")
Back to Journals » Open Access Journal of Clinical Trials » Volume 6
Randomized controlled trial to evaluate the effect of canola oil on blood vessel function in peripheral arterial disease: rationale and design of the Canola-PAD Study
Authors Enns J, Zahradka P, Guzman R, Baldwin A, Foot B, Taylor C
Received 3 July 2014
Accepted for publication 14 August 2014
Published 25 October 2014 Volume 2014:6 Pages 117—125
DOI https://doi.org/10.2147/OAJCT.S70576
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Greg Martin
Jennifer E Enns,1,2 Peter Zahradka,1–3 Randolph P Guzman,4,5 Alanna Baldwin,1 Brendon Foot,1 Carla G Taylor1–3
1Canadian Centre for Agri-Food Research in Health and Medicine, St Boniface Research Centre, Winnipeg, Canada; 2Department of Physiology, University of Manitoba, Winnipeg, Manitoba, Canada; 3Department of Human Nutritional Sciences, University of Manitoba, Winnipeg, Manitoba, Canada; 4IH Asper Clinical Research Institute, St Boniface Hospital, Winnipeg, Canada; 5Section of Vascular Surgery, Department of Surgery, St Boniface Hospital, Winnipeg, Canada
Background: Individuals with peripheral arterial disease (PAD) are at high risk for cardiac events due to atherosclerosis. Dietary fatty acid composition has been shown to modulate blood vessel properties, but whether a diet enriched in conventional canola oil can improve clinical endpoints in PAD is not known.
Purpose: To describe the rationale and design of a clinical trial testing the effect of canola oil consumption on vascular function and cardiovascular risk factors in an 8-week dietary intervention in individuals with PAD.
Methods: The Canola-PAD Study was a single center, prospective, double-blind, randomized controlled trial in 50 patients over 40 years old with PAD. Participants were randomized into two groups and consumed food items containing either conventional canola oil (25 g/day) or an oil mixture representing the Western diet (25 g/day) for 8 weeks as part of their usual diet. The primary outcome was vascular function (ankle-brachial index, arterial stiffness, endothelial dysfunction, walking capacity, and cognitive function). Secondary measurements included anthropometrics, serum lipid profile and fatty acid composition, markers of inflammation and glycemic control, and serum metabolite profile.
Discussion: The Canola-PAD Study uses an innovative and noninvasive approach to evaluate the effect of canola oil on clinically relevant outcomes in individuals with PAD, including arterial stiffness, walking capacity, and cognitive function. The findings will help to inform clinical guidelines and recommendations for dietary fat intake.
Keywords: peripheral arterial disease, ankle-brachial index, arterial stiffness, vascular function, cognitive function, canola oil
Background
Peripheral arterial disease (PAD), a type of cardiovascular disease (CVD) affecting over 10 million individuals in North America, is characterized by the formation of atherosclerotic lesions in the blood vessels of the lower limbs. This disease leads to the loss of the vessels’ elastic properties (arterial stiffness) and reduces blood flow in the legs,1,2 causing ischemia and painful muscle cramping (intermittent claudication), which limits walking capacity. The gold standard for diagnosis of PAD is an ankle-brachial index (ABI) <0.9.2 As a result of the underlying atherosclerotic disease, individuals with PAD have a significantly greater risk of heart attack and stroke than the general population. It has also been demonstrated that increased arterial stiffness is associated with vascular dementia and decreases in the indices of memory and cognition.3,4
Dietary fat has long been implicated in the etiology of CVD. Epidemiological studies have collectively demonstrated that both the amount of fat in the diet and the fatty acid composition play a role in the maintenance of normal vascular tone.5 Vegetable oil consumption as well as higher intakes of monounsaturated fatty acids (MUFAs) and omega-3 fatty acids, such as α-linolenic acid (ALA), are associated with a decreased risk of PAD.6–9 Conventional canola oil is low in saturated fatty acids (SFAs), high in MUFAs, and is the best source of omega-3 fatty acids among the commonly consumed vegetable oils.10 Diet modeling studies have demonstrated that dietary recommendations for SFA (<7%–10% energy), MUFA (10% energy), and ALA (0.6%–1.2% energy) can be achieved with canola oil as the primary dietary fat source.11 However, these dietary recommendations for the amount and type of fatty acids are largely based on heart disease, whereas evidence for effects of canola oil in PAD, and particularly on vascular function, is lacking.
Noticeable symptoms are often absent in individuals with PAD, making it difficult to use preventative approaches in managing this condition. Although there has been considerable focus on serum cholesterol as a risk factor for CVD, there is increasing emphasis on the use of evidence-based clinical endpoints,12 such as vascular function, to identify presymptomatic disease and to evaluate the efficacy of therapeutic interventions. Indices of blood vessel function such as arterial compliance (elasticity/stiffness) and flow-mediated dilatation (endothelial dysfunction) can be monitored with instruments that provide rapid results with high sensitivity. It is generally agreed that these and related methods are capable of monitoring changes in vascular properties that become compromised early in the atherogenic process,13–17 and that they are appropriate for examining the changes that occur during short-term dietary interventions.18
We designed the Canola-PAD Study, a randomized controlled trial, to determine the effect of conventional canola oil consumption on functional and metabolic parameters of PAD. This study used ABI and noninvasive assessments of function in vivo as well as anthropometrics and serum biochemistry to establish whether canola oil has positive effects on vascular function and cardiovascular risk factors in individuals with PAD.
