")
Back to Journals » Psychology Research and Behavior Management » Volume 7
Psychological treatments for gambling disorder
Received 29 May 2014
Accepted for publication 24 June 2014
Published 7 October 2014 Volume 2014:7 Pages 285—295
DOI https://doi.org/10.2147/PRBM.S40883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Carla J Rash, Nancy M Petry
Department of Medicine, University of Connecticut Health Center, Farmington, CT, USA
Abstract: This review discusses the research evidence for psychological treatment of gambling disorder. Several treatment options for gamblers have been explored, ranging from self-help and peer support, to brief and motivational interventions, to more intensive therapy approaches. Involvement in peer support programs seems to be optimal when combined with professional treatment; however, engagement and retention in peer support is limited. Self-directed interventions appear to benefit some gamblers; however, the involvement of therapist support, either in person or by telephone, may bolster these effects and such support need not be extensive. These self-directed options reduce the barriers associated with treatment-seeking, and may reach a wider range of gamblers than professionally delivered treatments alone. Brief and motivational approaches similarly may extend treatment options to more gamblers, namely at-risk and problem gamblers and those not seeking treatment. Of more extensive therapies, no consistent benefit of one approach emerges, although cognitive–behavioral interventions have been most often applied. Overall, several treatments have been developed for gambling disorder and results are promising, but variability in findings suggests a need for further systematic evaluation.
Keywords: gambling treatment, cognitive behavioral treatment, brief interventions, pathological gambling, problem gambling, behavioral addictions
Background
Disordered gambling is a maladaptive pattern of wagering that persists despite negative consequences in major areas of functioning such as finances, relationships, and psychological health. In the Diagnostic and Statistical Manual (DSM) of Mental Disorders, Fifth Edition (DSM-5),1 gambling disorder was relocated from the impulse control disorder chapter to the newly-expanded chapter for substance-related and addictive disorders. In addition, its name was changed from pathological gambling to gambling disorder. In the present article, the term “pathological gambling” will be used as described in the prior edition (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition [DSM-IV]).
DSM-5 criteria for gambling disorder remain largely intact from the prior edition and include: 1) needing to wager larger amounts; 2) experiencing restlessness or irritability when restricting gambling; 3) repeated inability to control or stop gambling; 4) preoccupation with gambling; 5) gambling in response to negative affect; 6) gambling to recoup losses; 7) lying about gambling; 8) jeopardizing relationships, work, or educational opportunities due to gambling; and 9) relying on financial bailouts from others to relieve financial pressures related to gambling. Diagnosis of gambling disorder is met when four or more of these criteria are present in a 12-month period. Subthreshold gamblers, who meet fewer criteria, are often referred to as problem gamblers; they can experience some negative consequences related to their gambling and may be at risk for escalation of their gambling problems. Intervention in this group may prevent escalation of gambling to the more severe form of the disorder.2
Prevalence
Population estimates of lifetime gambling disorder range from 0.4%–2.0% of the general population, with problem gamblers contributing an additional 1.3%–2.3%.3–6 About a third of pathological gamblers will recover naturally,7 and for the remainder several effective treatment options are available. This article will discuss the various psychological treatment options for gambling disorder and problem gambling, ranging from lower intensity interventions (self-help, brief treatments) to those involving greater therapist contact.
Self-directed interventions
Self-help interventions may facilitate recovery by reducing the barriers (eg, cost, stigma, transportation, child care) associated with seeking professional treatment. Gamblers Anonymous (GA) support meetings are the most accessible of the treatments available for gambling,8 but more recently-developed interventions such as bibliotherapy and self-directed computer interventions may also be effective options for those seeking nonprofessional treatments.
Gamblers anonymous
GA, similar to the Alcoholics Anonymous 12-step programs upon which it is modeled, strongly advocates complete abstinence from gambling. Like its sister programs, GA has adopted the disease model and views disordered gambling as a lifelong affliction that can be controlled via gambling abstinence, but not cured.8 For this reason, any beliefs gamblers may hold about their ability to control their gambling now or in the future are actively discouraged. Social support from peers and family members is an integral part of the organization. Senior members provide support for gambling recovery (eg, dealing with cravings, slips, acknowledging progress) and the negative consequences of gambling. For example, members experienced in managing their own debts may provide aid in setting up debt repayment plans and negotiating with creditors.8 Family members can attend sister meetings (GamAnon) or in some cases attend open meetings with the affected member.
Relatively few studies have been conducted on GA as part of recovery, particularly among those who use GA as their primary treatment mode. An early report9 of 232 GA attendees noted that early dropout in GA is common, with 48% failing to return within their first three meetings and only 8% achieving at least 1 year of abstinence. Individuals with more severe gambling problems and/or interest in abstinence may be more likely to persist in GA.10 Even among individuals who stay involved with GA, differences are present among those who are successful abstainers and those experiencing relapse (any gambling) in the past 12 months. In a sample of 75 individuals with at least 12 months of GA involvement, Oei and Gordon11 found that the abstainers had significantly higher mean attendance and participation, social support, and 12-step-related beliefs compared to relapsers. These results might suggest that increased GA involvement leads to abstinence; however, alternative explanations might be that abstinence leads to greater GA involvement or that a third variable (eg, motivation) spurs both abstinence and greater treatment involvement.
