")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 10
Review of applications of microneedling in dermatology
Authors Iriarte C , Awosika O, Rengifo-Pardo M, Ehrlich A
Received 23 May 2017
Accepted for publication 1 July 2017
Published 8 August 2017 Volume 2017:10 Pages 289—298
DOI https://doi.org/10.2147/CCID.S142450
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Christopher Iriarte,1 Olabola Awosika,2 Monica Rengifo-Pardo,1,2 Alison Ehrlich1,2
1George Washington University School of Medicine and Health Sciences, Washington, DC, USA; 2Department of Dermatology, The George Washington Medical Faculty Associates, Washington, DC, USA
Abstract: Microneedling (MN) is a novel therapeutic modality in dermatology. Through physical trauma from needle penetration, MN induces a wound healing cascade with minimal damage to the epidermis. This allows for enhancement in the absorption of mainstay topical therapies across the thick stratum corneum. MN has become increasingly utilized over the last several years as it is a relatively simple procedure that is cost-effective, well tolerated, and offers both cosmetic and therapeutic benefits. The ability to treat localized areas of disease has led to numerous studies gauging its potential in focal diseases of inflammation, dyschromia, and photodamage. This review discusses the principles and evidence behind the expanding applications of MN. It has shown promising results as an adjuvant therapy for enhanced drug delivery in the treatment of atrophic scars, alopecia, actinic keratoses, and disorders of pigmentation such as melasma. The efficacy in treatment of vitiligo remains limited. Overall, the procedure has few adverse sequelae compared to other therapies, is highly efficacious, and is a viable resurfacing option for skin of color. Future research is needed to determine the frequency, interval, and specific device settings that foster optimal results. Additionally, large controlled trials are needed to shed light on the utility of MN as an evidence-based regimen for the treatment of various dermatologic conditions.
Keywords: microneedling, scars, acne, alopecia, hyperpigmentation, actinic keratosis
Introduction
Microneedling (MN), also known as collagen induction therapy, is a process involving repetitive puncturing of the skin with sterilized microneedles. Its original conception can be traced back to 1995, when Orentreich and Orentreich developed the concept of “subcision”, or using hypodermic needles to induce wound healing in depressed cutaneous scars.1 In 2006, Dr. Desmond Fernandes developed the first MN product which became the modern-day Dermaroller® (Dermaroller Deutschland GmbH, Wolfenbuettel, Germany).2
MN offers a relatively low cost and minimally invasive tool for the treatment of multiple cosmetic and dermatologic conditions.3 The basis of MN relies on physical trauma. It has been proposed that the trauma generated by needle penetration in the skin induces regeneration of the dermis.4 The needles penetrate the stratum corneum and create small holes known as micro-conduits with minimal damage to the epidermis. This sequentially leads to the generation of growth factors which stimulate the production of collagen and elastin in the papillary layer of the dermis.3 The natural wound healing cascade is induced as platelets and neutrophils are recruited to release growth factors such as TGF-alpha, TGF-beta, and platelet-derived growth factor (PDGF).2 This ultimately results in the deposition of collagen by fibroblasts.
A variety of MN products have been developed to treat scarring and wrinkles, enable skin rejuvenation, and improve skin appearance.5 Clinical trials over the last several years have shed light on the applications of MN beyond cosmetic indications, including actinic keratoses (AK), disorders of pigmentation, hyperhidrosis, and striae.6 Additionally, the role of MN in the treatment of hair pathology has become a recent field of focus as it is thought to stimulate stem cells in the dermal papilla, increase blood flow to hair follicles, and recruit growth factors and signaling pathways which induce hair restoration.7 MN is also postulated to induce normal wound healing, specifically by breaking collagen strands in the superficial dermis and inducing collagen synthesis immediately under the epidermis.8 This mechanism is the guiding principle behind the application of MN in the treatment of scars of various etiologies.
This review of the literature is focused on exploring the expanding indications of MN. In addition, this review will highlight the efficacy and adverse effect prolife of MN in comparison with more common treatment modalities used for various indications in dermatology.
Methods
The studies selected for this review were gathered by searching the PubMed, MEDLINE, Cochrane databases, and electronic journals of dermatology. The search terms used for this review included “microneedling”, “collagen induction”, “reviews”, and “trials”. Only articles published in English were considered for inclusion in this review. Articles were obtained in all circumstances and references were checked for additional information when considered applicable. Available studies involving human subjects were included in the review. Additionally, only studies regarding manual MN techniques were considered for inclusion. Priority was given to controlled clinical trials, both prospective and retrospective, with a minimum of ten patients as the sample size. Uncontrolled clinical trials were included so long as a statement was made regarding the study’s experimental design and limitations. Smaller case series with less than ten patients were included if they were the only available data for specific indications such as alopecia areata (AA) or verruca plantaris.
Types of MN
Currently, there are many mechanical MN devices registered with the US Food and Drug Administration (FDA), with the majority being a variation of either the Dermaroller or the Dermapen® (Dermapen, Salt Lake City, UT, USA). The Dermaroller is a hand-held device with a cylindrical roller of 24 circular arrays.6,9 Each array is equipped with eight medical grade solid steel microneedles, totaling to 192 needles on one Dermaroller device.6,9 The device is used in a multi-directional fashion (vertically, horizontally, and diagonally) directly over the skin. Medical models include the CIT 8™ and MF 8™, which consist of needle heights of 500 µm and 1,500 µm, respectively.6 Various models have also been developed for use in the home, including the Beauty Mouse® (Dermaroller Deutschland GmbH) which consists of 480 needles to use on larger skin surfaces.5 The Dermapen is a spring-loaded MN device which acts as an electrically powered pen, delivering stamp-like motions across the skin.10 Several commercial variations of this device exist based on the same principles.