Methods and design
Study design and research aims
The Canola-PAD Study was a single-site, double-blinded, randomized, controlled dietary intervention trial conducted at the IH Asper Clinical Research Institute, St Boniface Hospital, Winnipeg, Canada. The primary aim of the study was to examine the effects of canola oil consumption on vascular function and cardiovascular risk factors in individuals with PAD. Specifically, we wanted to determine whether consumption of food products containing canola oil (25 g/day) is superior to those containing an oil mixture representing the Western diet (25 g/day). Participants in the two study arms (n=25/group) were provided with food items containing the study oils for consumption as part of their usual food intake for 8 weeks. The primary outcome was vascular function (ABI, arterial stiffness, endothelial dysfunction, walking capacity, and cognitive function), and secondary outcomes included anthropometrics, serum lipid profile and fatty acid composition, markers of inflammation and glycemic control, and serum and urinary metabolite profile. Assessments were completed at baseline and 8 weeks. The protocol was approved by the University of Manitoba Research Ethics Board and the St Boniface Hospital Research Review Committee. The study was registered with ICMJE (NCT01250275).
Inclusion and exclusion criteria
Patients diagnosed with PAD (ABI <0.9) who exhibited moderate hyperlipidemia (10-year risk 20%–30%, as defined by the recommendations for the management and treatment of dyslipidemia19), and absence of chronic illness or genetic causes of hypercholesterolemia were asked to join the study. The inclusion and exclusion criteria are detailed in Table 1.
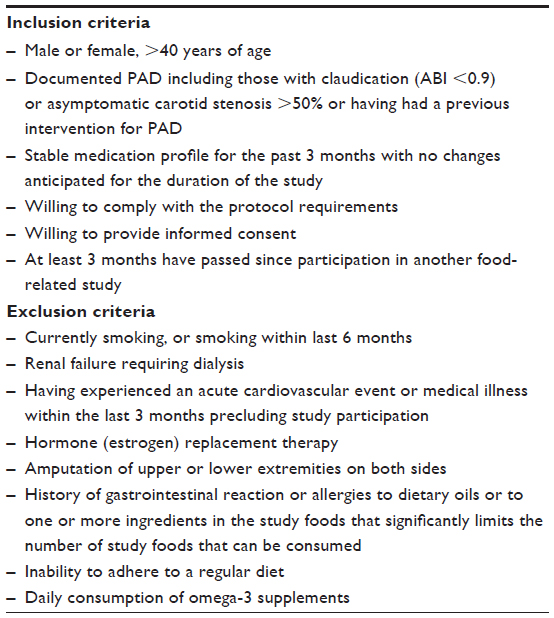 | Table 1 Canola-PAD Study inclusion and exclusion criteria |
Recruitment and screening visit
Recruitment and enrollment in the study are detailed in Figure 1. Participant recruitment began in October 2011, and the final participant completed the intervention in December 2012. Potential participants were identified through the Vascular Surgery Clinic at St Boniface Hospital, and were provided with a brief description of the study. Interested individuals attended a screening visit where they provided written informed consent before any study-related procedures were performed. The general consent form described the study schedule and dietary intervention, and detailed the biological materials that were to be collected (blood and urine), the procedure for storing the samples, the specific analyses planned, and the potential risks associated with sampling of biological fluids. A separate consent form gave participants the option of allowing nontargeted analysis of plasma and urine samples using a metabolomics approach and gene expression analysis of saliva samples.
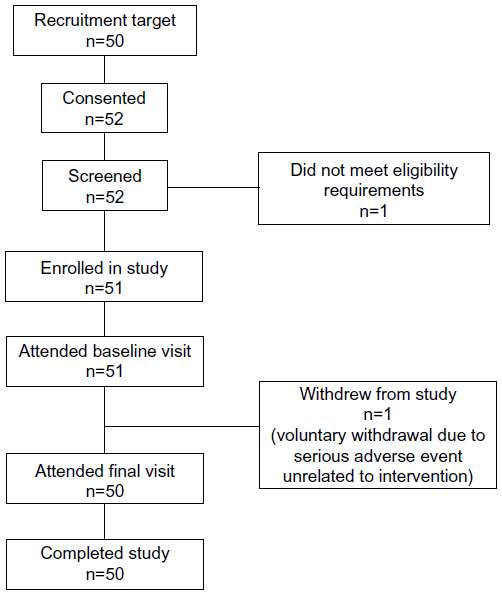 | Figure 1 Study flow chart. |
Participants who gave consent underwent a complete medical history including age, sex, alcohol use, exercise habits, current medical problems including documented PAD, medication intake including supplements, and a family history of previous events (eg, hypertension, heart disease, stroke, and diabetes). A blood sample was obtained by finger tip puncture for measurement of glycated hemoglobin. Participants completed the Mini Mental State Examination (MMSE) to screen for cognitive impairment. Participants who scored ≤23 on the MMSE were not included in further cognitive testing; however, they did remain in the study and participated in all of the other noncognitive assessments. Participants also completed a food frequency questionnaire20 to determine usual food consumption, including visible oils/fats and foods containing fat, as well as a questionnaire to record any food allergies and food dislikes/dietary preferences. To assess background dietary intake (including fat intake), a 3-day food record was distributed and completed before the baseline visit.
