")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 10 » Issue 1
Profile of a fixed-dose combination of tiotropium/olodaterol and its potential in the treatment of COPD
Authors Muruganandan S, Jayaram L
Received 15 December 2014
Accepted for publication 20 April 2015
Published 18 June 2015 Volume 2015:10(1) Pages 1179—1189
DOI https://doi.org/10.2147/COPD.S54154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Sanjeevan Muruganandan,1 Lata Jayaram2,3
1Department of Respiratory and Sleep Medicine, Austin Health, 2Department of Respiratory and Sleep Medicine, Western Health, 3University of Melbourne, Melbourne, Victoria, Australia
Abstract: Chronic obstructive pulmonary disease (COPD) is a progressive, debilitating disorder that results in frequent exacerbations and impacts quality of life. It represents a growing burden of health care cost, both from societal and economic perspectives. Short- and long-acting bronchodilators remain the mainstay of therapy in COPD patients. New fixed-dose combination inhalers with novel pharmacological combinations of long-acting β2-agonists and muscarinic antagonists and delivered once-daily through a variety of devices are currently being developed and licensed for the treatment of COPD. There is mounting research suggesting that combining a fixed dose of a β2-agonist and a muscarinic antagonist achieves better bronchodilation and clinical outcomes compared with either agent alone. These once-daily dosing inhalers are anticipated to impact favorably on patient preference and compliance. This review examines the fixed-dose combination of tiotropium bromide and olodaterol delivered by a Respimat® Soft Mist™ inhaler at doses of 2.5/5 µg and 5/5 µg in moderate-to-very-severe COPD, and its potential role in COPD compared with other long-acting β2-agonist with long-acting muscarinic antagonist combinations and delivery devices.
Keywords: fixed-dose combination inhalers, olodaterol, tiotropium bromide, COPD treatment, long-acting β2-agonists, long-acting muscarinic antagonist
Introduction
Chronic obstructive pulmonary disease (COPD) is broadly defined, and encompasses several clinical and pathologic entities, primarily emphysema and chronic bronchitis. Patients with COPD have evidence of airflow obstruction that is chronic, progressive, and for the most part fixed. Based on World Health Organization estimates as of 2004, 65 million people worldwide are affected by at least moderate-to-severe COPD.1 It is projected to move from the sixth to the fourth most common cause of death worldwide by 2030.2 COPD has a significant impact on patients’ quality of life. In general, the more severe the airflow limitation is, the greater the magnitude of symptoms and the frequency of exacerbations as well as hospital admissions.
Maintenance therapies in COPD patients are multidimensional and include pharmacological and nonpharmacological options, which are used in tandem with the aim of reducing exacerbations, improving quality of life, and increasing exercise tolerance. Long-acting β2-agonist (LABA) bronchodilators and long-acting muscarinic antagonist (LAMA) bronchodilators are the mainstay of therapy in COPD patients. Bronchodilators exert their effect by smooth-muscle relaxation, resulting in improved lung emptying, reduced thoracic gas volume and residual volume, as well as lessened dynamic hyperinflation and improved inspiratory capacity.3
Over the last decade, LABA formoterol, salmeterol, which requires twice-daily dosing, and more recently once-daily indacaterol, and the once-daily LAMA tiotropium have dominated therapeutic options in moderate-to-severe COPD.4 While comparative trials have established tiotropium to be equivalent or superior to LABAs in COPD,5,6 studies have demonstrated that when these drugs are used concurrently, there is further significant improvement in lung function and health-related quality of life measures, symptoms scores, rescue medication use,7–9 and exercise capacity.5,10 These data justify further research in this area, and recent studies have focused on the development of novel once-daily combinations of LABAs and LAMAs in one inhaler. These LAMAs and LABAs potentially offer greater convenience and compliance compared with the use of two separate inhalers.
The four new LABA/LAMA combinations available or nearing completion of Phase 3 trials include glycopyrronium bromide/indacaterol maleate (QVA149 [Ultibro®]; Novartis International AG, Basel, Switzerland) (available in Australia, Japan, and Europe) and delivered via the Breezhaler®; umeclidinium bromide/vilanterol trifenatate (Anoro®; GlaxoSmithKline, London, UK) (available in Australia, USA, and Europe), delivered via the Ellipta®, tiotropium bromide/olodaterol (Spoleto®; Boehringer Ingelheim, Ingelheim, Germany) delivered with the Respimat® Soft Mist™ inhaler, and aclidinium bromide/formoterol (LAS40464; Almirall, Barcelona, Spain) delivered via the Genuair® inhaler (available in Europe). Each combination is delivered through a unique dry powder delivery device, making comparative assessments difficult.
When to use combination LABA/LAMA therapy and fixed-dose combination (FDC) LABA/LAMA therapy?
Given the importance of bronchodilation in COPD, national and international guidelines reinforce inhaled bronchodilators as the cornerstone of treatment in all stages of disease severity. FDC inhalers are able to provide extra bronchodilation compared with either monotherapy alone, and are recommended for the use of persistent symptoms despite LABA or LAMA monotherapy (with or without inhaled corticosteroids [ICS]) (Level B4 or Level 211 evidence for improving forced expiratory volume in 1 second [FEV1] and symptoms). The Global initiative of Obstructive Lung Diseases (GOLD)4 strategy has been used in major COPD trials to categorize the severity of disease and to guide commencement of LABA or LAMA therapy.
In the GOLD4 strategy document, patients are divided into four groups (A, B, C, and D) based on FEV1, Medical Research Council (MRC) symptoms score, and the frequency of exacerbations in 1 year as follows: A) GOLD 1–2 (ie, FEV1 ≥50% predicted), few symptoms MRC <1, low exacerbation frequency (ie, ≤1 exacerbation/year and no hospitalization); B) GOLD 1–2, frequent symptoms MRC ≥2, low exacerbation frequency; C) GOLD 3–4 (ie, FEV1 <50% predicted), few symptoms MRC <1, high exacerbation frequency (≥2 exacerbation/year or ≥1 hospitalization/year); D) GOLD 3–4, frequent symptoms MRC ≥2, high exacerbation frequency. LABA/LAMA combination therapy is recommended for patients in groups B–D.4 Group B patients may use either a LABA or LAMA monotherapy, but the combination of a LABA plus a LAMA is presented as an alternative option. Patients in group C are recommended to use either LABA with an ICS or LAMA monotherapy, with alternative options of a LABA plus a LAMA, or a LABA or a LAMA plus a phosphodiesterase-4 (PDE-4) inhibitor. The same drug combinations are recommended for patients in group D.4
In the Australian COPD guidelines,11 the rationale to use a FDC bronchodilator in an inhaler-naive patient or to change a patient’s current inhaler is based on similar factors to GOLD4 in conjunction with attention to the complexity of device, patient’s preference, and occurrence of adverse events (AEs).11 The British Thoracic Society guidelines12 currently recommend the use of combination bronchodilator therapy in cases where the addition of ICS to a bronchodilator is declined or not tolerated.12 It is also suggested that LAMA plus a LABA should be offered to patients with stable COPD and an FEV1 >50% who remain breathless or have exacerbations despite maintenance therapy with a LABA.12 The American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society (ERS) suggest that clinicians may administer combination inhaled therapies (LAMA, LABA, or ICS) for symptomatic patients with stable COPD and FEV1 <60% predicted13 (graded as a weak recommendation with moderate quality evidence to support its use). There is still little evidence to determine the efficacy of FDC LABA/LAMA inhalers on exacerbation rates.