Other devices use additional technology to build upon the applications of mechanical MN. Indications for these newer modalities include superficial scars, hyperhidrosis, and wrinkles.6 These MN modalities include fractional radiofrequency microneedling (FRFM), DermaFrac™ (Genesis Biosystems, Lewisville, TX, USA), light emitting diode (LED) MN devices, and MN delivery systems.6 FRFM is differentiated from manual MN due to the method of each insulated needle releasing a radiofrequency current from the needle tip producing changes in dermal structural components.6,11 In DermaFrac treatment, MN is combined with microdermabrasion, LED light, and simultaneous serum infusion into the dermis.6 LED MN rollers combine solely LED light and MN. MN delivery systems are a method of transdermal drug administration in which solid microneedles pierce the skin followed by topical drug application. Alternatively, drugs can be delivered directly into the dermis through hollow needles.12 Of note, in 2011, Fluzone® Intradermal influenza virus vaccine (Sanofi Pasteur, Swiftwater, PA, USA) became the first and only microneedle-based product approved by the FDA for this process.13,14 It is recommended that the use of MN to enhance absorption of topical agents be performed with caution as non-sterilized drugs may contain particles that penetrate the skin to varying degrees and contribute to further complications, such as infection due to the permeation of pathogenic microbes.12
Applications of MN
The sections that follow will provide an overview of the clinical trials in dermatology that have been performed with manual MN, as well as several case series. Specific information regarding study design, treatment intervals, MN devices used, and comparative efficacy can be found in the accompanying tables. These tables summarize the major studies covered in this review for each respective indication that follows. Each section concludes with our summary of the current state of the literature and future areas for research specific to each indication.
Scars
Several studies show efficacy of MN for scar treatment (Table 1). In a pilot study, El-Domyati et al quantified the histological changes induced by MN in ten patients with atrophic facial scars from acne.15 Skin biopsies were obtained at baseline and post-treatment with Dermaroller. There was a statistically significant increase in the production of collagen types I, III, and VII and a decrease in total elastin by the end of treatment (p < 0.05). All patients reported mild pain and edema at the treatment site which resolved within 24 hours. Otherwise, no adverse effects were noted. Patients collectively reported a 51%–60% improvement in scar appearance, 40%–50% improvement in skin texture, and 80%–85% overall satisfaction (p = 0.001) following six treatment sessions over the course of 3 months.15
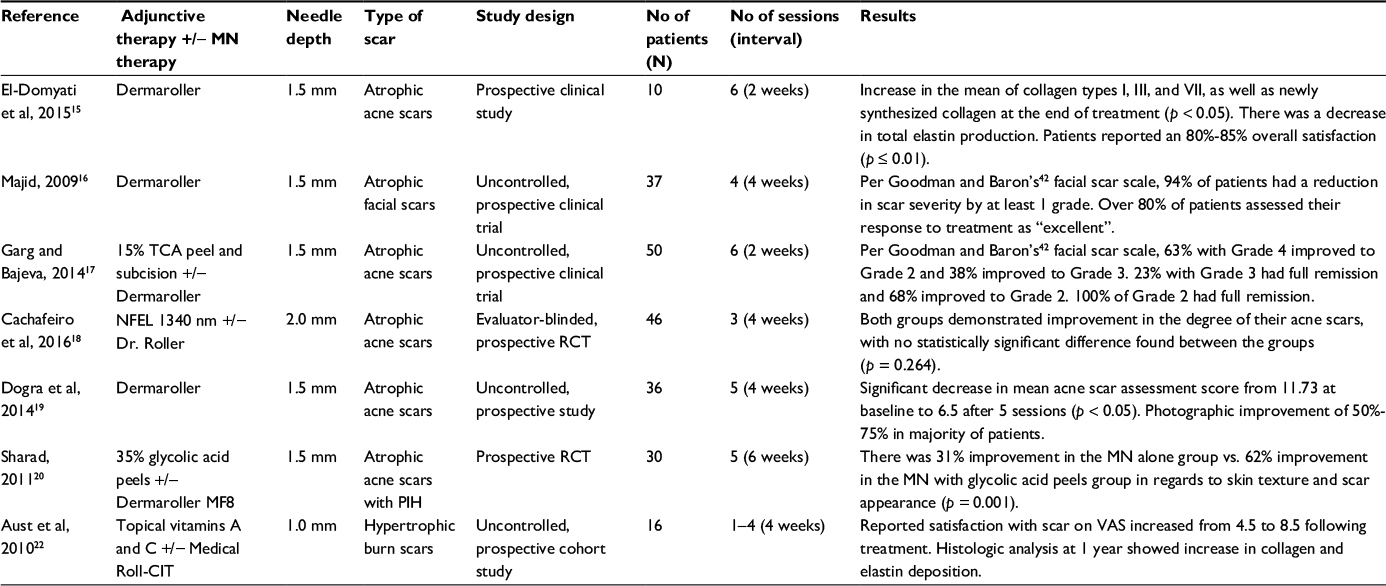 | Table 1 Scars treated with microneedling therapy Notes: Dermaroller® and Dermaroller MF8™; Dermaroller Deutschland GmbH, Wolfenbuettel, Germany. Dr. Roller™; Vydence Medical, São Carlos, São Paulo, Brazil. Medical Roll-CIT™; Vivida, Cape Town, South Africa. Abbreviations: MN, microneedling; N, sample size; TCA, trichloroacetic acid; NFEL, non-ablative fractional erbium laser; RCT, randomized controlled trial; PIH, post-inflammatory hyperpigmentation; VAS, visual analog scale (graded from 1 to 10). |
In a cohort study, Majid relied on clinical outcomes rather than histologic changes to assess improvement of atrophic facial scars in response to MN therapy.16 Thirty-seven patients were offered Dermaroller treatments and followed over the course of 2 months. Over 80% of the patients assessed their response to treatment as “excellent” on a 10-point scale. Of the patients who completed the study, 94.4% graded the reduction in the severity of their scars by at least one objective grade. No adverse effects were noted.16