Randomization and blinding
The randomization sequence was prepared from a random-numbers table and individual assignments were stored in opaque envelopes. To ensure that there was equal representation of type 2 diabetes within both arms of the study, participants were first stratified according to their glycated hemoglobin levels (≤6% or >6%), and then randomly assigned to one of the two dietary treatment groups. To reduce potential bias during data collection and evaluation of study endpoints, both the research team (ie, individuals who interacted directly with the participants and those involved in analysis of the samples) and the participants were blinded to the dietary intervention from the time of randomization for the duration of the study.
Baseline and week-8 assessments
Participants were assessed for changes to their medication profile and current medical conditions throughout the study. Anthropometrics (height, body weight, body mass index, body fat distribution, waist circumference) and blood pressure were obtained. A fasting blood sample was drawn for assessment of fasting plasma lipid profile (total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides), glucose, insulin, glycated hemoglobin, markers of vascular function, oxidative stress and inflammation, fatty acid composition, and nontargeted metabolomics analysis (where consent was given). A urine sample was also collected to assess markers of vascular function and metabolism.
Noninvasive assessment of vascular function included measurement of ABI and arterial stiffness (brachial-to-ankle pulse wave velocity) using the Omron VP-1000 vascular profiler (Omron Healthcare Inc., Lake Forest, IL, USA). Radial pulse wave analysis was conducted using the SphygmoCor pulse wave monitoring system (AtCor Medical, Sydney, NSW, Australia) and SphygmoCor Px Aortic BP waveform analysis software (AtCor Medical). Endothelial function was assessed using the Itamar EndoPAT-2000 device (Itamar Medical Inc., Franklin, MA, USA). Advanced glycation end products (AGEs) were assessed by an AGE reader (Diagnoptics Technologies, Groningen, Netherlands). A selection of cognitive tests was administered to assess various aspects of the participant’s level of functioning cognition. Each of the following tests was administered by trained study staff: i) Hopkins Verbal Learning Test, an assessment of verbal learning and memory; ii) Digit Symbol Similarities Test, an assessment of executive functioning, including perceptual speed, motor speed, visual scanning, and memory; and iii) Digit Span Test, a measurement of short-term memory and working memory. Cognitive testing data from patients with severe internal carotid artery stenosis (≥70%) will be excluded from analysis because of the potential of this condition to influence cognitive function.21
Participants were asked to undertake a treadmill test22 to establish pain-free walking distance (distance and time at the onset of claudication) and maximum walking distance (total distance and time).
Intervention
Participants were provided with a 2- to 3-week supply of frozen food items including entrées, side dishes, salad dressing, and baked goods (Table 2) containing conventional canola oil (25 g/day) or an oil mixture representing the typical Western diet (25 g/day), to be consumed daily as part of their usual food intake. A dose of 25 g/day was chosen, as it would provide ~40% of the daily fat intake (based on a total fat intake of 67 g/day assuming that this population consumes ~1,800 kcal/day and 30% energy from fat) and this amount could be accommodated within 1–2 food items per day. The two study arms provide a comparison of conventional canola oil (low SFA, high MUFA, and good source of omega-3 polyunsaturated fatty acid [PUFA]) with an oil mixture representing the Western diet. The Western diet is characterized by high intakes of high-fat (high SFA and rich in omega-6 PUFA23,24) and high-sugar foods. In our study, the fatty acid composition of the canola oil-containing foods (100% conventional canola oil) would provide 6% SFA, 62% MUFA, 32% PUFA (2:1 ratio for omega-6:omega-3 PUFA), whereas the fatty acid composition of the food items containing the oil mixture representing the Western diet (2:1:1 ratio of butter, coconut oil, high linoleic safflower oil) would provide 59% SFA, 20% MUFA, and 22% PUFA (50:1 ratio for omega-6:omega-3 PUFA); these fatty acid compositions will be verified by gas chromatography by sampling food products throughout the study. Furthermore, the analysis of the 3-day food records (before baseline and during week 6) will be used to interpret how the consumption of the study foods changes the overall dietary fatty acid profile in canola oil and control groups.