This review will focus on the combination of the novel LABA and LAMA, olodaterol with tiotropium bromide and aims to provide an insight in to the pharmacokinetics, pharmacodynamics, the Respimat® device, as well as the clinical evidence thus far.
Pharmacology
Pharmacokinetics and pharmacodynamics
Olodaterol
Olodaterol (Striverdi®) is a long-acting, inhaled, β2-adrenergic receptor agonist with a 24-hour bronchodilator profile. Olodaterol received its first global approval in 2013 for the long-term, once-daily; maintenance bronchodilator treatment of airflow obstruction in patients with COPD in Canada.14 It has been approved in a number of European countries as a once-daily dose of 5 μg given through a Respimat® Soft Mist™ inhaler.15
Olodaterol is a potent and selective agonist of the human β2-adrenergic receptor in vitro.16 Following inhalation, olodaterol binds to and activates β2-adrenergic receptors in the airway, stimulating adenyl cyclase to synthesize cyclic 3′5′-adenosine monophosphate, which then leads to smooth-muscle relaxation and bronchodilation.16 In vitro and in vivo data show that olodaterol potently reverses stimulated bronchi contraction, and reduces pro-fibrotic cellular activity in human lung fibroblast.16–18 The half-life of olodaterol is 17.8 hours.19 In animal studies, olodaterol has demonstrated efficacy over 24 hours.16 Rapid onset of action with improvement in lung function has been noted within 5 minutes after the first dose in Phase 3 trials in patients with COPD.20
Ferguson et al20 more recently established the long-term efficacy and safety of a once-daily olodaterol at 5 μg and 10 μg in patients with GOLD stage 2–4 COPD. This was a two replicate, randomized, double-blind, placebo-controlled, parallel group, Phase 3 trial over 48 weeks.20 van Noord et al21 investigated the efficacy of four different doses of olodaterol as a once-daily bronchodilator in a Phase 2 clinical trial, and showed a clear dose–response relationship with significant improvement in FEV1 from baseline with values ranging between 0.070 L and 0.119 L for at least 24 hours in patients with COPD.21 In another Phase 2 randomized, double-blind, crossover study, van Noord et al22 demonstrated a statistically significant increase in lung function (FEV1) outcome for at least 24 hours from baseline. Olodaterol was superior to placebo (P<0.001) in peak FEV1 (0.121–0.213 L) and a clear dose–response relationship was observed, with values ranging from 0.070 L for olodaterol 2 μg to 0.119 L for olodaterol 20 μg. Overall, the 5 μg dose offered a superior 24-hours profile compared to both the 10 μg daily dose and the twice-daily 2 μg dose.23 Olodaterol was tolerated at all doses that were tested. There was no relationship of total daily dose to the overall incidence of AEs.20 Comparatively, Koch et al24 performed a replicate, multicenter, randomized, double-blind, placebo-controlled, parallel group, Phase 3 study investigating the long-term efficacy and safety of once-daily olodaterol via Respimat® versus placebo and formoterol in patients with moderate-to-very-severe COPD. Olodaterol 10 μg was shown to have similar improvement in FEV1 area under the curve from 0 hour to 3 hours (AUC0–3) and trough FEV1 to twice-daily formoterol.24 The 10 μg daily dose did not provide additional improvement compared to the 5 μg daily dose.24 A recent meta-analysis where 18 trials were identified (eight, olodaterol; ten, indacaterol) evaluating the efficacy of olodaterol and indacaterol in patients with COPD, concluded that both olodaterol and indacaterol had similar efficacy when compared under similar trial conditions.25
Tiotropium bromide
Tiotropium bromide (Spiriva®) is an anticholinergic bronchodilator, normally administered as a dry powder through a HandiHaler® device. It is an antagonist of three muscarinic receptor subtypes.26 Tiotropium demonstrates competitive and reversible receptor antagonism and in vitro studies have shown that tiotropium has a half-life on the M3 receptor of 36 hours.27 FEV1 rises slowly following one dose reaching a peak after 1–3 hours and the peak response is followed by a plateau of long duration.26 van Noord et al28 found that trough FEV1 increased by 0.19 L (18%) from initial baseline after 8 days of daily administration. Tiotropium bromide is predominantly a renally excreted drug.26
Tiotropium bromide has been in the market for at least 15 years and is the first-line long-acting anticholinergic bronchodilator for maintenance therapy in COPD. It has a duration of action of more than 24 hours.6,29,30 It is taken once daily using a HandiHaler® device and was compared with standard therapy in the four-year Understanding Potential Long-term Impact on Function with Tiotropium (UPLIFT) trial, showing significant improvement in lung function and health status with no evidence of increased cardiovascular risk.31 It has level A evidence (Supplementary material) for reducing exacerbations and repeated hospitalization as well as improving symptoms and health status, and level B evidence of improving the effectiveness of pulmonary rehabilitation.4,32 In two other large trials, tiotropium was superior to salmeterol in reducing exacerbations although the difference was small.33,34
More recently, comparisons have been made between tiotropium bromide and the newer individual LAMAs and LABAs as well as their respective FDCs (Table 1). Indacaterol, a LABA, was approved in 2011 as a maintenance therapy for COPD. The INVIGORATE35 study compared indacaterol with tiotropium bromide in a randomized, placebo-controlled study involving 3,444 patients with severe COPD. There was no difference in trough FEV1; the estimated least squared mean (LSM) trough FEV1 difference between the groups was −0.011 L (LSM with indacaterol [n=1,450] 1.134 L [standard error (SE) 0.008] versus tiotropium [n=1,467] 1.145 L [SE 0.008]; one-sided 97.5% confidence interval [CI] lower limit −0.026 L; P<0.0001), exacerbation rates (indacaterol, 0.79 versus tiotropium, 0.61, ratio 1.29 [one-sided 97.5% CI upper limit 1.44]), and AEs at 12 weeks.35 Indacaterol produced statistical and clinically significant improvement in clinical outcomes of dyspnea (assessed by the transition dyspnea index [TDI]), use of rescue therapy (salbutamol), and health status (assessed by St George’s Respiratory Questionnaire [SGRQ]) when compared to tiotropium.36
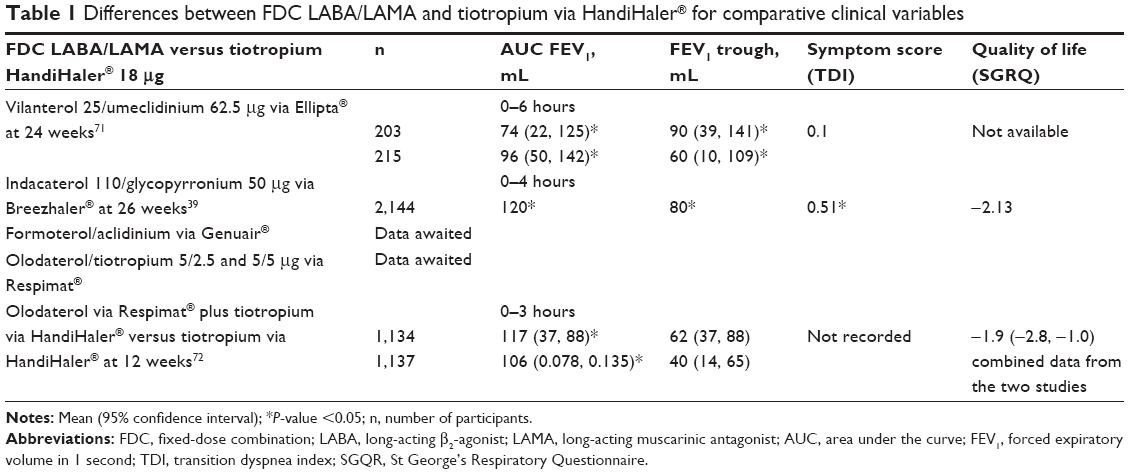 | Table 1 Differences between FDC LABA/LAMA and tiotropium via HandiHaler® for comparative clinical variables |
