")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
Prevalence of depression and its relationship with work characteristics in a sample of public workers
Authors Luca M, Bellia S, Bellia M, Luca A, Calandra C
Received 2 November 2013
Accepted for publication 8 January 2014
Published 25 March 2014 Volume 2014:10 Pages 519—525
DOI https://doi.org/10.2147/NDT.S56989
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Maria Luca,1 Salvatore Bellia,2 Marcello Bellia,3 Antonina Luca,4 Carmela Calandra1
1Department of Medical and Surgery Specialties, Psychiatry Unit, 2Department of Biomedical Sciences, General Pathology Unit, University Hospital Policlinico-Vittorio Emanuele, 3B Ramazzini Institute, 4Department GF Ingrassia, Section of Neuroscience, University Hospital Policlinico-Vittorio Emanuele, Catania, Sicily, Italy
Abstract: Occupation is a fundamental right, enabling social interaction and financial support for the individual. However, it is an undeniable source of stress, with consequences for physical and mental health. The prevalence of depression and somatic complaints were assessed in 1,013 public workers using the Beck Depression Inventory and a questionnaire investigating for the presence of somatic problems designed by the research team. The results were related to demographic characteristics, history of previous depressive episodes, work schedule (day work, night and day rotating shift work, day rotating shift work), and duration of current work schedule. There were more cases of moderate depression in the day rotating shift workers (84%) than in those working at night (83%). More women had mild or moderate depression than men (22% and 4% versus 10% and 3%, respectively). Severe depression was found only in men. Nearly 10% of depressed individuals reported previous depressive episodes. A link between depression and somatic complaints was also found. In particular, 59% of depressed subjects reported gastrointestinal complaints and 41% did not (P<0.001). In conclusion, the occurrence of depressive symptoms could be facilitated by occupation. A history of depressive symptoms should not be neglected, given the risk of recurrence. Somatic complaints could represent a “wake-up call” regarding depression. Global assessment and effective support are fundamental for promotion of a better quality of life in the at-risk category of workers.
Keywords: depression, somatic complaints, previous depressive episodes, workers, work schedule, working period
Introduction
Occupation is a fundamental right, enabling social interaction and financial support for the individual. However, it is an undeniable source of stress, with consequences for physical and mental health.
Research in this field is growing, especially regarding night work and rotating shift work, which have consequences for the circadian system,1 as well as general health (determining alterations of gastrointestinal, central nervous, and cardiovascular systems).2 The negative effect on the circadian system becomes evident when considering shift work sleep disorder, that is common among night and rotating shift workers and has impact on health and behavior. In fact, individuals with shift work sleep disorder (males in particular), have been found to have high rates of depression,3,4 sleepiness-related accidents, absenteeism, and ulcers.3 In addition, a sympathetic predominance and reduced heart rate variability have been demonstrated in white-collar workers complaining of poor sleep.5 The link between shift work and peptic ulcer disease is probably due to an imbalance of protective and aggressive factors acting on the gastric mucosa at night, but to date data in the literature are controversial.6,7 Moreover, a high level of job strain represents a risk factor for retirement on health grounds.8
With regard to depression, higher levels of symptoms of stress were found in nurses undertaking three-shift work compared with those performing two-shift work.9 The years of shift work also play a role in the occurrence of depressive symptoms, with the prevalence of depressive disorders found to be over six times higher in night workers who had worked 6–10 years when compared with those who had done so for 1–5 years.10 Further, middle-aged workers seem to have an increased suicide risk.11 However, mild emotional disorders (mild depression, tension, anxiety, or insomnia) were found to be less frequent among night and ex-night workers than among day workers, probably because day workers are more exposed to stress.12
Generally speaking, shift work, type of job, and work environment are important predictors of health-related outcomes in workers.13 For example, precarious employment has been associated with a high prevalence of occupational injuries, a higher mortality rate, and poor mental health.14 On the other hand, permanent workers were found to suffer greater distress about job pressure, whereas fixed term workers were more distressed by job insecurity.15
In the light of what has been reported, it is clear that the link between work and illness (both physical and mental) is complex and related to various factors. To the best of our knowledge, there are no studies investigating this issue from a holistic point of view, simultaneously considering the multiple demographic, clinical, and working variables that could play a role in the occurrence of work-related health problems. The aim of this study was to determine the prevalence of depression in a sample of workers and its relationship with age, sex, marital status, somatic complaints, work schedule (day work, day rotating shift work, night and day rotating shift work), duration of current work schedule, and presence of previous depressive episodes.