GA attendance may enhance outcomes of those in formal treatment programs. Petry12 compared gambling abstinence rates 2 months after initiating professional gambling treatment in a sample of 342 pathological gamblers with and without a history of attending GA. Of GA-experienced individuals, 48% achieved abstinence post-treatment compared to 36% of those without a history of GA attendance. Individuals with prior GA experience were also more likely to attend GA meetings after initiating professional treatment (P<0.001) and to attend more sessions of the professional treatment program (P<0.05). Although these results are encouraging, about half the sample did not attend GA when recommended to do so as a complement to their professional treatment. About two-thirds of the individuals with no GA history did not follow the advice to attend GA during professional treatment, and 34% of the individuals who had attended GA in their past declined to re-engage. In a randomized design, Petry et al13 found some reductions in gambling compared to baseline when patients were assigned to GA as a stand-alone treatment, but individuals in professionally delivered treatment conditions evidenced greater gains compared to the GA-only condition.
Two studies14,15 compared 12-step facilitation (TSF) treatment to another form of treatment, cognitive–behavioral therapy (CBT). Although based on the principles of GA, TSF sessions were professionally led and structured, and therapy was time-limited (8 weeks of one to two sessions per week). Toneatto and Dragonetti15 found no differences in outcomes of participants randomized to CBT or TSF at a 12-month follow-up. In Marceaux and Melville’s study,14 both types of treatment demonstrated improvement in the number of DSM symptoms endorsed relative to a wait-list control (P<0.001) at the post-treatment assessment, with no differences present between the active treatments.
Table 1 presents a summary of gambling studies and their characteristics.
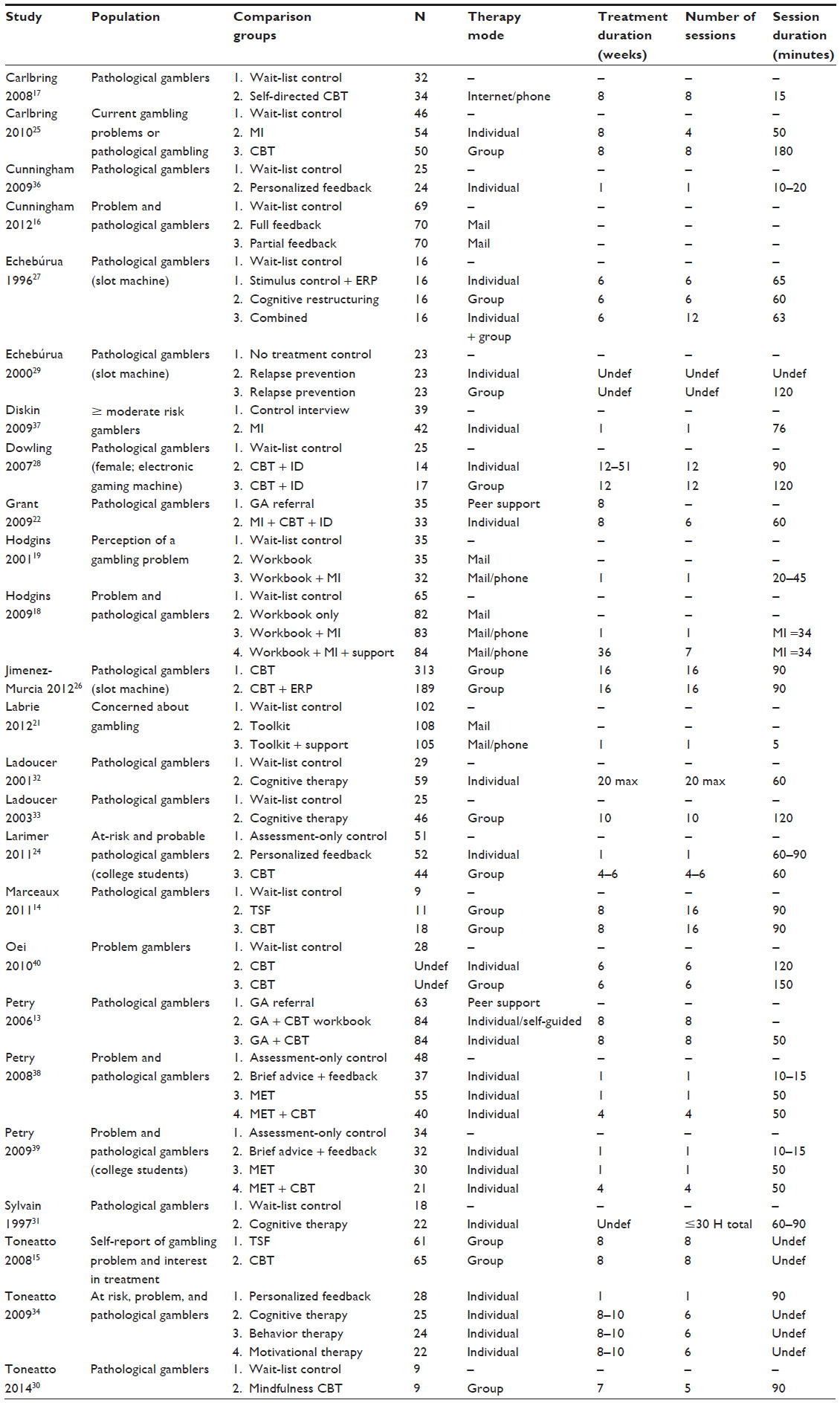 | Table 1 Summary of study characteristics |
Other self-directed options
Some individuals may prefer individual, self-directed options such as bibliotherapy (eg, workbooks), internet-based interventions relative to GA, or in-person therapy. The workbook materials have been evaluated as stand-alone interventions and in combination with telephone or in-person support.