Glycopyrronium bromide, a LAMA, was compared to tiotropium as well as placebo in the glycopyrronium bromide in COPD airways 2 study (GLOW2)37 study, which involved 802 patients with moderate-to-severe COPD. Trough FEV1, TDI, SGRQ, reducing exacerbation, and rescue medication use was comparable in both groups.37 More recently, similar findings were also found by Chapman et al38 where 657 patients with moderate-to-severe COPD were randomized 1:1 to glycopyrronium and tiotropium.38 The FDC Ultibro® (glycopyrronium plus indacaterol) has been compared to tiotropium in three different Phase 3 studies, namely SHINE,39 BLAZE,40 and SPARK.41 In SHINE,39 Ultibro® improved trough FEV1 when compared with open-label tiotropium (LSM differences 80 mL; P<0.001 in all comparisons). The dyspnea score for Ultibro® was also significantly higher than for tiotropium (LSM difference 0.49, 95% CI 0.07–0.91; P=0.021).39 These results however did not reach clinical significance. The overall rate of mild, moderate, and severe exacerbations was significantly reduced by glycopyrronium plus indacaterol compared with open-label tiotropium (14% reduction, relative risk [RR] 0.86, 95% CI 0.78–0.94, P=0.0017), similar to glycopyrronium alone. While glycopyrronium plus indacaterol also reduced moderate-to-severe exacerbation rates significantly compared with glycopyrronium monotherapy, they were comparable to open-label tiotropium (10% reduction, RR 0.90, 95% CI 0.79–1.02, P=0.096).41
Olodaterol and tiotropium bromide
Muscarinic receptors and β2-adrenoreceptors are physiological antagonists for smooth-muscle tone in the airway. In the airway, these receptors are expressed at different sites, indicating that the effect of combining β2-agonists and muscarinic antagonists results in dilatation across the whole bronchial tree.9,42–43 β2-agonists decrease the release of acetylcholine (ACh), and then amplify the bronchial smooth-muscle relaxation induced by the muscarinic antagonist. Tashkin et al demonstrated that combining bronchodilators with different mechanisms of action might increase the maximum degree of bronchodilation compared to using either drugs alone.7 Preclinical studies examining the combination of olodaterol and tiotropium bromide found beneficial effects, in particular offering superior bronchoprotection44,45 and anti-inflammatory effects.42 Bouyssou et al examined this FDC tiotropium and olodaterol on ACh-induced bronchoconstriction in anesthetized dogs. Inhalation of 3.0 μg of tiotropium with 6.00 μg of olodaterol (BI 1744) using a Respimat® Soft Mist™ inhaler connected to the tracheal tube provided dose-dependent protection against ACh-induced bronchoconstriction compared with either monotherapy.45 There were no relevant cardiovascular effects noted. In another study, Bouyssou et al assessed the synergistic bronchoprotection activity of olodaterol combined with tiotropium bromide and ciclesonide against ovalbumin-induced bronchoconstriction in anesthetized guinea pigs. Combining olodaterol with either tiotropium or ciclesonide displayed bronchoprotection in a dose-dependent manner.44
Drug delivery via Respimat® Soft Mist™ inhaler
Respimat® is a fine-mist inhaler delivering the medication independent of inspiratory effort and patient coordination.46 Respimat® overcomes some of the limitations of pressurized metered dose inhalers (pMDI), dry powder inhalers, and nebulizers as it is portable, propellant-free, and does not need a spacer/holding chamber. It uses mechanical energy for actuation. Given the small aerosol particle size, it is thought to have more uniform delivery to the smaller airways.46
In patients with COPD, drug delivery through a Respimat® was equally effective at a lower dose compared to a drug delivered through a pMDI.47 It is unclear if device preference leads to improved adherence or clinical outcomes. Schürmann et al47 showed that 81% preferred the device compared with a pMDI using the patient satisfaction and preference questionnaire, after a 7-week treatment period.47 There was no difference between inhalers for efficacy measures such as peak expiratory flow, rescue inhaler use, and symptom scores.46
Respimat® device and cardiovascular risk
There have been concerns regarding the safety issues around a Respimat® device delivering tiotropium. Initially, the Lung Health study34 indicated that there was increased risk of cardiac deaths in patients using ipratropium bromide, a short-acting antimuscarinic agent.34 A meta-analysis raised concerns, as it showed an increase in the primary composite end point of cardiovascular death, myocardial infarction, or stroke (RR 1.60, 95% CI 1.22–2.10) and of all-cause mortality (RR 1.29, 95% CI 1.00–1.65).48 This meta-analysis48 used 17 studies, 12 of which involved tiotropium bromide delivered by a HandiHaler®. Understanding Potential Long-term impact on Function with Tiotropium31 study is a randomized trial of 5,993 patients with COPD, where tiotropium delivered by a HandiHaler® device was compared to placebo. It concluded that tiotropium was not associated with increased risk of mortality.31 Another systematic review and meta-analysis of randomized, placebo-controlled trials involving patients using tiotropium delivered by a Respimat® device in 2011 showed a 50% increased risk of mortality.49 There was a dose-dependent effect on all-cause mortality.49 Cardiovascular death was increased with an RR of 2.05 (95% CI 1.06–3.99).49 Two other independent systematic reviews and meta-analyses have reported a similar significant increased risk of all-cause mortality with tiotropium delivered through a Respimat®.50,51 Jenkins et al in an editorial in Thorax in 2013 concluded in the absence of evidence supporting a clinical benefit advantage with tiotropium Respimat® compared with tiotropium HandiHaler®, tiotropium delivered by a Respimat® should not be prescribed in the treatment of COPD.52 More recently, these concerns have increased by a Dutch database study,53 which suggested that patients with COPD treated with the Respimat® had a 27% greater mortality rate compared with those treated with the HandiHaler®. Wise et al (TIOSPIR study) conducted a randomized, double-blind, parallel group trial involving 17,135 patients with COPD, evaluating the safety and efficacy of tiotropium delivered by a Respimat® as a once-daily dose. Tiotropium 2.5 μg or 5 μg via a Respimat® had a safety