Materials and methods
Data collection
One thousand and thirteen public workers (706 men and 307 women, mean age 40.8±88 years) referred to the Occupational Health Unit by their employers for a check-up were enrolled consecutively from January 2009 to January 2010 and assessed using anonymous questionnaires. Each individual signed their written informed consent.
Sample characteristics
The sample population was divided into three categories of workers, according to their work schedule: day workers who worked only in the morning hours (n=289, 28.5%); night and day rotating shift workers (n=358, 35.3%); and day rotating shift workers (n=366, 36.1%).
Measurements
Each individual was assessed using the Italian version of the Beck Depression Inventory (BDI) for the presence and severity of depressive symptoms. The BDI is composed of 21 items each with a score from 0 to 3. A total BDI score of 0–9 indicates normal, 10–18 indicates mild depression, 19–29 indicates moderate depression, and 30–63 indicates severe depression.16,17
All workers in the study were asked to supply the following demographic data: sex, age, marital status, work schedule (night and day rotating shift work, day rotating shift work, day work), duration of current work schedule and, if present, previous episodes of mood disorder (depression, mania, irritability, unstable mood). In addition, the research group designed the list below to investigate for the presence of somatic complaints/disorders:
- cardiovascular system (hypertension, hypotension, bradycardia, tachycardia, extrasystoles, atrial fibrillation, angina pectoris, previous myocardial infarction, other)
- respiratory system (dyspnea, recurrent cough, asthma, pain associated with breathing, previous pneumonia, other)
- gastrointestinal system (abdominal colic, heartburn, constipation, diarrhea, jaundice, increased appetite, decreased appetite, other)
- urinary system (kidney stones, pain or burning with urination, increased urination, decreased urine output, hematuria, other)
- reproductive system (decreased sexual desire, increased sexual desire, impotence, amenorrhea, bleeding, menstrual pain, other)
- musculoskeletal system (bone and joint pain, osteoporosis, fatigue, other)
- cutaneous system (itching, rashes, spots on sun-exposed areas, bubbles, blisters, dry skin, other)
- blood and lymphatic system (anemia, leukemia, platelet disorders, other)
- nervous system (headache, tremors, paralysis, movement disorders, seizures, visual disturbances, hearing impairment, other).
Each individual was asked to underline the listed problems which affected him/her and indicate any other nonlisted problems.
Data analysis
The data were analyzed using Statistical Package for Social Science software (SPSS Inc., Chicago, IL, USA). Quantitative values are shown as the mean ± standard deviation and categorical variables are expressed as the frequency (percentage). Differences between proportions were evaluated using the chi-squared test. Correlations were evaluated using Pearson’s correlation. P-values ≤0.05 were considered to be statistically significant.
Results
Sample characteristics
The sample consisted of 1,013 public workers, comprising 531 (52%) health workers, 445 (43%) transport operators, and 37 (3%) university employees. Seven hundred and six (70%) were male and 307 (30%) were female. The mean age of the total sample was 40.8±8.8 (range 24–64) years; the mean age was 41±8.6 years for men and 39.4± 9 years for women. Three age groups were formed as follows: 24–35 years (n=313, 31%), 36–50 years (n=547, 54%), and 51–64 years (n=153, 15%, see Table 1). Eight hundred and twelve individuals (80%) were married, 43 (4%) were divorced, 143 (14%) were single, and 15 (1%) were widowed; 617 men (87%) and 195 women (63%) were married; 15 men (2%) and 28 women (9%) were divorced; 72 men (15%) and 71 women (23%) were single; and three men (0.4%) and 12 women (4%) were widowed.