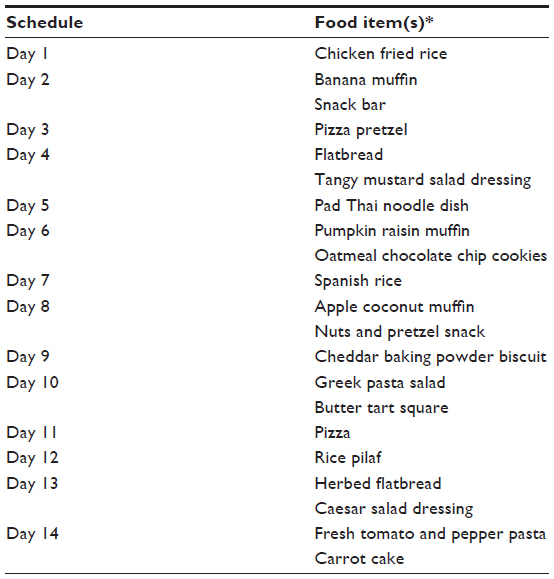 | Table 2 Two-week cycle of study food products |
The food items were based on standard recipes and modified appropriately for the dose of oil and according to sensory testing. Food preparation was done in the Department of Human Nutritional Sciences, University of Manitoba, Winnipeg, Canada. The food items were similar in appearance, calories, and macronutrient and micronutrient composition between the two groups. Participants received a 2-week supply of frozen food items at the baseline visit. For convenience, the food items for the rest of the study were delivered to participants at their homes at the end of Weeks 2 and 5. The food items were also available to immediate family members to assist with compliance.
Dietary adherence and safety measures
During Weeks 2 and 5, participants were contacted by the study staff by telephone to assess their compliance and tolerability of the study foods, report any adverse changes in medical conditions or adverse events, and to identify food preferences. Participants were given the opportunity to modify the selection of food items they were provided for the next 3-week period, and they were reminded to complete a 3-day food record at Week 6 to be submitted at the final study visit. Dietary adherence will also be assessed by reviewing the 3-day food records for inclusion of study food items and by analyzing the plasma phospholipid fatty acid profile before and after the intervention.
Although consumption of the study food products was not considered to pose significant risk to the participants, any adverse changes in medical conditions or adverse events taking place during the study period were recorded, whether or not they required medical attention. The severity, duration, relation to the study food product, clinical action taken, and outcome of each adverse event were noted and reviewed by the clinical co-investigator (RPG). Twenty-one adverse events were reported: two occurrences of nausea, one each of flatulence and indigestion, and all others were not related to the food products. One serious adverse event was reported; this serious adverse event was not related to the study food products, but required the individual to withdraw from the study. The serious adverse event was promptly reported to the University of Manitoba Research Ethics Board. Participants were free to withdraw from the study at any time for any reason, without penalty.
Statistical considerations and data analysis
Since there have been no previous studies investigating a canola oil intervention in PAD, we calculated the sample size based on a previous study we conducted in PAD participants using pulses (dried beans, dried peas, lentils, and chickpeas) as the 8-week dietary intervention and ABI as the primary outcome.25 This resulted in a total sample size of 44 participants (n=22/group) to give a statistical power of 0.80 to detect a 5% change in ABI from baseline to 8 weeks with a probability of P=0.05. We rounded up the sample size to 50 (n=25/group) to allow for the differing interventions, and any dropouts were replaced.
To compare the data on vascular function, anthropometrics, and biochemical assessments between the dietary groups at 8 weeks, we will use analysis of covariance models with 8-week values as the outcome, diet as the main effect, and baseline measurements as a covariate. Additional covariates will be considered for inclusion in the model when it is believed they are strongly associated with the outcome being modeled, and when randomization does not lead to sufficiently comparable baseline values between the groups. This approach provides optimal statistical power for detecting a diet effect and adjusts for any baseline differences between groups. Analyses will be performed with PROC GLM using the Statistical Analysis Software.26 The level of significance will be set at P<0.05.
Discussion
PAD is a type of atherosclerotic disease that occurs in the vessels of the limbs, and is associated with a tenfold increased risk for cardiovascular events, changes in cognitive function, and a reduction in quality of life due to limited walking capacity and mobility.1,2 PAD is present in as many as 14% of Americans between 50 and 80 years of age.27 Lifestyle changes are important in preventing and treating this condition, as smoking and a sedentary lifestyle are major risk factors for PAD.28,29 Dietary choices can also impact vascular function, as nutrient and dietary interventions have been shown to provide an acute means for improving arterial stiffness by targeting the functional mechanisms that regulate vascular tone.30
This trial aims to provide valuable data on the effects of canola oil consumption on vascular function and cardiovascular risk factors in individuals with PAD. To the best of our knowledge, this is the first randomized, controlled trial in PAD to use canola oil, which is low in SFAs, high in MUFAs, and the best source of omega-3 fatty acids among commonly consumed vegetable oils, as the primary source (up to one-half) of fat in the diet. A recent review describes the positive effects of consuming canola oil on circulating lipid levels and insulin sensitivity.31 The combination of MUFA and the omega-3 fatty acid ALA in canola oil may also deliver synergistic benefits to PAD individuals with type 2 diabetes and obesity by modulating gene expression, insulin signaling, fatty acid metabolism, and tissue lipid accumulation.10 Vascular function has been shown to improve with fish oil consumption in individuals with CVD,32,33 but very few trials have investigated the effects of MUFAs or ALA on blood vessels, and these have used food sources such as flaxseed oil, sunola oil, and walnuts,34–37 but not canola oil.
