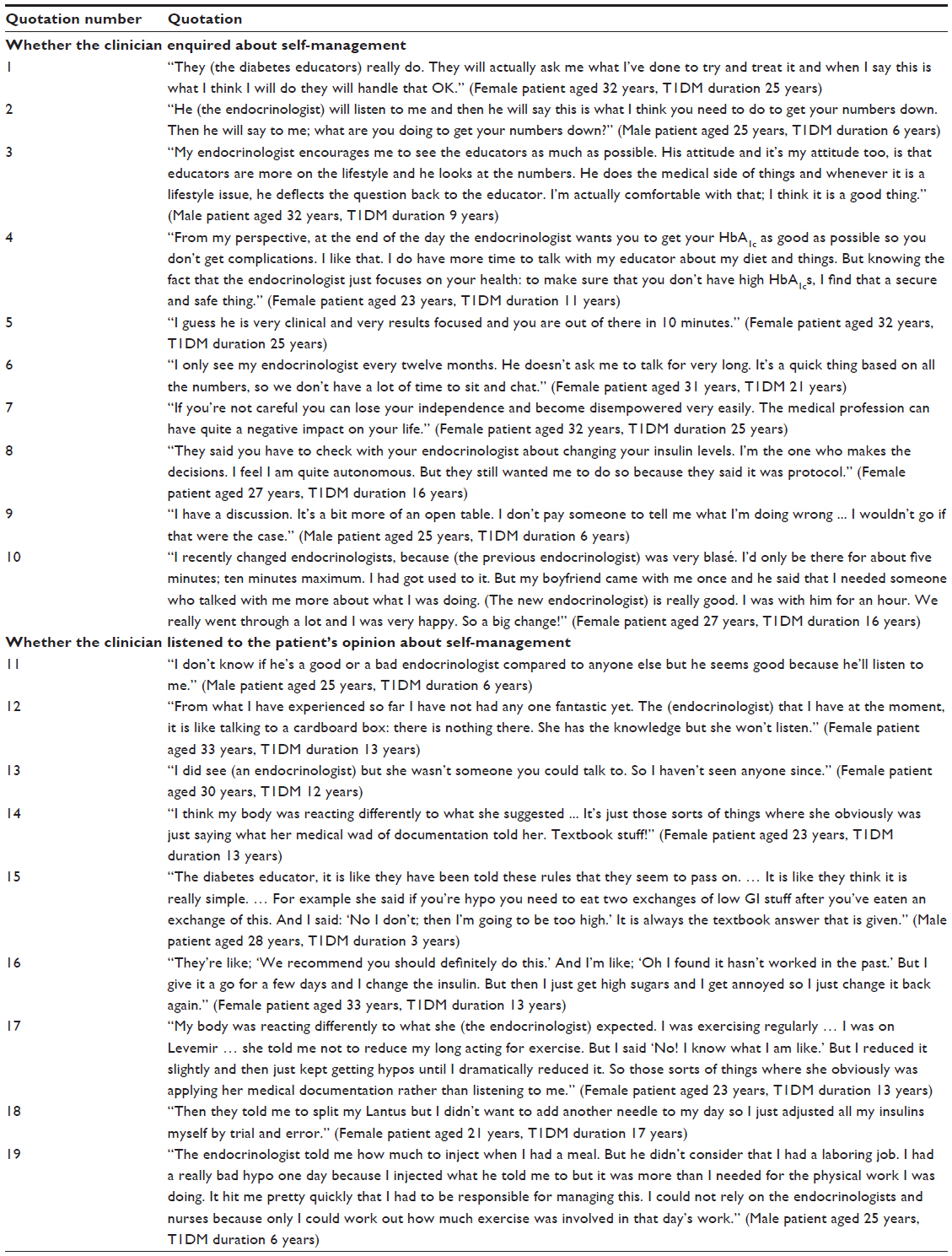 | Table 5 Participant quotations as to whether clinicians’ behavior acknowledged patient expertise |
Whether the clinician enquired about self-management
From a positive perspective, participants spoke of clinicians who treated the consultation as an open forum where patient expertise was sought, listened to, acknowledged, respected, and incorporated into the management regimen (Table 5, quotes 1 and 2). However, some participants perceived that there was a division of responsibility for SDM and that it was not the role of the endocrinologist to enquire about self-management. This division of clinician engagement in shared decision making was acceptable to some participants (Table 5, quotes 3 and 4). However, many participants expressed frustration that they had experienced negative interactions related to SDM across multidisciplinary clinician consultations. The reports of failure by some endocrinologists, in particular, to engage in a greater degree of SDM were consistent with the reported perceptions that clinicians were “time-poor”, and “results-orientated” (Table 5, quotes 5 and 6). Such time constraints led to situations where clinicians failed to enquire about the participants’ self-management practices. Participants perceived that the failure of clinicians to enquire about self-management practices was associated with a lack of respect for the expertise of the patient and led to feelings of disempowerment (Table 5, quotes 7 and 8). Further, failure of the clinician to enquire about the participants’ self-management was a reason cited for discontinuing consultation with that clinician (Table 5, quotes 9 and 10).