A clinical trial by Garg and Baveja assessed the efficacy of combination therapy using subcision, MN, and 15% trichloroacetic acid peel in the management of 50 patients with atrophic acne vulgaris scars.17 The patients were treated for a total of six sessions with scar grading done at baseline and 1 month after treatment. Complete remission was demonstrated in all patients with Grade 2 scars and 22.7% of patients with Grade 3 scars. Additionally, of the 16 patients with Grade 4 scars at baseline, ten patients improved to Grade 2 and the remaining six improved to Grade 3. Overall, 100% of patients had objective improvement in scars by at least 1 grade. Adverse events other than transient erythema and edema included acne eruptions, post-inflammatory hyperpigmentation (PIH) resolving after 5 months of topical treatment (with combination of tretinoin, hydroquinone, and mometasone), and cervical lymphadenopathy lasting 3 weeks.17
Several studies have also compared the efficacy of laser and MN treatments. Cachafeiro et al compared 1,340 nm non-ablative fractional erbium laser and Dr. Roller™ (Vydence Medical, São Carlos, São Paulo, Brazil) for the treatment of 46 patients with facial atrophic acne scars.18 These patients were randomized to one of the two groups and received three treatment sessions monthly regardless of assignment. Both groups demonstrated improvement at 2 and 6 months post-treatment, with no statistically significant difference between them (p = 0.264). While efficacy was similar, the adverse event profile varied. The MN group experienced erythema for an average of 1 day compared to the laser group, for which the erythema lasted an average of 3 days. Additionally, 13.6% of the patients in the laser group experienced PIH while none of the patients in the MN group did.18
Another emerging field of study in MN is its applicability in the treatment of scars in various ethnic groups. One clinical trial by Dogra et al evaluated the utility of MN for treating atrophic acne scars in Asian populations.19 On an objective scale of 18 points, patients’ assessments of their scars decreased from 11.73 to 6.5 following five MN treatments, indicating significant improvement. In a study with patients of darker pigmented skin, the use of MN combined with glycolic acid peels for the treatment of acne scars was assessed in 30 Indian patients with atrophic box type and rolling scars with PIH.20 Patients were assigned to receive treatment with MN only or with MN and 35% glycolic acid peels. There was significant improvement in skin texture, scarring, and a reduction in PIH in the group treated with the combined approach when compared to MN alone (p = 0.001).20
MN has also been used to enhance treatment of hypertrophic surgical scars by increasing drug delivery of topical agents to the dermis.21 Aust et al demonstrated MN to be an effective alternative for burn patients with hypertrophic scars.22 In this study, 16 patients with post-burn scarring were treated with MN after 4 weeks of preparation with topical vitamin A and C to maximize collagen production. Each patient reported satisfaction with scar appearance on an objective visual analog scale (VAS) from 1 to 10, with 10 indicating the most satisfaction. Prior to treatment, the average VAS score was 4.5. This score increased to 8.5 following one to four sessions of MN treatment with continued application of topical vitamin A and C twice daily. Histologic analysis of 3 mm punch biopsies at 1 year demonstrated an increase in collagen and elastin deposition both quantitatively and qualitatively using van Gieson and hematoxylin and eosin stains.
Studies with various-sized MN devices that evaluate the frequency and interval between treatments for optimal effects, would be an appropriate next step in further elaborating on the efficacy of MN. Many of the aforementioned studies demonstrated that MN had comparable efficacy to laser treatments for atrophic facial scars. However, MN is generally better tolerated with fewer long-term adverse sequelae.23 Scar type appears to be a factor affecting clinical response to MN, as icepick scars and deep-seated atrophic scars responded less ideally to treatment.15
Alopecia
MN has been proposed as a mechanism for adjuvant hair regrowth in alopecia. The efficacy of MN in both androgenetic alopecia (AGA) and AA has been highlighted over the last 5 years (Table 2).
