")
Back to Journals » Clinical Ophthalmology » Volume 9
Prolonged increase in tear meniscus height by 3% diquafosol ophthalmic solution in eyes with contact lenses
Authors Nagahara Y, Koh S , Nishida K, Watanabe H
Received 6 April 2015
Accepted for publication 13 May 2015
Published 9 June 2015 Volume 2015:9 Pages 1029—1031
DOI https://doi.org/10.2147/OPTH.S86173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yukiko Nagahara,1 Shizuka Koh,1 Kohji Nishida,1 Hitoshi Watanabe1,2
1Department of Ophthalmology, Osaka University Graduate School of Medicine, Suita, Osaka, 2Kansai Rosai Hospital, Amagasaki, Hyogo, Japan
Purpose: This study aimed to evaluate the increase in tear meniscus height (TMH) induced by 3% diquafosol ophthalmic solution in eyes with contact lens (CL).
Methods: Ten healthy subjects wearing high-water-content CLs received topical instillation of two ophthalmic solutions – 3% diquafosol ophthalmic solution in one eye and artificial tears in the other eye. Lower TMH was measured at 5 minutes, 10 minutes, 15 minutes, 30 minutes, and 60 minutes after instillation by anterior segment optical coherence tomography.
Results: TMH increased significantly (P<0.001) at 5 minutes and 15 minutes after instillation of saline compared with the baseline values. After instillation of 3% diquafosol ophthalmic solution, TMH significantly increased (P<0.05) at 5 minutes, 15 minutes, 30 minutes, and 60 minutes compared with the baseline values. Increases in TMH after diquafosol instillation were significantly greater (P<0.05) at 15 minutes, 30 minutes, and 60 minutes than increases in TMH after saline instillation.
Conclusion: Topical instillation of 3% diquafosol ophthalmic solution increases TMH for up to 60 minutes in eyes with high-water-content CLs.
Keywords: diquafosol ophthalmic solution, tear meniscus height, dry eye, contact lenses, tear film
Introduction
As reported in the “Contact Lens Discomfort” report by the Tear Film and Ocular Surface Society, several biophysical tear film changes have been associated with contact lens (CL) wear. Decrease in tear volume is one of the changes related to CL discomfort.1 Previously, we reported a remarkable decrease of tear meniscus height (TMH) with CL wear,2 especially with high-water-content CL wear by quantitative TMH measurement using anterior segment optical coherence tomography (AS-OCT). Because 75%–90% of tear volume exists in the upper and lower tear menisci,3 reduction of TMH during CL wear may be a major factor that induces CL-related dry eye symptoms. Artificial tears and tear retention agents have been widely used as possible options for tear supplementation during CL wear. Our previous preliminary investigation in a limited number of subjects showed a significant increase in TMH at 5 minutes after instillation of 3% diquafosol ophthalmic solution (Diquas, ophthalmic solution 3%; Santen Pharmaceutical, Osaka, Japan) during high-water-content CL wear.2 Diquafosol ophthalmic solution stimulates secretion of tear fluid and mucin. These actions have been reported to improve tear film stability and provide therapeutic relief for dry eye symptoms in various types of dry eyes.4–9 Therefore, we speculate that eyes with a remarkable reduction in TMH due to high-water-content CL wear might benefit from an increase in wetness by tear fluid secretion caused by diquafosol instillation.
In our current study, we evaluated whether diquafosol had the capacity to prolong increases of TMH in eyes with high-water-content CL wear in a greater number of subjects.
Materials and methods
This study was approved by the Institutional Review Board of Kansai Rosai Hospital. This research adhered to the tenets of the Declaration of Helsinki, and we obtained informed consent from all participants after the nature and possible consequences of the study were explained to them.
Twenty eyes of ten normal subjects (eight men, two women; average age: 38.1±5.8 years) with no ocular disease, except refractive errors, were analyzed. No subject had worn CLs, had undergone ocular surgery, used eye drops, or taken systemic medication. Subjects were asked to wear commercially available CLs, specifically, etafilcon A lenses (1-day ACUVUE; Johnson & Johnson, Tokyo, Japan). This lens has a high water content of 58.0% and a diameter of 14.2 mm, and it was classified by the US Food and Drug Administration as a group IV lens.