Cunningham et al16 varied self-help material content, investigating whether providing normative information (eg, average amounts gambled) as part of personalized feedback improves treatment outcomes. Two hundred and nine problem and pathological gamblers were randomized to 1) mailed personalized feedback with normative content; 2) mailed partial feedback without normative content; or 3) a wait-list control. No differences between conditions were present for overall dollars wagered or highest dollar amount wagered in one session, but participants in the partial feedback condition reduced their gambling frequency relative to participants in the other two conditions (P<0.05). These results are somewhat unexpected, as the normative component was thought to spur reflection and change in problem gamblers through re-evaluation of their own perceptions of gambling. Such perceptions, however, may be based on biased information, for example, “All the gamblers I know gamble as much as I do.” In any case, providing this normative information was not useful in the study.
Several studies blended self-directed interventions with telephone support. Carlbring and Smit17 examined the efficacy of a self-help Internet intervention plus 8 weeks of brief telephone support (about 4 hours total) relative to a wait-list control condition in a sample of 66 pathological gamblers. Participants randomized to the Internet intervention reported significant improvements (P<0.001) in gambling symptoms compared to the wait-list control at a post-treatment assessment. The reductions in gambling symptoms relative to baseline were sustained in follow-ups at 6, 18, and 36 months, but long-term group comparisons were not possible given the use of a wait-list control.
Studies by Hodgins and colleagues18–20 directly examined the added value of minimal therapist telephone contact to a workbook intervention, with results suggesting an advantage of this limited contact. In the initial study, Hodgins et al19 compared gambling outcomes in 102 gamblers who perceived their gambling as problematic randomized to a wait-list control, a workbook alone condition, or the same workbook with a brief, one-session motivational telephone interview (20–45 minutes). Participants in the latter condition showed improvements, with 32% abstinent at the 1-month follow-up, but gambling abstinence in the workbook-only condition (21%) was similar to the wait-list control (18%). The workbook plus motivational session condition continued to show an advantage in outcomes compared to the workbook-only condition through the 3-month and 6-month follow-ups, but between-group differences were not significant at the 12-month follow-up. Group differences again emerged at a 24-month follow-up, with the motivational group achieving significantly (P<0.05) lower gambling frequency, expenditures, and gambling severity relative to the workbook-only condition.20
Hodgins et al18 built on this prior design with the addition of a fourth condition involving enhanced telephone support (six booster sessions over 9 months) added to the telephone motivational interview, plus a mailed self-help workbook. Both motivational conditions (workbook plus single motivational telephone session, or same plus six booster calls) reduced gambling, compared to the workbook alone, or wait-list conditions with no added benefit from the enhanced telephone support in the short-term or throughout the 9-month follow-up. However, the workbook-only condition also showed benefits in terms of reduction of gambling losses, and of reduction of the likelihood of meeting the criteria for pathological gambling, in this study.
The Hodgins et al study18 examined whether increased telephone support enhanced outcomes, and found that it did not. Another study21 tested a minimalist telephone intervention in a sample of 315 individuals concerned about their gambling. Subjects were randomized to a wait-list control, a workbook toolkit, or the toolkit plus a 5-minute scripted telephone introduction to the toolkit. Researchers found little benefit in telephone support added to a self-help workbook when telephone contact was limited to about 5 minutes. However, the toolkit conditions evidenced greater proportions of participants achieving abstinence at the 3-month follow-up (61%) relative to paticipants in the wait-list control condition (41%). Results from this study suggest that a contact threshold may exist under which therapist contact provides no added advantage, but given the results of the Hodgins and colleague studies,18–20 the contact time need not be substantial (ie, a single session of 20–45 minutes may improve outcomes). However, these telephone supports18,19,21 differed not only in their length, but also in their nature, and it is possible that the motivational interviewing content used in the Hodgins et al studies18,19 may be integral to improving outcomes using brief support. Further studies will be needed to confirm or deny the importance of duration and content of telephone support in conjunction with workbook materials in the treatment of gambling disorder.
In one of the few studies comparing efficacy of workbook materials to more extensive individual therapy, Petry et al13 compared gambling outcomes among 231 pathological gamblers randomized to a GA referral alone, GA referral plus a CBT-based self-guided workbook, and GA referral plus eight weekly individual CBT sessions. Results suggested that the individual CBT condition achieved significant improvements in gambling indices relative to those in the GA referral alone condition, with those in the workbook condition achieving marginal improvements over the GA referral condition. For example, the percentage of individuals no longer classified as pathological gamblers at the post-treatment assessment was 69% in the individual CBT condition, 51% in the workbook condition, and 47% in the GA referral-only condition (P<0.02). GA attendance was similar and low (two meetings over 2 months on average) across groups, but treatment engagement was higher in the professionally delivered therapy condition. Nearly 30% of those in the workbook condition failed to complete any chapters, whereas 93% of those assigned to the individual therapy condition attended at least one treatment session. Therapist contact appears to enhance engagement and outcomes, compared to conditions without such involvement in treatment-seeking pathological gamblers.
Overall, peer support or self-directed workbooks may be viable options for gambling recovery and preferred by some individuals. GA attendance alone and particularly in combination with professional treatment may provide benefits, but a significant portion of individuals with gambling disorder refuse GA even when encouraged by a professional, suggesting that GA is not a desirable avenue of change for many treatment seekers. Bibliotherapy and self-directed Internet interventions may reduce gambling for some individuals, but it appears that supplementing these materials with some therapist contact, either by phone or in person, improved outcomes in most studies. Professionally delivered treatment, in particular, may be important for individuals with more severe gambling problems who are actively seeking treatment.