Whether the clinician listened to the patient’s opinion about self-management
Participants emphasized the need for clinicians to listen to their patients’ opinions about their self-management experiences and that failure to listen was a reason to terminate a therapeutic relationship (Table 5, quotes 11, 12, and 13). Participants cited examples of clinician recommendations for diabetes management regimens based on theoretical expertise that did not account for the implementation constraints that participants had experienced.
Consultations where clinicians failed to listen to the participants’ experiences were often characterized by reliance on theoretical knowledge (“textbook stuff”) rather than engaging with the real-world problems for which the participants were seeking help (Table 5, quotes 14 and 15). Similarly, some clinicians failed to listen to the needs and preferences of their patients. This resulted in the clinician recommending ineffective or unsuitable treatment regimens (Table 5, quotes 16 and 17) or regimens that were later abandoned by participants (Table 5, quotes 18 and 19).
Whether clinicians’ behavior was supportive and encouraged patient autonomy
Participants described clinicians who were supportive of SDM as having the following attributes (Table 6): taking a personal interest in the patient (Table 6, quotes 20 and 21); not trivializing patient concerns (Table 6, quotes 22 and 23); enquiring about patient-led self-management; listening to the patient and providing treatment options (Table 6, quotes 24 and 25); suggesting small achievable steps in management change (Table 6, quote 26); providing flexible access to clinician advice by phone or email (Table 6, quotes 27 and 28); and providing affirmation of the outcomes achieved by the patient (Table 6, quotes 29 and 30).
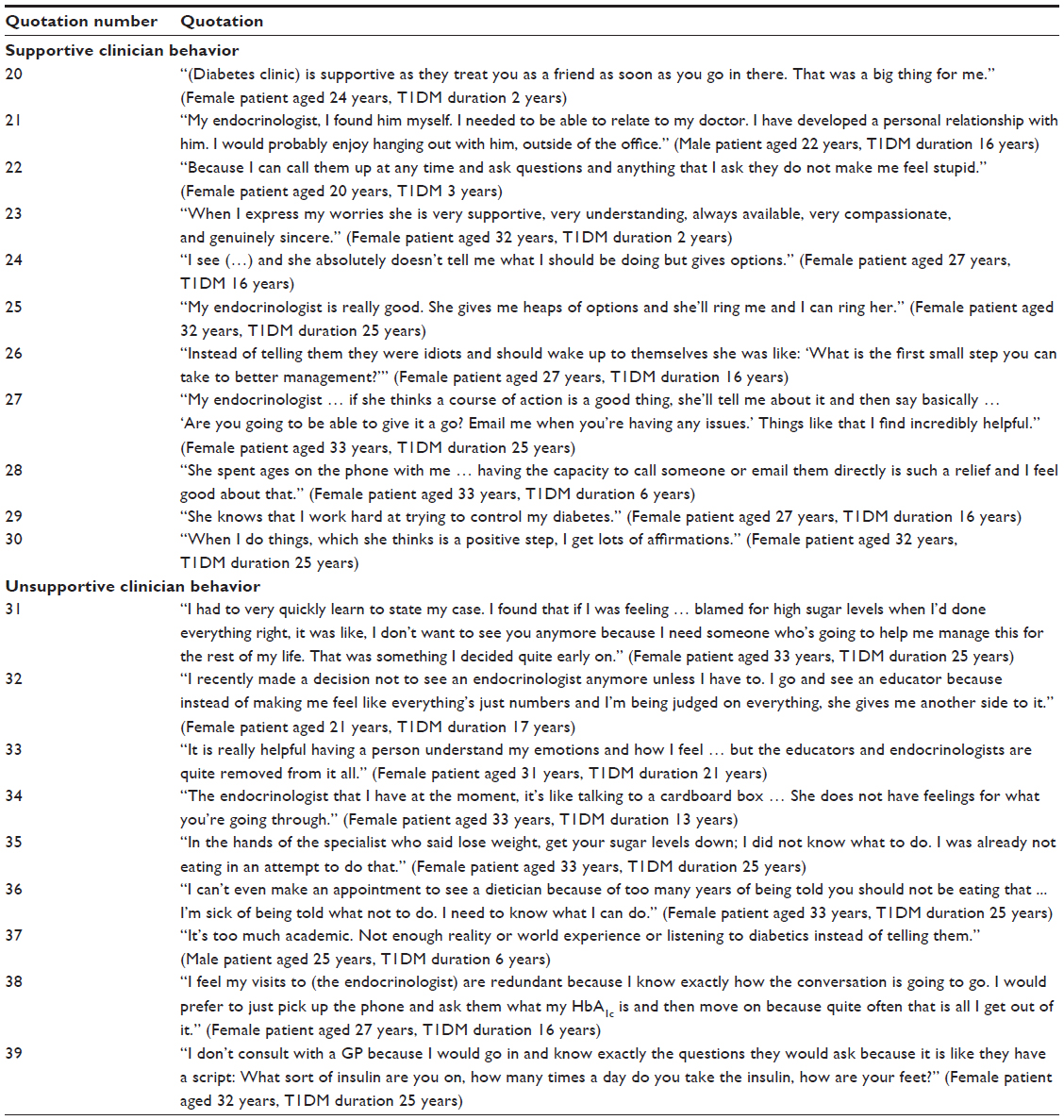 | Table 6 Participant quotations about whether clinicians’ behavior was supportive and encouraged patients’ autonomy |