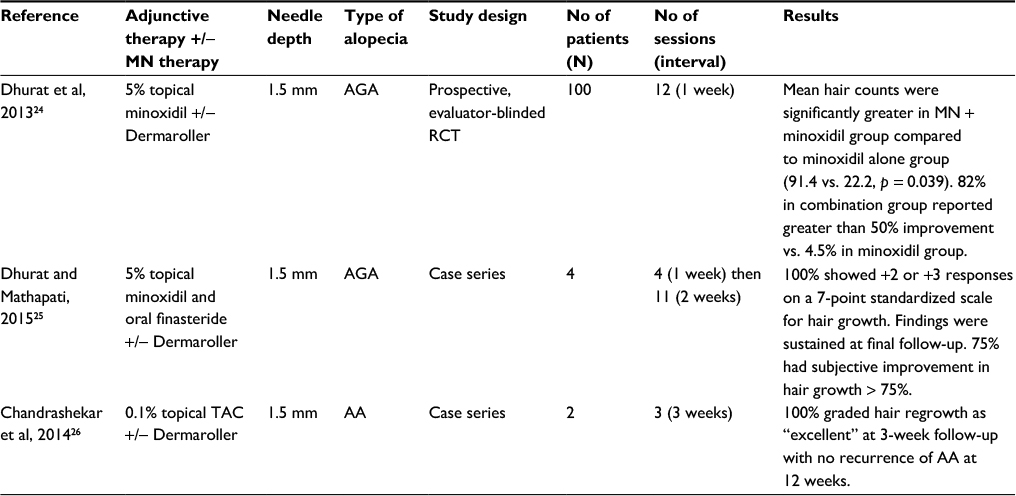 | Table 2 Alopecia treated with microneedling therapy Notes: Dermaroller®; Dermaroller Deutschland GmbH, Wolfenbuettel, Germany. Abbreviations: MN, microneedling; N, sample size; AGA, androgenetic alopecia; RCT, randomized controlled trial; TAC, triamcinolone; AA, alopecia areata. |
AGA
Dhurat et al found that combination treatment of MN with minoxidil was statistically superior to minoxidil alone in the treatment of 100 male patients with AGA.24 Over 12 weeks, Dermaroller treatment combined with 5% minoxidil lotion was administered to half of the participants, with 80% showing moderately or greatly increased hair regrowth per the investigators. Of the same subset, 82% of the patients reported subjective improvement greater than 50% in their hair growth. In the arm receiving 5% minoxidil alone, only 4.5% of patients reported greater than 50% improvement. By the end of the study, mean change in hair count was significantly greater for the MN group (91.4 vs. 22.2, p = 0.039). Additionally, the initiation of new hair growth was first noticeable at 6 weeks in the MN group compared to 10 weeks in the minoxidil alone group. No adverse effects were noted by any of the participants.24
Dhurat and Mathapati then published a follow-up case series of four men with AGA unresponsive to conventional treatments. Combination therapy was administered to participants with their prior treatment regimen (either topical minoxidil or oral finasteride) and Dermaroller over a course of 6 months.25 All four patients had moderately or greatly increased hair regrowth and reported subjective increases in hair thickness after 1 month of treatment.25
AA
MN has been proposed as a viable alternative to conventional treatment for AA as well. The mainstay of therapy for AA is currently intralesional corticosteroids, such as kenalog (ILK). However, the collagen induction offered by MN is thought to counter steroid-induced atrophy as well as cause less pain than injection.26
Chandrashekar et al analyzed outcomes from treating resistant AA with MN and topical corticosteroids.26 Two adult patients with AA recalcitrant to ILK, topical steroids, and minoxidil 5% lotion received topical triamcinolone applied before and after Dermaroller. Both patients graded hair regrowth as “excellent” and had no recurrence at 3-month follow-up. The ability to assess for common adverse effects of steroid treatment such as atrophy, scarring, and increased susceptibility to infection were limited in this study.
While these clinical studies show promising data for the efficacy of MN in the treatment of alopecia, these results are limited by relatively small sample sizes. Additionally, it is unclear if similar results are reproducible in women with hair disorders. Further investigations of combination therapy with minoxidil and finasteride, including MN frequency, needle size, and duration of treatment are needed to see if these results are reproducible in both genders and sustained over longer periods of time.
Pigmentary disorders
Several studies have proposed MN as an alternative to conventional treatment in disorders of pigmentation affecting darker skin types, including melasma, vitiligo, and periorbital hyperpigmentation (Table 3).
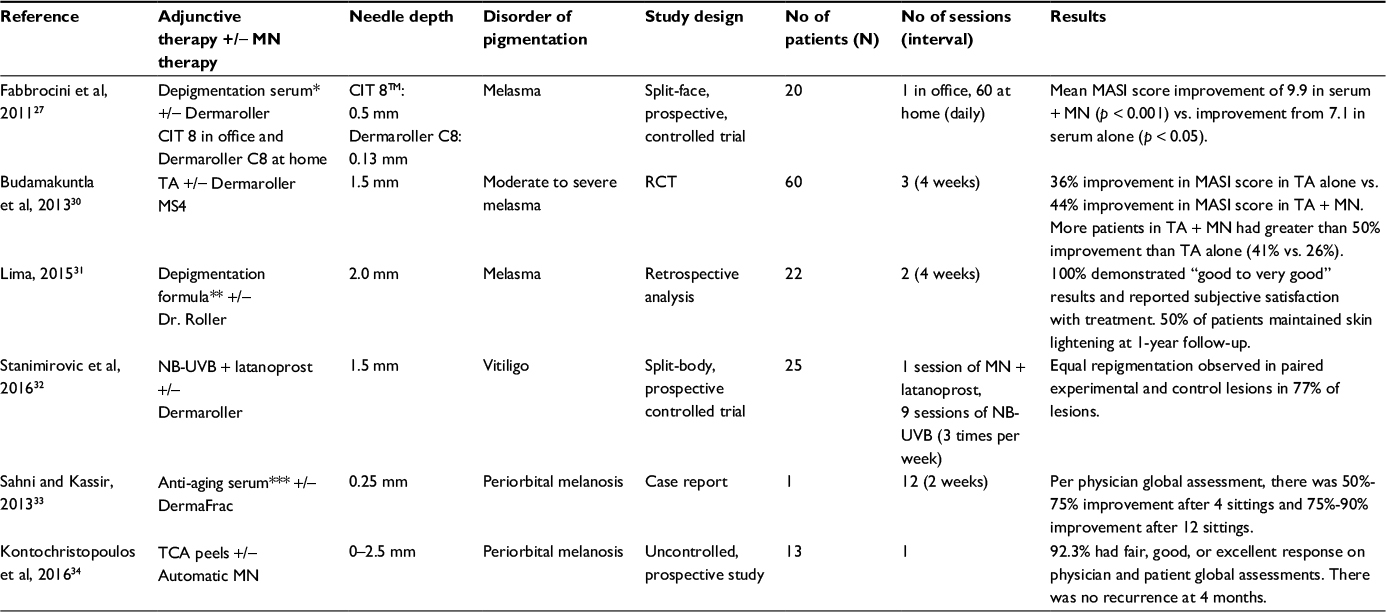 | Table 3 Disorders of pigmentation treated with microneedling therapy Notes: *Depigmentation serum: 4-butylresorcinol and sophora-alpha (prenylated flavonoids from the roots of Sophora flavescens). **Depigmentation formula: 0.05% tretinoin, 4% hydroquinone, and 1% fluocinonide and sunscreen SPF 60. ***Anti-aging serum: myristoyl pentapeptide 17 (SymPeptide), acetyl octapeptide-3 (SNAP 8), palmitoyl pentapeptide-4 (Matrixyl), acetyl hexapeptide-8 (Argirilene) and tripeptide (Syn-ake). Dermaroller®, Dermaroller CIT 8™, Dermaroller C8; and Dermaroller MS4™; Dermaroller Deutschland GmbH, Wolfenbuettel, Germany. Dr. Roller™; Vydence Medical, São Carlos, São Paulo, Brazil. DermaFrac™; Genesis Biosystems, Lewisville, TX, USA. Abbreviations: MN, microneedling; N, sample size; MASI, Melasma Area and Severity Index; RCT, randomized controlled trial; TA, tranexamic acid; NB-UVB, narrowband ultraviolet B; latanoprost, 0.005% latanoprost solution; TCA, 10% trichloroacetic acid; Automatic MN, Automatic Microneedle Therapy System-Handhold; CIT, collagen induction therapy. |