profile and exacerbation efficacy similar to that of 18 μg tiotropium using a HandiHaler®.54 More importantly, the TIOSPIR study showed no difference in mortality between the two delivery systems. This is a well-conducted study and provides more robust evidence than either the meta-analysis or the database study.53 Recently, Tashkin et al55 presented an abstract at the ERS Congress, where they pooled data from all randomized, placebo-controlled, double-blind and parallel group clinical trials of tiotropium in COPD of ≥4 weeks’ duration for which they estimated baseline creatinine clearance (Cockcroft-Gault) to provide a safety evaluation of tiotropium in both the HandiHaler® and Respimat®. A total of 10,905 patients (15 trials involved tiotropium delivered using a HandiHaler® and seven trials involved tiotropium delivered via a Respimat®) were evaluated and the conclusion was that the incidence of AEs, serious AEs, and fatal AEs with both inhaler devices compared to placebo showed no association with mild-to-moderately-impaired renal function. The database for patients with severe renal impairment is too small to draw any conclusion.55 However, the questions still remains if tiotropium delivered through the Respimat® device is safe in patients with a cardiac history or severe renal impairment, as these patient populations were excluded from the TIOSPIR study.
Clinical efficacy
Phase 3 trials
Tiotropium with olodaterol is a once-daily FDC using a Respimat® Soft Mist™ inhaler. Currently, clinical results with this particular combination have been presented as abstracts in the American Thoracic Society Congress in May 2014 and ERS Congress in September 2014 in addition to the recent publication by Buhl et al.56
Dosing
Two clinical Phase 2 trials57,58 have investigated the optimal dosing for olodaterol added to a fixed dose of tiotropium57 and for tiotropium added to a fixed dose of olodaterol.58 Significant improvements in peak FEV1 were demonstrated with tiotropium/olodaterol in three different doses of olodaterol combined with fixed dose tiotropium 5/2 μg (0.087 L, P=0.008), 5/5 μg (0.082 L, P=0.012), and 5/10 μg (0.144 L, P<0.0001) versus tiotropium monotherapy. There were also significant improvements in trough FEV1 with tiotropium/olodaterol 5/10 μg versus tiotropium monotherapy (0.168 L, P=0.034).57 The other initial Phase 2 trial by Aalbers et al58 was reported at the ERS congress in 2012. It is a dose-ranging randomized, double-blind, four-period, incomplete crossover trial of 4-weeks duration in 232 COPD patients with post-bronchodilator FEV1 of ≥30% and <80% of predicted normal. The study tested tiotropium (1.25 μg, 2.5 μg, and 5 μg) with either olodaterol 5 μg or 10 μg in separate Respimat® Soft Mist™ inhaler devices. Efficacy was measured by comparing respective doses of olodaterol as monotherapy. Tiotropium with olodaterol significantly improved lung function (FEV1) over 24 hours compared with olodaterol alone at all doses tested. After 4 weeks, the combination provided an adjusted mean difference of 0.144 L (95% CI, 0.105–0.182 L) in lung function compared to olodaterol monotherapy at baseline over the first 6 hours (FEV1 AUC0–6) and an adjusted mean difference in trough FEV1 of up to 0.080 L (95% CI, 0.042–0.119 L).58
Clinical efficacy
The TOviTO is a Phase 3 program,59 which consists of ten studies evaluating the potential benefits and safety profile of the FDC of olodaterol and tiotropium through a Respimat® Soft Mist™ inhaler. This is the largest Phase 3 trial involving over 8,000 patients with moderate-to-very-severe COPD. It includes two pivotal registration trials NCT01431274 (TOnado 1)56 and NCT01431287 (TOnado 2),56 involving over 5,000 patients and assessing lung function, quality of life, and safety.
Lung function and quality of life
TOnado 156 and TOnado 256 are a multicentered, multinational, randomized, double-blind, five-arm, parallel group studies randomizing a total of 5,163 COPD patients across the spectrum of disease severity from GOLD stage 2 to GOLD stage 4 at more than 500 trial sites in approximately 40 countries. They were performed to assess the efficacy and safety of once-daily-inhaled FDC of tiotropium and olodaterol (2.5/5 μg, 5/5 μg) compared with the individual components using the Respimat® inhaler over 52 weeks. The primary outcome measures were FEV1 AUC0–3 response and trough FEV1 response compared to baseline as well as the SGRQ total score at 24 weeks. Secondary outcomes were Mahler Transition Dyspnea Index focal score at 24 weeks and rescue medication use. There was a significant and clinically relevant improvement in lung function in both FDC of tiotropium and olodaterol doses compared with each monotherapy: with FEV1 AUC0–3 improving by over 100 mL. Statistically significant benefits were noted in quality of life and symptom measures with FDC compared with monotherapy, but these did not reach the anticipated minimal clinically important difference.
VIVACITO60 (NCT01559116), the third study within the TOviTO program, is a 6-week randomized, double-blind, crossover trial aimed at characterizing the 24-hour lung function profiles of tiotropium and olodaterol FDC at two different doses (2.5/5 μg, 5/5 μg) compared with monotherapy and placebo. All medications were delivered by the Respimat® Soft Mist™ inhaler. The primary endpoint FEV1 AUC0–24 response at week 6 improved significantly at both doses of FDC compared with tiotropium (mean treatment difference of 110–127 mL, P<0.0001) or olodaterol (mean treatment difference of 115 mL, P<0.0001), monotherapies, or with placebo (mean treatment difference of 280 mL, P<0.0001). Both doses of the tiotropium and olodaterol FDC showed similar lung function profiles with an increase of 200 mL in trough FEV1 compared with placebo.60
ENERGITO61 (NCT01969721), the fourth study in the TOviTO program, is intended to provide evidence of superior improvements in lung function with high- and low-dose FDC of tiotropium and olodaterol (FDC1.25/2.5 μg and 2.5/2.5 μg) compared with high and low dose FDC of fluticasone propionate and salmeterol (Accuhaler® 250/50 μg and 500/50 μg) in 228 COPD patients. In this four-period crossover trial, patients will undergo pulmonary function tests at regular intervals for 24 hours at the end of each 6-week treatment period. The primary outcome is change from baseline in FEV1 AUC0–12. This study is currently recruiting patients and is due to complete in January 2015.