Typically, supportive consultations involved an acknowledgement by the clinician of the inherent necessity to adapt any advice offered by them to real-world scenarios. To assist with this need, such clinicians often provided access by email or phone for further advice if implementation of the agreed management plan proved difficult. Participants reported that this consultation style provided both support and affirmation of their capacity to cope with the daily demands of maintaining target levels of disease management.
Participants stated that when consultations were not characterized by SDM, they were left feeling disempowered and blamed for failure to reach treatment target levels (Table 6, quotes 31 and 32). Such consultations involved a failure by clinicians to demonstrate empathy (Table 6, quotes 33 and 34), or criticism of participants’ lifestyle choices without offering constructive alternatives (Table 6, quotes 35 and 36). Participants reported that some clinicians had “script-like consultation routines” that discouraged any involvement in SDM. Many participants had decided to terminate consultation altogether with various clinicians or groups of clinicians because of repeated experiences of failure of these clinicians to orient toward SDM (Table 6, quotes 37, 38, and 39).
Whether clinicians provided advice that patients could utilize to improve self-management
Thematic analysis revealed three categories of factors impacting on clinician behavior regarding provision of advice that the patient could utilize to improve self-management (Table 7). These three factors related to the capacity of the participant to be able to trust the clinician’s advice, the consistency of advice provided across the health care team, and whether the clinician suggested new technologies for self-management.