Melasma
The enhanced transdermal drug absorption seen with MN has achieved better results than skin lightening agents alone in the treatment of melasma.27–29 Budamakuntla et al observed enhanced results of MN followed by topical tranexamic acid in comparison to tranexamic acid microinjections in treating moderate to severe melasma in 60 patients.30 After three treatment sessions (at 0, 4, and 8 weeks), the patients were followed for 3 months. There was 35.72% improvement in the mean Melasma Area and Severity Index (MASI) score in the microinjection group (p < 0.01) compared to 44.41% in the MN group (p < 0.001). Notably, only 26% of patients in the microinjection group achieved 50% improvement compared to 41% in the MN group. Neither group experienced major side effects, but some reported mild discomfort, burning sensation, and erythema.30
In a pilot study, the use of depigmentation serum containing 4-butylresorcinol and sophora-alpha (prenylated flavonoids from the roots of Sophora flavescens) alone was compared to the combination treatment of depigmentation serum and MN (MN + serum) in 20 female patients (Fitzpatrick Skin Type III–IV) with melasma.27 In the MN + serum group, baseline mean MASI score decreased by 9.9 points (p < 0.001) compared to a 7.1 point decrease (p < 0.05) in the serum only group 2 months post-treatment. Results were confirmed by the significant increase in brightness of patients receiving combination treatment in comparison to the group receiving serum alone (17.4% vs. 11.2%; p < 0.05).27
MN combination therapy also has favorable results in melasma when combined with daily sunscreen use. In a retrospective analysis of 22 cases of recalcitrant melasma (unresponsive to topical bleaches and sunscreen), MN was administered followed by night time application of a depigmentation formula (0.05% tretinoin + 4% hydroquinone + 1% fluocinonide acetonide) and daily tinted sunscreen (SPF 60) 24 hours after initial skin needling.31 The procedure was repeated 30 days after the first treatment. All 22 patients reported satisfaction with results at 2 month follow-up. Photographic analysis at 24-month follow-up in eleven patients demonstrated continued maintenance of skin lightening observed at the 2-month visit.31
Vitiligo
The efficacy of MN in combination treatment for vitiligo remains unclear. Stanimirovic et al investigated repigmentation of patients with resistant bilateral symmetrical vitiligo by comparing treatment with narrowband ultraviolet B and topical 0.005% latanoprost solution with and without Dermaroller.32 Seventeen patients in each group had repigmentation (37.8% of treated lesions) and only 8.8% of repigmenting lesions had greater than 50% repigmentation. However, there was no statistically significant difference in repigmentation between groups.32
Periorbital melanosis
MN therapy has been successful in the treatment of periorbital hyperpigmentation. One male patient demonstrated 75%–90% improvement with DermaFrac treatment (combination of MN and active ingredients, including kojic acid or anti-aging serum containing myristoyl pentapeptide 17 [SymPeptide], acetyl octapeptide-3 [SNAP 8], palmitoyl pentapeptide-4 [Matrixyl], acetyl hexapeptide-8 [Argirilene] and tripeptide [Syn-ake]) after 12 sessions.33 The patient also reported 7 out of 10 improvement on the Patient’s Global Assessment scale in his pigmentation.