Professionally delivered treatments
Cognitive–behavioral therapy
CBT interventions target maladaptive cognitions and related behaviors, with emphasis on understanding the interrelatedness of cognitions, emotions, and behavior. Content differs across studies in the extent of cognitive versus behavioral emphasis, but all include both elements to some degree. Petry’s eight-session format8,13 includes topics such as identifying and managing triggers, conducting functional analysis of gambling episodes, increasing alternate activities, dealing with urges and cravings, building interpersonal conflict skills, recognizing and correcting cognitive biases, and preventing relapse. Its efficacy was examined in a sample of 231 pathological gamblers randomized to one of three conditions:13 a) GA referral alone; b) GA referral plus a self-directed CBT workbook; or c) GA referral plus individual CBT sessions. As noted above, participants in the individual CBT format evidenced the most gains by the end of treatment with maintenance of some effects through the 1-year follow-up period.
Benefits of this approach were also seen in a study by Grant et al,22 who randomized 68 pathological gamblers to six sessions of group therapy or a GA referral-only control condition. The group therapy combined CBT with motivational interviewing and imaginal desensitization. Gambling severity decreased significantly and a higher percentage of participants (64%) were abstinent in the therapy condition relative to the control (17%) at the post-treatment assessment (P<0.001). Of the 35 treatment responders (out of 44 individuals receiving treatment; defined as a 35% reduction in gambling severity scores), 28 achieved abstinence in the treatment period and 27 reported abstinence at the 6-month follow-up.23 Some rebounding from the post-treatment assessments was present, but all gambling severity measures maintained significant gains from baseline levels through 6 months in within-subject comparisons.
Larimer et al24 evaluated a brief (four to six session) version of Petry’s CBT,8 delivered in group format to a sample of 147 at-risk or probable pathological gambling college students. Participants in the group CBT were compared to those randomized to a single session individual personalized feedback condition or an assessment-only control. In this sample, both active interventions reduced gambling consequences and DSM-IV criteria relative to the control condition (P<0.05), with larger effect sizes found in the personalized feedback condition. The feedback session also reduced gambling frequency (P<0.02). While this study found both interventions promising with no added benefit of more extended therapy contact, the sample included younger and less severe gamblers, and attrition was high from the group treatment with less than half of those randomized to the group therapy condition receiving at least 50% of scheduled sessions. These gamblers, in their need and desire for more intensive and group formatted treatments, may differ substantially from adult treatment-seeking and more severe gamblers who likely have experienced more negative consequences related to their gambling.
Two studies25,26 examined the potential benefits of adding behavioral exposure components to a traditional CBT framework. In the Carlbring et al study,25 the eight-session group CBT content focused on cognitive restructuring, skill building, identification of high-risk situations, and coping strategies. Imaginal exposure to gambling urges with response prevention was an additional and unique component of the therapy. This CBT was provided in a group format and was compared to a four-session individual motivational interviewing therapy condition and a wait-list control in a sample of 150 problem and pathological gamblers. At the end of treatment, participants in both active treatments demonstrated improvements (P<0.04) in the primary outcome using DSM-IV symptom criteria, compared to the control condition, and there were no differences between the active treatments. Neither active treatment improved secondary gambling indices (eg, frequency, dollars wagered, or heavy gambling) relative to the control.
Another study26 added an exposure and response prevention component to a 16-week group CBT. Participants were 502 male pathological gamblers receiving CBT or CBT plus exposure, but this study did not use random assignment procedures. Results suggested no differences between the two conditions in gambling outcomes, including relapse, but the exposure group exhibited poorer attendance and greater dropout rates. The authors conclude that exposure was not beneficial; however, it is important to view these results in the context of the study limitations, namely no randomization or control condition.
The design of a study by Echeburua et al27 allowed for direct comparison of behavioral, cognitive, and combined approaches. Treatment-seeking pathological gamblers (N=64) were randomized to 6 weeks of a) wait-list control; b) individual stimulus control and exposure with response prevention; c) group cognitive restructuring; or d) combined treatment (double therapy contact time). More participants in the three active treatments (59%) were deemed treatment successes at the 6-month follow-up relative to the control condition (25%, P<0.05), defined as two or fewer gambling episodes in the months following treatment with expenditures not exceeding the patient’s baseline weekly total gambling expenditures. The individual behavioral condition produced the highest rates of success. At the 6-month and 12-month follow-ups, 75% and 69% of participants, respectively, in the individual behavioral condition met this criterion compared to 63% and 38% of participants in the group cognitive condition, and 38% and 38% of the combined treatment condition. In this study, the behavioral treatment was superior in the long term, but both therapy format (group versus individual) and contact time varied across conditions, making conclusions about effective therapy ingredients difficult to draw.