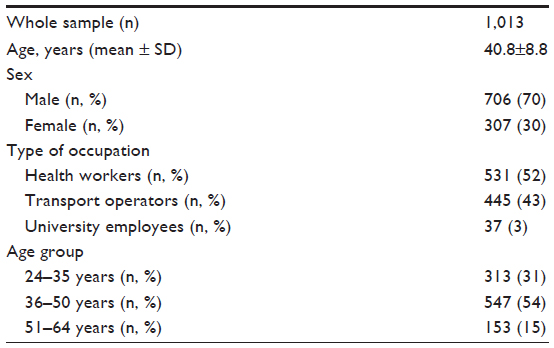 | Table 1 General characteristics of the study sample |
Relationship between BDI score and sex, marital status, and age group
Of the 1,013 individuals in the study, 841 (83%) reported depression and 172 (17%) reported no depression. Specifically, 138 (14%) had mild depression, 31 (3%) had moderate depression, and three (0.3%) had severe depression. Females had higher rates of depression than men, (26% versus 13%). In terms of severity, they presented more cases of mild depression (22% versus 10%) and moderate depression (4% versus 3%). On the other hand, only men showed severe depression (0.4%).
The highest percentage of nondepressed individuals was found in the married category (85%), followed by those who were single (82%). The highest rates of mild depression were found in widowed (47%) and divorced (28%) subjects, and the highest rates of moderate depression were found in divorced subjects (7%), followed by married (3%) and single (3%) subjects. Severe depression was found in a few cases (0.2% of married and 0.7% of single subjects). A statistically significant difference was found when comparing the percentage of married nondepressed subjects (85%) and that of nondepressed divorced subjects (65%, P<0.05); a statistically significant difference was also found between rates of mild depression in married subjects (13%) and widowed subjects (47%, P<0.05, see Table 2).
 | Table 2 Marital status and depression |
The risk of depression increased with increasing age. The percentage of subjects aged 51–64 years suffering from mild depression was significantly greater than that in subjects aged 24–35 years (18% versus 11%, respectively, P<0.05). One case of moderate depression and one of severe depression were found in each age group; hence, these few cases have been grouped into a unique class (moderate-severe depression) while performing the statistical analysis pertaining the age groups (see Table 3).
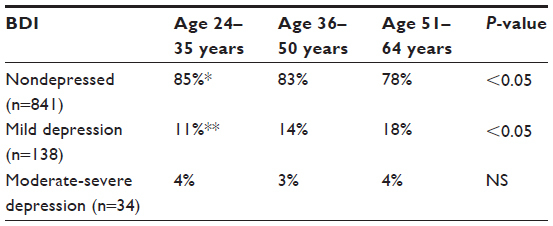 | Table 3 Age groups and depression |
Relationship between BDI score and work schedule
Fifty-two (18%) day workers reported depression and 237 (82%) did not, 62 (17%) of night and day rotating shift workers reported depression and 296 (83%) did not, and 57 (16%) of day rotating shift workers reported depression and 309 (84%) did not. No marked differences in severity of depression were identified. Interestingly, there were more cases of moderate depression among day rotating shift workers (3%) than in night and day rotating shift workers (2%, see Table 4). Rates of depression were higher among women regardless of work schedule, except for severe depression, which was found only in men (see Table 5).