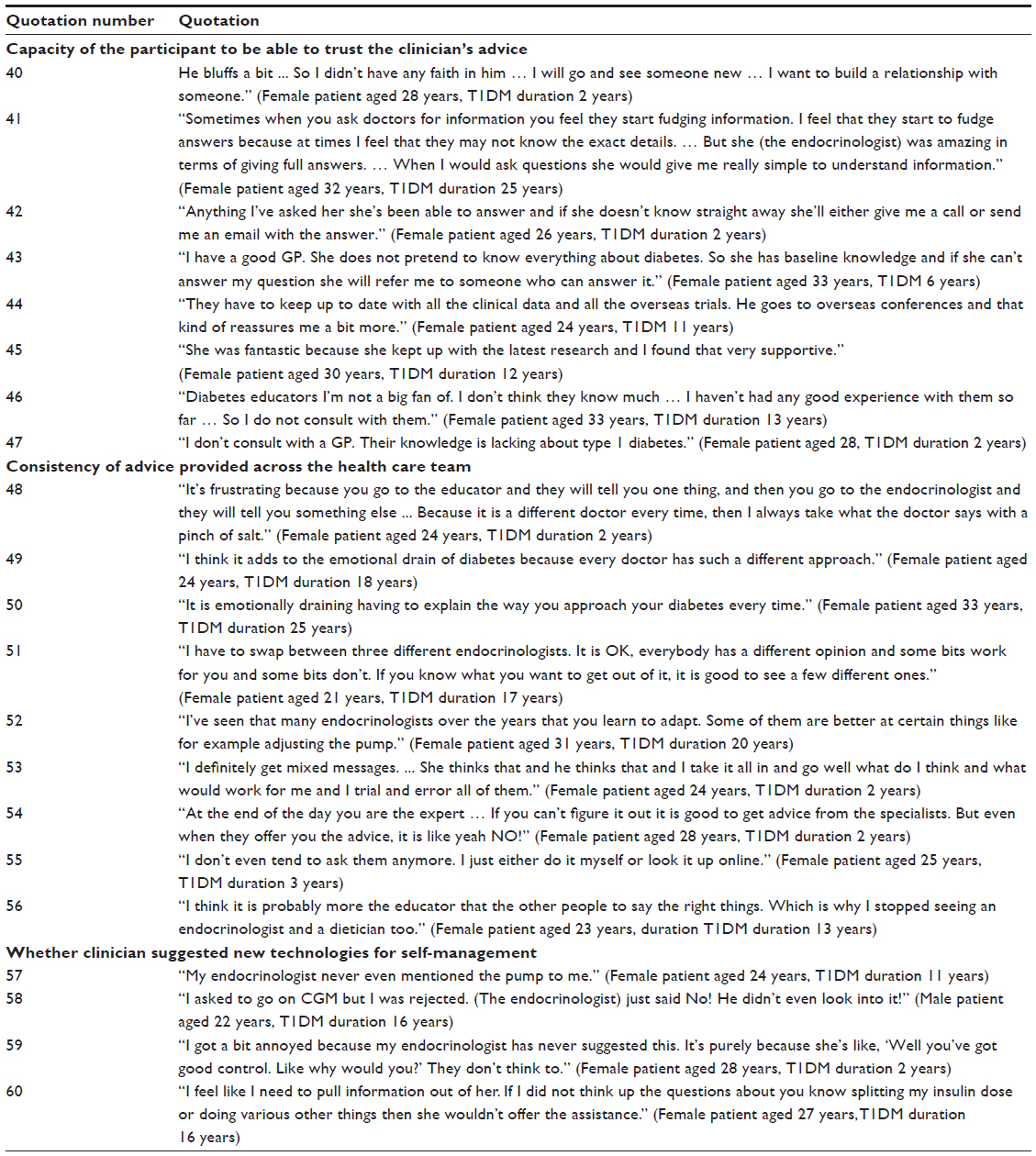 | Table 7 Participant quotations about whether clinicians provided advice that patients could utilize to improve self-management |
Capacity of the participant to be able to trust the clinician’s advice
Participants reported that a fundamental basis for SDM was an ability to be able to depend on the integrity of clinician advice. Trust in the quality of the information exchanged in a consultation was vital for development of a therapeutic relationship (Table 7, quotes 40 and 41). Participants identified that the imperative for accurate information was more important than for the immediacy of information, and a delayed response provided participants with reassurance that the clinician was attempting to obtain the best available information. Such information exchange often involved use of email post-consultation (Table 7, quotes 42 and 43). Participants reported a preference for clinicians who were aware of current research and evidence-based practice (Table 7, quotes 44 and 45). Participants identified a lack of trust in clinician advice as a reason to discontinue further consultation with that clinician (Table 7, quotes 46 and 47).