Two studies28,29 directly compared individual versus group-delivered CBT. Dowling et al28 randomly assigned 56 female pathological gamblers to 12 sessions of group (2 hours each) or individual (1.5 hours each) CBT that included imaginal desensitization or a wait-list control. Both treatments evidenced improvement in gambling behavior outcomes (eg, frequency, duration, financial expenditure) compared to the control, with no significant differences between the active treatments (P<0.05). In terms of clinical significance, 79% and 65% of those randomized to individual therapy and group therapy, respectively, no longer met diagnostic criteria for pathological gambling at the 6-month follow-up. While these results appear to favor the individual therapy condition, the study design allowed rescheduling of individual sessions but not group sessions, leading to differences in treatment duration (12–51 weeks for those in the individual therapy versus 12 weeks in the group condition), and differences in treatment exposure (those in individual therapy received 12 sessions, while group therapy recipients attended an average of ten sessions) between the treatment conditions. Thus, the results may be a function of duration or exposure variables, rather than the therapy format.
Another study29 employed a relapse prevention protocol. Treatment-seeking pathological gamblers (N=69) completed behavioral treatment using stimulus control plus in vivo exposure with response prevention. After finishing the initial treatment, participants were randomly assigned to individual or group relapse prevention or a no further treatment control. The active treatments were equally effective, with 83% of those in individual CBT and 78% of those in the group CBT achieving the criterion of two or fewer gambling episodes in the 12 months following treatment with total dollars gambled not exceeding their baseline weekly total. These rates significantly exceeded the 56% achieving this criterion in the control group (P<0.05), suggesting that any continued relapse prevention therapy is useful but the format of therapy (group versus individual) is not important.
Mindfulness approaches are also being explored for the treatment of gambling disorder. In a small pilot study, Toneatto et al30 compared 18 pathological gamblers assigned to a wait-list control or group-based mindfulness-enhanced CBT. Relative to the control, the experimental group reported significantly fewer DSM-IV gambling symptoms at the post-treatment evaluation (P<0.05).
Cognitive therapy
Given the faulty cognitions that characterize gambling disorder, some interventions have focused directly on attempting to alter these cognitions. Sylvain et al31 randomly assigned 40 male pathological gamblers to either a wait-list control condition or cognitive therapy. The content of the cognitive therapy included corrections of misconceptions related to gambling, problem-solving training, social skills training, and relapse prevention. The therapy sessions ranged 60–90 minutes, with a maximum of 30 total contact hours (16.7 hours on average). End-of-treatment ratings showed significant effects between the treatment and control groups on all five primary outcomes (eg, diagnostic criteria, desire to gamble) and two of three indices of gambling frequency. However, these estimates may be biased because eleven participants (eight assigned to treatment and three to control) dropped out of the study, and these individuals were excluded from analyses.
Ladouceur et al32 tested a cognitive therapy based on an approach by Sylvain et al31 that focused on the cognitive correction and relapse prevention components, with emphasis on the cognitive aspects of relapses and high risk situations (eg, thoughts about feeling lucky). Pathological gamblers (N=88) were randomized to receive up to 20 weekly individual sessions of cognitive treatment or a wait-list control. Fifty-nine participants were assigned to the cognitive therapy condition at randomization, but only data from a limited subset of 35 responders were used for analyses. At the end of treatment, participants in the treatment condition endorsed fewer gambling diagnostic criteria, gambled on fewer occasions, spent less time gambling, and spent less money on gambling compared to those in the wait-list control (P<0.05). A follow-up study33 of 58 pathological gamblers found significant reductions in DSM-IV symptoms at the end of treatment when the therapy was delivered in a group format. Compared to pre-treatment gambling, benefits were sustained long-term (up to 12 months in Ladoucer et al32 and up to 24 months in Ladoucer et al33), but because these studies employed a wait-list control, long-term effects were not compared to a non-treated comparison group. While the above results are promising, these studies31–33 failed to use intent to treat analyses. The exclusion of treatment dropouts from analyses may lead to artificially inflated views of the success of treatment programs.
Toneatto and Gunaratne34 directly compared cognitive therapy to other active treatments. Problem gamblers (N=99) were randomized to a) six sessions of cognitive therapy; b) six sessions of behavioral therapy; c) six sessions of motivational interviewing therapy; or d) a single 90-minute motivational session with feedback and a handout. All groups demonstrated improvement in gambling frequency and severity at post-treatment and the 1-year follow-up, with no between-condition effects reaching significance. Together, these data suggest that cognitive therapy may hold promise in the treatment of gambling behavior, but does not appear to be any more efficacious than other interventions, some of which have been studied and found efficacious in more tightly designed and analyzed studies.
Brief and motivational interventions
Despite the potential advantages of treatment, rates of treatment seeking are quite low, at about 6%–12% among pathological gamblers.7,35 Some individuals may not know about the availability of treatment, and some may explore treatment options but lose motivation to persist in treatment, as evidenced by the high dropout rates for both GA (eg, 48% drop out within first 3 meetings)9 and professional treatments (eg, 26%–47%).32,33 Like those seeking treatment for substance disorders, many individuals with gambling problems are conflicted in their desire to change. They may be pushed into treatment by well-meaning family or friends, believe they can gain control over their problematic gambling on their own, or be unaware of the extent of negative impact that gambling has on their lives. Motivational approaches attempt to address client ambivalence towards change, for example by weighing the advantages and disadvantages of changing their gambling behavior. Some motivational therapies provide personalized and/or normative feedback which, as cited earlier,16 may or may not be helpful in reframing mistaken client perceptions about their gambling.
Motivational approaches have also been explored as an avenue to engage problem or at-risk gamblers who have not yet met diagnostic criteria for gambling disorder, in an attempt to prevent escalation of gambling behavior and related negative consequences.