OTEMTO 162 and 263 (NCT01964352), the fifth and sixth studies in the TOviTO program, are both randomized, double-blind, placebo- and active-controlled (tiotropium) parallel group studies to assess the efficacy of 12 weeks of once-daily treatment of two doses of tiotropium with olodaterol FDC via the Respimat® Soft Mist™ inhaler in 1,550 patients with COPD. The primary outcomes are FEV1 AUC0–3, trough FEV1 and SGRQ total score, at 12 weeks. Recruiting has not yet commenced for this trial.
Exercise endurance
TORRACTO64 (NCT01525615), the seventh study, is a randomized, double-blind, placebo-controlled study to determine the effect of 12-weeks treatment of inhaled tiotropium with olodaterol FDC at two different doses (2.5/5 μg and 5/5 μg) delivered by the Respimat® Soft Mist™ inhaler on exercise endurance time during constant work rate cycle ergometry in 390 patients with COPD. The primary end point was endurance time to symptom limitation at 12 weeks. The geometric mean endurance time during constant work rate cycle ergometry was 527.51 seconds with tiotropium and olodaterol FDC 5/5 μg (14% increase versus placebo; P=0.021) and 503.46 seconds with tiotropium and olodaterol FDC 2.5/5 μg (9% increase versus placebo; P=0.142) after 12 weeks compared to placebo (463.63 seconds). At week 12, the slope of the intensity of breathing discomfort (Borg scale) during exercise decreased with tiotropium and olodaterol FDC 5/5 μg (P=0.060) and with tiotropium and olodaterol FDC 2.5/5 μg (P=0.022).
MORACTO 165 (NCT201533922) and 266 (NCT0153935) are replicate randomized, double-blind, placebo- and active-controlled, incomplete crossover studies assessing the efficacy of high- and low-dose tiotropium and olodaterol FDC on endurance time measured by cycle ergometry and lung hyperinflation measured by inspiratory capacity. Participants (n=295 and n=291) received 4/5 treatments T/O: 5/5 μg T/O; 2.5/5 μg; T 5 μg O 5 μg, or placebo. This trial is completed and results are awaited.
PHYSACTO67 (NCT02085161), the tenth trial in the TOviTO program, is a 12-week randomized, placebo, parallel group study examining the efficacy of FDC tiotropium and olodaterol compared with monotherapy (T/O 5/5 μg, T 5 μg; O 5 μg; placebo), exercise capacity, and physical activity in addition to supervised exercise training and behavior modification in 300 patients. The Endurance Shuttle Walk Test assesses exercise capacity, the primary outcome, at 8 weeks. Secondary outcome measures include daily walking intensity measured with an activity monitor and lung function. This trial is currently recruiting participants.
A trial assessing the efficacy of FDC tiotropium and olodaterol on exacerbations and survival, DYNAGITO68 (NCTO2296138), has started recruiting patients as of January 2015.
Safety
TOnado 156 and 256 are randomized trials, which were performed to assess safety of the FDC of olodaterol and tiotropium being delivered via the Respimat® Soft Mist™ inhaler. Pooled safety results over the 52-week period were reported in 5,163 patients. Incidence of AEs was generally balanced across all treatment groups with the majority being mild-to-moderate in severity. Overall, 6.4% of AEs were considered treatment-related. The rates of serious AEs and fatalities were similar across treatment arms.
Cardiovascular side effects, in particular prolonged QT, occurred in a dose-dependent manner. In healthy volunteers, the upper limit of the 90% CI of the placebo adjusted change from baseline was below 10 ms with olodaterol 10 μg. Patients taking tiotropium had a 30–60-ms change in the corrected QT (QTc) interval. No patients had a QTc interval of >500 ms, and this finding was not replicated in any of the other studies. (Spiriva® HandiHaler® [tiotropium bromide inhalation powder] package insert. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals Inc.; January 2004).
Discussion
FDC LABA/LAMA therapy is expected to become part of the pharmacological armamentarium in the management of COPD with the recent availability of several new once-daily LABA and muscarinic antagonists and their associated promise of improved efficacy and compliance. Studies to date have demonstrated that combining olodaterol combined with tiotropium delivered via the Respimat® Soft Mist™ device, improves lung function, dyspnea, and quality of life measures significantly compared with its mono components alone in patients with GOLD stage 2–4 COPD. These agents however have not demonstrated additional clinical benefit to existing individual LABAs and LAMAs used concurrently.11 The current consensus from the Thoracic Society of Australia and New Zealand suggests that FDCs have a role as add–on therapy in improving symptomatic breathlessness: they provide an effective, convenient, and potentially safer alternative to a LABA/ICS combination in step up therapy in symptomatic patients on regular LAMA, reducing the overuse of ICS in this group.11
Once-daily medication is anticipated to increase compliance with inhaler therapy, a documented problem in patients with COPD. The use of a single, long-acting inhaler is reportedly associated with higher treatment persistence and adherence rates when compared with multiple long-acting inhaler use.69 With the advent of several new FDC long-acting once-daily LAMA/LABA combinations such as vilanterol/umeclidinium and indacaterol/glycopyrronium, the unique role of each combination including olodaterol/tiotropium needs to be determined. The diversity of the duration and rapid onset of action provided by these new agents may encourage the practice of personalized medicine where choices are guided by patient preference to drug and device, as well as phenotypic features (eg, breathlessness, non-eosinophilic airway inflammation).
The inhalational device used to deliver the FDC of olodaterol and tiotropium is a novel approach and overcomes some of the limitations of pMDI, such as hand-breath coordination and generation of high inspiratory flow.70 Currently, the evidence is inconclusive about the dangers of Respimat® delivering tiotropium. Meta-analyses and epidemiological studies comparing the tiotropium delivered via the Respimat® device with the HandiHaler® have raised the concern of an increased risk of cardiovascular events.48–51 This has been disproven in a large, well-designed and well-conducted prospective study (TIOSPIR) examining safety as its primary end point.53 The hypothesis that these findings may be due to an anticholinergic class effect remains to be tested.