The Canola-PAD Study employed several noninvasive vascular testing methods to assess vascular function. Pulse wave velocity is a measure of the time taken for a pressure wave to travel a specific distance, and is considered the gold standard method for measuring arterial stiffness because it is simple, noninvasive, robust, and reproducible.38 Pulse wave velocity is increased in people with arterial stiffness, and age-specific reference values have been established.39 Pulse wave analysis examines the shape of the pulse wave and provides an indirect measure of arterial stiffness through augmentation of the pulse wave by the reflected waveform. In our study, the peripheral pulse wave was recorded at the radial artery via applanation tonometry. The software uses algorithms to calculate the aortic augmentation index, a measure of how much the central aortic pressure is augmented by the increased pulse wave reflection in people with vascular disease,38 and this affects the workload on the heart. Together, pulse wave velocity and pulse wave analysis provide information on systemic arterial stiffness, central aortic pressure, and other hemodynamic parameters not obtained during measurement of blood pressure. The utility of these measurements in predicting adverse cardiovascular outcomes has been validated40,41 and is supported by extensive clinical data.38 Measuring endothelial function using EndoPAT technology provides data on the responsiveness of the endothelial vasomotor response before and during reactive hyperemia. Peripheral arterial tonometry (PAT) involves recording the finger arterial pulse wave amplitude, which is a measure of pulsatile volume changes.42 Abnormalities in the pulse wave amplitude are indicative of atherosclerotic disease.43 Endothelial dysfunction has been demonstrated to be an adequate surrogate marker for vascular function, and is associated with cardiovascular risk factors.44,45 The AGE reader measures tissue accumulation of AGEs by means of skin autofluorescence. While not strictly a measure of vascular function, this noninvasive technology provides data on cardiovascular risk, since AGEs have been shown to contribute to oxidative stress and are associated with microvascular and macrovascular complications in type 2 diabetes.46
Cardiovascular factors have long been recognized as drivers in the vascular pathogenesis of cognitive decline.47,48 Arterial stiffness is one such pathophysiological process that has been linked to accelerated cognitive aging.3,48–50 The neuropsychological function of PAD patients has not been well studied, especially in response to intervention. In the Canola-PAD Study, we used three tests to obtain a well-rounded assessment of performance in various cognitive domains. The Hopkins Verbal Learning Test51 assesses verbal learning and semantic memory. This test has been used in patients with coronary heart disease to demonstrate an improvement in cognitive function following cardiac surgical procedures.52,53 The Digit Symbol Similarities Test54 assesses the participants’ executive functioning, including perceptual speed, motor speed, visual scanning, and memory. Lower performance in this test has been associated with the presence of vascular disease (ABI <0.9 or intermittent claudication).55–57 The Digit Span Test54 measures short-term memory, attention, and concentration. Several studies have demonstrated a link between PAD and neuropsychological deficits using this test score.58,59 These tests were selected for the Canola-PAD Study because they are well validated and internationally recognized with high retest reliability and interadministrator dependability.60–64 Our study will examine whether data from the cognitive function tests are correlated to changes in arterial stiffness in individuals with PAD consuming the different dietary fats.
Positive aspects of the Canola-PAD Study
Several aspects of the trial design aided participant recruitment and compliance. All participants were recruited through the St Boniface Hospital Vascular Surgery Clinic, and remained under the care of their vascular surgeon (RPG), proving continuity of care during the intervention. Participants were provided with their results from the vascular function assessments, and most were interested to learn about their vascular health. The study food items were generally well accepted and tolerated. The ability to tailor the food items participants received to their individual dietary preferences was appreciated, and making the food items available to participants’ family members was also thought to improve compliance.
Challenges and limitations
One of the challenges in conducting this trial was working with participants who were for the most part elderly and not very mobile. Some participants declined to undergo treadmill testing for various reasons, such as needing a walking aid (cane/walker), or they felt that the 12% treadmill incline would be too difficult to manage safely. Obtaining blood samples was sometimes problematic, since the participants’ peripheral blood vessels could be frail and easily collapse. Some participants found the 3-hour visit required to conduct all of the vascular assessments and tests to be taxing and too lengthy. However, they were satisfied with the organization of the study where all phlebotomy services and vascular testing occurred in a single clinic at the Asper Clinical Research Institute.