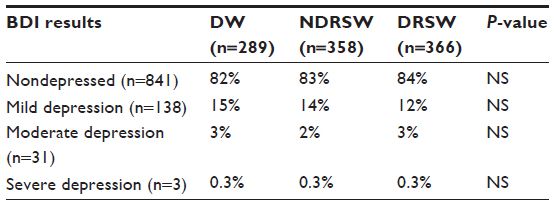 | Table 4 Relationship between BDI results, work schedule, and depression |
 | Table 5 Work schedule, sex, and depression |
Relationship between BDI score and duration of current work schedule
Three categories for duration of current work schedule were considered, from the most recent to the most distant, ie, workers who started working in 2005–2010, those who started working in 1990–2004, and those who started working in 1970–1989. These categories were created for every work schedule.
For day workers and day rotating shift workers, the percentages of nondepressed subjects were higher among those who started working more recently, ie, in 2005–2010, but decreased with increasing duration of current work schedule (1990–2004), and then increased again in those who had started shift work in 1970–1989. For night and day rotating shift workers, the highest percentage of nondepressed individuals was found in the group that started working more recently (2005–2010), but this percentage fell steeply with increasing duration of current work schedule (1990–2004 and 1970–1989, see Table 6).
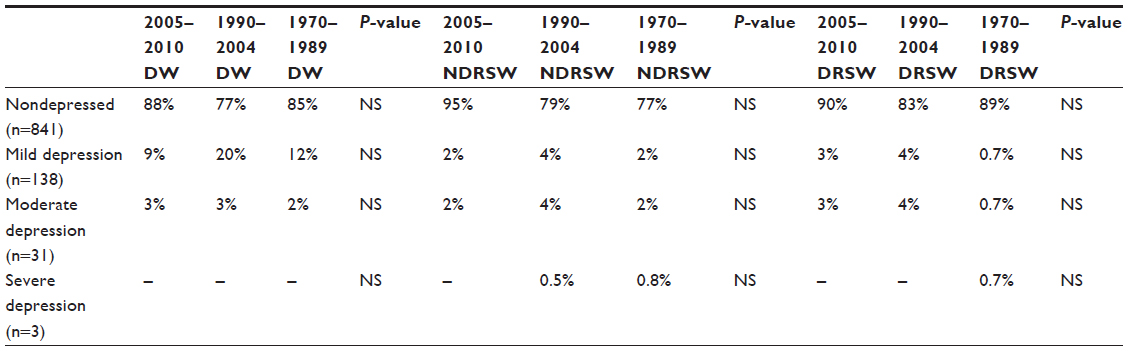 | Table 6 Work schedule, working period, and depression |
Relationship between BDI score and history of depressive episodes and somatic complaints
Previous depressive episodes and cardiovascular, respiratory, and gastrointestinal problems were the most frequently reported complaints, so the statistical analysis was limited to these variables. Thirty-seven subjects in the whole sample reported previous depressive episodes; 17 (45%) suffered from depression according to the BDI and 20 (55%) did not.
A total of 247 subjects reported cardiovascular problems, particularly tachycardia, arrhythmia, and hypertension. Of these, 230 were not depressed (representing 27% of the total number of subjects without depression) and 17 were depressed (representing 10% of all depressed workers). One hundred and ten subjects complained of respiratory problems, particularly chronic bronchitis, cough, and dyspnea. Eighty-five of these were not depressed (10% of the total number of subjects without depression) and 25 were depressed (14% of all depressed workers).
In total, 386 workers reported gastrointestinal problems, particularly dyspepsia, epigastric pain, constipation, irritable bowel syndrome; of these 235 were not depressed (27% of the total number of subjects without depression) and 101 were depressed (59% of all depressed workers). Gastrointestinal disturbances (33%) were the most frequently reported somatic problem in the whole sample.
Cardiovascular disturbances were reported by 93% of nondepressed subjects and 7% of depressed subjects; respective percentages were 77% and 23% for respiratory disturbances and 70% and 30% for gastrointestinal disturbances.