Published safety data to date with FDC olodaterol/tiotropium in Phase 2 and 3 studies have shown no significant increased side effects compared with placebo. In conjunction with the increasing choice in FDC LABA/LAMA medications delivered by alternative devices, there may be a reluctance to use the Respimat® device until further data are available.
Large head-to-head comparisons among the new long FDC LABA/LAMA assessing the efficacy and safety profile with respect to cardiovascular outcomes are required. The benefits may lie in specific points of difference and reassurance of the FDC’s safety profile.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization (WHO). World Health Report, 2004: Changing History. World Health Organization; 2004. Available from: www.who.int. Accessed October 5, 2014. | ||
Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. | ||
Cazzola M, Page CP, Calzetta L, Matera MG. Pharmacology and therapeutics of bronchodilators. Pharmacol Rev. 2012;64(3):450–504. | ||
Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Global Initiative for Chronic Obstructive Lung Disease; 2014. Available from: http://www.goldcopd.org/. Accessed October 5, 2014. | ||
Vogelmeier C, Kardos P, Harari S, Gans SJ, Stenglein S, Thirlwell J. Formoterol mono- and combination therapy with tiotropium in patients with COPD: a 6-month study. Respir Med. 2008;102(11):1511–1520. | ||
Vincken W, van Noord JA, Greefhorst AP, et al; Dutch/Belgian Tiotropium Study Group. Improved health outcomes in patients with COPD during 1 yr’s treatment with tiotropium. Eur Respir J. 2002;19(2):209–216. | ||
Tashkin DP, Ferguson GT. Combination bronchodilator therapy in the management of chronic obstructive pulmonary. Respir Res. 2013;14:49. | ||
van der Molen T, Cazzola M. Beyond lung function in COPD management: effectiveness of LABA/LAMA combination therapy on patient-centered outcomes. Prim Care Respir J. 2012;21(1):101–108. | ||
Cazzola M, Molimard M. The scientific rationale for combining long-acting β2-agonists and muscarinic antagonists in COPD. Pulm Pharmacol Ther. 2010;23:257–267. | ||
Jayaram L, Wong C, McAuley C, Rea H, Zeng I, O’Dochartaigh C. Combined therapy with tiotropium and formoterol in chronic obstructive pulmonary disease: effect on 6-minute walk test. COPD. 2013;10(14):466–472. | ||
Abramson M, Crockett AJ, Dabscheck E, et al; on behalf of Lung Foundation Australia and the Thoracic Society of Australia and New Zealand. The COPD-X Plan: Australian and New Zealand Guidelines for the management of Chronic Obstructive Pulmonary Disease V2.38. Brisbane; 2014. | ||
National Clinical Guideline Centre. Chronic Obstructive Pulmonary Disease: Management of Chronic Obstructive Pulmonary Disease in Adults in Primary and Secondary Care. London: National Clinical Guideline Centre; 2010. | ||
Qaseem A, Wilt TJ, Weiberger SE, et al; American College of Physicians; American College of Chest Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American college of physicians, America college of chest physicians, America thoracic society and European Respiratory society. Ann Intern Med. 2011;155:179–191. | ||
Health Canada. Summary Basis of Decision (SBD) for Striverdi Respimat (Olodaterol Hydrochloride); 2013. Available from: http://www.hc-sc.gc.ca/. Accessed November 4, 2014. | ||
Boehringer-ingelheim.com [homepage on the internet]. c2010-14 [updated October 18, 2014; cited December 10, 2014]. Available from: www.boehringer-ingelheim.com. Accessed December 12, 2014. | ||
Bouyssou T, Casarosa P, Naline E, et al. Pharmacological characterization of olodaterol, a novel inhaled β2-adrenoceptor agonist exerting a 24-hour-long duration of action in preclinical models. J Pharmacol Exp Ther. 2010;334(1):53–62. | ||
Brown SM, Barnes PJ, Donnelly LE. Effect of Olodaterol on the Relaxation of Small Airways [abstract]. Amsterdam: Annual Congress of the European Respiratory Society; 2011. | ||
Ahmedat AS, Warnken M, Juergens UR, Paul Pieper M, Racké K. The long acting Beta2-adrenoceptor agonist olodaterol mediates inhibition of prepro-endothelin-1 expression in human lung fibroblasts. Am J Respir Crit Care Med. 2011;183:A605. | ||
Casarosa P, Kollak I, Kiechle T, et al. Functional and biochemical rationales for the 24-hour-long duration of action of olodaterol. J Pharmacol Exp Ther. 2011;337(3):600–609. | ||
Ferguson GT, Feldman GJ, Hofbauer P, et al. Efficacy and safety of olodaterol once daily delivered via Respimat® in patients with GOLD 2–4 COPD: results from two replicate 48-week studies. Int J Chron Obstruct Pulmon Dis. 2014;9:629–645. | ||
van Noord JA, Smeets JJ, Drenth BM, et al. 24-hour bronchodilation following a single dose of the novel β2-agonist olodaterol in COPD. Pulm Pharmacol Ther. 2011;24(6):666–672. | ||
van Noord JA, Korducki L, Hamilton A, Koker P. Four weeks once daily treatment with BI 1744 CL, a novel long-acting β2-agonist, is effective in COPD patients [abstract]. Am J Respir Crit Care Med. 2009;179:A6183. | ||
Joos G, Aumann JL, Coeck C, Korducki L, Hamilton AL, van Noord J. Comparison of 24-hour FEV1 profile for once-daily versus twice-daily treatment with olodaterol, a novel long-acting β2-agonist, in patients with COPD [abstract]. Am J Respir Crit Care Med. 2012;185:A2930. | ||
Koch A, Pizzichini E, Hamilton A, et al. Lung function efficacy and symptomatic benefit of olodaterol once daily delivered via Respimat® versus placebo and formoterol twice daily in patients with GOLD 2–4 COPD: results from two replicate 48-week studies. Int J Chron Obstruct Pulmon Dis. 2014;9:697–714. | ||
Roskell NS, Anzueto A, Hamilton A, Disse B, Becker K. Once-daily long-acting beta-agonists for chronic obstructive pulmonary disease: an indirect comparison of olodaterol and indacaterol. Int J Chron Obstruct Pulmon Dis. 2014;9:813–824. | ||
Maesen FP, Smeets JJ, Sledsens TJ, Wald FD, Cornelissen PJ. Tiotropium bromide, a new long-acting antimuscarinic bronchodilator: a pharmacodynamic study in patients with chronic obstructive pulmonary disease (COPD). Dutch Study Group. Eur Respir J. 1995;8:1506–1513. | ||
Coulson FR, Fryer AD. Muscarinic acetylcholine receptors and airway diseases. Pharmacol Ther. 2003;98:59–69. | ||