Consistency of advice provided across the health care team
Participants identified that a barrier to SDM occurred when inconsistent advice was provided across the health care team. The occurrence of these situations was heightened when participants were exposed to a rotation of unfamiliar hospital-based clinicians in outpatient clinics (Table 7, quote 48). Not only was the capacity to engage in SDM compromised, but provision of inconsistent advice added to the burden of living with a chronic illness (Table 7, quotes 49 and 50). However, some participants reported that provision of multiple or conflicting clinician opinions had inherent benefits because it exposed the participant to greater options (Table 7, quotes 51 and 52) and because clinician opinion was not consistent it encouraged greater patient autonomy (Table 7, quotes 53 and 54). However, for other participants, the burden of dealing with the inconsistency of advice between clinicians acted as a driver to discontinue further consultation with clinicians (Table 7, quotes 55 and 56).
Whether the clinician suggested new technologies for self-management
Participants reported a tendency for some clinicians to fail to recommend new technologies to assist with self-management. This led to participant-driven instigation of discussion with clinicians about whether to introduce the use of new technologies into the management regimen. Some participants perceived that certain providers were not familiar with, or were resistant to, use of new technologies (Table 7, quotes 57 and 58). Participants identified a perceived lack of clinician familiarity with these new technologies as a barrier to SDM (Table 7, quotes 59 and 60).
Discussion
Overall, we found that a high proportion of survey participants expressed some level of agreement that they had experienced facets of SDM being implemented in their clinician encounters. The results were consistent across all clinician groups in the multidisciplinary diabetes team studied. The wide spread of locations of our respondents, which is consistent with the population distribution across Australia, reduced the risk that a small number of clinicians who actively engaged in SDM in each clinician group had unduly influenced the overall results. We found that our participants in the focus groups preferred clinicians who engaged in SDM. The focus groups revealed that participant perception of a failure by clinicians to engage in SDM was a common reason cited for discontinuing consultation with that clinician or group of clinicians.
The focus group discussion indicated that SDM is best implemented when there is clinician respect for patient expertise in re-evaluating the management plan and there is ready accessibility to clinician advice outside of face-to-face consultation time, which is consistent with the work of Mol.43 Mol proposes that SDM should not be seen as a series of static decisions made by the patient and clinician at a particular time, but as a process that requires never-ending adaptability to the “messy reality of life”. Legare and Witteman recognize the need for adaptive tools to support such a flexible model of SDM.2
Our participants’ reports that clinician engagement in SDM is affected by the time pressure of clinician workloads has been noted in other studies.44 However, there is no evidence to support the premise that SDM is more time-consuming than other models of care.2 A division in the types of responsibility for SDM amongst different members of the health care team, as observed by some of our participants, has been suggested as a method to improve more widespread facilitation of SDM.3
Our finding that the advice provided was sometimes inconsistent across the multidisciplinary groups suggests that clinicians need to better case manage their diabetes patients. Our study provides impetus for better coordination of multidisciplinary care. However our findings provide evidence that among the multidisciplinary clinicians consulted, SDM was being practiced, and that this ideological shift in health service delivery is emerging in clinical practice. Our findings are consistent with a recent comparative international study by the Commonwealth Fund that examined SDM in patients with complex chronic illness and found that patients in Switzerland, the UK, Australia, New Zealand, and the USA were the most likely to report facets of shared decision-making, with strong majorities (65%–73%) saying that their clinicians always or often spent enough time with them, encouraged questions, and provided clear explanations.45
Recruitment of the study sample by self-selection and through advertisements in diabetes-related support organizations introduced a potential for bias into this study. Eighty percent of the survey sample was female. The Australian National Diabetes Register records incidence rates for children younger than 15 years as approximately equal for males and females. However, for the age groups 15–19 years, 20–24 years, 25–29 years, and 30–34 years, males slightly exceed females, thus skewing our bias further towards females. Eighty-four percent of participants had private health insurance and 79% had tertiary or higher levels of education. These are higher than national averages. Further, 34% of the sample reported that their last HbA1c was less than 7%, whereas it has been reported that less than 20% of adults with diabetes in Australia maintain an HbA1c level <7%.46,47 Further, our attrition rate from all services was 2%, whereas attrition rates in Australia have been reported in this age group as high as 50%.38 The demographic and clinical characteristics of our sample, particularly in relation to their level of education, might indicate that bias would be more towards patients who actively sought SDM. People with less education and those with fewer numeracy skills report decreased levels of engagement with SDM.48 The survey data may overemphasize the uptake of SDM by diabetes educators, dieticians, and general practitioners due to the smaller numbers of participants in our study consulting those clinicians. Further, the clinical indicators recorded in our survey were self-reported and therefore the results may be subject to recall and reporting bias. Due to the specific age range of our participants, our results may not be generalizable across all type 1 diabetes health services.