Summary
In summary, we expect that the Canola-PAD Study will provide data on the effectiveness of the canola oil intervention on clinically relevant outcomes for vascular function, including ABI, arterial stiffness, walking capacity and cognitive function, in individuals with PAD. We will be able to evaluate direct effects on blood vessel function via the noninvasive assessments of pulse wave analysis and pulse wave velocity, and to compare these results with changes in CVD risk markers. The study will provide important information on the safety and tolerability of a diet enriched in canola oil compared to a typical Western diet oil mixture in a PAD population. The findings may also support current recommendations for canola oil consumption as a healthy source of dietary fat for management of PAD.
Acknowledgments
We wish to thank the members of the research team who helped us with participant recruitment and screening (Wendy Weighell, Terri Gregor), vascular assessments (Wendy Weighell, Terri Gregor, Angela Wilson, and Brendon Foot), neurological assessments (Angela Wilson and Brendon Foot), blood sample collection (Terri Gregor and Angela Wilson), and sample processing (Raissa Perrault, Shannon Neumann, Danielle Hanke, and Leslee Tworek) at the Asper Clinical Research Institute. Our thanks are due to Kristy Loewen for developing the study food products and to Dr Michel Aliani and Donna Ryland for advice and access to the facilities in the Barbara Burns Food Innovation Laboratory, Department of Human Nutritional Sciences, University of Manitoba. Also, we thank the team members responsible for food preparation (Kristy Loewen, Haylie Koslowsky, and Hilary Wilson) and deliveries (Karlee Dyck, Amanda Hamel, and Meagan Einarson). Dr Doug Staley (Office of Clinical Research, St Boniface Hospital) and Brenden Dufault (Center for Healthcare Innovation, University of Manitoba) are thanked for advice regarding the sample size calculation and statistical analyses, respectively. This study was funded by the Canola Council of Canada through the Canola/Flax Canadian Agri-Science Cluster.
Author contributions
CGT and PZ conceived, designed, and oversaw the study. RPG provided oversight of data acquisition, including patient recruitment and care during the intervention. AB and BF maintained regulatory oversight and were involved in data acquisition. JEE drafted the manuscript with CGT and PZ, and these authors are involved in ongoing data analysis and interpretation. All authors critically reviewed and approved the manuscript, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Aslam F, Haque A, Foody J, Lee LV. Peripheral arterial disease: current perspectives and new trends in management. South Med J. 2009;102(11):1141–1149. | |
Mukherjee D, Cho L. Peripheral arterial disease: considerations in risks, diagnosis, and treatment. J Natl Med Assoc. 2009;101(10):999–1008. | |
Waldstein SR, Rice SC, Thayer JF, Najjar SS, Scuteri A, Zonderman AB. Pulse pressure and pulse wave velocity are related to cognitive decline in the Baltimore longitudinal study of aging. Hypertension. 2008;51(1):99–104. | |
Poels MM, van Oijen M, Mattace-Raso FU, et al. Arterial stiffness, cognitive decline, and risk of dementia: the Rotterdam study. Stroke. 2007;38(3):888–892. | |
Hall WL. Dietary saturated and unsaturated fats as determinants of blood pressure and vascular function. Nutr Res Rev. 2009;22(1):18–38. | |
Ciccarone E, Di Castelnuovo A, Salcuni M, et al; Gendiabe Investigators. A high-score Mediterranean dietary pattern is associated with a reduced risk of peripheral arterial disease in Italian patients with type 2 diabetes. J Thromb Haemost. 2003;1(8):1744–1752. | |
Gimeno SG, Hirai AT, Harima HA, et al; Japanese-Brazilian Diabetes Study Group. Fat and fiber consumption are associated with peripheral arterial disease in a cross-sectional study of a Japanese-Brazilian population. Circ J. 2008;72(1):44–50. | |
Lane JS, Magno CP, Lane KT, Chan T, Hoyt DB, Greenfield S. Nutrition impacts the prevalence of peripheral arterial disease in the United States. J Vasc Surg. 2008;48(4):897–904. | |
Katsouyanni K, Skalkidis Y, Petridou E, Polychronopoulou-Trichopoulou A, Willett W, Trichopoulos D. Diet and peripheral arterial occlusive disease: the role of poly-, mono-, and saturated fatty acids. Am J Epidemiol. 1991;133(1):24–31. | |
Hanke D, Love K, Noto A, Zahradka P, Taylor CG. Canola oil: evolving research in obesity and insulin resistance. In: Thiyam-Hollander U, Eskin NAM, Matthaus B, editors. Canola and Rapeseed: Production, Processing, Food Quality, and Nutrition. New York, NY: CRC Press (Taylor and Francis Group); 2013:252–276. | |