Kontochristopoulos et al also explored the use of MN in periorbital hyperpigmentation by treating 13 female patients with MN followed by 10% trichloroacetic acid peels.34 Almost all patients (92.3%) demonstrated significant improvement (“fair or better”) according to patient global assessments. Transient side effects including mild discomfort, edema, and erythema were commonly observed.34
MN therapy is promising in melasma and periorbital melanosis. Notably, MN poses a viable alternative to resurfacing procedures for darker skinned patients, given the lack of dyspigmentation as an adverse event. However, there are limited data to support its potential in improving vitiligo. Hence, there is a need for randomized controlled studies with larger populations to further explore the potential of MN as a treatment for pigmentation disorders in skin of color.
Verruca
The benefits of MN as a method of drug delivery in verruca was seen by Konicke and Olasz achieving complete cure rate in three patients (Table 4). MN was used in combination with 0.2–0.5 mL of topical bleomycin at 1 unit per mL over an average of 4 treatments.35 Notably, there was no tissue necrosis as seen with intralesional bleomycin and patients reported minimal pain. Comparatively, cure rates with intralesional bleomycin range from 0% to 95%, with variability attributed to poor infiltration of the lesion.36 MN may be a viable option for guaranteeing complete cure rates in plantar warts through enhancing the delivery of bleomycin in lesions.
 | Table 4 Verruca plantaris treated with microneedling therapy Abbreviations: MN, microneedling; N, sample size; Bleo, 0.2–0.5 mL of topical bleomycin; MN pen, microneedling pen-type device. |
Clinical trials with large sample sizes are needed to elucidate the actual role of MN in the treatment of verruca. The above study focused on the treatment of isolated verruca plantaris; thus, large clinical trials analyzing the efficacy of MN in the treatment of common warts would be an area of further research.
Actinic keratoses
Patients with AK have shown mixed results from MN as adjunctive therapy to currently accepted treatments (Table 5). In a split-face study, Torezan et al evaluated the use of MN after application of methyl aminolevulinate photodynamic therapy (MAL-PDT) compared to the use of MAL-PDT without MN in ten patients with AK.37 MAL-PDT combined with Dermaroller (MN-MAL-PDT) had greater improvement than MAL-PDT alone for all measured parameters, including photoaging and facial erythema (p = 0.01 for global score). Average AK clearance was 88.3%, with no statistically significant difference between the treatment arms (90.5% for MN-MAL-PDT side vs. 86% for MAL-PDT side). Pain level, based on VAS score, was greater on the MN-MAL-PDT side (6 vs. 4, p = 0.004). No prolonged side effects were observed. One patient in the MN group did develop a secondary bacterial infection which required treatment with oral antibiotics.37
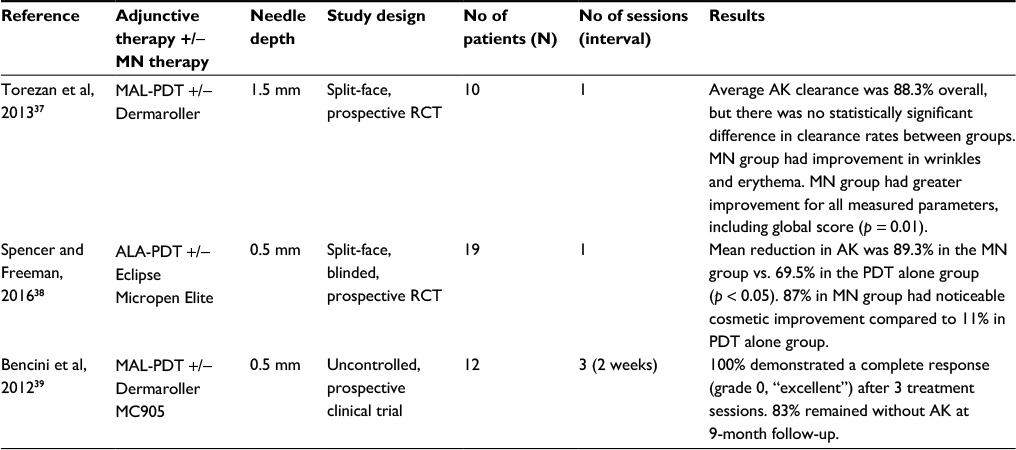 | Table 5 Actinic keratoses treated with microneedling therapy Notes: Dermaroller®; Dermaroller Deutschland GmbH, Wolfenbuettel, Germany. Eclipse Micropen Elite™; Eclipse Aesthetics, Dallas, TX, USA. Dermaroller MC905™; Alpha Strumenti, Milan, Italy. Abbreviations: MN, microneedling; N, sample size; MAL-PDT, methyl aminolevulinate photodynamic therapy; RCT, randomized controlled trial; AK, actinic keratoses; ALA-PDT, delta aminolevulinic acid photodynamic therapy. |
Spencer and Freeman demonstrated MN can enhance topical delta aminolevulinic acid PDT (ALA-PDT) in the treatment of AK.38 In their split-face study, 20 patients with at least four non-hyperkeratotic AK on each side of the face were randomly assigned to either MN therapy with Eclipse Micropen Elite™ followed by ALA-PDT or ALA-PDT alone. Researchers found a statistically significant difference (p < 0.05) between treatment groups, as average AK clearance was 89.3% in the MN-assisted side and 69.5% in the PDT only side. Furthermore, a blinded assessment found 15 patients achieved significant cosmetic improvement after 4 months, with 13 of the 15 patients having been in the MN treatment group. The procedure was safe and well tolerated with no significant side effects reported.38
The use of MN to treat AK was also evaluated in 12 organ transplant recipients with 59 AK unresponsive to classic PDT therapy.39 They received three sessions of cyclic PDT with use of Dermaroller MC905™ prior to topical application of 16% MAL. All lesions demonstrated a grade 0 (excellent) response after three sessions and were free of any new AK for at least 4 months. At 9 month follow-up, two of the patients had relapsed while the others remained clear. No adverse events were reported. The lack of a PDT alone comparison arm impaired the ability to assess the advantage offered solely by MN in the treatment of recurrent AK.39
Overall, MN shows promising results as an adjuvant therapy for the treatment of refractory AK. Large controlled clinical trials are needed to determine the utility of using MN for AK, especially on areas of the body other than the face.