The relationship between previous depressive episodes, somatic complaints, and current depression was investigated using Pearson’s chi-squared test. Comparing individuals with and without depression (mild to severe) or previous depressive episodes, a statistically significant correlation was found between previous depressive episodes and current depression (χ2=48.261, P<0.001). Gastrointestinal problems were the most common somatic complaints in individuals with depression, with 59% of depressed subjects reporting gastrointestinal complaints and 41% of depressed subjects not reporting such complaints (P<0.001).
Discussion and conclusion
Stress is associated with a variety of physical and mental health problems, including physiological hyperarousal, negative cognition, and negative mood.18 A high risk of hospitalization for depression has been demonstrated in human service workers.19 Moreover, a higher rate of antidepressant use has been found in employees undertaking a person-related work than in individuals doing non-person-related work.20
Our present findings suggest that marital status plays a role in the risk of depression. We found the lowest rate of depression among married individuals, and the highest rate of mild depression in individuals who were widowed. Age was also related to the presence of depressive symptoms, with a significantly higher prevalence of mild depression found among older subjects (aged 51–64 years). In this study, approximately 10% of depressed subjects reported having had previous depressive episodes. Moreover, even though no statistically significant differences were found when considering depression and work schedule/duration of current work schedule, the raw values suggest some influence of these variables on the occurrence of depressive symptoms. A link between depression and somatic complaints (gastrointestinal disturbances in particular) was also found.
The prevalence of major depression in our sample of workers was higher than that in the general Italian population.21 Our data support the hypothesis that work represents an objective source of stress and could facilitate the occurrence of depressive symptoms. Several studies have reported that symptoms of depression are commonly perceived by patients as interfering significantly with their work performance. Moreover, epidemiologic research found that community workers with depression were at least five times more likely to miss work than workers with no symptoms of depression. Depressed patients being treated in primary care miss two to four more days of work per month due to disability than patients without depression.22 These data underscore the importance of screening for symptoms of depression among workers.23
As reported elsewhere in the literature,24 in our sample, the frequency of depression in women (26%) was higher than that in men (13%). The higher prevalence of depression in female workers probably reflects their different role in society. In reality, women are exposed to a “double burden”, having to dedicate themselves to both work and family; paradoxically, they might prefer to work at night in order to have more time to take care of children.25 Hence, shift work might affect mental health in men and women in different ways.26 In addition, the woman traditionally stays home after the birth of a child, because she is the one mainly responsible for caring for children.27 With regard to their role in the workplace, women usually report less decision-making opportunities and more work-related stress than their male colleagues.28 In contrast with data reported in the literature,29 work schedule did not significantly influence the likelihood of depression, even though moderate depression was more frequent in day workers than in night and day rotating shift workers. For night workers in particular, the duration of the current work schedule has been suggested to play a role in the likelihood of depressive symptoms.26
The prevalence of depression was positively related to the duration of all current work schedules; however, the risk of having depressive symptoms was lower in day workers and day rotating shift workers who had been working these shifts for longer periods of time. In contrast, this risk did not decrease in night and day rotating shift workers, indicating that night shifts have some degree of long-term “depressogenic” effect. Night work can trigger disturbances in the sleep/wake cycle and difficulty in maintaining family and social relationships, with consequent negative influences on marital relationships, care of children, and social contacts, and deterioration of health that can manifest in disturbances of sleep and eating habits.2 Previous depressive episodes, as expected, increased the likelihood of depression, so represent a predictor of recurrent depressive episodes; therefore, a history of depression should not be underestimated.30,31 A proportion of individuals complaining of cardiovascular, respiratory and gastrointestinal problems were found to be depressed. In particular, 30% of individuals complaining of gastrointestinal disturbances were depressed, and somatic complaints may be linked to an underlying psychiatric illness.32 A previous study has reported a positive association between the characteristics of somatic symptoms (number, frequency, and associated disability) and severity of depression in patients with major depressive disorder.33 In view of this, when assessing workers, such complaints should be interpreted as a possible “wake-up call” for depression. Hence, global assessment and effective support are fundamental for promotion of better quality of life in this at-risk category of workers.