Johnson GH, Keast DR, Kris-Etherton PM. Dietary modeling shows that the substitution of canola oil for fats commonly used in the United States would increase compliance with dietary recommendations for fatty acids. J Am Diet Assoc. 2007;107(10):1726–1734. | |
Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(13):1425–1443. | |
Al-Qaisi M, Kharbanda RK, Mittal TK, Donald AE. Measurement of endothelial function and its clinical utility for cardiovascular risk. Vasc Health Risk Manag. 2008;4(3):647–652. | |
Lane HA, Smith JC, Davies JS. Noninvasive assessment of preclinical atherosclerosis. Vasc Health Risk Manag. 2006;2(1):19–30. | |
Simon A, Chironi G, Levenson J. Comparative performance of subclinical atherosclerosis tests in predicting coronary heart disease in asymptomatic individuals. Eur Heart J. 2007;28(24):2967–2971. | |
Wang X, Keith JC Jr, Struthers AD, Feuerstein GZ. Assessment of arterial stiffness, a translational medicine biomarker system for evaluation of vascular risk. Cardiovasc Ther. 2008;26(3):214–223. | |
Cohn JN, Duprez DA, Grandits GA. Arterial elasticity as part of a comprehensive assessment of cardiovascular risk and drug treatment. Hypertension. 2005;46(1):217–220. | |
Stamatelopoulos K, Karatzi K, Sidossis LS. Noninvasive methods for assessing early markers of atherosclerosis: the role of body composition and nutrition. Curr Opin Clin Nutr Metab Care. 2009;12(5):467–473. | |
Genest J, Frohlich J, Fodor G, McPherson R; Working Group on Hypercholesterolemia and other Dyslipidemias. Recommendations for the management of dyslipidemia and the prevention of cardiovascular disease: summary of the 2003 update. CMAJ. 2003;169(9):921–924. | |
Shatenstein B, Payette H, Nadon S, Gray-Donald K; Division on Nutrition and Healthy Aging, Quebec Network on Aging Research. An approach for evaluating lifelong intakes of functional foods in elderly people. J Nutr. 2003;133(7):2384–2391. | |
Lin CJ, Tu PC, Chern CM, et al. Connectivity features for identifying cognitive impairment in presymptomatic carotid stenosis. PLoS One. 2014;9(1):e85441. | |
Bruce RA. Exercise testing of patients with coronary heart disease. Principles and normal standards for evaluation. Ann Clin Res. 1971;3(6):323–332. | |
Odermatt A. The Western-style diet: a major risk factor for impaired kidney function and chronic kidney disease. Am J Physiol Renal Physiol. 2011;301(5):F919–F931. | |
Ooi EM, Ng TW, Watts GF, Barrett PH. Dietary fatty acids and lipoprotein metabolism: new insights and updates. Curr Opin Lipidol. 2013;24(3):192–197. | |
Zahradka P, Wright B, Weighell W, et al. Daily non-soy legume consumption reverses vascular impairment due to peripheral artery disease. Atherosclerosis. 2013;230(2):310–314. | |
SAS Institute Inc. SAS version 9.3. Cary, NC: SAS Institute Inc.; 2011. | |
Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the national health and nutrition examination survey, 1999–2000. Circulation. 2004;110(6):738–743. | |
Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286(11):1317–1324. | |
Syvanen K, Korhonen P, Partanen A, Aarnio P. Endothelial function in a cardiovascular risk population with borderline ankle-brachial index. Vasc Health Risk Manag. 2011;7:97–101. | |
Brostow DP, Hirsch AT, Collins TC, Kurzer MS. The role of nutrition and body composition in peripheral arterial disease. Nat Rev Cardiol. 2012;9(11):634–643. | |
Lin L, Allemekinders H, Dansby A, et al. Evidence of health benefits of canola oil. Nutr Rev. 2013;71(6):370–385. | |
Lovegrove JA, Griffin BA. The acute and long-term effects of dietary fatty acids on vascular function in health and disease. Curr Opin Clin Nutr Metab Care. 2013;16(2):162–167. | |
Wang Q, Liang X, Wang L, et al. Effect of omega-3 fatty acids supplementation on endothelial function: a meta-analysis of randomized controlled trials. Atherosclerosis. 2012;221(2):536–543. | |
Nestel PJ, Pomeroy SE, Sasahara T, et al. Arterial compliance in obese subjects is improved with dietary plant n-3 fatty acid from flaxseed oil despite increased LDL oxidizability. Arterioscler Thromb Vasc Biol. 1997;17(6):1163–1170. | |
Ros E, Núñez I, Pérez-Heras A, et al. A walnut diet improves endothelial function in hypercholesterolemic subjects: a randomized crossover trial. Circulation. 2004;109(13):1609–1614. | |
Cortés B, Núñez I, Cofán M, et al. Acute effects of high-fat meals enriched with walnuts or olive oil on postprandial endothelial function. J Am Coll Cardiol. 2006;48(8):1666–1671. | |
West SG, Krick AL, Klein LC, et al. Effects of diets high in walnuts and flax oil on hemodynamic responses to stress and vascular endothelial function. J Am Coll Nutr. 2010;29(6):595–603. | |