Qualitative studies such as this one collect large amounts of data from a small number of informants or study sites. They are not designed to estimate proportions in a wider population, quantify relationships between predetermined variables, or provide a single representative or average view or opinion. Instead, they seek to document and explain the variation in a wide range of views, needs, values, practices, and beliefs.
Conclusion
Assisting type 1 diabetes self-management practices through shared decision-making and empowering patients by promoting patient autonomy can be instrumental in avoiding diabetes-related disease complications and improving glycemic control.22 Our findings indicate that although some clinicians are embracing SDM, the reported experiences of young adults with type 1 diabetes indicate there are opportunities to improve clinician engagement in SDM across all groups of the multidisciplinary diabetes team.
The results suggest that such improvements could lead to increased patient uptake of diabetes-related health services by retaining patients who are currently rejecting certain clinician services due to the failure of those clinicians to practice SDM. The high attrition rate of young adults from diabetes health services,37,38 and the poor health outcomes faced by this group,46,47 act as strong imperatives to ensure that diabetes health services are more patient-centered. This study provides insights into ways that may assist in improving health service delivery and health outcomes for these young adults.
Author contributions
JW researched data, contributed to the conception, design and discussion of the research, wrote, reviewed, and edited the manuscript. MW researched data, contributed to discussion, reviewed and edited the manuscript. JG, RD, and JB contributed to the conception design and discussion of the research, and reviewed and edited the manuscript. All authors guarantee this work and are accountable for all aspects of this work.
Acknowledgments
This research was conducted under the auspices of a program of research funded by the National Health and Medical Research Council (NHMRC) of Australia: NHMRC Program Grant 568612. The failure of the majority of Australian adults to reach clinically dictated treatment target levels of Type 1 diabetes control is a case study in the program. We thank the young adults that were involved in the focus groups and/or the survey for their contribution to this research. We acknowledge Janet Long’s contribution to data analysis and discussion and the editorial contribution of Dr Wendy Lipworth, Professor Don Chisholm AO, and Professor Lesley Campbell AM. A version of this paper was presented at the International Society for Quality in Health Care, 29th International Conference. Geneva, Switzerland. 21–24 October 2012.
Disclosure
The authors declare that they have no competing interests in this work.
References
Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med. 1997;44(5):681–692. | |
Legare F, Witteman HO. Shared decision making: examining key elements and barriers to adoption into routine clinical practice. Health Aff (Millwood). 2013;32(2):276–284. | |
Friedberg MW, Van Busum K, Wexler R, Bowen M, Schneider EC. A demonstration of shared decision making in primary care highlights barriers to adoption and potential remedies. Health Aff (Millwood). 2013;32(2):268–275. | |
Barry MJ, Edgman-Levitan S. Shared decision making – pinnacle of patient-centered care. N Engl J Med. 2012;366(9):780–781. | |
Australian Commission on Safety and Quality in Health Care. Patient-Centred Care: Improving Quality and Safety through Partnerships with Patients and Consumers. Sydney, Australia: Australian Commission on Safety and Quality in Health Care; 2011. | |
Gerteis M, Edgman-Levitan S, Daley J, DelBanco TL. Through the Patient’s Eyes: Understanding and Promoting Patient-Centred Care. San Francisco, CA, USA: Jossey-Bass; 1993. | |
Schaller D. Patient-Centered Care: What Does It Take? Picker Insitute and Commonwealth Fund; 2007. Available from: http://www.commonwealthfund.org/Publications/Fund-Reports/2007/Oct/Patient-Centered-Care-What-Does-It-Take.aspx. Accessed December 17, 2013. | |