van Noord JA, Smeets JJ, Custers FL, Korducki L, Cornelissen PJ. Pharmacodynamic steady state of tiotropium in patients with chronic obstructive pulmonary disease. Eur Respir J. 2002;19:639–644. | ||
van Noord JA, Bantje TA, Eland ME, Korducki L, Cornelissen PJG. A randomised controlled comparison of tiotropium and ipratropium in the treatment of chronic obstructive pulmonary disease. Thorax. 2002;55(4):289–294. | ||
Casaburi R, Mahler DA, Jones PW, et al. A long-term evaluation of once-daily inhaled tiotropium in chronic obstructive pulmonary disease. Eur Respir J. 2002;19(2):217–224. | ||
Tashkin DP, Celli B, Senn S, et al; UPLIFT Study Investigators. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. | ||
Kesteri S, Casaburi R, Kukafka D, Copper CB. Improvement in self-reported exercise participation with the combination of tiotropium and rehabilitative exercise training in COPD patients. Int J Chron Obstruct Pulmon Dis. 2008;3:126–136. | ||
Vogelmeier C, Hederer B, Glaab T, et al; POET-COPD Investigators. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med. 2011;364(12):1093–1103. | ||
Anthonisen NR, Connett JE, Enright PL, Manfreda J. Hospitalizations and mortality in the Lung Health Study. Am J Respir Crit Care Med. 2002;166(3):333–339. | ||
Decramer ML, Chapman KR, Dahl R, et al; INVIGORATE Investigators. Once-daily indacaterol versus tiotropium for patients with severe chronic obstructive pulmonary disease (INVIGORATE): a randomised, blinded, parallel-group study. Lancet Respir Med. 2013;1(7):524–533. | ||
Rodrigo GJ, Neffen H. Comparison of indacaterol with tiotropium or twice-daily long-acting beta-agonists for stable COPD: a systematic review. Chest. 2012;142:1104–1110. | ||
Kerwin E, Hébert J, Gallagher N, et al. Efficacy and safety of NVA237 versus placebo and tiotropium in patients with COPD: the GLOW2 study. Eur Respir J. 2012;40(5):1106–1114. | ||
Chapman KR, Beeh KM, Beier J, et al. A blinded evaluation of the efficacy and safety of glycopyrronium, a once-daily long-acting muscarinic antagonist, versus tiotropium, in patients with COPD: the GLOW5 study. BMC Pulm Med. 2014;14(1):4. | ||
Bateman ED, Ferguson GT, Barnes N, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. Eur Respir J. 2013;42(6):1484–1494. | ||
Mahler DA, Decramer M, D’Urzo A, et al. Dual bronchodilation with QVA149 reduces patient-reported dyspnoea in COPD: the BLAZE study. Eur Respir J. 2014;43(6):1599–1609. | ||
Wedzicha JA, Decramer M, Ficker JH, et al. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): a randomised, double-blind, parallel-group study. Lancet Respir Med. 2013;1(3):199–209. | ||
Dale PR, Cernecka H, Schmidt M, et al. The pharmacological rationale for combining muscarinic receptor antagonists and beta-adrenoreceptor agonists in the treatment of airway and bladder disease. Curr Opin Pharmacol. 2014;16:31–42. | ||
Costa L, Roth M, Miglino N, et al. Tiotropium sustains the anti-inflammatory action of olodaterol via the cyclic AMP pathway. Pulm Pharmacol Ther. 2014;27:29–37. | ||
Bouyssou T, Casarosa P, Pieper M, et al. Synergistic Bronchoprotective Activity of the Long-Acting Beta 2-Agonist Olodaterol with Tiotropium (Long-Acting M3 Antagonist) and Ciclesonide (Inhaled Steroid) on the Ovalbumin-Induced Bronchoconstriction in Anaesthetized Guinea Pigs [abstract]. Amsterdam: Annual Congress of the European Respiratory Society; 2011. | ||
Bouyssou T, Schnapp A, Casarosa P, Pieper MP. Addition of the new once-daily LABA BI 1744 to tiotropium results in superior bronchoprotection in pre-clinical models [abstract]. Am J Respir Crit Care Med. 2010;181:A4445. | ||
Brand P, Hederer B, Austen G, Dewberry H, Meyer T. Higher lung deposition with Respimat Soft Mist Inhaler than HFA-MDI in COPD patients with poor technique. Int J Chron Obstruct Pulmon Dis. 2008;3:763–770. | ||
Schürmann W, Schmidtmann S, Moroni P, Massey D, Qidan M. Respimat® Soft Mist™ inhaler versus hydrofluoroalkane metered dose inhaler. Treat Respir Med. 2005;4(1):53–61. | ||
Singh S, Loke YK, Furberg CD. Inhaled anticholinergics and risk of major adverse cardiovascular events in patients with chronic obstructive pulmonary disease. JAMA. 2008;300(12):1439–1450. | ||
Singh S, Loke YK, Enright PL, Furberg CD. Mortality associated with tiotropium mist inhaler in patients with chronic obstructive pulmonary disease: systematic review and meta-analysis of randomized controlled trials. BMJ. 2011;342:d3215. | ||
Karner C, Chong J, Poole P. Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;7:CD009285. | ||
Gershon A, Croxford R, Calzavara A, et al. Cardiovascular safety of inhaled long-acting bronchodilators in individuals with chronic obstructive pulmonary disease. JAMA. 2013;173:1175–1184. | ||
Bush A, Pavord ID. Tiotropium Respimat increases the risk of mortality. Thorax. 2013;68:6–8. | ||
Verhamme K, Afonso A, Romio S, Stricker BC, Brusselle GG, Sturkenboom MC. Use of tiotropium Respimat SMI versus tiotropium HandiHaler and mortality in patients with COPD. Eur Respir J. 2013;42:606–615. | ||
Wise RA, Anzueto A, Cotton D, et al; TIOSPIR Investigators. Tiotropium Respimat inhaler and the risk of death in COPD. N Engl J Med. 2013;369(16):1491–1501. | ||
Tashkin D, Metzdorf N, Hallman C, Konen-Bergmann M, Kupas K, Dahl R. Safety of Tiotropium in Renally Impaired Patients [Abstract]. Munich, Germany: European Respiratory Society Annual Congress; 2014:923. | ||
Buhl R, Maltais F, Abrahams R, et al. Tiotropium and olodaterol fixed dose combination versus mono-components in COPD (GOLD 2–4). Eur Respir J. 2015;45:969–979. | ||
Maltais F, Beck E, Webster D, et al. Four weeks once daily treatment with tiotropium + olodaterol (BI 1744) fixed dose combination compared with tiotropium in COPD patients [abstract]. Eur Respir J. 2010;36(suppl 54):1014s. | ||
Aalbers R, Maleki-Yazdi MR, Hamilton A, et al. Dose-finding study for tiotropium and olodaterol when administered in combination via the Respimat® inhaler in patients with COPD [abstract]. Eur Respir J. 2012;40:2882S. | ||
Boehringer Ingelheim. TOviTO™ Clinical Trial Programme; 2014. Available from: http://www.boehringer-ingelheim.com. Accessed November 9, 2014. | ||