Conclusion
Since the development of the first Dermaroller 20 years ago, a variety of new MN devices have been introduced. Accordingly, the applications of MN in dermatology have expanded to numerous indications over the past several years. This review highlights evidence of the potential for MN in the treatment of several dermatologic conditions, including disorders of pigmentation, premalignant lesions such as AK, scarring secondary to acne and surgical procedures, and hair pathologies. Advantages include, but are not limited to, the good tolerability of treatment among patients, increased transdermal delivery of drugs, and practicality of use in skin of color. Transient erythema is the most common adverse event.3 Granulomatous reaction in response to unauthorized use of topical products not approved for intradermal injection has been reported in three patients receiving MN therapy at medical spas.40 Otherwise, adverse events are rare and never result in systemic toxicity.3 Additionally, histologic analysis of skin following MN treatment has demonstrated an intact epidermis with no changes in melanocyte number, thereby having minimal risks of dyspigmentation relative to currently accepted treatments.41 Overall, MN offers a simple yet cost-effective therapeutic modality with minimal adverse events and a promising safety profile.
It is important to keep in mind that most comparative studies on MN have been case reports, case series, or small randomized controlled trials. Future large controlled clinical trials exploring the utility of MN are imperative to provide validation as more than a cosmeceutical therapy and as an evidence-based treatment option for patients with a variety of dermatologic disorders. This would help offset any potential publication bias as it is likely that small negative MN studies may not get published. Furthermore, the necessary number of treatment sessions and ideal MN settings including needling length and depth should be explored. Lastly, research elucidating the details of the mechanism of action of MN specifically in the treatment of alopecia and pigmentary disorders would be beneficial, as the micro-conduits created by MN are fast-healing and increased delivery in the dermis may not be the sole contributor to observed effects in these areas.
Disclosure
Doctor Olabola Awosika’s fellowship is funded by Janssen Biotech, Inc. The authors report no conflicts of interest in this work.
References
Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21(6):543–549. | ||
Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005;17(1):51–63. | ||
Doddaballapur S. Microneedling with dermaroller. J Cutan Aesthet Surg. 2009;2(2):110–111. | ||
Lee JC, Daniels MA, Roth MZ. Mesotherapy, microneedling, and chemical peels. Clin Plast Surg. 2016;43(3):583–595. | ||
McCrudden MT, McAlister E, Courtenay AJ, González-Vázquez P, Raj Singh TR, Donnelly RF. Microneedle applications in improving skin appearance. Exp Dermatol. 2015;24(8):561–566. | ||
Singh A, Yadav S. Microneedling: advances and widening horizons. Indian Dermatol Online J. 2016;7(4):244–254. | ||
Jeong K, Lee YJ, Kim JE, Park YM, Kim BJ, Kang H. Repeated microneedle stimulation induce the enhanced expression of hair-growth-related genes. Int J Trichol. 2012;4(2):117–130. | ||
Fabbrocini G, Fardella N, Monfrecola A, Proietti I, Innocenzi D. Acne scarring treatment using skin needling. Clin Exp Dermatol. 2009;34(8):874–879. | ||
Bahuguna A. Microneedling-Facts and Fictions. Asian J Med Sci. 2013;4:1–4. | ||
Arora S, Gupta BP. Automated microneedling device–A new tool in dermatologist’s kit–A review. J Pak Med Assoc. 2012;22:354–357. | ||
Chandrashekar BS, Sriram R, Mysore R, Bhaskar S, Shetty A. Evaluation of microneedling fractional radiofrequency device for treatment of acne scars. J Cutan Aesthet Surg. 2014;7(2):93–97. | ||
Bariya SH, Gohel MC, Mehta TA, Sharma OP. Microneedles: an emerging transdermal drug delivery system. J Pharm Pharmacol. 2012;64(1):11–29. | ||
US Food and Drug Administration. FDA Approval Letter - Fluzone Intradermal; 2009. Available from: http://www.fda.gov/BiologicsBloodVaccines/Vaccines/ApprovedProducts/ucm255160.htm. Accessed May 1, 2017. | ||
Milewski M, Mitra A. Recent developments in microneedle technology for transdermal drug delivery and vaccination. Drug Development Delivery; 2012. Available from: http://www.specialtypharma.com/Main/Back-Issues/Recent-Developments-in-Microneedle-Technology-for-48.aspx. Accessed June 23, 2017. | ||
El-Domyati M, Barakat M, Awad S, Medhat W, El-Fakahany H, Farag H. Microneedling therapy for atrophic acne scars: an objective evaluation. J Clin Aesthet Dermatol. 2015;8(7):36–42. | ||
Majid I. Microneedling therapy in atrophic facial scars: an objective assessment. J Cutan Aesthet Surg. 2009;2(1):26–30. | ||