Robb G, Seddon M; Effective Practice Informatics and Quality (EPIQ). Quality improvement in New Zealand healthcare. Part 6: keeping the patient front and centre to improve healthcare quality. N Z Med J. 2006;119(1242):U2174. | |
Moulton B, King JS. Aligning ethics with medical decision-making: the quest for informed patient choice. J Law Med Ethics. 2010;38(1):85–97. | |
Harter M, Muller H, Dirmaier J, Donner-Banzhoff N, Bieber C, Eich W. Patient participation and shared decision making in Germany – history, agents and current transfer to practice. Z Evid Fortbild Qual Gesundhwes. 2011;105(4):263–270. | |
Moumjid N, Christine D-B, Denois-Regnier V, Roux P, Soum-Pouyalet F. Shared decision making in the physician-patient encounter in France: a general overview in 2011. Z Evid Fortbild Qual Gesundhwes. 2011;105(4):259–262. | |
van der Weijden T, van Veenendaal H, Drenthen T, et al. Shared decision making in The Netherlands, is the time ripe for nationwide, structural implementation? Z Evid Fortbild Qual Gesundhwes. 2011;105(4):283–88. | |
Legare F, Stacey D, Forest P-G, Coutu M-F. Moving SDM forward in Canada: milestones, public involvement, and barriers that remain. Z Evid Fortbild Qual Gesundhwes. 2011;105(4):245–253. | |
Coulter A, Edwards A, Elwyn G, Thomson R. Implementing shared decision making in the UK. Z Evid Fortbild Qual Gesundhwes. 2011;105(4):300–304. | |
Stacey D, Bennett CL, Barry MJ, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2011;10:CD001431. | |
Attale C, Lemogne C, Sola-Gazagnes A, et al. Therapeutic alliance and glycaemic control in type 1 diabetes: a pilot study. Diabetes Metab. 2010;36(6 Pt 1):499–502. | |
Cvengros JA, Christensen AJ, Cunningham C, Hillis SL, Kaboli PJ. Patient preference for and reports of provider behavior: impact of symmetry on patient outcomes. Health Psychol. 2009;28(6):660–667. | |
Kinmonth AL, Woodcock A, Griffin S, Spiegal N, Campbell MJ. Randomised controlled trial of patient centred care of diabetes in general practice: impact on current wellbeing and future disease risk. The Diabetes Care From Diagnosis Research Team. BMJ. 1998;317(7167):1202–1208. | |
Bauman A, Fardy H, Harris P. Getting it right: why bother with patient-centred care? Med J Aust. 2003;179(5):253–256. | |
Nolte E, McKee M. Caring for People with Chronic Conditions: A Health System Perspective. Berkshire, UK: World Health Organization; 2008. | |
Deci EL, Ryan RM. The “what” and “why” of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000;11(4):227–268. | |
Williams GC, McGregor HA, Zeldman A, Freedman ZR, Deci EL. Testing a self-determination theory process model for promoting glycemic control through diabetes self-management. Health Psychol. 2004;23(1):58–66. | |
Coulter A, Parsons S, Askham J. Where are the Patients in Decision-Making about their Own Care. Copenhagen, Denmark: World Health Organization Regional Office for Europe; 2008. | |
Salzburg Global Seminar. The Salzburg Statement on Shared Decision-Making. 2011. Available from: http://us.cochrane.org/sites/us.cochrane.org/files/uploads/Ford,%20Peg%20-%20Salzburg-Statement-ammended5.pdf. Accessed December 17, 2013. | |
Grol R, Wensing M, Mainz J, et al. Patients in Europe evaluate general practice care: an international comparison. Br J Gen Pract. 2000;50(460):882–887. | |
Bezold C. The future of patient-centered care: scenarios, visions, and audacious goals. J Altern Complement Med. 2005;11 Suppl 1:S77–S84. | |
Koch S. Improving quality of life through eHealth – the patient perspective. Stud Health Technol Inform. 2012;180:25–29. | |
Robinson JH, Callister LC, Berry JA, Dearing KA. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract. 2008;20(12):600–607. | |
Gilbertson HR, Brand-Miller JC, Thorburn AW, Evans S, Chondros P, Werther GA. The effect of flexible low glycemic index dietary advice versus measured carbohydrate exchange diets on glycemic control in children with type 1 diabetes. Diabetes Care. 2001;24(7):1137–1143. | |
Parillo M, Annuzzi G, Rivellese AA, et al. Effects of meals with different glycaemic index on postprandial blood glucose response in patients with type 1 diabetes treated with continuous subcutaneous insulin infusion. Diabet Med. 2011;28(2):227–229. | |