Several studies explored single session interventions for problem and pathological gamblers. As noted previously, single session motivational telephone support19,20 is effective for improving gambling outcomes, but increased contact time does not necessarily improve results beyond those obtained from the single session intervention.18 Cunningham et al36 found that a single session (15–25 minutes) intervention of personalized feedback can reduce total money gambled (P<0.02) for pathological gamblers compared to a wait-list control at a 3-month follow-up, but not gambling severity and single occasion maximum total wagered. Compared to an assessment control condition, Diskin and Hodgins37 found a single session of motivational interviewing to be effective in reducing gambling frequency and total dollars wagered in problem gamblers at a 12-month follow-up (P<0.05). These studies suggest that single session interventions may be a low cost and effective avenue for short-term and longer-term effects in at least a subset of problem gamblers.
Motivational approaches can also be blended with other treatment components. As outlined earlier, Grant et al22 compared results from 68 pathological gamblers randomized to six sessions of group therapy that included motivational interviewing and CBT, or a GA referral-only control condition. The combined motivational interviewing plus CBT group therapy approach improved outcomes relative to the control condition.
Other studies38,39 compared brief interventions that isolated potential effects of motivational interviewing. Similar to Hodgins et al,18 results from these studies suggest that more extensive, multi-session interventions may not be necessary to confer benefits to gamblers. Petry et al38 evaluated a motivational-based approach in 180 non-treatment-seeking problem and pathological gamblers randomized to one of four conditions: a) an assessment-only control; b) brief advice (single session of 10 minutes) including personalized normative feedback; c) a single 50-minute session of motivational enhancement therapy (MET); or d) an initial MET session followed by three sessions of CBT. Only the brief advice condition evidenced significantly reduced gambling severity and dollars wagered at the post-treatment assessment relative to the control (P<0.05). The MET plus CBT condition evidenced delayed improvements in gambling severity reduction (P<0.05), but not dollars wagered, in the follow-up phase relative to the control. At the 6-week and 9-month follow-ups, respectively, 47% and 48% of the control group, 66% and 71% of the brief advice condition, 54% and 58% of the MET condition, and 50% and 59% of the MET plus CBT condition were classified as recovered or improved, based on severity scores and dollars wagered.
Another study by Petry et al39 found a different pattern of effects when evaluating the same four conditions in 117 college student problem and pathological gamblers. In this sample, the combined treatment interventions evidenced improvements in gambling severity, gambling frequency, and total wagered relative to the control across the 9-month study period (P<0.05), with no differences observed between the active treatments. In terms of clinically significant improvement, participants in the MET condition had a threefold increase in the odds of being classified as substantially improved (defined as gambling <10.5% of their income) compared to the control condition at the 9-month study follow-up. The brief advice and MET plus CBT conditions did not differ significantly from the control group in this classification at the long-term follow-up. In contrast to the earlier Petry et al study38 in which the brief advice condition was superior, the subsequent Petry et al study39 found that all three of the active treatments were effective, with the most consistent benefits evident for the MET alone group. These populations differed, with the earlier Petry et al38 study cohort having more severe gambling problems, and recruitment focusing on substance abuse clinic and low-income community medical clinic patients versus college students.
Other studies likewise found no differences between types of interventions. Toneatto and Gunaratne34 found no significant differences in outcomes from 99 problem gamblers randomized to six sessions of cognitive, behavioral, or motivational therapy, or a single session (90 minutes) of brief advice with feedback condition. Carlbring et al25 compared therapeutic results of a group receiving eight sessions of CBT, a group receiving four sessions of motivational interviewing, and a wait-list control group, finding that both active groups improved significantly compared to the control, with no differences between CBT and motivational therapies. Similarly, Oei et al40 evaluated an individual (six 2-hour sessions over 6 weeks) or group (2.5 hours once-weekly for 6 weeks) motivational plus CBT approach in 102 problem gamblers compared to wait-list control. The two active treatments evidenced significant gains compared to the control, but the active treatments did not differ significantly from one another.
Conclusion
This review of gambling treatment studies indicates a benefit of some forms of active treatment compared to no treatment or wait-list control conditions. An array of options have been explored, including workbook and peer support, brief and motivational, cognitive and/or behavioral, and blended treatments.
Peer support received in GA confers some benefits to participants, especially when combined with professional treatment. However, even when recommend by a professional, overall engagement in GA is low. Other self-directed options, such as workbooks and Internet intervention, represent alternate methods of accessing treatment, with fewer barriers compared to professional treatments. These interventions show some promise, especially when blended with at least minimal professional support, but more extended professional contact does not seem to improve outcomes.
Professionally delivered treatments appear to significantly improve outcomes relative to wait-list controls, peer support, and self-directed interventions in more severe treatment-seeking gamblers. The advantages of professionally delivered treatments may lie in greater engagement with treatment materials. Interestingly, in comparisons among active treatments (eg, cognitive, behavioral, cognitive–behavioral, or blended therapy), no consistent advantages emerge for any particular approach. Likewise, group and individually delivered therapies appear similarly effective. These results parallel those of psychotherapeutic approaches used in treatment of other disorders; many treatments confer benefits, and it is much more difficult to show differences between active treatments than between any two particular forms of therapy.41,42 Furthermore, such comparisons require much larger samples, given the smaller differences in effect sizes when comparing two active treatments.41
Increasing access to and engagement in treatments will be important issues to address as the field progresses. Brief and motivational interventions may offer opportunities for engaging gamblers earlier, before their gambling escalates and possibly preventing some of the harm associated with this disorder. Several options have been explored, including brief advice, personalized feedback, and motivational-based approaches. Interestingly, results across several studies suggest that more may not necessarily be better in terms of patient response, but again, there is no clear evidence of any particular form of brief treatment being more efficacious than others.