Garg S, Baveja S. Combination therapy in the management of atrophic acne scars. J Cutan Aesthet Surg. 2014;7(1):18–23. | ||
Cachafeiro T, Escobar G, Maldonado G, Cestari T, Corleta O. Comparison of nonablative fractional erbium laser 1,340 nm and microneedling for the treatment of atrophic acne scars: a randomized clinical trial. Dermatol Surg. 2016;42(2):232–241. | ||
Dogra S, Yadav S, Sarangal R. Microneedling for acne scars in Asian skin type: an effective low cost treatment modality. J Cosmet Dermatol. 2014;13(3):180–187. | ||
Sharad J. Combination of microneedling and glycolic acid peels for the treatment of acne scars in dark skin. J Cosmet Dermatol. 2011;10(4):317–323. | ||
Eilers RE Jr, Ross EV, Cohen JL, Ortiz AE. A combination approach to surgical scars. Dermatol Surg. 2016;42(Suppl 2):S150–156. | ||
Aust MC, Knobloch K, Reimers K, et al. Percutaneous collagen induction therapy: an alternative treatment for burn scars. Burns. 2010;36(6):836–843. | ||
Hartmann D, Ruzicka T, Gauglitz GG. Complications associated with cutaneous aesthetic procedures. J Dtsch Dermatol Ges. 2015;13(8):778–786. | ||
Dhurat R, Sukesh M, Avhad G, Dandale A, Pal A, Pund P. A randomized evaluator blinded study of effect of microneedling in androgenetic alopecia: a pilot study. Int J Trichology. 2013;5(1):6–11. | ||
Dhurat R, Mathapati S. Response to microneedling treatment in men with androgenetic alopecia who failed to respond to conventional therapy. Indian J Dermatol. 2015;60(3):260–263. | ||
Chandrashekar B, Yepuri V, Mysore V, Charmalaya V. Alopecia areata--successful outcome with microneedling and triamcinolone acetonide. J Cutan Aesthet Surg. 2014;7(1):63–64. | ||
Fabbrocini G, De Vita V, Fardella N, et al. Skin needling to enhance depigmenting serum penetration in the treatment of melasma. Plast Surg Int. 2011;2011:158241. | ||
Fabbrocini G, De Vita V, Izzo R, Monfrecola G. The use of skin needling for the delivery of a eutectic mixture of local anesthetics. G Ital Dermatol Venereol. 2014;149(5):581–585. | ||
Escobar-Chavez JJ, Bonilla-Martinez D, Villegas-Gonzalez MA, Molina-Trinidad E, Casas-Alancaster N, Revilla-Vazuez AL. Microneedles: a valuable physical enhancer to increase transdermal drug delivery. J Clin Pharmacol. 2011;51(7):964–977. | ||
Budamakuntla L, Loganathan E, Suresh DH, et al. A randomised, open-label, comparative study of tranexamic acid microinjections and tranexamic acid with microneedling in patients with melasma. J Cutan Aesthet Surg. 2013;6(3):139–143. | ||
Lima Ede A. Microneedling in facial recalcitrant melasma: report of a series of 22 cases. An Bras Dermatol. 2015;90(6):919–921. | ||
Stanimirovic A, Kovacevic M, Korobko I, Situm M, Lotti T. Combined therapy for resistant vitiligo lesions: NB-UVB, microneedling, and topical latanoprost, showed no enhanced efficacy compared to topical latanoprost and NB-UVB. Dermatol Ther. 2016;29(5):312–316. | ||
Sahni K, Kassir M. DermafracTM: an innovative new treatment for periorbital melanosis in a dark-skinned male patient. J Cutan Aesthet Surg. 2013;6(3):158–160. | ||
Kontochristopoulos G, Kouris A, Platsidaki E, Markantoni V, Gerodimou M, Antoniou C. Combination of microneedling and 10% trichloroacetic acid peels in the management of infraorbital dark circles. J Cosmet Laser Ther. 2016;18(5):289–292. | ||
Konicke K, Olasz E. Successful treatment of recalcitrant plantar warts with bleomycin and microneedling. Dermatol Surg. 2016;42(8):1007–1008. | ||
Saitta P, Krishnamurthy K, Brown LH. Bleomycin in dermatology: a review of intralesional applications. Dermatologic Surgery. 2008;34(10):1299–1313. | ||
Torezan L, Chaves Y, Niwa A, Sanches JA, Festa-Neto C, Szeimies RM. A pilot split-face study comparing conventional methyl aminolevulinate- photodynamic therapy (PDT) with microneedling-assisted PDT on actinically damaged skin. Dermatol Surg. 2013;39(8):1197–1201. | ||
Spencer JM, Freeman SA. Microneedling prior to Levulan PDT for the treatment of actinic keratoses: a split-face, blinded trial. J Drugs Dermatol. 2016;15(9):1072–1074. | ||
Bencini PL, Galimberti MG, Pellacani G, Longo C. Application of photodynamic therapy combined with pre-illumination microneedling in the treatment of actinic keratosis in organ transplant recipients. Br J Dermatol. 2012;167(5):1193–1194. | ||
Soltani-Arabshahi R, Wong JW, Duff KL, Powell DL. Facial allergic granulomatous reaction and systemic hypersensitivity associated with microneedle therapy for skin rejuvenation. JAMA Dermatol. 2014:150(1):68–72. | ||
Aust MC, Reimers K, Repenning C, et al. Percutaneous collagen induction: minimally invasive skin rejuvenation without risk of hyperpigmentation- fact or fiction? Plast Reconstr Surg. 2008;122(5):1553–1563. | ||
Goodman GJ, Baron JA. Postacne scarring: a qualitative global scarring grading system. Dermatol Surg. 2006;32(12):1458–1466. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.