In conclusion, this work has some limitations but also some strengths. The main strength of this study lies in the large number of workers evaluated in terms of both somatic and mental conditions. Another strength of our study is that it included contemporaneous analysis of workers undertaking a variety of shift work schedules. To the best of our knowledge, this is the first study to evaluate day workers, night and day rotating shift workers, and day rotating shift workers simultaneously while taking into consideration depression and somatic complaints. The main limitation of our study is that its design did not allow determination of the time of onset of depressive symptoms, which would be useful when correlating depression and work characteristics. Future prospective studies are necessary to confirm our results.
This paper highlights a need for careful psychiatric assessment of workers, in particular when treating them for somatic complaints. It is interesting to note that none of the workers who were found to be depressed were referred to the Occupational Health Unit by their employers for a suspected psychiatric illness, but only for a check-up. Psychological observation of workers should play an increasingly important role in the field of occupational medicine.
Acknowledgment
This article is dedicated to the memory of Dr Maurizio Cristofolini.
Disclosure
The authors report no conflicts of interest in this work.
References
Scott AJ. Shift work and health. Prim Care. 2000;27:1057–1079. | |
Costa G. The impact of shift and night work on health. Appl Ergon. 1996;27:9–16. | |
Drake CL, Roehrs T, Richardson G, Walsh JK, Roth T. Shift work sleep disorder: prevalence and consequences beyond that of symptomatic day workers. Sleep. 2004;27:1453–1462. | |
Yu SF, Gu GZ, Zhou WH, Zhou SY, Yang XF, Sun SY. [Gender difference of relationship between occupational stress and depressive symptoms]. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 2001;29:887–892. Chinese. | |
Kageyama T, Nishikido N, Kobayashi T, Kurokawa Y, Kaneko T, Kabuto M. Self-reported sleep quality, job stress, and daytime autonomic activities assessed in terms of short-term heart rate variability among male white-collar workers. Ind Health. 1998;36:263–272. | |
Johns CE, Newton JL, Westley BR, May FE. The diurnal rhythm of the cytoprotective human trefoil protein TFF2 is reduced by factors associated with gastric mucosal damage: ageing, Helicobacter pylori infection, and sleep deprivation. Am J Gastroenterol. 2005;100:1491–1497. | |
Van Mark A, Spallek M, Groneberg DA, Kessel R, Weiler SW. Correlates shift work with increased risk of gastrointestinal complaints or frequency of gastritis or peptic ulcer in H. pylori-infected shift workers? Int Arch Occup Environ Health. 2000;83:423–431. | |
Mäntyniemi A, Oksanen T, Salo P, et al. Job strain and the risk of disability pension due to musculoskeletal disorders, depression or coronary heart disease: a prospective cohort study of 69,842 employees. Occup Environ Med. 2012;69:574–581. | |
Kandolin I. Burnout of female and male nurses in shiftwork. Ergonomics. 1993;36:141–147. | |
Scott AJ, Monk TH, Brink LL. Shiftwork as a risk factor for depression: a pilot study. Int J Occup Environ Health. 1997;3 Suppl 2:2–9. | |
Tamakoshi A, Ohno Y, Yamada T, et al. Depressive mood and suicide among middle-aged workers: findings from a prospective cohort study in Nagoya, Japan. J Epidemiol. 2000;10:173–178. | |
Portela LF, Rotenberg L, Waissmann W. Self-reported health and sleep complaints among nursing personnel working under 12 h night and day shifts. Chronobiol Int. 2004;21:859–870. | |
Parkes KR. Shiftwork, job type, and the work environment as joint predictors of health-related outcomes. J Occup Health Psychol. 1999;4:256–268. | |