Prior reviews and meta-analyses43–47 note the heterogeneity in methodological rigor of gambling treatment research, which fortunately does appear to be improving. Nonetheless, many of the existing studies failed to employ intent-to-treat analyses, and this failure to account for treatment refusal and treatment dropout likely yields overestimation of gambling treatment effects.48 In addition, relatively few studies utilized control conditions beyond wait-lists, which obviate the ability to assess long-term efficacy. Overall, several approaches show promise in the treatment of problem and disordered gambling, including brief, motivational, and cognitive–behavioral interventions. Regardless of the form of therapy applied, gambling problems do seem to dissipate over time among those who seek, or who are provided, treatment. As the field moves forward, it will be important to design well-controlled studies with sufficient sample sizes, and carefully and closely monitor changes in gambling among all randomized participants. Rather than attempting to develop “new” treatments, a more systematic evaluation of existing therapies is likely to guide implementation of effective interventions in clinical care. This systematic evaluation might take advantage of developments in statistical analysis that better accommodate missing data, time-varying covariates, and dynamic processes.49 The availability of structured effective treatments may be especially important, as more therapists are likely to begin assessing for gambling problems and treating them now that gambling is aligned with substance use disorders in the DSM-5.
Acknowledgment
Preparation of this report was supported in part by NIH grant R01DA021567.
Disclosure
The authors report no conflicts of interest in this work.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington: American Psychiatric Publishing; 2013. | |
Toce-Gerstein M, Gerstein DR, Volberg RA. A hierarchy of gambling disorders in the community. Addiction. 2003;98(12):1661–1672. | |
Gerstein D, Hoffmann J, Larison C, et al. Gambling Impact and Behavior Study: Report to the National Gambling Impact Study Commission. Chicago: National Opinion Research Center at the University of Chicago; 1999. | |
Kessler RC, Hwang I, LaBrie R, et al. DSM-IV pathological gambling in the National Comorbidity Survey Replication. Psychol Med. 2008;38(9):1351–1360. | |
Petry NM, Stinson FS, Grant BF. Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2005;66(5):564–574. | |
Welte J, Barnes G, Wieczorek W, Tidwell MC, Parker J. Alcohol and gambling pathology among US adults: prevalence, demographic patterns and comorbidity. J Stud Alcohol. 2001;62(5):706–712. | |
Slutske WS. Natural recovery and treatment-seeking in pathological gambling: results of two US national surveys. Am J Psychiatry. 2006;163(2):297–302. | |
Petry NM. Pathological Gambling: Etiology, Ccomorbidity, and Treatment. Washington: American Psychological Association; 2005. | |
Stewart RM, Brown RI. An outcome study of Gamblers Anonymous. Br J Psychiatry. 1988;152(2):284–288. | |
Brown RIF. Dropouts and continuers in Gamblers Anonymous: Part four. Evaluation and Summary. J Gambl Behav. 1987;3(3):202–210. | |
Oei TP, Gordon LM. Psychosocial factors related to gambling abstinence and relapse in members of gamblers anonymous. J Gambl Stud. 2008;24(1):91–105. | |
Petry NM. Patterns and correlates of Gamblers Anonymous attendance in pathological gamblers seeking professional treatment. Addict Behav. 2003;28(6):1049–1062. | |
Petry NM, Ammerman Y, Bohl J, et al. Cognitive–behavioral therapy for pathological gamblers. J Consult Clin Psychol. 2006;74(3):555–567. | |
Marceaux JC, Melville CL. Twelve-step facilitated versus mapping-enhanced cognitive–behavioral therapy for pathological gambling: A controlled study. J Gambl Stud. 2011;27(1):171–190. | |
Toneatto T, Dragonetti R. Effectiveness of community-based treatment for problem gambling: A quasi-experimental evaluation of cognitive–behavioral vs twelve-step therapy. Am J Addict. 2008;17(4):298–303. | |
Cunningham JA, Hodgins DC, Toneatto T, Murphy M. A randomized controlled trial of a personalized feedback intervention for problem gamblers. PLoS ONE. 2012;7(2):e31586. | |
Carlbring P, Smit F. Randomized trial of internet-delivered self-help with telephone support for pathological gamblers. J Consult Clin Psychol. 2008;76(6):1090–1094. | |
Hodgins DC, Currie SR, Currie G, Fick GH. Randomized trial of brief motivational treatments for pathological gamblers: More is not necessarily better. J Consult Clin Psychol. 2009;77(5):950–960. | |
Hodgins DC, Currie SR, el-Guebaly N. Motivational enhancement and self-help treatments for problem gambling. J Consult Clin Psychol. 2001;69(1):50–57. | |
Hodgins DC, Currie S, el-Guebaly N, Peden N. Brief motivational treatment for problem gambling: a 24-month follow-up. Psychol Addict Behav. 2004;18(3):293–296. | |
LaBrie RA, Peller AJ, LaPlante DA, et al. A brief self-help toolkit intervention for gambling problems: A randomized multisite trial. Am J Orthopsychiatry. 2012;82(2):278–289. | |