In accordance with the procedure we used in our previous study,2 TMH measurements were performed using a commercial AS-OCT (SS-1000; Tomey Corp, Nagoya, Japan). Cross-sectional images of the lower TMH were taken vertically, across the central cornea, in every subject. TMH was defined as the line distance from the fluid surface of the CL–meniscus junction to the lower eyelid–meniscus junction. On the basis of the previously described methods,2,10,11 the lower TMH values were calculated using the cross-sectional AS-OCT images.
At 20 minutes after lens insertion, each subject randomly received a single drop of 3% diquafosol ophthalmic solution in one eye and an isotonic borate-buffered saline solution (Soft Santear; Santen Pharmaceutical, Osaka, Japan) in the other eye. AS-OCT images were taken prior to and at 5 minutes, 15 minutes, 30 minutes, and 60 minutes after eye drop instillation in both eyes of each subject. The change in TMH (ΔTMH) was calculated as the difference between the baseline TMH value and the TMH value after instillation. In addition, the time course of ΔTMH with two eye drops was evaluated, and the ΔTMH values were compared between the two eye drops.
Results
The ΔTMH data obtained before and after instillation of 3% diquafosol ophthalmic solution and saline in eyes with CL wear are shown in Figure 1. Mean ΔTMHs after saline instillation were 55.8 μm, 32.7 μm, 8.4 μm, and −0.6 μm at 5 minutes, 15 minutes, 30 minutes, and 60 minutes after instillation, respectively. Mean ΔTMHs after diquafosol instillation were 75.1 μm, 66.9 μm, 52.3 μm, and 34.4 μm at 5 minutes, 15 minutes, 30 minutes, and 60 minutes after instillation, respectively. Compared with the baseline TMH values, significant increases of TMH were observed at 5 minutes, 15 minutes, 30 minutes, and 60 minutes after diquafosol instillation and at 5 minutes and 15 minutes after saline instillation. The ΔTMH after diquafosol instillation was significantly greater (P<0.05) at 15 minutes, 30 minutes, and 60 minutes compared with the ΔTMH after saline instillation.
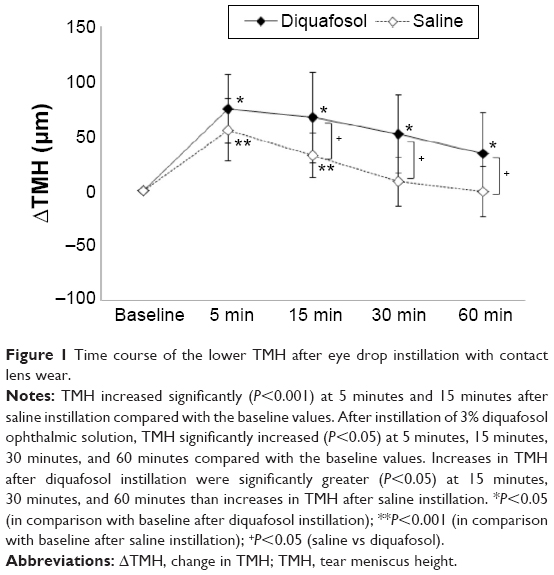 | Figure 1 Time course of the lower TMH after eye drop instillation with contact lens wear. |
Discussion
In our present study, a significant, prolonged increase in TMH was observed up to 60 minutes after diquafosol instillation in eyes with high-water-content CL wear. Furthermore, increase in TMH after diquafosol instillation was significantly greater at 15 minutes, 30 minutes, and 60 minutes than the increase in TMH after saline instillation. The results of our present study were consistent with those of our previous study,2 and it added convincing evidence of prolonged increase in wetness via use of diquafosol in eyes with CL wear.
Contact lenses divide the tear film into pre- and postlens tear films, and this compartmentalization affects biophysical changes in the tear film.1 According to a previous report,12 after instillation of artificial tears, the thickness of prelens tear film increased temporarily for a few minutes. However, there were no significant changes in the postlens tear film. It has been reported that the postlens tear film plays an important role in interactions with the ocular surface and may influence ocular comfort.1,13–15 Although prolonged increase in prelens TMH of eyes with CL wear after instillation of diquafosol ophthalmic solution was demonstrated in our current study, postlens tear film dynamics remain unknown. Although a study addressing this issue is currently under way, it will be helpful to clarify pre- and postlens tear film dynamics after instillation of artificial tears and tear retention agents in eyes with CL wear, especially symptomatic CL wearers. Using AS-OCT, future quantitative investigations of changes in thickness of pre- and postlens tear films will be possible.