Beeh KM, Westerman J, Kirsten AM, et al. The 24-h lung-function profile of once-daily tiotropium and olodaterol fixed-dose combination in chronic obstructive pulmonary disease. Pulm Pharmacol Ther. 2015;32:53–59. | ||
clinicaltrials.gov [homepage on the internet]. Characterization of Lung Function Profile of Inhaled Tiotropium + Olodaterol Fixed Dose Combination Compared to Fluticasone Propionate + Salmeterol Fixed Dose Combination in COPD Patients. ClinicalTrials.gov Identifier: NCT01969721; 2013 [updated December 11, 2014]. Available from: https://clinicaltrials.gov/ct2/show/NCT01969721. Accessed December 12, 2014. | ||
clinicaltrials.gov [homepage on the internet]. Tiotropium + Olodaterol Fixed Dose Combination (FDC) in Chronic Obstructive Pulmonary Disease (OTEMTO 1). ClinicalTrials.gov Identifier: NCT01964352; 2013 [updated December 11, 2014]. Available from: https://clinicaltrials.gov/ct2/show/NCT01964352. Accessed December 12, 2014. | ||
clinicaltrials.gov [homepage on the internet]. Tiotropium + Olodaterol Fixed Dose Combination (FDC) in Chronic Obstructive Pulmonary Disease (OTEMTO 2). ClinicalTrials.gov Identifier: NCT02006732; 2013 [updated December 11, 2014]. Available from: https://clinicaltrials.gov/ct2/show/NCT02006732. Accessed December 12, 2014. | ||
Maltais F, Iturri JG, Kirsten A, et al. P250 effects of 12 weeks of once-daily tiotropium and olodaterol fixed-dose combination on exercise endurance in patients with COPD. Thorax. 2014;69(suppl 2):A186–A187. | ||
clinicaltrials.gov [homepage on the internet]. Effect on Exercise Endurance and Lung Hyperinflation of Tiotropium + Olodaterol in COPD Patients. ClinicalTrials.gov Identifier: NCT01533922; 2012 [updated April 30, 2014]. Available from: https://clinicaltrials.gov/ct2/show/NCT201533922. Accessed December 12, 2014. | ||
clinicaltrials.gov [homepage on the internet]. Effect on Exercise Endurance and Lung Hyperinflation of Tiotropium + Olodaterol in COPD Patients. ClinicalTrials.gov Identifier: NCT01533935; 2012 [updated April 30, 2014]. Available from: https://clinicaltrials.gov/ct2/show/NCT01533935. Accessed December 12, 2014. | ||
clinicaltrials.gov [homepage on the internet]. To Evaluate the Effect of Inhaled Medication Together With Exercise and Activity Training on Exercise Capacity and Daily Activities in Patients With Chronic Lung Disease With Obstruction of Airways. ClinicalTrials.gov Identifier: NCT02085161; 2014 [updated December 11, 2014]. Available from: https://clinicaltrials.gov/ct2/show/NCT02085161. Accessed December 12, 2014. | ||
Comparing the Efficacy of Tiotropium + Olodaterol (5/5 μg) Fixed Dose Combination (FDC) Over Tiotropium 5 μg in Reducing Moderate to Severe Exacerbations in Patients With Severe to Very Severe Chronic Obstructive Pulmonary Disease. ClinicalTrials.gov Identifier: NCT02296138; 2014 [updated December 11, 2014]. Available from: http://clinicaltrials.gov/ct2/show/NCT02296138. Accessed December 12, 2014. | ||
Yu AP, Guérin A, Ponce de Leon D, et al. Therapy persistence and adherence in patients with chronic obstructive pulmonary disease: multiple versus single long-acting maintenance inhalers. J Med Econ. 2011;14:486–496. | ||
Anderson P. Use of Respimat® Soft Mist™ Inhaler in COPD patients. Int J Chron Obstruct Pulmon Dis. 2006;1(3):251. | ||
GlaxoSmithKline. FDA Advisory Committee Briefing Document. ANOROTM ELLIPTATM (umeclidinium bromide/vilanterol inhalation powder) for treatment of chronic obstructive pulmonary disease. NDA 203975. Presented to Pulmonary-Allergy Drug Advisory Committee; 2013. Available from: www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/Pulmonary-AllergyDrugsAdvisory Committee/UCM367414.pdf. Accessed December 7, 2014. | ||
ZuWallack R, Allen L, Hernandez G, Ting N, Abrahams R. Efficacy and safety of combining olodaterol Respimat® and tiotropium HandiHaler® in patients with COPD: results of two randomized, double-blind, active-controlled studies. Int J COPD. 2014;9:1133–1144. |
Supplementary materials
- Classification of Levels of Evidence
Level A: Evidence is from end points of well-designed RCTs that provide a consistent pattern of findings in the population for which the recommendation is made. It requires substantial number of studies involving substantial number of participants.
Level B: Evidence is from endpoints of intervention studies that include a limited number of patients, post hoc or subgroup analysis of RCTs, or meta-analysis of RCTs. In general, Category B pertains when few randomized trials exist, and were undertaken in a population that differs from the target population of the recommendation, or the results are somewhat inconsistent.
Level C: Evidence is from outcomes of uncontrolled or non-randomized trials or from observational studies.
Level D: Panel consensus judgment based on clinical experience or knowledge that does not meet the above-listed criteria.
NHMRC Level 1: Evidence obtained from systemic review of all relevant randomized controlled trials.
NHMRC Level 2: Evidence obtained from at least one properly designed and conducted randomized controlled trial.
NHMRC Level 3Level 3.1: Evidenced obtained from well-designed pseudorandomized controlled trials (alternate allocation or some other method)
Level 3.2: Evidence obtained from comparative studies (including systematic reviews of such studies) with concurrent controls and allocation not randomized, cohort studies, case-control studies, or interrupted time series with a control group
Level 3.3: Evidence obtained from comparative studies with historical control, two or more single arm studies, or interrupted time series without a parallel group.
NHMRC Level 4: Evidence obtained from case series, either posttest or pretest/posttest. - Modified Medical Research Council Dyspnea (mMRC) scale
Score 0: I get breathless only with strenuous exercise.
Score 1: I get short of breath when hurrying on a level ground or walking up a slight hill.
Score 2: On level ground, I walk slower than other people my age because of breathlessness, or I have to stop for a breath when walking at my own pace.
Score 3: I stop for breath after walking about 100 yards or after a few minutes on level ground.
Score 4: I am too breathless to leave the house or I am breathless when dressing.
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.