Laurent S, Cockcroft J, Van Bortel L, et al; European Network for Non-invasive Investigation of Large Arteries. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27(21):2588–2605. | |
Reference Values for Arterial Stiffness’ Collaboration. Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: ‘establishing normal and reference values’. Eur Heart J. 2010;31(19):2338–2350. | |
Weber T, Wassertheurer S, Rammer M, et al. Validation of a brachial cuff-based method for estimating central systolic blood pressure. Hypertension. 2011;58(5):825–832. | |
Asmar R, Benetos A, Topouchian J, et al. Assessment of arterial distensibility by automatic pulse wave velocity measurement. Validation and clinical application studies. Hypertension. 1995;26(3):485–490. | |
Poredos P, Jezovnik MK. Testing endothelial function and its clinical relevance. J Atheroscler Thromb. 2013;20(1):1–8. | |
Perticone F, Ceravolo R, Pujia A, et al. Prognostic significance of endothelial dysfunction in hypertensive patients. Circulation. 2001;104(2):191–196. | |
Celermajer DS, Sorensen KE, Gooch VM, et al. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet. 1992;340(8828):1111–1115. | |
Kuvin JT, Patel AR, Sliney KA, et al. Assessment of peripheral vascular endothelial function with finger arterial pulse wave amplitude. Am Heart J. 2003;146(1):168–174. | |
Goldin A, Beckman JA, Schmidt AM, Creager MA. Advanced glycation end products: sparking the development of diabetic vascular injury. Circulation. 2006;114(6):597–605. | |
Hanon O, Haulon S, Lenoir H, et al. Relationship between arterial stiffness and cognitive function in elderly subjects with complaints of memory loss. Stroke. 2005;36(10):2193–2197. | |
Gorelick PB, Scuteri A, Black SE, et al. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42(9):2672–2713. | |
Benetos A, Watfa G, Hanon O, et al; PARTAGE Study Investigators. Pulse wave velocity is associated with 1-year cognitive decline in the elderly older than 80 years: the PARTAGE study. J Am Med Dir Assoc. 2012;13(3):239–243. | |
Watson NL, Sutton-Tyrrell K, Rosano C, et al. Arterial stiffness and cognitive decline in well-functioning older adults. J Gerontol A Biol Sci Med Sci. 2011;66(12):1336–1342. | |
Brandt J, Benedict RHB. The Hopkins Verbal Learning Test – Revised; Professional manual. Lutz, FL: Psychological Assessment Resources, Inc. 2001. | |
Lal BK, Younes M, Cruz G, Kapadia I, Jamil Z, Pappas PJ. Cognitive changes after surgery vs stenting for carotid artery stenosis. J Vasc Surg. 2011;54(3):691–698. | |
Rosengart TK, Sweet J, Finnin EB, et al. Neurocognitive functioning in patients undergoing coronary artery bypass graft surgery or percutaneous coronary intervention: evidence of impairment before intervention compared with normal controls. Ann Thorac Surg. 2005;80(4):1327–1334; discussion 1334–1335. | |
Wechsler D. Wechsler Adult Intelligence Scale – Revised. New York: Psychological Corporation; 1981. | |
Waldstein SR, Tankard CF, Maier KJ, et al. Peripheral arterial disease and cognitive function. Psychosom Med. 2003;65(5):757–763. | |
Rafnsson SB, Deary IJ, Smith FB, Whiteman MC, Fowkes FG. Cardiovascular diseases and decline in cognitive function in an elderly community population: the Edinburgh Artery Study. Psychosom Med. 2007;69(5):425–434. | |
Haan MN, Shemanski L, Jagust WJ, Manolio TA, Kuller L. The role of APOE epsilon4 in modulating effects of other risk factors for cognitive decline in elderly persons. JAMA. 1999;282(1):40–46. | |
Phillips NA, Mate-Kole CC. Cognitive deficits in peripheral vascular disease. A comparison of mild stroke patients and normal control subjects. Stroke. 1997;28(4):777–784. | |
Mangiafico RA, Sarnataro F, Mangiafico M, Fiore CE. Impaired cognitive performance in asymptomatic peripheral arterial disease: relation to C-reactive protein and D-dimer levels. Age Ageing. 2006;35(1):60–65. | |
Brandt J. The Hopkins verbal learning test: development of a new memory test with six equivalent forms. Clin Neuropsychol. 1991;5(2):125–142. | |
Benedict RHB, Schretlen D, Groninger L, Brandt J. The Hopkins verbal learning test-revised: normative data and analysis of interform and test-retest reliability. Clin Neuropsychol. 1998;12:43–55. | |
Shapiro AM, Benedict RH, Schretlen D, Brandt J. Construct and concurrent validity of the Hopkins verbal learning test-revised. Clin Neuropsychol. 1999;13(3):348–358. | |
Schroeder RW, Twumasi-Ankrah P, Baade LE, Marshall PS. Reliable digit span: a systematic review and cross-validation study. Assessment. 2012;19(1):21–30. | |
Rasmusson DX, Bylsma FW, Brandt J. Stability of performance on the Hopkins verbal learning test. Arch Clin Neuropsychol. 1995;10(1):21–26. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.