Significant, prolonged increases of prelens TMH were observed after diquafosol instillation. It is expected that diquafosol ophthalmic solution, which has the potential to increase tear volume over the ocular surface beneath CLs, will become a treatment option for CL-related dryness.
Disclosure
The authors report no conflicts of interest in this work.
References
Craig JP, Willcox MD, Argüeso P, et al; members of TFOS International Workshop on Contact Lens Discomfort. The TFOS International Workshop on contact lens discomfort: report of the contact lens Interactions with the tear film subcommittee. Invest Ophthalmol Vis Sci. 2013;54(11):123–156. | ||
Nagahara Y, Koh S, Maeda N, Nishida K, Watanabe H. Prominent decrease of tear meniscus height with contact lens wear and efficacy of eye drop instillation. Eye Contact Lens. Epub 2015 Apr 1. | ||
Holly FJ. Physical chemistry of the normal and disordered tear film. Trans Ophthalmol Soc U K. 1985;104(pt 4):374–380. | ||
Matsumoto Y, Ohashi Y, Watanabe H, Tsubota K; Diquafosol Ophthalmic Solution Phase 2 Study Group. Efficacy and safety of diquafosol ophthalmic solution in patients with dry eye syndrome: a Japanese phase 2 clinical trial. Ophthalmology. 2012;119(10):1954–1960. | ||
Takamura E, Tsubota K, Watanabe H, Ohashi Y; Diquafosol Ophthalmic Solution Phase 3 Study Group. A randomised, double-masked comparison study of diquafosol versus sodium hyaluronate ophthalmic solutions in dry eye patients. Br J Ophthalmol. 2012;96(10):1310–1315. | ||
Shimazaki-Den S, Iseda H, Dogru M, Shimazaki J. Effects of diquafosol sodium eye drops on tear film stability in short BUT type of dry eye. Cornea. 2013;32(8):1120–1125. | ||
Koh S, Ikeda C, Takai Y, Watanabe H, Maeda N, Nishida K. Long-term results of treatment with diquafosol ophthalmic solution for aqueous-deficient dry eye. Jpn J Ophthalmol. 2013;57(5):440–446. | ||
Mori Y, Nejima R, Masuda A, et al. Effect of diquafosol tetrasodium eye drop for persistent dry eye after laser in situ keratomileusis. Cornea. 2014;33(7):659–662. | ||
Yamaguchi M, Nishijima T, Shimazaki J, et al. Clinical usefulness of diquafosol for real-world dry eye patients: a prospective, open-label, non-interventional, observational study. Adv Ther. 2014;31(11):1169–1181. | ||
Fukuda R, Usui T, Miyai T, Yamagami S, Amano S. Tear meniscus evaluation by anterior segment swept-source optical coherence tomography. Am J Ophthalmol. 2013;155(4):620–624. | ||
Ohtomo K, Ueta T, Fukuda R, et al. Tear meniscus volume changes in dacryocystorhinostomy evaluated with quantitative measurement using anterior segment optical coherence tomography. Invest Ophthalmol Vis Sci. 2014;55(4):2057–2061. | ||
Chen Q, Wang J, Tao A, Shen M, Jiao S, Lu F. Ultrahigh resolution measurement by optical coherence tomography of dynamic tear film changes on contact lenses. Invest Ophthalmol Vis Sci. 2010;51(4):1988–1993. | ||
Bruce AS, Mainstone JC. Lens adherence and postlens tear film changes in closed-eye wear of hydrogel lenses. Optom Vis Sci. 1996;73(1):28–34. | ||
Little SA, Bruce AS. Postlens tear film morphology, lens movement and symptoms in hydrogel lens wearers. Ophthalmic Physiol Opt. 1994;14(1):65–69. | ||
Little SA, Bruce AS. Role of the post-lens tear film in the mechanism of inferior arcuate staining with ultrathin hydrogel lenses. CLAO J. 1995;21(3):175–181. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.