Inoue M, Nishikitani M, Tsurugano S, Yano E. [The health of permanent workers and workers with precarious employment: a literature review]. Sangyo Eiseigaku Zasshi. 2011;53:117–1139. Japanese. | |
Inoue M, Tsurugano S, Yano E. Job stress and mental health of permanent and fixed-term workers measured by effort-reward imbalance model, depressive complaints, and clinic utilization. J Occup Health. 2011;53:93–101. | |
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An Inventory for Measuring Depression. Arch Gen Psychiatry. 1961;4:561–571. | |
Richter P, Werner J, Heerlein A, Kraus A, Sauer H. On the validity of the Beck Depression Inventory. A review. Psychopathology. 1998;31:160–168. | |
Manocha R, Black D, Sarris J, Stough C. A randomized, controlled trial of meditation for work stress, anxiety and depressed mood in full-time workers. Evid Based Complement Alternat Med. 2011;2011:960583. | |
Wieclaw J, Agerbo E, Mortensen PB, Bonde JP. Risk of affective and stress related disorders among employees in human service professions. Occup Environ Med. 2006;63:314–319. | |
Madsen IE, Diderichsen F, Burr H, Rugulies R. Person-related work and incident use of antidepressants: relations and mediating factors from the Danish work environment cohort study. Scand J Work Environ Health. 2010;36:435–444. | |
Istituto Nazionale per l’Assicurazione contro gli Infortuni sul Lavoro. [Depressione: male al femminile. Solo il 40% in cura dopo un anno di disturbi]. 2011. Italian. Available from: http://www.inail.it/Portale/appmanager/portale/desktop?_nfpb=true&_pageLabel=PAGE_SALASTAMPA&nextPage=Prodotti/News/2011/Lavoro_e_sicurezza/info-939635749.jsp+. Accessed February 22, 2014. | |
Simon GE, Revicki D, Heiligenstein J, et al. Recovery from depression, work productivity, and health care costs among primary care patients. Gen Hosp Psychiatry. 2000;22:153–162. | |
Lam RW, Michalak EE, Bond DJ, Tam EM, Axler A, Yatham LN. Which depressive symptoms and medication side effects are perceived by patients as interfering most with occupational functioning? Depress Res Treat. 2012;2012:630206. | |
Parker G, Brotchie H. Gender differences in depression. Int Rev Psychiatry. 2010;22:429–436. | |
Barton J. Choosing to work at night: a moderating influence on individual tolerance to shiftwork. J Appl Psychol. 1994;79:449–454. | |
Bara AC, Arber S. Working shifts and mental health – findings from the British Household Panel Survey (1995–2005). Scand J Work Environ Health. 2009;35:361–367. | |
Jerg-Bretzke L, Limbrecht K. Where have they gone? – a discussion on the balancing act of female doctors between work and family. GMS Z Med Ausbild. 2012;29:Doc19. | |
Theorell T, Hammarström A, Gustafsson PE, Magnusson Hanson L, Janlert U, Westerlund H. Job strain and depressive symptoms in men and women: a prospective study of the working population in Sweden. J Epidemiol Community Health. 2014;68:78–82. | |
Flo E, Pallesen S, Magerøy N, et al. Shift work disorder in nurses – assessment, prevalence and related health problems. PLoS One. 2012;7(4):e33981 | |
Colman I, Naicker K, Zeng Y, Ataullahjan A, Senthilselvan A, Patten SB. Predictors of long-term prognosis of depression. CMAJ. 2011;183:1969–1976. | |
Hardeveld F, Spijker J, De Graaf R, Nolen WA, Beekman AT. Prevalence and predictors of recurrence of major depressive disorder in the adult population. Acta Psychiatr Scand. 2010;122:184–191. | |
Pinto E, Gillet I, Guelfi JD. [Somatic complains, psychiatric disorders and MMPI 2]. Encephale. 1999;25:103–109. French. | |
Garcia-Campayo J, Ayuso-Mateos JL, Caballero L, et al. Relationship of somatic symptoms with depression severity, quality of life, and health resources utilization in patients with major depressive disorder seeking primary health care in Spain. Prim Care Companion J Clin Psychiatry. 2008;10:355–362. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.