Marsh K, Barclay A, Colagiuri S, Brand-Miller J. Glycemic index and glycemic load of carbohydrates in the diabetes diet. Curr Diab Rep. 2011;11(2):120–127. | |
Porcellati F, Bolli GB, Fanelli CG. Pharmacokinetics and pharmacodynamics of basal insulins. Diabetes Technol Ther. 2011;13 Suppl 1:S15–S24. | |
Heptulla RA, Rodriguez LM, Mason KJ, Haymond MW. Gastric emptying and postprandial glucose excursions in adolescents with type 1 diabetes. Pediatr Diabetes. 2008;9(6):561–566. | |
Liang WW. Seasonal changes in preprandial glucose, A1c, and blood pressure in diabetic patients. Diabetes Care. 2007;30(10):2501–2502. | |
Chiu KC, Chu A, Go VLW, Saad MF. Hypovitaminosis D is associated with insulin resistance and beta cell dysfunction. Am J Clin Nutr. 2004;79(5):820–825. | |
Joosten EA, DeFuentes-Merillas L, de Weert GH, Sensky T, van der Staak CP, de Jong CA. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother Psychosom. 2008;77(4):219–226. | |
Peters A, Laffel L; American Diabetes Association Transitions Working Group. Diabetes care for emerging adults: recommendations for transition from pediatric to adult diabetes care systems: a position statement of the American Diabetes Association, with representation by the American College of Osteopathic Family Physicians, the American Academy of Pediatrics, the American Association of Clinical Endocrinologists, the American Osteopathic Association, the Centers for Disease Control and Prevention, Children with Diabetes, The Endocrine Society, the International Society for Pediatric and Adolescent Diabetes, Juvenile Diabetes Research Foundation International, the National Diabetes Education Program, and the Pediatric Endocrine Society (formerly Lawson Wilkins Pediatric Endocrine Society). Diabetes Care. 2011;34(11):2477–2485. | |
Perry L, Steinbeck KS, Dunbabin JS, Lowe JM. Lost in transition? Access to and uptake of adult health services and outcomes for young people with type 1 diabetes in regional New South Wales. Med J Aust. 2010;193(8):444–449. | |
Goodrich J, Cornwell J. Seeing the person in the patient: the point of care review paper. London, UK; 2008. http://www.kingsfund.org.uk/sites/files/kf/Seeing-the-person-in-the-patient-The-Point-of-Care-review-paper-Goodrich-Cornwell-Kings-Fund-December-2008.pdf. Accessed December 17, 2013. | |
Ngo-Metzger Q, Telfair J, Sorkin DH, et al. Cultural competency and the culture of care: obtaining the patients’ perspective. The Commonwealth Fund; 2006. Available from: http://www.commonwealthfund.org/usr_doc/Ngo-Metzger_cultcompqualitycareobtainpatientperspect_963.pdf. Accessed December 17, 2013. | |
Morgan DL, Krueger RA. When to use focus groups and why. In: Morgan DL, editor. Successful Focus Groups: Advancing the State of the Art. Newbury Park, CA, USA: Sage Publications; 1993. | |
Creswell J. Research Design: Qualitative, Quantitative and Mixed Method Approaches. 3rd ed. Thousand Oaks, CA, USA: Sage Publications; 2009. | |
Mol A. The Logic of Care: Health and the Problem of Patient Choice. 1st ed. Oxford, UK: Routledge; 2008. | |
Legare F, Ratte S, Stacey D, Kryworuchko J, Gravel K, Graham I. Interventions for improving the adoption of shared decision-making by healthcare professionals. Cochrane Database Syst Rev. 2010;5:CD006732. | |
Schoen C, Osborn R, Squires D, Doty M, Pierson R, Applebaum S. New 2011 survey of patients with complex care needs in eleven countries finds that care is often poorly coordinated. Health Aff (Millwood). 2011;30(12):2437–2448. | |
Bryant W, Greenfield JR, Chisholm DJ, Campbell LV. Diabetes guidelines: easier to preach than to practise? Med J Aust. 2006;185(6):305–309. | |
McIntyre DH. DAFNE (Dose Adjustment for Normal Eating): structured education in insulin replacement therapy for type 1 diabetes. Med J Aust. 2006;184(7):317. | |
Kiesler DJ, Auerbach SM. Optimal matches of patient preferences for information, decision-making and interpersonal behavior: evidence, models and interventions. Patient Educ Couns. 2006;61(3):319–341. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.