Grant JE, Donahue CB, Odlaug BL, Kim SW, Miller MJ, Petry NM. Imaginal desensitization plus motivational interviewing for pathological gambling: randomised controlled trial. Br J Psychiatry. 2009;195(3):266–267. | |
Grant JE, Donahue CB, Odlaug BL, Kim SW. A 6-month follow-up of imaginal desensitization plus motivational interviewing in the treatment of pathological gambling. Ann Clin Psychiatry. 2011;23(1):3–10. | |
Larimer ME, Neighbors C, Lostutter TW, et al. Brief motivational feedback and cognitive behavioral interventions for prevention of disordered gambling: a randomized clinical trial. Addiction. 2011;107(6):1148–1158. | |
Carlbring P, Jonsson J, Josephson H, Forsberg L. Motivational interviewing versus cognitive behavioral group therapy in the treatment of problem and pathological gambling: A randomized controlled trial. Cogn Behav Ther. 2010;39(2):92–103. | |
Jimenez-Murcia S, Aymami N, Gomez-Peña M, et al. Does exposure and response prevention improve the results of group cognitive–behavioural therapy for male slot machine pathological gamblers? Br J Clin Psychol. 2012;51(1):54–71. | |
Echebúrua E, Báez C, Fernández-Montalvo J. Comparative effectiveness of three therapeutic modalities in the psychological treatment of pathological gambling: Long-term outcome. Behav Cogn Psychother. 1996;24(1):51–72. | |
Dowling N, Smith D, Thomas T. A comparison of individual and group cognitive–behavioural treatment for female pathological gambling. Behav Res Ther. 2007;45(9):2192–2202. | |
Echeburúa E, Fernández-Montalvo J, Báez C. Relapse prevention in the treatment of slot-machine pathological gambling: Long-term outcome. Behav Ther. 2000;31(2):351–364. | |
Toneatto T, Pillai S, Courtice EL. Mindfulness-enhanced cognitive behavioral therapy for problem gambling: A controlled pilot study. Int J Ment Health Addiction. 2014;12:197–205. | |
Sylvain C, Ladoucer R, Boisvert JM. Cognitive and behavioral treatment of pathological gambling: a controlled study. J Consult Clin Psychol. 1997;65(5):727–732. | |
Ladouceur R, Sylvain C, Boutin C, et al. Cognitive treatment of pathological gambling. J Nerv Ment Dis. 2001;189(11):774–780. | |
Ladouceur R, Sylvain C, Boutin C, Lachance S, Douet C, Leblond J. Group therapy for pathological gamblers: a cognitive approach. Behav Res Ther. 2003;41(5):587–596. | |
Toneatto T, Gunaratne M. Does the treatment of cognitive distortions improve clinical outcomes for problem gambling? J Contemp Psychother. 2009;39:221–229. | |
Suurvali H, Hodgins D, Toneatto T, Cunningham J. Treatment seeking among Ontario problem gamblers: results of a population survey. Psychiatr Serv. 2008;59(11):1343–1346. | |
Cunningham JA, Hodgins DC, Toneatto T, Rai A, Cordingley J. Pilot study of a personalized feedback intervention for problem gamblers. Behav Ther. 2009;40(3):219–224. | |
Diskin KM, Hodgins DC. A randomized controlled trial of a single session motivational intervention for concerned gamblers. Behav Res Ther. 2009;47(5):382–388. | |
Petry NM, Weinstock J, Ledgerwood DM, Morasco B. A randomized trial of brief interventions for problem and pathological gamblers. J Consult Clin Pscyhol. 2008;76(2):318–328. | |
Petry NM, Weinstock J, Morasco BJ, Ledgerwood DM. Brief motivational interventions for college student problem gamblers. Addiction. 2009;104(9):1569–1578. | |
Oei TP, Raylu N, Casey LM. Effectiveness of group and individual formats of a combined motivational interviewing and cognitive behavioral treatment program for problem gambling: a randomized controlled trial. Behav Cogn Psychother. 2010;38(2):233–238. | |
Kazdin AE, Bass D. Power to detect differences between alternative treatments in comparative psychotherapy outcome research. J Consult Clin Psychol. 1989;57(1):138–147. | |
Wampold B. Methodological problems in identifying efficacious psychotherapies. Psychother Res. 1997;7(1):21–43. | |
Cowlishaw S, Merkouris S, Dowling N, Anderson C, Jackson A, Thomas S. Psychological therapies for pathological and problem gambling [review]. Cochrane Database Syst Rev. 2012;11:CD008937. | |
Gooding P, Tarrier N. A systematic review and meta-analysis of cognitive-behavioural interventions to reduce problem gambling: hedging our bets? Behav Res Ther. 2009;47(7):592–607. | |
Pallesen S, Mitsem M, Kvale G, Johnsen BH, Molde H. Outcome of psychological treatment of pathological gambling: a review and meta-analysis. Addiction. 2005;100(10):1412–1422. | |
Petry N. Disordered gambling and its treatment. Cogn Behav Pract. 2009;16(4):457–467. | |
Problem Gambling Research and Treatment Centre, Monash University. Guideline for screening, assessment and treatment in problem gambling. Clayton: Monash University; 2011. Available from: http://www.med.monash.edu.au/assets/docs/sphc/pgrtc/guideline/problem-gambling-guidelines-web.pdf. Accessed July 24, 2014. | |
Westphal JR. Are the effects of gambling treatment overestimated? Int J Ment Health Addiction. 2007;5(1):65–79. | |
Stout RL. Advancing the analysis of treatment process. Addiction. 2007;102(10):1539–1545. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.